1. Introduction
Throughout their careers, elite and amateur sports athletes are exposed to many musculoskeletal injuries that result in severe consequences for health, sports participation, training, or performance [
1]. No less important, all rehabilitation plans involve an over-repetition of certain body movements in the same environment, representing a long, non-dynamic, and exhaustive process [
2]. Consequently, injured players usually become unmotivated, affecting their mental health [
3]. This harmful psychological condition can slow down physical recovery [
4].
On the other hand, the main objective of the various agents involved in a player’s career is the rapid recovery from these injuries. One therapeutic resource that has been growing in interest in the last few years to improve the rehabilitation process’s quality is virtual reality technology (VR) [
5]. VR is a visual-based computer simulation that can reproduce a realistic and controlled environment [
6]. Perceiving and interacting within the created environment are fundamental concepts of VR with important applications in building safe, customized, and enjoyable rehabilitation training environments [
7]. Indeed, from a rehabilitation perspective, VR has become popular in therapeutic programs for different pathologic conditions [
8]. Nowadays, it is possible to find several VR applications developed to support physical, physiological, and even social rehabilitation [
5,
9]. However, in sports rehabilitation, in elite or amateur soccer players, limited data are available about the improvement and engagement of injured players using therapy methods during recovery.
Recent studies developed in the sport context have reported that VR training improves balance, physical functional performance, and physical health compared to therapeutic exercise and may be considered a supplementary therapy to therapeutic exercise [
10,
11,
12]. Several multidisciplinary research groups, including sports scientists, engineers, psychologists, and other health professionals, have hypothesized that sports players could benefit from VR environments during musculoskeletal injury recovery because those systems face participants with multimodal stimulation close to the real context [
11]. Moreover, sports players are provided with suggestions (i.e., a set of external, temporal, or spatial stimuli) that aim to facilitate the performance of the exercise to be rehabilitated [
2].
Based on this rationale, VR gaming could be effective, convenient, enjoyable, entertaining, and affordable since participants receive immediate rewards when specific goals are completed. These VR environments may be an alternative for maintaining exercise adherence by increasing incentives and self-efficacy with positive visual and auditory feedback [
12].
However, it is still an open question which type, intensity, and duration of VR gaming in rehabilitation after a musculoskeletal injury can help players recover faster from injury, enhance cognitive awareness and motivation, and improve their decision-making capacity. For instance, more research is needed to better describe the implementation process of VR games and identify their advantages when included in a rehabilitation program.
To address these fundamental requirements, this study describes the implementation of an entire rehabilitation session using a VR system to help elite or amateur soccer players recover from musculoskeletal injuries. Specifically, the main purposes of this study were (1) to describe a new technological solution for the rehabilitation of musculoskeletal injuries based on VR gaming, and (2) to analyze the variation in rated perceived exertion and heart rate of the participants when undergoing a rehabilitation session based on different VR games according to the standard components of the exercise training.
2. Materials and Methods
2.1. Participants
This study involved 37 participants, 18 males, aged between 19 and 53 years (M = 23.69; SD = 6.98 yrs), recruited at the academic institute. The participants were students from different courses, including engineering, tourism, and physical education. Key inclusion criteria were: (1) students aged 18 years or older from an academic institute; (2) voluntary motivation to participate in the study. The only exclusion criterion was any medical contraindications to sub-maximum exercise according to the guidelines of the American College of Sports Medicine [
13].
All procedures applied were approved by the Ethics Committee of the Faculty of Human Kinetics, CEIFMH No. 39/2021. The investigation was conducted following the Declaration of Helsinki, and informed consent was obtained from all participants. All data were analyzed considering the participants’ confidentiality.
2.2. Virtual Reality Gaming Development
The development of this system required exploratory research based on open interviews with physiotherapists who work directly with professional soccer players. After a qualitative analysis of the transcribed interviews, a list of physical rehabilitation exercises emerged and was validated among all stakeholders. The list of combined exercises makes up for an entire session of musculoskeletal injury rehabilitation. The session was designed and developed in a soccer-themed virtual environment, integrating games mainly for soccer players (
Table 1).
A set of five customized VR games (i.e., “Weight Transfer”, “Military March”, “Side Squat”, “Progressive March”, and “Walking along a Straight Line”; see descriptions below) for soccer players were used to provide a complete rehabilitation session after a musculoskeletal injury.
The VR games contain specific soccer motives and other gamification techniques that help keep users engaged in the process. Although each VR game has been designed to cover the main training domain (e.g., aerobic endurance, upper/lower strength, and motor ability), several game parameters were used to aid the content personalization towards meeting the player’s needs.
Weight Transfer: The weight transfer exercise requires the user to put one foot forward and one foot behind. The purpose of the exercise was to transfer the weight forward and back by raising the toe of the leg that was in front, transferring the weight of the user backward, lowering the toe, and raising the heel of the foot of the leg that was behind to transfer the weight of the user forward. Considering this, the game developed required the user to lift the left toe to select a color to “shoot” signaled in the goal. After selection, the user had to rest the toes of the foot and finally lift the right heel. Raising the right heel activates the laser (used to aim) and the timer (time the user has to select one of the circles). When the user selected the right circle by pressing the trigger from the command, they gained points, and if they chose the wrong one or did not select it in the required time, they lost points.
Military March: The exercise requires the user to raise the left knee until it forms a 90-degree angle with the belly and stretches the right arm simultaneously, then repeat for the opposing members. Considering that aspect, a dartboard was created that the user had to point with their knee and only shoot when the hand was lifted. To implement this idea, two balloons in the air were put in the environment responsible for knowing if the user raised the requested hand. To know how high the balloons had to be, we added the height of the user with the size of their arm when calibrating the avatar. To make the user raise their knee, there was an integrated laser that only appeared when the user lifted their knee to the height they wanted. When the user accomplished these two movements, the user could aim at the dartboard and press the hand’s controller, which was lifted and earned points. To penalize the user when losing balance, the knee was raised, and the user lost points and received audio feedback.
Side Squat: The side squat requires the user to step sideways while pushing the hips back and bringing the torso toward the floor, then stand on the other side and prepare to repeat the back-and-forth movement. The development of this exercise was divided into two parts: the first part was necessary to create something that obligated the user to move to the left and right sides. For that reason, a ball was implemented that went to the left and right sides. The second part was implementing something that obligated the user to crouch down as necessary for the exercise. It was chosen to put inside the virtual environment an object that would indicate if the user did not crouch down when changing sides. The height of the object was determined after the calibration of the avatar. If the user touched their head on the object inside the virtual environment, they lost the opportunity to catch the ball.
Progressive March: The progressive march exercise requires the user to raise the knee until it forms a 90-degree angle with the belly. The user would start in the middle of the field, and when they raised their leg, the avatar in the virtual environment was “pushed” forward, having a virtual movement of the avatar whenever the user raised their leg. When approaching the goal, opponents would appear (opponents of another team that will trip the user), and the user could “shoot” at them by pressing the command button. The user gained points for each “exterminated” adversary, and the user lost points for each adversary that managed to trip them. When getting close to the goal, the user could shoot against the goal for extra points.
Walking along a Straight Line: Walking along a straight line requires the user to follow a straight line with the left foot on the floor and the heel of the right foot touching (on the floor) the left toes, then move the left foot forward of the right foot with the heel of the left foot touching the right toes and repeating until the end of the line. The gamification of the exercise was based on allowing the user to “shoot” to the circles with the color shown in the flag while walking in a straight line in the virtual environment on top of a pole, similar to the previous exercise. To play the game and perform the exercise, the user needed to place the left foot in front of the right foot, touching the heel of the same to the tip of the right foot. After placing the feet in the correct position, a counter was triggered, and the colors of the flags were chosen randomly. Afterward, the user had to walk straight until flag number one and shoot to the right circle. After that, the user had to walk backward until flags number two and three, always shooting to the goal when arriving at the flags.
2.3. Quality of the Movement Assessment and Scoring
A scoring system was used in each exercise to measure if the user was performing the exercise correctly. The system worked by adding points when the user performed the movement correctly and subtracting points when they performed it incorrectly. With this system it was possible to calculate if the user had completed the exercises efficiently. The scoring system ranged between 0 and 200 points for each activity, where 200 points mean that the user performed the activity without any movement failing. In each game described in
Section 2.2, a VR gamification process was implemented. Considering the main goal of each game, the end user won points or was penalized according to their performance. If the end user did not perform correctly, they lost points and received audio feedback in each situation.
2.4. Software and Hardware
The hardware part of the system consisted of the physical equipment required, and the software was responsible for developing the application and connecting with the hardware. As the sensors were placed on key body points (3 “trackers”: on hands, on waist, and on feet), it was possible to know if the user was correctly performing the required exercise. Considering that the application developed used virtual reality with full-body detection, selecting a computer powerful enough to handle this type of computer graphic effort was necessary.
To develop a full-body tracking experience, the option was to use a headset from HTC Vive. We planned to develop the VR system with full-body tracking since it helps to reduce cognitive overhead when performing tasks that involve cognitive processing [
14]. The model chosen was the HTC Vive Pro Set, including a head-mounted display (HMD), two controllers, four SteamVR base stations 2.0, and three trackers. The base stations send signals to the HMD and also track the controllers and trackers.
Virtual reality typically does not use trackers in its systems because they do not need to detect anything other than the head and the hands of the user. As previously mentioned, we chose HTC Vive because it was the best option for obtaining full-body tracking. These trackers bring any real-world object into the virtual world [
15]. In our case, we needed the trackers to collect data from the user’s feet and body to know their position to translate it into the virtual environment.
Unity3D was the game engine used to develop the application. Unity3D is a multi-platform game engine (smartphone, Mac, PC, video game consoles, and web) developed by Unity Technologies. It offers rapid prototyping and the possibility to deploy developed applications on different VR devices. It allows the easy generation of VR applications.
Unity was also employed to experience VR content supporting HTC Vive, Oculus Rift, Valve Index, and others. This plugin helps developers in three main things: loading 3D models for VR controllers, handling input from those controllers, and estimating what the hand looks like using those controllers [
16]. When opening the SteamVR [
17], it is possible to visualize each component of the HTC VIVE hardware automatically and add the wanted trackers afterward.
With the previous tool, creating a virtual reality system was possible, but not full-body tracking. With that in mind, an inverse kinematics library for Unity was selected. Inverse kinematics (IK) is a way to automatically calculate the joint angles of, e.g., a leg or arm based on where the end effector (typically the foot or hand) should be. This allows avatars to synthetically reproduce human motions, even with a limited number of sensor points [
18]. IK works alongside the trackers’ XYZ values to calculate the joint angles.
In developing a virtual application, the environments are critical since the better the environment is, the more immersive the experience can be [
19]. The 3D creation of this application was the combined strength of two creations: the virtual environment and the avatar.
The virtual environment is one of the critical factors for the experience because it creates a connection between the user and the virtual world. All the VR gamification was developed in a specific soccer environment (a virtual replica of a real stadium), making it more realistic and familiar. The software used for modeling the stadium was Blender, based on 2D floor plans available online to model it on an accurate scale.
The avatar is also critical because it allows users to be aware of their members within the virtual world. To create empathy with the avatar, a face was made through 3 photographs, thus allowing all users to select their own avatar in the future. The avatar skeleton was created to link with FinalIK in Unity, thus becoming full-body tracking.
2.5. Study Design
The experiment comprises the following phases. First, participants were asked to fill out a pre-study form, where they had to answer questions related to their demographics (age, gender, nationality) and previous experience with similar technology. Second, a brief explanation of how the system works was given, and then the sensors of the HTC Vive Pro were provided for the user to place on their body. After placing these sensors, the E4 was supplied to place on the wrist. Third, the participants performed 5 VR games accompanied by an explanatory tutorial before starting each of the games. Fourth, at the end of each exercise, the participant reported the perceived exertion (RPE) on that exercise. Fifth, the System Usability Scale (SUS) was collected in the post-experience phase to assess possible application failures. Subsequently, to measure the overall user experience, the Intrinsic Motivation Inventory (IMI) was gathered to understand how immersive the experimental apparatus was.
2.6. Instruments
E4 wristband: The E4 wristband is an empathic band that offers real-time physiological data through four sensors. (1) an electrode for electrodermal activity (EDA), (2) a 3-axis accelerometer, (3) a temperature sensor, and (4) a photoplethysmograph (PPG) to measure blood volume pulse (BVP) from which it derives HR and the inter-beat interval (IBI) [
20].
Rated Perceived Exertion (RPE) Scale: The perceived exertion scale is a scale that allows measurement of the level of intensity of physical activity. In this study, we used the OMNI rating of perceived exertion [
21]. Previously, before participating in the VR game, all participants were individually instructed on the specifics of the OMNI scale, as well as when they were asked individually. The researcher interviewed each participant right after each VR game using the OMNI picture system, which clearly elucidates the different levels of effort and the different possible response options (with 0 indicating a minimum response and 10 indicating a maximum response)
System Usability Scale (SUS): The usability of the VR games was assessed using the European Portuguese Validation of the System Usability Scale (SUS) [
22]. This self-administered instrument allows the evaluation of the usability of the system as well as the user interface. The criteria help to assess the effectiveness, efficiency, and satisfaction with the system. The scale contains 10 questions rated from 1 to 5, with 1 being strongly disagree and 5 strongly agree.
Intrinsic Motivation (IMI): The Portuguese version of the Intrinsic Motivation Inventory was applied to assess the intensity of intrinsic motivation concerning the performance of VR games [
23]. Intrinsic motivation refers to behavior driven by internal rewards. In other words, the motivation to engage in a behavior arises from within the individual because it is naturally satisfying to the behavior [
24,
25]. The score was obtained by averaging the quotation of the items for each dimension. A “Global Intrinsic Motivation” may be considered, with higher scores indicating a greater intrinsic motivation to perform the target activity.
Immersive Tendencies: The level of immersion in the VR games system was assessed using the Immersive Tendencies Questionnaire [
26]. This instrument comprises 18 items and utilizes a scale of 1 (never) to 7 (often), organized into three subdimensions, namely, involvement (seven items), attentional focus (seven items), and tendency to play video games (two items). Two items (item 9 and item 13) are not included in the subdimensions.
Presence: The Witmer–Singer Presence Questionnaire was used to characterize the participants’ experience in the VR games environment [
26,
27]. The Presence Questionnaire is a questionnaire that measures the extent to which a user feels present in the virtual experience, consisting of 24 questions divided into four components: involvement, sensory fidelity, adaptation/immersion, and interface quality. This instrument uses a scale of 1 to 7, with 1 being not convincing and 7 very convincing.
2.7. Statistical Analysis
First, all data were tested for normality (i.e., the Shapiro–Wilk test), and preliminary analyses were performed. Second, descriptive statistics for demographics were calculated. Third, the Friedman test was conducted to assess if there was a change in the rated perceived exertion and heart rate across the five virtual games, following the intensity tracking across an exercise training session: warm-up: (light-to-moderate intensity), conditioning (moderate-to-vigorous intensity), and cool-down (light-to-moderate intensity). Finally, post-hoc tests to compare the rated perceived exertion and heart rate between each virtual game were conducted using individual Wilcoxon signed rank tests. Statistical analyses were performed using IBM SPSS Statistics v.26.0 (IBM, Armank, NY, USA). The significance level was set to p < 0.05.
4. Discussion
This study proposes a potential VR game solution for musculoskeletal injury rehabilitation in elite or amateur soccer players. Based on the physical fitness components that must be trained in the return to the training recovery phase, five virtual games were built with high perceived usability scores, experience, execution/quality of the exercise performed, and the final punctuation achieved in each game. Second, RPE and HR monitoring were used to test a complete rehabilitation session using five virtual games regarding intensity requested throughout the three training session phases (warm-up, conditioning, cool-down). The RPE tracking throughout the session showed better results than HR regarding the intensity expected in each training session phase. Nonetheless, both indicators showed an increase in the first phase of the training session and a decrease in the last stage, which agrees with the recommendations for prescribing a training session.
First, one of the most important issues when a VR game solution for musculoskeletal injury rehabilitation is developed is for it to have acceptance, be usable, support future adoption, and provide interest/enjoyment to the end users [
28,
29]. In our study, a high perception of usability and experience was found, and the estimated time of the experience was lower than the actual time spent, representing a high immersion with the system. A recent review shows that the number of studies describing the acceptability and usability of VR in neuromotor rehabilitation is growing in interest [
30]. However, studies conducted on professional sports athletes are scarce. With the same purpose as our study but using a different sample, Touloudi et al. [
27]) conducted an exploratory study to examine the acceptance, future adoption, interest/enjoyment, and usability of an immersive virtual reality system for exercise training [
31]. The results were closer to ours, showing that participants noted a significant preference, acceptance, interest/enjoyment, and usability of an immersive virtual reality system. However, contrary to Touloudi et al.’s (2022) results, in our study, most participants faced some difficulties or required extra help to understand the immersive virtual reality system. This is probably partly explained by the fact that our sample presented a generally low background in virtual reality. This supports the recommendation of building a tutorial during the experience to support the end user.
Another experiment developed with injured elite soccer players from the same English Championship showed a high VR experience, high standard in quality of graphics and sound, high level of immersion, and VR technology that was comfortable to wear and use [
11]. Our findings partially corroborate these results, showing that these VR games may have great value as a rehabilitation tool. This methodology is expected to increase engagement (i.e., perceived usability, experience, immersive tendency, and presence) and provide a context for more goal-directed movements in the rehabilitation program based on the quality of the movement assessment and the game scores. This system’s important feature provides real-time feedback, which encourages the player to complete the present game stage and motivates them to go to the following stages quickly [
32]. Based on these results, we assume our technological solution for musculoskeletal injury rehabilitation based on VR gaming is a good tool to be used in the context of elite or amateur soccer.
Secondly, VR games have been looked at from an individual perspective. The study of individual VR situations or exercises facilitates the analysis of the impact of each game individually. However, it limits the entire perspective of using several games, intra-connected, with different functional fitness purposes to compose a complete rehabilitation session. To the best of our knowledge, no other study has analyzed the intensity of a VR game sequence throughout an entire rehabilitation session using the rated perceived exertion scale combined with heart rate. It is believed that this may be an objective way to plan physical training throughout the rehabilitation session and improve the end user’s experience throughout the rehabilitation, making the process more pleasant and safe. The results of our study reinforce the use of complementary information from two different instruments to assess the internal load on participants.
To reduce musculoskeletal injuries when introducing a sequence of VR rehabilitation exercises with different physical fitness purposes, it is recommended to include in the training session a warm-up and cool-down, stretching exercises, and a gradual progression of the volume and intensity of the session [
13]. This is a fundamental consideration for exercise prescription with important implications for decreasing the risk of performing repeated VR exercises. It is well known that a single exercise session should include the following phases: (i) warm-up: 5–10 min of a light-to-moderate-intensity aerobic and muscular endurance activity; (ii) conditioning: 20–60 min of aerobic, resistance, flexibility, and neuromotor exercise; and (iii) cool-down: 5–10 min of light-to-moderate-intensity cardiorespiratory and muscular endurance activities [
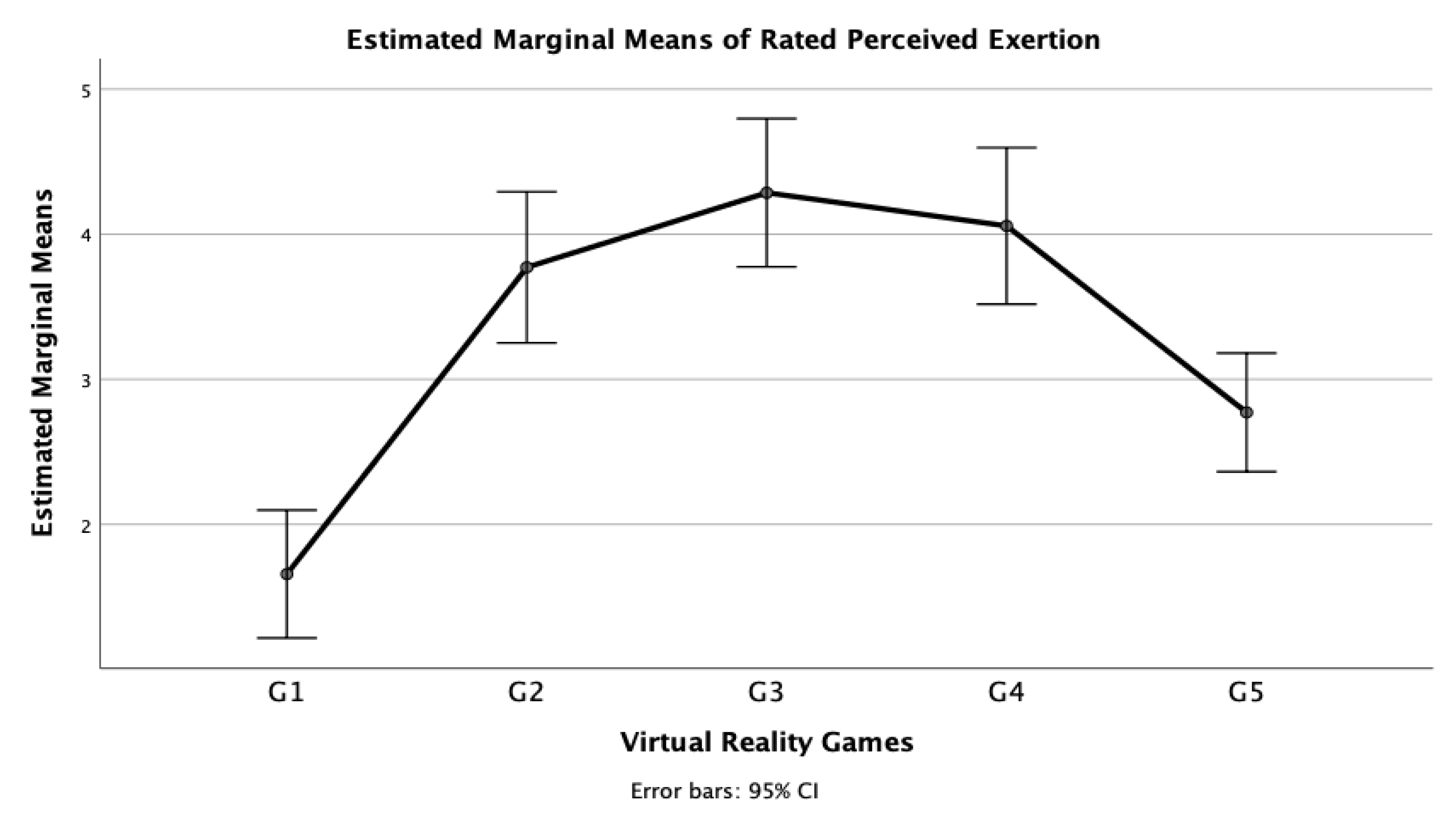
33]. In this study, we used the RPE and HR monitoring throughout the VR games sequence, aiming to assess the gradual progression of the intensity in the session from warm-up to conditioning phases and a regression (i.e., a decrease in the demand of the exercise) between the conditioning and cool-down phases. Indeed, both metrics analyzed (i.e., RPE and HR) showed a gradual progression and then regression of the intensity of the session, being more evident in the curve of RPE (
Figure 1). These results allowed us to validate, in terms of the progression of the intensity, a complete rehabilitation session based on different virtual reality gaming according to the standard components of the exercise training.
Some limitations must be acknowledged when interpreting our results. The first concerns the scarcity of prior literature using a similar experimental design that restricts the comparison with our novel results. Second, the students recruited at the academic institution involved in this user-experience pilot study are different from elite or amateur soccer players, where this solution may be implemented. We also did not control whether participants had football-related connections. Different considerations may arise when using other populations at this technological solution’s development stage. For safety reasons, the sample comprised only non-injured people, which is a good decision at this development stage. However, some concerns may arise about using the system with injured soccer players that may affect the development of the system. Finally, more longitudinal and experimental studies are needed to reinforce the efficacy of using a VR system to recover from musculoskeletal injuries in this entire rehabilitation session.


 ,
, 





{kind=link}
{kind=link}









