One-Year Results of a Randomized Controlled Clinical Trial of Immediately Loaded Short Implants Placed in the Lower Posterior Single Molar Using a Complete Digital Workflow

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
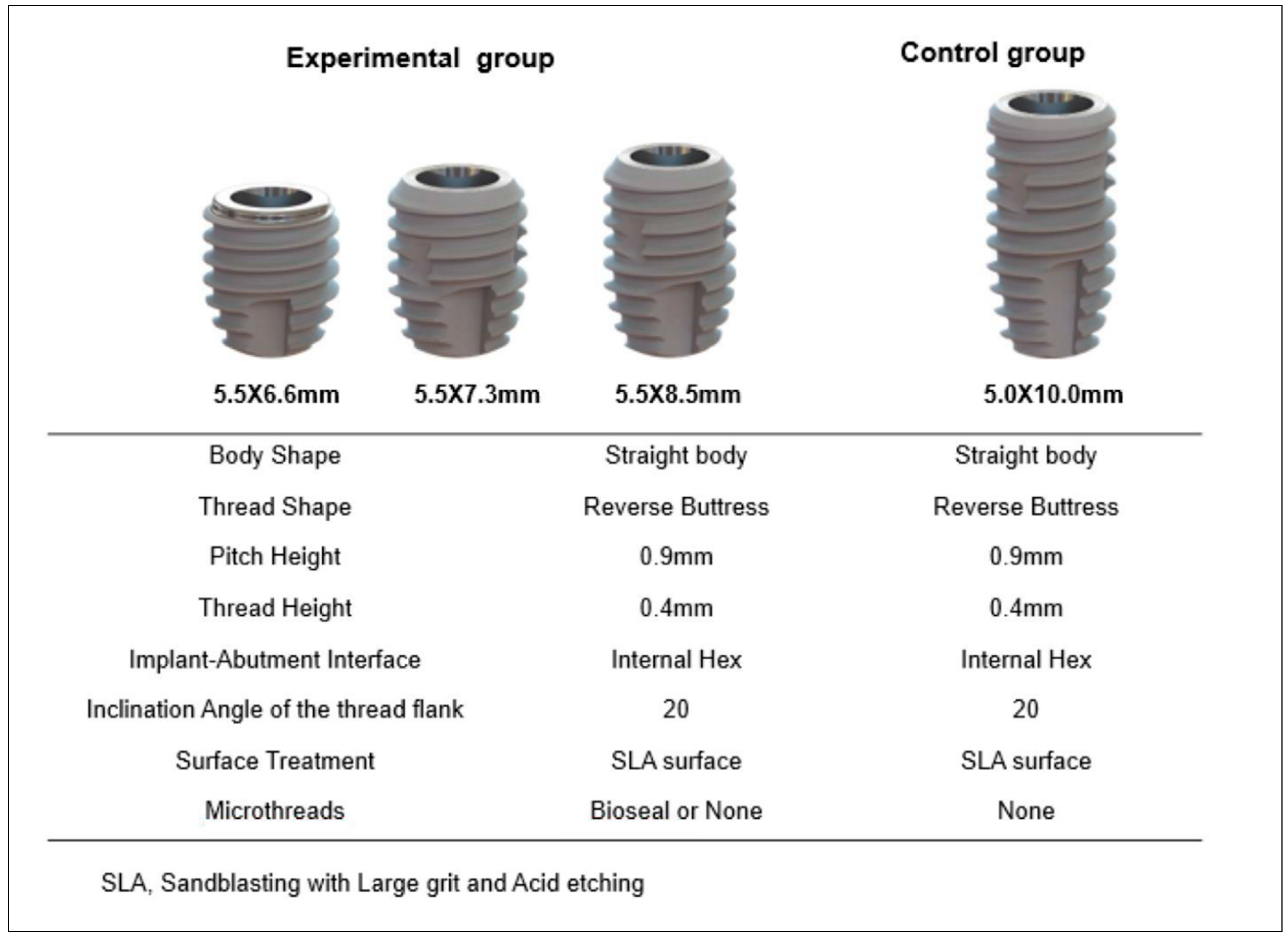
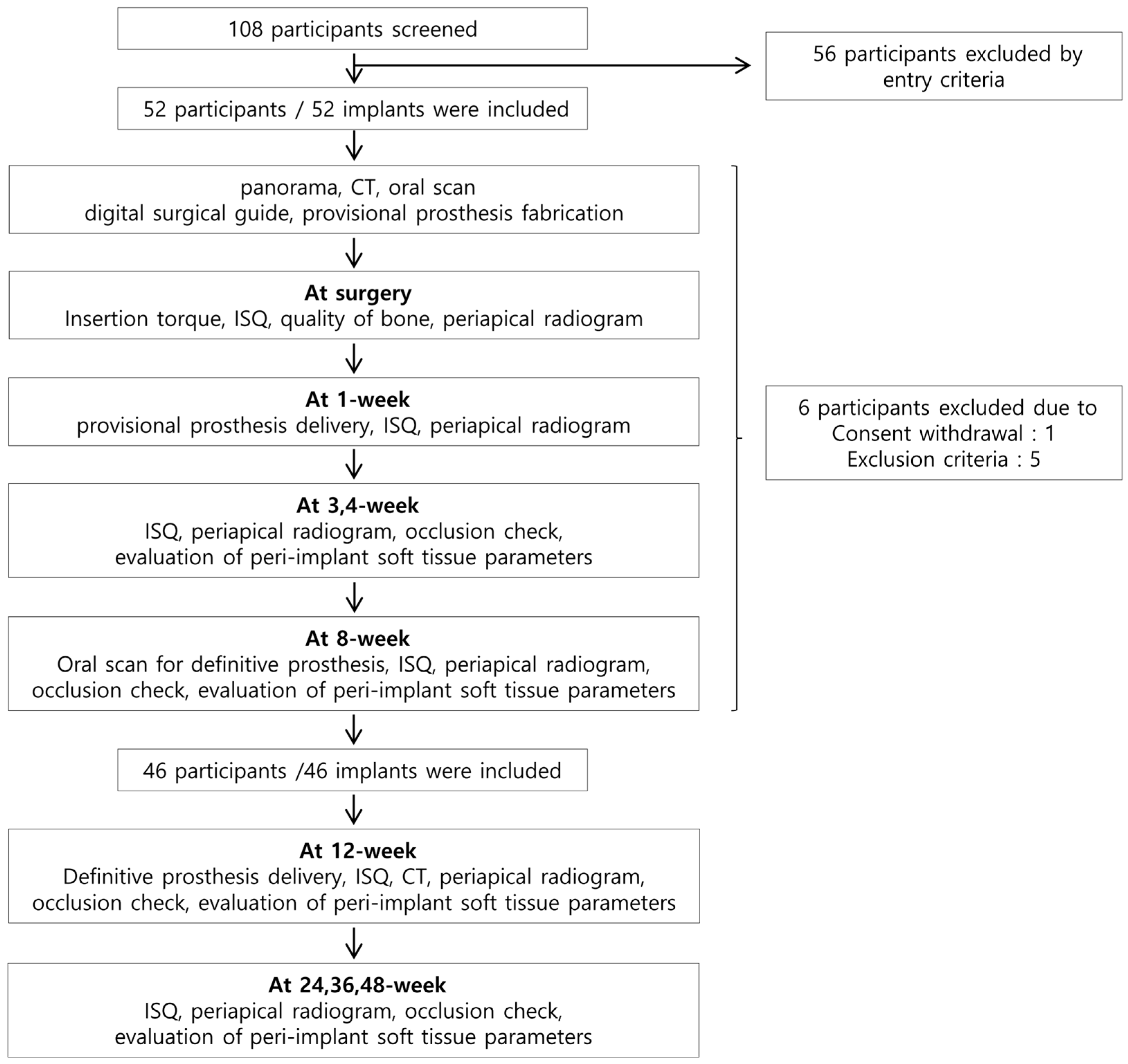
2.1. Clinical Study Design
2.2. Study Population and Entry Criteria
2.3. Treatment Procedure
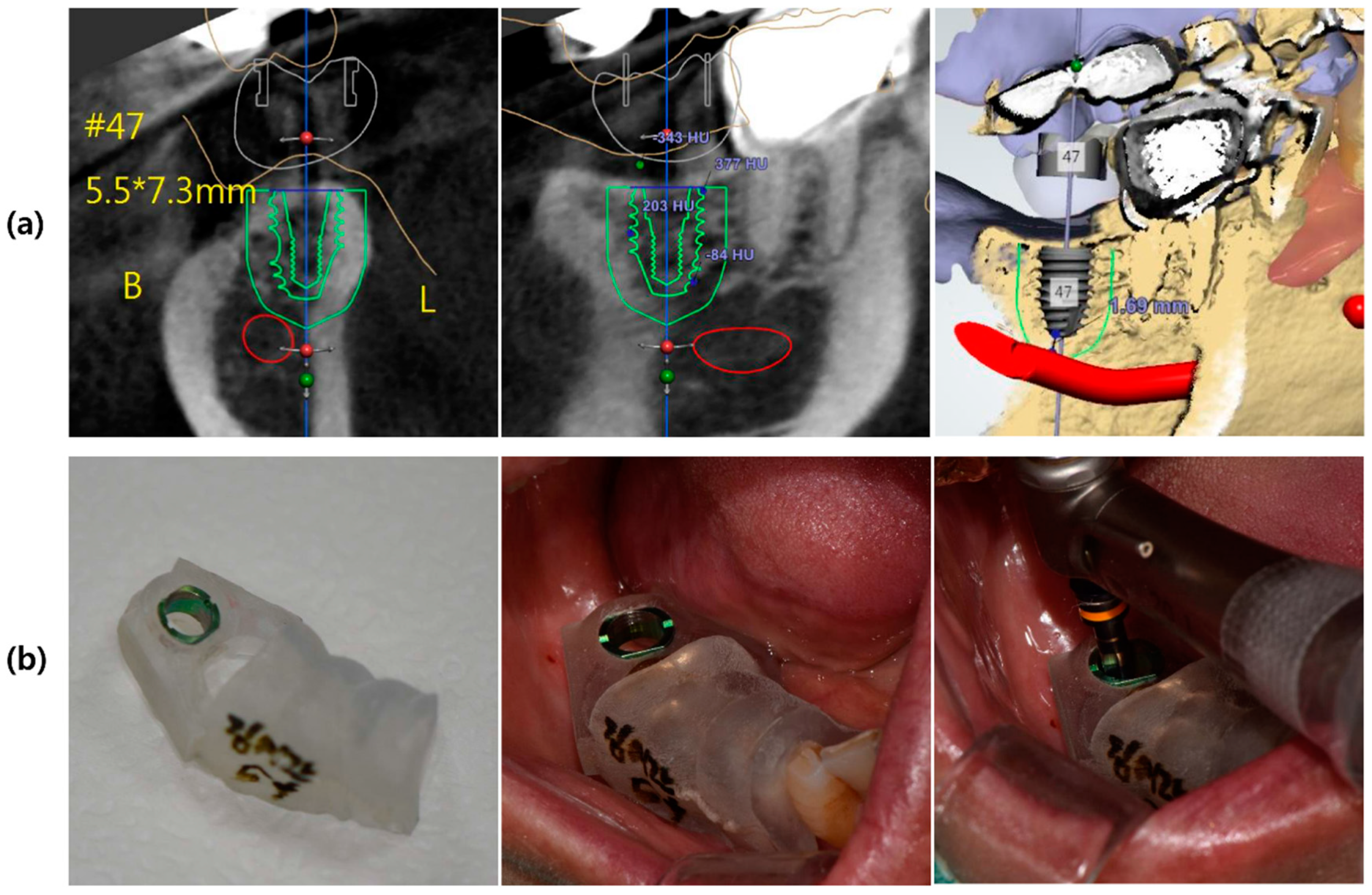
2.3.1. Virtual Planning, 3D Surgical Templates, Ti-Customized Abutment, and Temporary Prostheses
2.3.2. Template-Guided Implant Placement and Evaluation of Implant Stability
2.3.3. Post-Operative Care
2.3.4. Prosthetic Procedure
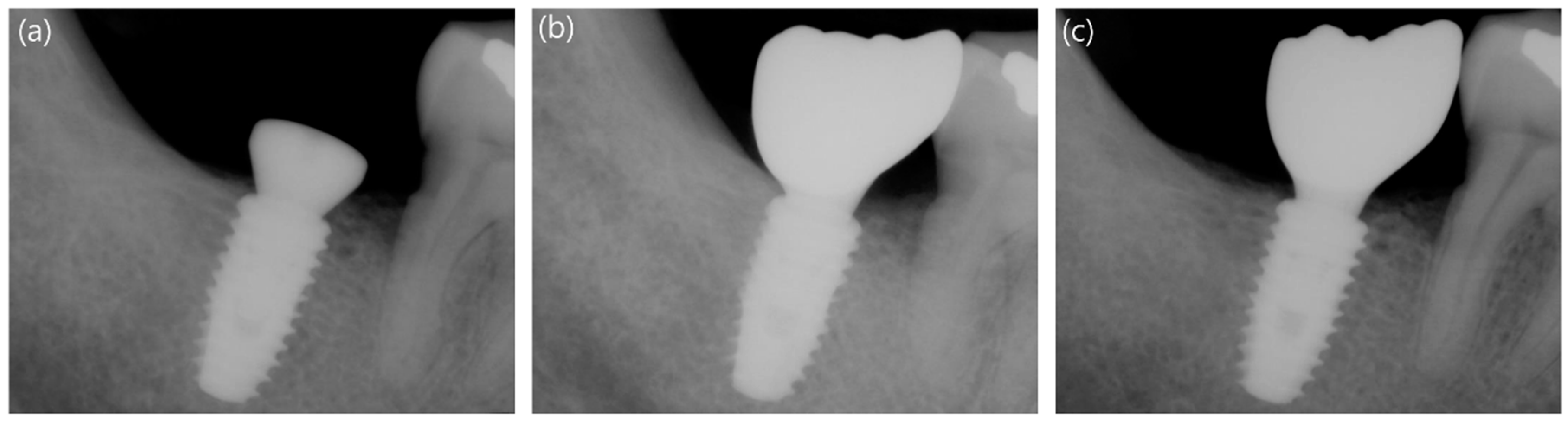
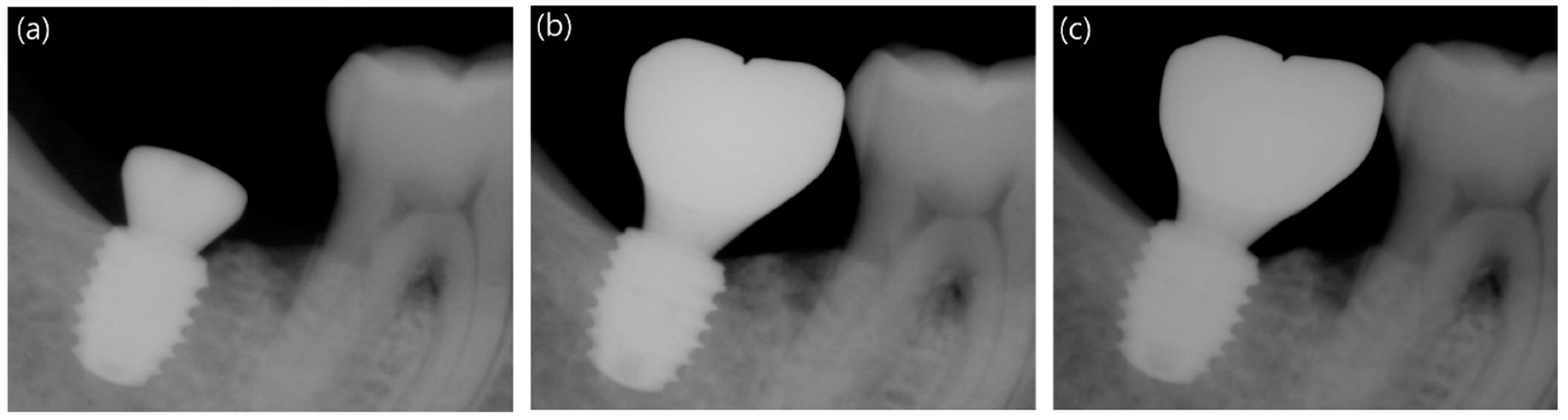
2.3.5. Measurement of Marginal Bone Loss
2.3.6. Follow-Up Procedures and Implant Success
2.4. Statistical Analysis
3. Results
3.1. Participants and Implant Placed
3.2. Demographic Characteristics of the Participants
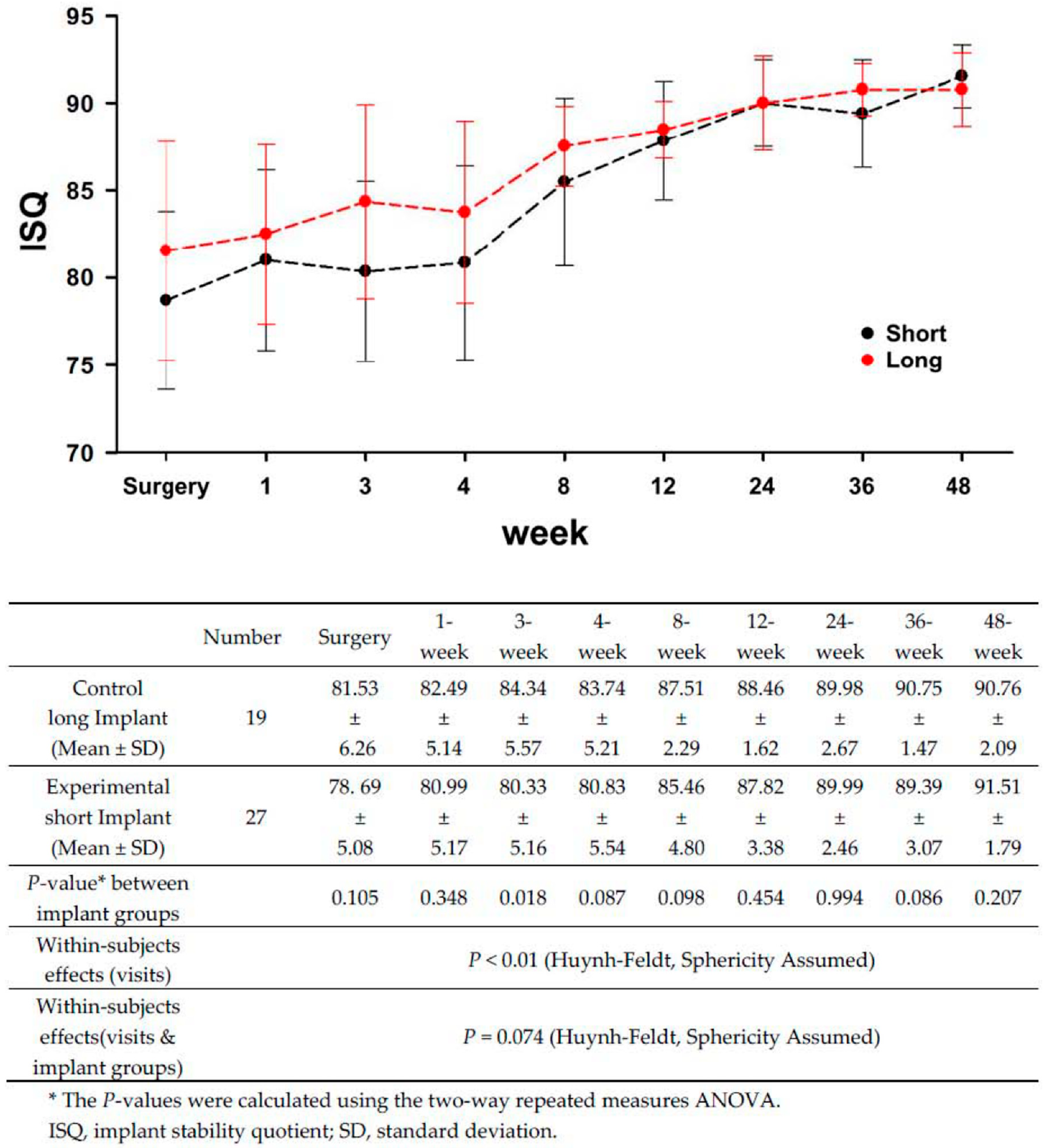
3.3. Comparison of Implant Stability between the Long and Short Implants
3.4. Comparison of Marginal Bone Loss between the Long and Short Implants
3.5. Evaluation of the Peri-Implant Soft Tissue Parameters and Success Rates of the Long and Short Implants
4. Discussion
4.1. Short Implants and Implant Stability
4.2. Implant Length and Stability Dip
4.3. Marginal Bone Loss and Success Rates of Long and Short Implants
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Joda, T.; Brägger, U. Complete digital workflow for the production of implant-supported single-unit monolithic crowns. Clin. Oral Implants Res. 2014, 25, 1304–1306. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Buser, D. Digital implant dentistry—A workflow in five steps. CAD/CAM 2013, 4, 16–20. [Google Scholar]
- Arunyanak, S.P.; Harris, B.T.; Grant, G.T.; Morton, D.; Lin, W.-S. Digital approach to planning computer-guided surgery and immediate provisionalization in a partially edentulous patient. J. Prosthet. Dent. 2016, 116, 8–14. [Google Scholar]
- Brodala, N. Flapless surgery and its effect on dental implant outcomes. Int. J. Oral Maxillofac. Implants 2009, 24, 118–125. [Google Scholar] [PubMed]
- Sicilia, A.; Botticelli, D. Computer-guided implant therapy and soft- and hard-tissue aspects. The Third EAO Consensus Conference 2012. Clin. Oral Implants Res. 2012, 23 (Suppl. 6), 157–161. [Google Scholar] [CrossRef]
- Neldam, C.A.; Pinholt, E.M. State of the art of short dental implants: A systematic review of the literature. Clin. Implant Dent. Relat. Res. 2012, 14, 622–632. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Hämmerle, C.H. Advances in bone augmentation to enable dental implant placement: Consensus Report of the Sixth European Workshop on Periodontology. J. Clin. Periodontol. 2008, 35 (Suppl. 8), 168–172. [Google Scholar] [Green Version]
- Urban, I.A.; Jovanovic, S.A.; Lozada, J.L. Vertical ridge augmentation using guided bone regeneration (GBR) in three clinical scenarios prior to implant placement: A retrospective study of 35 patients 12 to 72 months after loading. Int. J. Oral Maxillofac. Implants 2009, 24, 502–510. [Google Scholar]
- Felice, P.; Soardi, E.; Pellegrino, G.; Pistilli, R.; Marchetti, C.; Gessaroli, M.; Esposito, M. Treatment of the atrophic edentulous maxilla: Short implants versus bone augmentation for placing longer implants. Five-month post-loading results of a pilot randomised controlled trial. Eur. J. Oral Implantol. 2011, 4, 191–202. [Google Scholar]
- Scarano, A.; Piattelli, A.; Murmura, G.; Iezzi, G.; Assenza, B.; Mancino, C. Delayed expansion of the atrophic mandible by ultrasonic surgery: A clinical and histologic case series. Int. J. Oral Maxillofac. Implants 2015, 30, 144–149. [Google Scholar]
- Bahat, O. Branemark system implants in the posterior maxilla: Clinical study of 660 implants followed for 5 to 12 years. Int. J. Oral Maxillofac. Implants 2000, 15, 646–653. [Google Scholar] [PubMed]
- Naert, I.; Koutsikakis, G.; Duyck, J.; Quirynen, M.; Jacobs, R.; Van Steenberghe, D. Biologic outcome of implant-supported restorations in the treatment of partial edentulism: Part 1: A longitudinal clinical evaluation. Clin. Oral Implants Res. 2002, 13, 381–389. [Google Scholar]
- Herrmann, I.; Lekholm, U.; Holm, S.; Kultje, C. Evaluation of patient and implant characteristics as potential prognostic factors for oral implant failures. Int. J. Oral Maxillofac. Implants 2005, 20, 220–230. [Google Scholar]
- Mangano, F.G.; Shibli, J.A.; Sammons, R.L.; Iaculli, F.; Piattelli, A.; Mangano, C. Short (8-mm) locking-taper implants supporting single crowns in posterior region: A prospective clinical study with 1-to 10-years of follow-up. Clin. Oral Implants Res. 2014, 25, 933–940. [Google Scholar] [PubMed]
- Rossi, F.; Botticelli, D.; Cesaretti, G.; De Santis, E.; Storelli, S.; Lang, N.P. Use of short implants (6 mm) in a single-tooth replacement: A 5-year follow-up prospective randomized controlled multicenter clinical study. Clin. Oral Implants Res. 2016, 27, 458–464. [Google Scholar] [CrossRef]
- Esposito; Cannizzaro, G.; Soardi, E.; Pellegrino, G.; Pistilli, R.; Felice, P. A 3-year post-loading report of a randomised controlled trial on the rehabilitation of posterior atrophic mandibles: Short implants or longer implants in vertically augmented bone? Eur. J. Oral Implantol. 2011, 4, 301–311. [Google Scholar]
- Telleman, G.; Raghoebar, G.M.; Vissink, A.; Den Hartog, L.; Huddleston Slater, J.J.; Meijer, H.J. A systematic review of the prognosis of short (<10 mm) dental implants placed in the partially edentulous patient. J. Clin. Periodontal. 2011, 38, 667–676. [Google Scholar] [CrossRef] [Green Version]
- Cochran, D.L.; Morton, D.; Weber, H.-P. Consensus statements and recommended clinical procedures regarding loading protocols for endosseous dental implants. Int. J. Oral Maxillofac. Implants 2004, 19, 109–113. [Google Scholar]
- Esposito, M.; Grusovin, M.G.; Maghaireh, H.; Worthington, H.V. Interventions for replacing missing teeth: Different times for loading dental implants. Cochrane Database Syst. Rev. 2013, CD003878. [Google Scholar] [CrossRef]
- Sanz-Sanchez, I.; Sanz-Martin, I.; Figuero, E.; Sanz, M. Clinical efficacy of immediate implant loading protocols compared to conventional loading depending on the type of the restoration: A systematic review. Clin. Oral Implants Res. 2015, 26, 964–982. [Google Scholar] [CrossRef]
- Benic, G.I.; Mir-Mari, J.; Hämmerle, F.; Christoph, H. Loading protocols for single-implant crowns: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Implants 2014, 29, 222–238. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191. [Google Scholar]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar]
- Buser, D.; Mericske-stern, R.; Pierre Bernard, J.P.; Behneke, A.; Behneke, N.; Hirt, H.P.; Belser, U.C.; Lang, N.P. Long-term evaluation of non-submerged ITI implants. Part 1: 8-year life table analysis of a prospective multi-center study with 2359 implants. Clin. Oral Implants Res. 1997, 8, 161–172. [Google Scholar]
- Misch, C.E. Density of bone: Effect on treatment planning, surgical approach, and healing. In Contemporary Implant Dentistry; Mosby-Year Book, Inc.: St. Louis, MO, USA, 1993; pp. 469–485. [Google Scholar]
- Scherer, U.; Stoetzer, M.; Ruecker, M.; Gellrich, N.-C.; von See, C. Template-guided vs. non-guided drilling in site preparation of dental implants. Clin. Oral Investig. 2015, 19, 1339–1346. [Google Scholar]
- Piero, P.; Lorenzo, C.; Daniele, R.; Rita, G.; Luca, P.; Giorgio, P. Survival of short dental implants≤ 7 mm: A review. Int. J. Contemp. Dent. Med. Rev. 2015, 2015, 011015. [Google Scholar]
- Renouard, F.; Nisand, D. Impact of implant length and diameter on survival rates. Clin. Oral Implants Res. 2006, 17 (Suppl. 2), 35–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldman, S.; Boitel, N.; Weng, D.; Kohles, S.S.; Stach, R.M. Five-Year Survival Distributions of Short-Length (10 mm or less) Machined-Surfaced and Osseotite® Implants. Clin. Implant Dent. Relat. Res. 2004, 6, 16–23. [Google Scholar] [PubMed]
- Sun, H.L.; Wu, Y.R.; Huang, C.; Shi, B. Failure rates of short (≤10 mm) dental implants and factors influencing their failure: A systematic review. Int. J. Oral Maxillofac. Implants 2011, 26, 816–825. [Google Scholar]
- Das Neves, F.D.; Fones, D.; Bernardes, S.R.; do Prado, C.J.; Neto, A.J.F. Short implants-an analysis of longitudinal studies. Int. J. Oral Maxillofac. Implants 2006, 21, 86–93. [Google Scholar]
- Weng, D.; Jacobson, Z.; Tarnow, D.; Hürzeler, M.B.; Faehn, O.; Sanavi, F.; Barkvoll, P.; Stach, R.M. A prospective multicenter clinical trial of 3i machined-surface implants: Results after 6 years of follow-up. Int. J. Oral Maxillofac. Implants 2003, 18, 417–423. [Google Scholar] [PubMed]
- Winkler, S.; Morris, H.F.; Ochi, S. Implant survival to 36 months as related to length and diameter. Ann. Periodontol. 2000, 5, 22–31. [Google Scholar] [PubMed]
- Camps-Font, O.; Burgueno-Barris, G.; Figueiredo, R.; Jung, R.E.; Gay-Escoda, C.; Valmaseda-Castellon, E. Interventions for Dental Implant Placement in Atrophic Edentulous Mandibles: Vertical Bone Augmentation and Alternative Treatments. A Meta-Analysis of Randomized Clinical Trials. J. Periodontol. 2016, 87, 1444–1457. [Google Scholar] [CrossRef]
- Annibali, S.; Cristalli, M.P.; Dell’Aquila, D.; Bignozzi, I.; La Monaca, G.; Pilloni, A. Short dental implants: A systematic review. J. Dent. Res. 2012, 91, 25–32. [Google Scholar] [CrossRef]
- Anitua, E.; Flores, J.; Flores, C.; Alkhraisat, M.H. Long-term Outcomes of Immediate Loading of Short Implants: A Controlled Retrospective Cohort Study. Int. J. Oral Maxillofac. Implants 2016, 31, 1360–1366. [Google Scholar] [CrossRef] [Green Version]
- Lai, H.C.; Si, M.S.; Zhuang, L.F.; Shen, H.; Liu, Y.l.; Wismeijer, D. Long-term outcomes of short dental implants supporting single crowns in posterior region: A clinical retrospective study of 5–10 years. Clin. Oral Implants Res. 2013, 24, 230–237. [Google Scholar] [PubMed]
- Schrott, A.; Riggi-Heiniger, M.; Maruo, K.; Gallucci, G.O. Implant loading protocols for partially edentulous patients with extended edentulous sites—A systematic review and meta-analysis. Int. J. Oral Maxillofac. Implants 2014, 29, 239–255. [Google Scholar] [CrossRef]
- Atsumi, M.; Park, S.H.; Wang, H.L. Methods used to assess implant stability: Current status. Int. J. Oral Maxillofac. Implants 2007, 22, 743–754. [Google Scholar]
- Romanos, G.E. Bone quality and the immediate loading of implants-critical aspects based on literature, research, and clinical experience. Implant Dent. 2009, 18, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Grandi, T.; Garuti, G.; Guazzi, P.; Tarabini, L.; Forabosco, A. Survival and success rates of immediately and early loaded implants: 12-month results from a multicentric randomized clinical study. J. Oral Implantol. 2012, 38, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Margossian, P.; Mariani, P.; Stephan, G.; Margerit, J.; Jorgensen, C. Immediate loading of mandibular dental implants in partially edentulous patients: A prospective randomized comparative study. Int. J. Periodontics Restor. Dent. 2012, 32, e51–e58. [Google Scholar]
- Sennerby, L.; Meredith, N. Implant stability measurements using resonance frequency analysis: Biological and biomechanical aspects and clinical implications. Periodontology 2008, 47, 51–66. [Google Scholar] [CrossRef]
- Simunek, A.; Strnad, J.; Kopecka, D.; Brazda, T.; Pilathadka, S.; Chauhan, R.; Slezak, R.; Capek, L. Changes in stability after healing of immediately loaded dental implants. Int. J. Oral Maxillofac. Implants 2010, 25, 1085–1092. [Google Scholar]
- Javed, F.; Romanos, G.E. The role of primary stability for successful immediate loading of dental implants. A literature review. J. Dent. 2010, 38, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Bischof, M.; Nedir, R.; Szmukler-Moncler, S.; Bernard, J.P.; Samson, J. Implant stability measurement of delayed and immediately loaded implants during healing. Clin. Oral Implants Res. 2004, 15, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Huwiler, M.A.; Pjetursson, B.E.; Bosshardt, D.D.; Salvi, G.E.; Lang, N.P. Resonance frequency analysis in relation to jawbone characteristics and during early healing of implant installation. Clin. Oral Implants Res. 2007, 18, 275–280. [Google Scholar] [CrossRef]
- Pommer, B.; Heuberer, S.; Nahler, L.; Watzek, G. How much bone loss can be prevented by alveolar ridge preservation? Systematic literature review and meta-analysis. Implant News 2012, 9, 795–799. [Google Scholar]
- Simons, W.F.; De Smit, M.; Duyck, J.; Coucke, W.; Quirynen, M. The proportion of cancellous bone as predictive factor for early marginal bone loss around implants in the posterior part of the mandible. Clin. Oral Implants Res. 2015, 26, 1051–1059. [Google Scholar] [CrossRef]
- Weber, H.P.; Crohin, C.C.; Fiorellini, J.P. A 5-year prospective clinical and radiographic study of non-submerged dental implants. Clin. Oral Implants Res. 2000, 11, 144–153. [Google Scholar]
- Cannizzaro, G.; Felice, P.; Leone, M.; Ferri, V.; Viola, P.; Esposito, M. Immediate versus early loading of 6.5 mm-long flapless-placed single implants: A 4-year after loading report of a split-mouth randomised controlled trial. Eur. J. Oral Implantol. 2012, 5, 111–121. [Google Scholar]
- Norton, M.R. The influence of insertion torque on the survival of immediately placed and restored single-tooth implants. Int. J. Oral Maxillofac. Implants 2011, 26, 1333–1343. [Google Scholar] [PubMed]
- Geng, J.P.; Tan, K.B.; Liu, G.R. Application of finite element analysis in implant dentistry: A review of the literature. J. Prosthet. Dent. 2001, 85, 585–598. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Lim, Y.J. Primary stability and self-tapping blades: Biomechanical assessment of dental implants in medium-density bone. Clin. Oral Implants Res. 2011, 22, 1179–1184. [Google Scholar] [CrossRef]
- Kumar, A.B.T.; Khalia, N.; Gayathri, G.V.; Kumar, B.H.D.; Mehta, D.S. Peri-implant crestal bone preservation: Where do we stand? Int. J. Oral Implantol. Clin. Res. 2013, 4, 72–77. [Google Scholar]
- Ryu, H.S.; Namgung, C.; Lee, J.H.; Lim, Y.J. The influence of thread geometry on implant osseointegration under immediate loading: A literature review. J. Adv. Prosthodont. 2014, 6, 547–554. [Google Scholar] [CrossRef]
- Ryu, H.S.; Namgung, C.; Heo, Y.K.; Lee, J.H.; Lim, Y.J. Early loading of splinted implants supporting a two-unit fixed partial denture in the posterior maxilla: 13-month results from a randomized controlled clinical trial of two different implant systems. Clin. Oral Implants Res. 2016, 27, 1017–1025. [Google Scholar] [CrossRef]
- Langer, B.; Langer, L.; Herrmann, I.; Jorneus, L. The wide fixture: A solution for special bone situations and a rescue for the compromised implant. Part 1. Int. J. Oral Maxillofac. Implants 1993, 8, 400–408. [Google Scholar]
- Renouard, F.; Arnoux, J.P.; Sarment, D.P. Five-mm-diameter implants without a smooth surface collar: Report on 98 consecutive placements. Int. J. Oral Maxillofac. Implants 1999, 14, 101–107. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Control (Neobiotech CMI IS-III Active® Long Implant) | Experimental (Neobiotech CMI IS-IIIActive® Short Implant) | p-Value | |
|---|---|---|---|---|
| Participant based (n = 46) | Participant number | 19 | 27 | 0.514 |
| Age (mean ± SD) | 55.42 ± 11.75 | 52.06 ± 11.05 | 0.305 | |
| 20–60 | 13 | 18 | 0.740 | |
| Over 60 | 6 | 9 | ||
| Sex | ||||
| Male /Female | 15/4 | 19/8 | 0.514 | |
| Implant based (n = 46) | Implant number | 19 | 27 | |
| Lower 1st molar / 2nd molar | 9/10 | 4/23 | ||
| Implant Type | 1.000 | |||
| ∅5.00 × 10 mm | 19 | / | ||
| ∅5.50 × 8.5 mm | / | 10 | ||
| ∅5.50 × 7.3 mm | / | 9 | ||
| ∅5.00 × 6.6 mm | / | 8 | ||
| Bone quality | 0.378 | |||
| D112 | 0 | 4 | ||
| D122 | 3 | 3 | ||
| D211 | 0 | 1 | ||
| D222 | 6 | 7 | ||
| D223 | 1 | 1 | ||
| D232 | 0 | 1 | ||
| D233 | 3 | 7 | ||
| D333 | 6 | 3 |
- ‘Control’ indicates the Neobiotech CMI IS-III active® long implant and ‘Experimental’ the Neobiotech CMI IS-III active® short implant.
- Data, except for age are presented as the number of implants or participants. The units of age are year.
- The p-values were calculated using the χ2 test (Pearson Chi-Square) for all variables except age. The p-value for age was calculated using the Mann–Whitney test.
- Bone quality was assessed based on the classification system of Misch (1993) during the drilling sequence. While drilling, divide the depth of the bone into three parts and evaluate the boat quality. D113 indicates that the bone is D1, D1, and D3 depending on the depth.
- SD, standard deviation.
| Control Neobiotech CMI IS-III Active® Long Implant | Experimental Neobiotech CMI IS-III Active® Short Implant | ||
|---|---|---|---|
| Participant number | 19 | 27 | p-value * |
| Insertion Torque (Ncm) (Mean ± SD) | 40.53 ± 5.35 | 38.89 ± 4.85 | 0.298 |
| ISQ at surgery (Mean ± SD) | 81.53 ± 6.26 | 78.69 ± 5.08 | 0.120 |
- * The p-values for insertion torque and ISQ were calculated by the t-test.
- ISQ, implant stability quotient; SD, standard deviation.
| Control Neobiotech CMI IS-III Active® Long Implant | Experimental Neobiotech CMI IS-III Active® Short Implant | |||
|---|---|---|---|---|
| Participant number | 19 | 27 | ||
| Duration | Area | Mean ± SD (mm) | Mean ± SD (mm) | p-value * |
| 12-week follow up | Mesial | −0.22 ± 0.98 | -0.15 ± 0.79 | 0.893 |
| Distal | 0.08 ± 0.81 | 0.20 ± 0.78 | 0.728 | |
| Avg. | −0.07 ± 0.78 | 0.03 ± 0.63 | 0.885 | |
| 48-week follow up | Mesial | −0.15 ± 0.94 | -0.13 ± 0.82 | 0.719 |
| Distal | 0.27 ± 0.80 | 0.23 ± 0.92 | 0.573 | |
| Avg. | 0.06 ± 0.82 | 0.05 ± 0.77 | 0.655 | |
- * The p-values were calculated using the Mann–Whitney test.
- Normality test was failed (Shapiro-Wilk, p < 0.05).
- Area, the radiographic measurement area for calculation of marginal bone loss; Avg., the average value of mesial and distal bone loss; SD, standard deviation.
| Control Neobiotech CMI IS-III Active® Long Implant | Experimental Neobiotech CMI IS-III Active® Short Implant | ||
|---|---|---|---|
| Participant number | 19 | 27 | |
| Parameters | Mean ± SD (mm) | Mean ± SD (mm) | p-value * |
| Plaque index | 0.22 ± 0.20 | 0.32 ± 0.22 | 0.168 |
| Calculus index | 0.00 ± 0.02 | 0.02 ± 0.05 | 0.465 |
| Sulcus bleeding index | 0.03 ± 0.07 | 0.09 ± 0.11 | 0.051 |
| Pocket Depth | 3.38 ± 0.63 | 3.31 ± 0.47 | 0.760 |
| Width of keratinized mucosa (mm) | 2.17 ± 0.54 | 2.18 ± 0.42 | 0.928 |
- * The p-values were calculated using the Mann–Whitney test.
- Plaque index: score 0, no detection of plaque; score 1, plaque only recognized by running a probe across the smooth marginal surface of the implant; score 2, plaque can be seen by the naked eye; score 3, abundance of soft matter.
- Calculus index: score 0, no detection of calculus; score 1, supragingival calculus covering ≤ 1/3 exposed tooth surface; score 2, supragingival calculus covering > 1/3 but < 2/3 tooth surface, flecks of subgingival calculus in cervical margin; score 3, supragingival calculus covering > 2/3 surface, continuous band of subgingival calculus.
- Sulcus bleeding index: score 0, no bleeding when a periodontal probe is passed along the gingival margin adjacent to the implant; score 1, isolated bleeding spot visible; score 2, blood forms a confluent red line on margin; score 3, heavy or profuse bleeding.
- SD, standard deviation.
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baek, Y.-W.; Lim, Y.-J.; Lee, J.; Koo, K.-T.; Kim, M.-J.; Kwon, H.-B. One-Year Results of a Randomized Controlled Clinical Trial of Immediately Loaded Short Implants Placed in the Lower Posterior Single Molar Using a Complete Digital Workflow. Appl. Sci. 2019, 9, 1282. https://doi.org/10.3390/app9071282
Baek Y-W, Lim Y-J, Lee J, Koo K-T, Kim M-J, Kwon H-B. One-Year Results of a Randomized Controlled Clinical Trial of Immediately Loaded Short Implants Placed in the Lower Posterior Single Molar Using a Complete Digital Workflow. Applied Sciences. 2019; 9(7):1282. https://doi.org/10.3390/app9071282
Chicago/Turabian StyleBaek, Yeon-Wha, Young-Jun Lim, Jungwon Lee, Ki-Tae Koo, Myung-Joo Kim, and Ho-Beom Kwon. 2019. "One-Year Results of a Randomized Controlled Clinical Trial of Immediately Loaded Short Implants Placed in the Lower Posterior Single Molar Using a Complete Digital Workflow" Applied Sciences 9, no. 7: 1282. https://doi.org/10.3390/app9071282