
Effects of Exercise on Cardiac Function Outcomes in Women Receiving Anthracycline or Trastuzumab Treatment for Breast Cancer: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registry
2.2. Data Sources and Search Terms
2.3. Eligibility Criteria
- Study type: published randomized controlled trials (RCTs) in English, French, Germany, Portuguese or Spanish languages.
- Participants: trials involving adult women with BC undergoing neoadjuvant or adjuvant anthracycline-containing therapy (AC-T) or TC-T.
- Intervention: Trials delivering an exercise intervention involving aerobic exercise (any exercise form that uses large muscle groups which predominately stresses the cardiovascular system) and/or resistance exercise (any exercise form that requires a muscle or a muscle group to work against external resistance which predominately stresses the musculoskeletal system), comparing to a non-exercise group. To be eligible, the exercise intervention had to be performed during AC-T or TC-T. Trials were not considered if Yoga, Tai Chi Chuan, Qigong or Pilates was defined as the exercise modality.
- Outcomes: Resting LVEF was defined as primary outcome. Secondary outcomes included diastolic function (E/A’ ratio, isovolumetric relaxation time, E/E’ lateral, and E/E’ septal), strain imaging and circulating biomarkers (troponin I or T; high-sensitivity troponin I or T; brain natriuretic peptide; amino terminal of B-type natriuretic peptide or n-terminal pro-b-type natriuretic peptide).
2.4. Data Management and Analysis
2.5. Risk of Bias Assessment
2.6. Statistical Analysis
3. Results
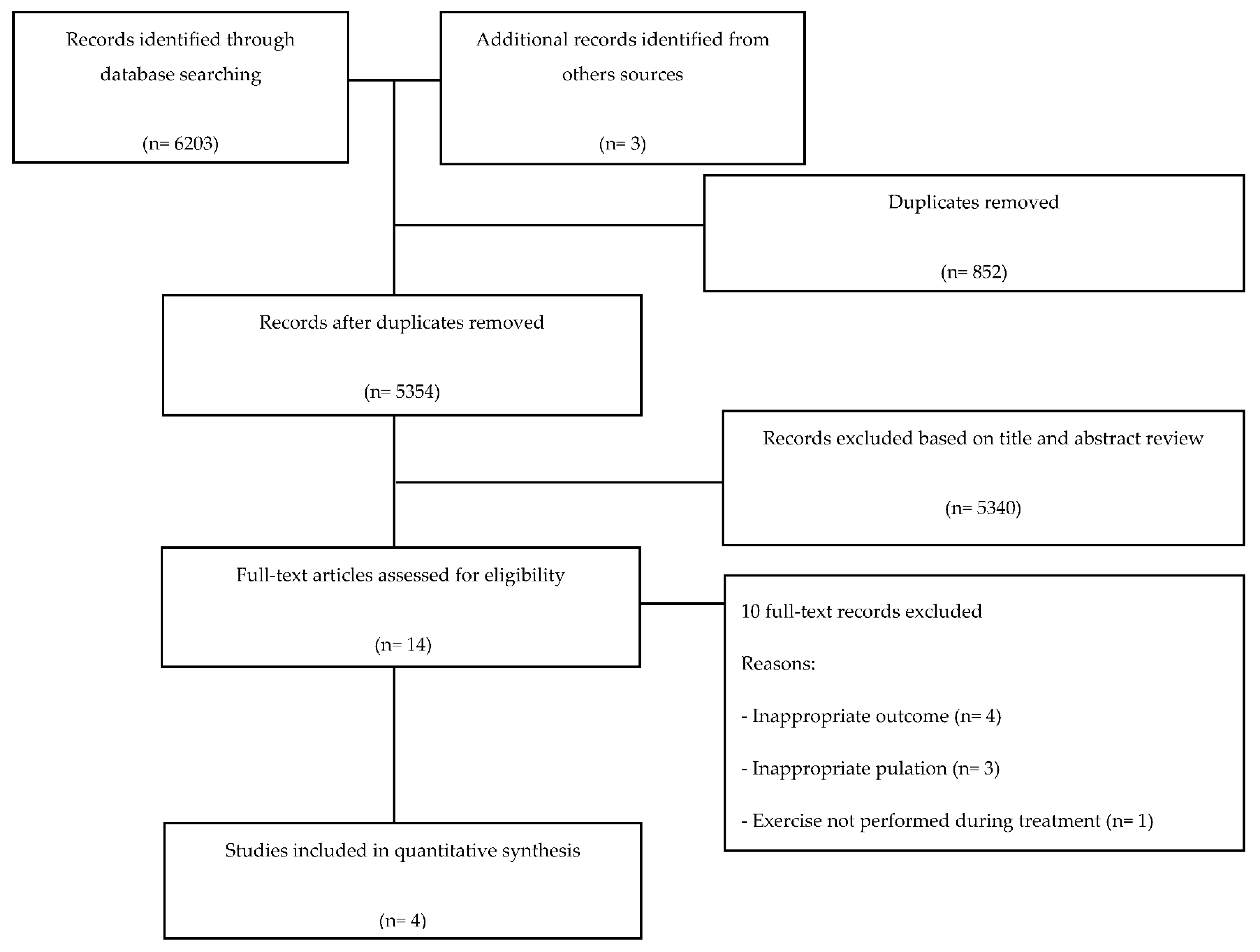
3.1. Study Selection
3.2. Overview of the Included Trials
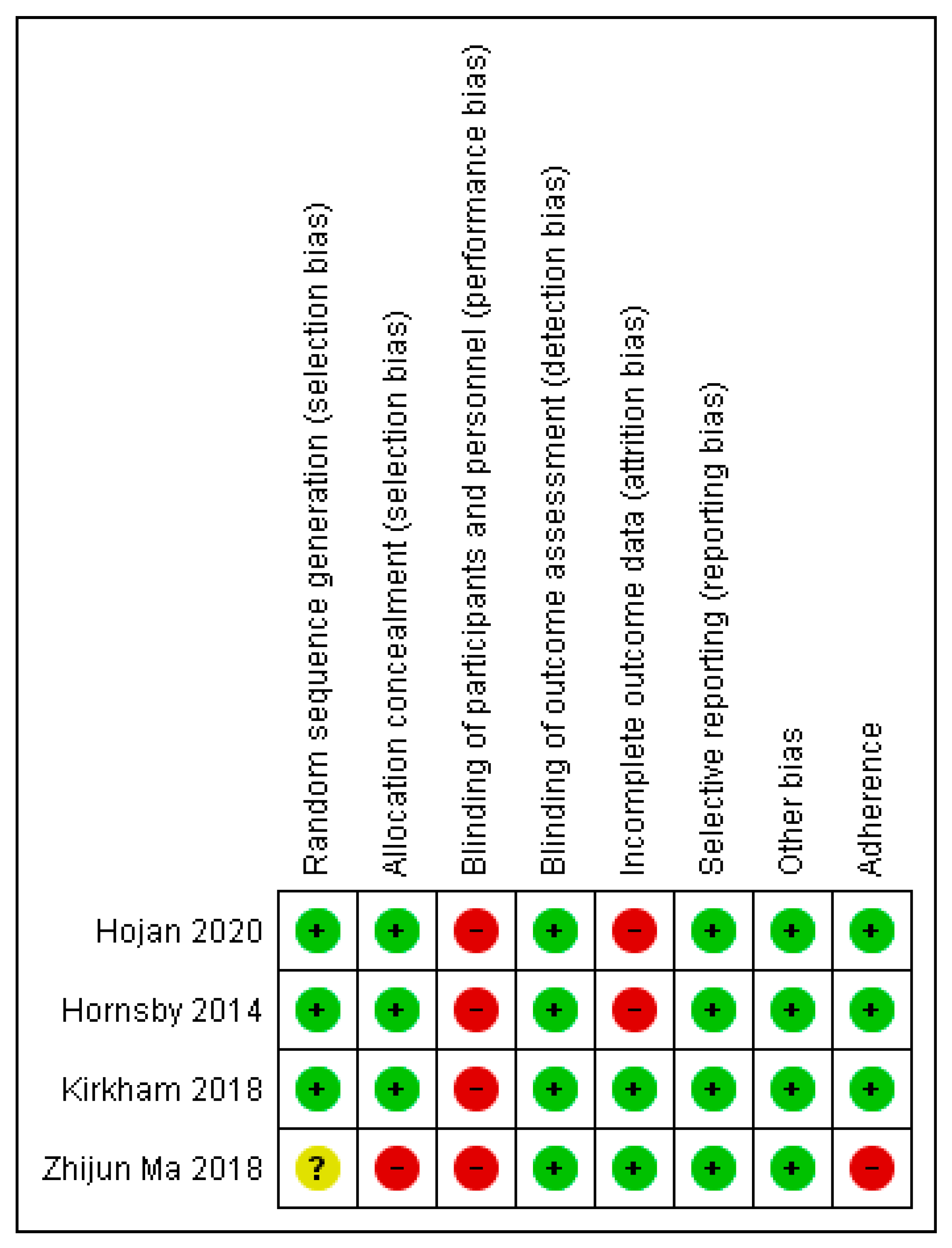
3.3. Risk of Bias
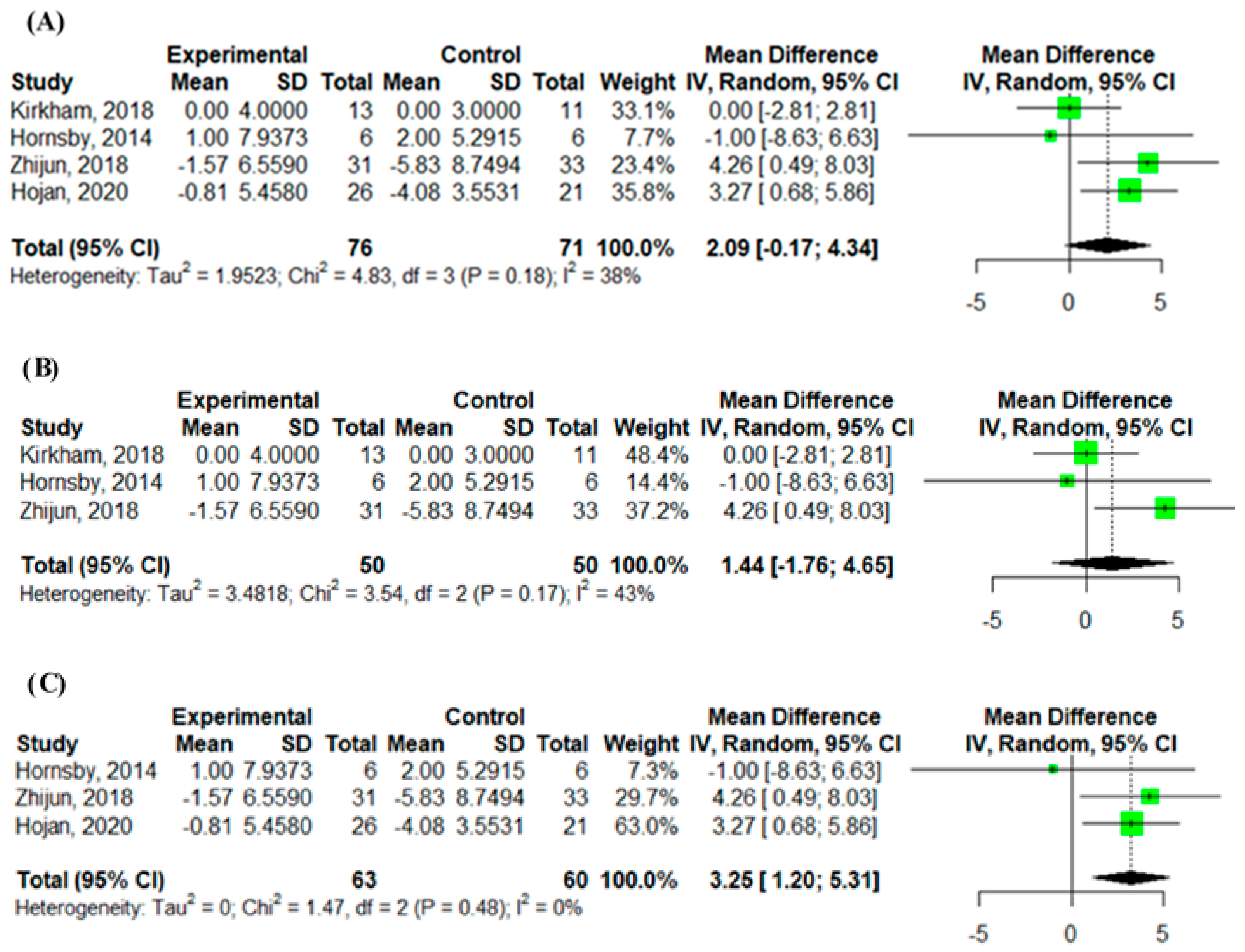
3.4. Effects of Intervention on Primary Outcome
Resting Left Ventricular Ejection Fraction
3.5. Effects of Intervention on Secondary Outcomes
3.5.1. Resting Parameters on Strain Imaging
3.5.2. Resting E/A Ratio
3.5.3. NT-proBNP and Troponin I
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Cancer Society. Cancer Facts & Figures 2020; American Cancer Society: Atlanta, GA, USA, 2020. [Google Scholar]
- American Cancer Society. Cancer Treatment & Survivorship Facts & Figures 2019–2021; American Cancer Society: Atlanta, GA, USA, 2019. [Google Scholar]
- Bodai, B.I.; Tuso, P. Breast cancer survivorship: A comprehensive review of long-term medical issues and lifestyle recommendations. Perm. J. 2015, 19, 48–79. [Google Scholar] [CrossRef] [Green Version]
- Chuy, K.L.; Yu, A.F. Cardiotoxicity of Contemporary Breast Cancer Treatments. Curr. Treat. Options Oncol. 2019, 20, 51. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Qadir, H.; Austin, P.C.; Lee, D.S.; Amir, E.; Tu, J.V.; Thavendiranathan, P.; Fung, K.; Anderson, G.M. A Population-Based Study of Cardiovascular Mortality Following Early-Stage Breast Cancer. JAMA Cardiol. 2017, 2, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Bradshaw, P.T.; Stevens, J.; Khankari, N.; Teitelbaum, S.L.; Neugut, A.I.; Gammon, M.D. Cardiovascular Disease Mortality Among Breast Cancer Survivors. Epidemiology 2016, 27, 6–13. [Google Scholar] [CrossRef] [Green Version]
- Armenian, S.H.; Lacchetti, C.; Barac, A.; Carver, J.; Constine, L.S.; Denduluri, N.; Dent, S.; Douglas, P.S.; Durand, J.-B.; Ewer, M.; et al. Prevention and Monitoring of Cardiac Dysfunction in Survivors of Adult Cancers: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2017, 35, 893–911. [Google Scholar] [CrossRef]
- Zamorano, J.L.; Lancellotti, P.; Muñoz, D.R.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.H.; Lyon, A.R.; et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef]
- Plana, J.C.; Galderisi, M.; Barac, A.; Ewer, M.S.; Ky, B.; Scherrer-Crosbie, M.; Ganame, J.; Sebag, I.A.; Agler, D.A.; Badano, L.; et al. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: A report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 1063–1093. [Google Scholar] [CrossRef]
- Sawaya, H.; Sebag, I.A.; Plana, J.C.; Januzzi, J.L.; Ky, B.; Tan, T.C.; Cohen, V.; Banchs, J.; Carver, J.R.; Wiegers, S.E.; et al. Assessment of echocardiography and biomarkers for the extended prediction of cardiotoxicity in patients treated with anthracyclines, taxanes, and trastuzumab. Circ. Cardiovasc. Imaging 2012, 5, 596–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cave, J.; Paschalis, A.; Huang, C.Y.; West, M.; Copson, E.; Jack, S.; Grocott, M. A systematic review of the safety and efficacy of aerobic exercise during cytotoxic chemotherapy treatment. Supportive Care Cancer 2018, 26, 3337–3351. [Google Scholar] [CrossRef]
- Furmaniak, A.C.; Menig, M.; Markes, M.H. Exercise for women receiving adjuvant therapy for breast cancer. Cochrane Database Syst. Rev. 2016, 9, CD005001. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.W.; Habel, L.; Weltzien, E.; Castillo, A.; Gupta, D.; Kroenke, C.H.; Kwan, M.L.; Quesenberry, C.P., Jr.; Scott, J.; Sternfeld, B.; et al. Exercise and Risk of Cardiovascular Events in Women With Nonmetastatic Breast Cancer. J. Clin. Oncol. 2016, 34, 2743–2749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.; Tripathy, D.; Demark-Wahnefried, W.; Courneya, K.S.; Sami, N.; Bernstein, L.; Spicer, D.; Buchanan, T.A.; Mortimer, J.E.; Dieli-Conwright, C.M. Effect of Aerobic and Resistance Exercise Intervention on Cardiovascular Disease Risk in Women With Early-Stage Breast Cancer: A Randomized Clinical Trial. JAMA Oncol. 2019, 5, 710–714. [Google Scholar] [CrossRef]
- Antunes, P.; Esteves, D.; Nunes, C.; Amarelo, A.; Fonseca-Moutinho, J.; Afreixo, V.; Costa, H.; Alves, A.; Joaquim, A. Effects of physical exercise on outcomes of cardiac (dys)function in women with breast cancer undergoing anthracycline or trastuzumab treatment: Study protocol for a systematic review. Syst. Rev. 2019, 8, 239. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; PRISMA-P Group; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; A Stewart, L. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions.Version 5.1.0 [Updated March 2011]; The Cochrane Collaboration: London, UK, 2011; Available online: www.cochranehandbook.org (accessed on 24 May 2020).
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2009. [Google Scholar]
- Hojan, K.; Procyk, D.; Horyńska-Kęstowicz, D.; Leporowska, E.; Litwiniuk, M. The Preventive role of Regular Physical Training in Ventricular Remodeling, Serum Cardiac Markers, and Exercise Performance Changes in Breast Cancer in Women Undergoing Trastuzumab Therapy-An REH-HER Study. J. Clin. Med. 2020, 9, 1379. [Google Scholar] [CrossRef]
- Hornsby, W.E.; Douglas, P.S.; West, M.J.; Kenjale, A.A.; Lane, A.R.; Schwitzer, E.R.; Ray, K.A.; Herndon, J.E.; Coan, A.; Gutierrez, A.; et al. Safety and efficacy of aerobic training in operable breast cancer patients receiving neoadjuvant chemotherapy: A phase II randomized trial. Acta Oncol. 2014, 53, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Kirkham, A.A.; Eves, N.D.; Shave, R.E.; Bland, K.; Bovard, J.; Gelmon, K.A.; Virani, S.A.; McKenzie, D.C.; Stöhr, E.J.; Waburton, D.E.R.; et al. The effect of an aerobic exercise bout 24 h prior to each doxorubicin treatment for breast cancer on markers of cardiotoxicity and treatment symptoms: A RCT. Breast Cancer Res. Treat. 2018, 167, 719–729. [Google Scholar] [CrossRef]
- Ma, Z. Effect of anthracycline combined with aerobic exercise on the treatment of breast cancer. Pak. J. Pharm. Sci. 2018, 31, 1125–1129. [Google Scholar]
- ACTRN12617001408370. Exercise for Diagnosis and Treatment of Heart Dysfunction among Breast Cancer Patients. Available online: https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=373668(Date registered: 5 October 2017) (accessed on 24 May 2020).
- ISRCTN3261790. Effects of Physical Exercise on Cardiac Health in Women with Breast Cancer. Available online: http://www.isrctn.com/ISRCTN32617901(Date assigned: 24 October 2018) (accessed on 24 May 2020).
- NCT03131024. Caloric Restriction and Exercise for Protection From Anthracycline Toxic Effects (CREATE). Available online: https://clinicaltrials.gov/ct2/show/NCT03131024(First Posted: 27 April 2017) (accessed on 24 May 2020).
- NCT02454777. High-Intensity Interval Training for Stage I-III Breast Cancer Patients. Available online: https://clinicaltrials.gov/ct2/show/NCT02454777(First Posted: 27 May 2015) (accessed on 24 May 2020).
- NCT03027063. Impact of Exercise on Mitigating the Cardio-toxic Effects of Adriamycin among Women Newly Diagnosed With Breast Cancer. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03027063(First Posted: 20 January 2017) (accessed on 24 May 2020).
- NCT03748550. Exercise to Prevent AnthraCycline-Based Cardio-Toxicity Study 2.0 (EXACT2) (EXACT 2). Available online: https://clinicaltrials.gov/ct2/show/NCT03748550(First Posted: 21 November 2018) (accessed on 24 May 2020).
- NCT01621659. Multidisciplinary Team IntervenTion in CArdio-ONcology (TITAN Study) (TITAN). Available online: https://clinicaltrials.gov/ct2/show/study/NCT01621659(First Posted: 18 June 2012) (accessed on 24 May 2020).
- NCT03850171. Cancer Adverse Effects PReventIon with Care & Exercise: The CAPRICE Study. (First Posted: 21 February 2019). Available online: https://clinicaltrials.gov/ct2/show/NCT03850171 (accessed on 24 May 2020).
- NCT03964142. Exercise-Based Cardiac Rehabilitation for the Prevention of Breast Cancer Chemotherapy-induced Cardiotoxicity (ONCORE). Available online: https://clinicaltrials.gov/ct2/show/NCT03964142(First Posted: 28 May 2019) (accessed on 24 May 2020).
- TCTR20190330002. The Exercise Effects on Cardiotoxicity in Breast Cancer Patients Receiving Anthracycline-Based Chemotherapy. Available online: http://www.clinicaltrials.in.th/index.php?tp=regtrials&menu=trialsearch&smenu=fulltext&task=search&task2=view1&id=4503(Date of Primary Registry: 30 March 2019) (accessed on 24 May 2020).
- Antunes, P.; Esteves, D.; Nunes, C.; Sampaio, F.; Ascensão, A.; Vilela, E.; Teixeira, M.; Amarelo, A.L.; Joaquim, A. Impact of exercise training on cardiotoxicity and cardiac health outcomes in women with breast cancer anthracycline chemotherapy: A study protocol for a randomized controlled trial. Trials 2019, 20, 433. [Google Scholar] [CrossRef] [Green Version]
- Jacquinot, Q.; Meneveau, N.; Chatot, M.; Bonnetain, F.; Degano, B.; Bouhaddi, M.; Dumoulin, G.; Vernerey, D.; Pivot, X.; Mougin, F. A phase 2 randomized trial to evaluate the impact of a supervised exercise program on cardiotoxicity at 3 months in patients with HER2 overexpressing breast cancer undergoing adjuvant treatment by trastuzumab: Design of the CARDAPAC study. BMC Cancer 2017, 17, 425. [Google Scholar] [CrossRef] [Green Version]
- Kirkham, A.A.; Paterson, D.I.; Prado, C.M.; Mackey, J.M.; Courneya, K.S.; Pituskin, E.; Thompson, R.B. Rationale and design of the Caloric Restriction and Exercise protection from Anthracycline Toxic Effects (CREATE) study: A 3-arm parallel group phase II randomized controlled trial in early breast cancer. BMC Cancer 2018, 18, 864. [Google Scholar] [CrossRef] [PubMed]
- Pituskin, E.; Haykowsky, M.; McNeely, M.; Mackey, J.; Chua, N.; Paterson, I. Rationale and design of the multidisciplinary team IntervenTion in cArdio-oNcology study (TITAN). BMC Cancer 2016, 16, 733. [Google Scholar] [CrossRef] [Green Version]
- D’Ascenzi, F.; Anselmi, F.; Fiorentini, C.; Mannucci, R.; Bonifazi, M.; Mondillo, S. The benefits of exercise in cancer patients and the criteria for exercise prescription in cardio-oncology. Eur. J. Prev. Cardiol. 2019, 2047487319874900. [Google Scholar] [CrossRef] [PubMed]
- Gilchrist, S.C.; Barac, A.; Ades, P.A.; Alfano, C.M.; Franklin, B.A.; Jones, L.W.; La Gerche, A.; Ligibel, J.A.; Lopez, G.; Madan, K.; et al. Cardio-Oncology Rehabilitation to Manage Cardiovascular Outcomes in Cancer Patients and Survivors: A Scientific Statement From the American Heart Association. Circulation 2019, 139, e997–e1012. [Google Scholar] [CrossRef] [PubMed]
- Nair, N.; Gongora, E. Heart failure in chemotherapy-related cardiomyopathy: Can exercise make a difference? BBA Clin. 2016, 6, 69–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginzac, A.; Passildas, J.; Gadéa, E.; Abrial, C.; Molnar, I.; Trésorier, R.; Duclos, M.; Thivat, E.; Durando, X. Treatment-Induced Cardiotoxicity in Breast Cancer: A Review of the Interest of Practicing a Physical Activity. Oncology 2019, 96, 223–234. [Google Scholar] [CrossRef]
- Kirkham, A.A.; Davis, M.K. Exercise Prevention of Cardiovascular Disease in Breast Cancer Survivors. J. Oncol. 2015, 2015, 917606. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.J.; Wu, P.T.; Middlekauff, H.R.; Nguyen, K.L. Aerobic exercise in anthracycline-induced cardiotoxicity: A systematic review of current evidence and future directions. Am. J. Physiol. Heart Circ. Physiol. 2017, 312, H213–H222. [Google Scholar] [CrossRef] [Green Version]
- Scott, J.M.; Zabor, E.C.; Schwitzer, E.; Koelwyn, G.J.; Adams, S.C.; Nilsen, T.S.; Moskowitz, C.S.; Matsoukas, K.; Iyengar, N.M.; Dang, C.T.; et al. Efficacy of Exercise Therapy on Cardiorespiratory Fitness in Patients With Cancer: A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2018, 36, 2297–2305. [Google Scholar] [CrossRef]
- Maginador, G.; Lixandrão, M.; Bortolozo, H.; Vechin, F.; Sarian, L.; Derchain, S.; Telles, G.; Zopf, E.; Ugrinowitsch, C.; Conceição, M. Aerobic exercise-induced changes in cardiorespiratory fitness in breast cancer patients receiving chemotherapy: A systematic review and meta-analysis. Cancers 2020, 12, 2240. [Google Scholar] [CrossRef] [PubMed]
- Howden, E.J.; Bigaran, A.; Beaudry, R.; Fraser, S.; Selig, S.; Foulkes, S.; Antill, Y.; Nightingale, S.; Loi, S.; Haykowsky, M.J.; et al. Exercise as a diagnostic and therapeutic tool for the prevention of cardiovascular dysfunction in breast cancer patients. Eur. J. Prev. Cardiol. 2019, 26, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Foulkes, S.J.; Howden, E.J.; Bigaran, A.; Janssens, K.; Antill, Y.; Loi, S.; Claus, P.; Haykowsky, M.J.; Daly, R.M.; Fraser, S.F.; et al. Persistent Impairment in Cardiopulmonary Fitness after Breast Cancer Chemotherapy. Med. Sci. Sports Exerc. 2019, 51, 1573–1581. [Google Scholar] [CrossRef] [PubMed]
- Haykowsky, M.J.; Mackey, J.R.; Thompson, R.B.; Jones, L.W.; Paterson, D.I. Adjuvant trastuzumab induces ventricular remodeling despite aerobic exercise training. Clin. Cancer Res. 2009, 15, 4963–4967. [Google Scholar] [CrossRef] [Green Version]
- Yu, A.F.; Flynn, J.R.; Moskowitz, C.S.; Scott, J.M.; Oeffinger, K.C.; Dang, C.T.; Liu, J.E.; Jones, L.W.; Steingart, R.M. Long-term Cardiopulmonary Consequences of Treatment-Induced Cardiotoxicity in Survivors of ERBB2-Positive Breast Cancer. JAMA Cardiol. 2020, 5, 309–317. [Google Scholar] [CrossRef]
- Costello, B.T.; Roberts, T.J.; Howden, E.J.; Bigaran, A.; Foulkes, S.J.; Beaudry, R.I.; Janssens, K.; Haykowsky, M.J.; Antill, Y.; Nightingale, S.; et al. Exercise Attenuates Cardiotoxicity of Anthracycline Chemotherapy Measured by Global Longitudinal Strain. JACC Cardio Oncol. 2019, 1, 295–304. [Google Scholar] [CrossRef]
- Chen, Y.M.; Li, Z.B.; Zhu, M.; Cao, Y.M. Effects of exercise training on left ventricular remodelling in heart failure patients: An updated meta-analysis of randomised controlled trials. Int. J. Clin. Pract. 2012, 66, 782–791. [Google Scholar] [CrossRef]
- Jewiss, D.; Ostman, C.; Smart, N.A. The effect of resistance training on clinical outcomes in heart failure: A systematic review and meta-analysis. Int. J. Cardiol. 2016, 221, 674–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, W.J.; Beaudry, R.I.; Liang, Y.; Clark, A.M.; Tomczak, C.R.; Nelson, M.D.; Ellingsen, O.; Haykowsky, M.J. Meta-analysis of Exercise Training on Left Ventricular Ejection Fraction in Heart Failure with Reduced Ejection Fraction: A 10-year Update. Prog. Cardiovasc. Dis. 2019, 62, 163–171. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hojan et al. [23] | Hornsby et al. [24] | Kirkham et al. [25] | MA [26] | |||
|---|---|---|---|---|---|---|
| Study register | NR | NR | NCT02006979 | NR | ||
| Randomly assigned/withdrawals | n = 68/n = 21 | n = 20/n = 1 | n = 27/n= 3 | n = 70/n= 6 | ||
| Sample size | EG = 26; CG = 21 | EG = 9; CG = 10 | EG = 13; CG = 11 | EG = 31; CG = 33 | ||
| Patients’ characteristics | Stage: IB-IIIA; Age: EG = 54.4 ± 6.2; CG: 54.6 ± 5.2 | Stage: IIB-IIIC; Age: EG = 46 ± 11; CG: 51 ± 6 | Stage: I-III; Age: EG = 51 ± 9; CG: 50 ± 10 | Stage: NR; Age: EG = 44.2 ± 5.7; CG: 43.5 ± 6.3 | ||
| Treatment type | TC-T | AC-T | AC-T | AC-T | ||
| Treatment setting | ||||||
| --- | n = 19 (EG = 9; CG = 10) | n = 8 (EG = 4; CG = 4) | --- | ||
| n = 47 (EG = 26; CG = 21) | --- | n = 16 (EG = 9; CG = 7) | n = 64 (EG = 31; CG = 33) | ||
| Aerobic training | plus | Resistance training | Aerobic training | Aerobic training | Aerobic training |
| Linear | Progressive | Non-linear | Linear | Linear | |
| Supervised | Supervised | Supervised | Supervised | Supervised | |
| 9 weeks/5 TPW (TNES = 45) | 12 weeks/3 TPW (TNES = 36) | Single exercise session prior to each AC-T (TNES = 4) | 16 weeks/3 TPW (TNES = 48) | ||
| Warm-up: 5 min/NR; cool-down: 3 min/NR; aerobic training: 45 min/40% to 80% HRmax; | Sets: 1–3; Reps: 8–10; Load: NR; | Warm-up: NR/NR; cool-down: NR/NR; aerobic training: range from 15–20 min to 30–45 min/range from 60% to 100% of PO; | Warm-up: 10 min/NR; cool-down: 5 min/NR; aerobic training: 30-min/70% of HRR; | Warm-up: 10 min/60–70% HRmax; cool-down: 10 min/60–70% HRmax; aerobic training: 30 min/50–95% HRmax; | |
| 98.7% | 82% | 100% | NR | ||
| No adverse events reported | One non-serious event (leg pain) | No adverse events | NR | ||
| Outcomes of interest | ||||||
| LVEF; GLS; E/A ratio | LVEF | LVEF; LV longitudinal strain; E/A ratio | LVEF; E/A ratio | ||
| NR | NR | NT-proBNP; cTnT | NT-proBNP; | ||
| Timeline assessments | -Baseline: 3 to 6 months after the start of trastuzumab -Post-intervention: After 9 weeks of exercise intervention | -Baseline; NR -Post-treatment: after 12 weeks of exercise intervention | -Baseline: 0 to 14 days prior the start of AC-T -Post-treatment: 7 to 14 days after AC-T | -Baseline: NR -Post-treatment: after 6 and 12 months AC-T | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antunes, P.; Esteves, D.; Nunes, C.; Amarelo, A.; Fonseca-Moutinho, J.; Afreixo, V.; Costa, H.; Alves, A.; Joaquim, A. Effects of Exercise on Cardiac Function Outcomes in Women Receiving Anthracycline or Trastuzumab Treatment for Breast Cancer: A Systematic Review and Meta-Analysis. Appl. Sci. 2021, 11, 8336. https://doi.org/10.3390/app11188336
Antunes P, Esteves D, Nunes C, Amarelo A, Fonseca-Moutinho J, Afreixo V, Costa H, Alves A, Joaquim A. Effects of Exercise on Cardiac Function Outcomes in Women Receiving Anthracycline or Trastuzumab Treatment for Breast Cancer: A Systematic Review and Meta-Analysis. Applied Sciences. 2021; 11(18):8336. https://doi.org/10.3390/app11188336
Chicago/Turabian StyleAntunes, Pedro, Dulce Esteves, Célia Nunes, Anabela Amarelo, José Fonseca-Moutinho, Vera Afreixo, Henrique Costa, Alberto Alves, and Ana Joaquim. 2021. "Effects of Exercise on Cardiac Function Outcomes in Women Receiving Anthracycline or Trastuzumab Treatment for Breast Cancer: A Systematic Review and Meta-Analysis" Applied Sciences 11, no. 18: 8336. https://doi.org/10.3390/app11188336