Smart Intravenous Infusion Dosing System
by
 , , , ,
, , , ,
Dragana Oros
1,* ,
,
Marko Penčić
1,
Jovan Šulc
1,
Maja Čavić
1,
Stevan Stankovski
1 ,
,
Gordana Ostojić
1 and
Olivera Ivanov
2,3 1
Faculty of Technical Sciences, University of Novi Sad, Trg Dositeja Obradovića 6, 21000 Novi Sad, Serbia
2
Faculty of Medicine, University of Novi Sad, Hajduk Veljkova 3, 21000 Novi Sad, Serbia
3
Oncology Institute of Vojvodina, Put Doktora Goldmana 4, 21204 Sremska Kamenica, Serbia
*
Author to whom correspondence should be addressed.
Appl. Sci. 2021, 11(2), 513; https://doi.org/10.3390/app11020513
Submission received: 12 November 2020
/
Revised: 9 December 2020
/
Accepted: 11 December 2020
/
Published: 7 January 2021
(This article belongs to the Special Issue Tele-Rehabilitation Robotics)
Abstract
:Intravenous (IV) infusion therapy allows the infusion fluid to be inserted directly into the patient’s vein. It is used to place medications directly into the bloodstream or for blood transfusions. The probability that a hospitalized patient will receive some kind of infusion therapy, intravenously, is 60–80%. The paper presents a smart IV infusion dosing system for detection, signaling, and monitoring of liquid in an IV bottle at a remote location. It consists of (i) the sensing and computation layer—a system for detection and signaling of fluid levels in the IV bottle and a system for regulation and closing of infusion flow, (ii) the communication layer—a wireless exchange of information between the hardware part of the system and the client, and (iii) the user layer—monitoring and visualization of IV therapy reception at a remote location in real time. All layers are modular, allowing upgrades of the entire system. The proposed system alerts medical staff to continuous and timely changes of IV bottles, which can have positive effects on increasing the success of IV therapy, especially in oncology patients. The prescribed drip time of IV chemotherapy for the full effect of cytostatics should be imperative.
1. Introduction
Intravenous (IV) infusion therapy is a traditional medical procedure that is applied in all branches of medicine and involves the insertion of fluid directly into a patient’s vein using a needle/cannula. IV infusion therapy is especially used during operative and postoperative procedures for the placement of drugs directly into the patient’s bloodstream and for the transfusion of blood or some of its components. In addition, it is used in patients with digestive system disorders; when treating dehydration; for the adjustment of electrolyte imbalances; in oncology patients; and, today, increasingly in the treatment of patients with coronavirus disease 2019 (COVID-19) [1]. Therefore, the probability that a hospitalized patient will receive some type of infusion therapy, intravenously, is 60–80% [2,3].
Although the use of IV infusion is mostly painless, in some cases the procedure is extremely painful, especially in oncology patients using cytostatics. While not all cytostatics are equally aggressive, several months of intravenous cytostatic therapy leaves serious and permanent damage to the veins. In addition to changing color and darkening, these veins greatly reduce their tone, which is why they “withdraw”, and, consequently, become difficult to find during the next therapy session. After several cycles of IV chemotherapy, at some point, there is no longer a vein on the patient’s hands that can withstand daily cytostatic therapy, which is a nightmare and a serious psychological problem for almost all oncology patients. For example, in patients with testicular cancer—seminoma- and non-seminoma-type—cisplatin/etoposide/bleomycin (PEB) and cisplatin/etoposide/ifosfamide (PEI) protocols are used in treatment, respectively. Initial chemotherapy lasts four cycles—shorter/longer if necessary, with one cycle involving 5 days of active IV therapy with cytostatics, 5 IV bottles per day, which is a total of 25 IV bottles during only one cycle. As a result, each subsequent cycle becomes more difficult for patients, not only due to exhaustion but also because the veins are no longer able to withstand all-day chemotherapy. The veins become weak and porous over time and quickly become inflamed, which is why daily therapy, instead of a few hours, lasts significantly longer. A solution for these and other problems would greatly encourage patients and thus increase the success of IV chemotherapy, which is our goal.
The process of administering IV chemotherapy involves the continuous and timely change of IV bottles which requires constant supervision and timely response of medical staff. However, in a situation when there is a large number of patients who receive different types of chemotherapy intravenously, several IV bottles a day, the presence of a nurse for each individual patient is practically impossible. It should be borne in mind that if the IV bottle is not replaced in time, the blood usually returns to the infusion tube, which results in a blocked cannula. There are two ways to solve this everyday problem. One is the use of a syringe and saline solution, which is extremely painful for the patient, and the other, if the first method does not help, is to replace the existing cannula with a new one, often through several attempts because the patient’s veins are already in an advanced stage of trauma, manifested in bruising.
Because of all of the above, we want to pay special attention and invest a great deal of effort to overcome this problem. In this paper, we propose a modern IV infusion dosing system that will be able to detect and signal the liquid level in the IV bottle, as well as to monitor and display the current state of IV infusion at a remote location such as the nurse room. This would significantly improve the traditional approach to IV therapy and greatly help both patients and medical staff, which is a real challenge for us. It should be noted that continuous and timely change of IV bottles can have positive effects on increasing the success of IV therapy, especially in oncology patients, where the drip times of IV bottles are strictly prescribed for the full effect of the drug.
The paper is structured as follows. The first section stresses the motivation and goal of the research. The second section deals with a review of the literature, covering different groups of problems. The third section describes the problem in more detail from an oncological point of view. The fourth section shows a real example of the oncology department on the basis of which the response time of the medical staff is determined. The fifth section shows the configuration and working principle of the smart IV infusion dosing system that we propose. A summary of the results and discussions are presented in Section 6. The final, seventh section contains the conclusion and directions of section research.
2. State of the Art
The development of a smart IV dosing system is a complex problem that includes different elements such as detection of fluid level in the IV bottle, signaling/alarms, regulation and closure of infusion flow, remote location IV therapy monitoring, patient’s database, the efficiency of medical staff, and medical staff response time to alarms. Our literature search identified a significant number of papers focusing on solving each of these individual problems. Therefore, the state of the art section in this paper is divided into five subsections. Each subsection identifies the corresponding problem by describing the state of the art and solving a specific problem.
2.1. Fluid Level Detection and Signaling Systems in IV Bottle/Bag
This subsection presents fluid level detection and signaling systems in an IV bottle/bag using various sensors and alarms placed in the patient rooms and/or nurse room.
A system for measuring the weight of an IV bottle to detect the liquid level in it using a load cell is shown in [4]. The microcontroller receives electrical signals and, on the basis of the defined parameters/response levels, activates the alarm/buzzer and displays a warning on the liquid-crystal display (LCD). The system for detecting fluid level in the IV bag using infrared (IR) sensors is shown in [5]. The converter sends a signal to the microcontroller that activates the voice module (sound recording), alerting the medical staff. The coupling of the load cell for measuring the weight of the IV bag (through fluid level detection in the bag), and the sensor for measuring the patient’s pulse, just before the cannula, is shown in [6]. If the bag empties or the patient’s pulse is outside the allowed values, then the microcontroller sends an alarm to the receiver at the nurse room via the Zigbee module. To detect the change in force/weight of the IV bag, the researchers used force sensors by mapping technique, as shown in [7]. On the basis of the defined threshold—the minimum level of liquid in the IV bottle—the microcontroller wirelessly sends an alarm signal to the nurse room. A sensor for detecting liquid in disposable plastic infusion or urine bags using a flexible capacitive sensor is shown in [8]. It consists of one or more conductive plates that are placed on the outer side of the bag, and with the change of liquid level, the capacitance between the plates changes. The second approach is based on an IR sensor that sends a signal regarding the fluid level in the IV bag to the Arduino controller and, if the minimum level is reached, the system generates a short message service (SMS) alarm to the medical staff [9]. An analysis of different systems for automated real-time IV infusion monitoring using a load cell, IR LED sensors, IR sensors, and ultrasonic sensors, along with the necessary electronics and communication to alert medical staff, is presented in [10]. An IV infusion monitoring system containing an IR sensor, an IV bag, a controller, a buzzer, and an LCD is shown in [11]. The IR sensor—transmitter and receiver—placed next to the IV bag sends a signal to the controller that, at the appropriate time, generates an alarm in the form of an audible and visual signal—a buzzer and an LCD, respectively. The sensor system for monitoring IV infusion shown in [12] uses three electrodes, the first of which is placed on the outlet of the IV bag (spike of drip chamber), the second in the middle of the drip chamber, and the third on the outlet of the drip chamber. By decreasing the fluid level in the IV bag and measuring the change in capacitance, the study generated the data on the remaining volume of the IV bag. A system for monitoring and controlling IV infusion using a photocell to detect and count liquid droplets through a drip chamber is shown in [13]. To display alarm states, the researchers formed a user interface with a screen attached to the IV stand. A prototype of a robotic IV infusion system is presented in [14]. It features an autonomous stand with Mecanum wheels powered by direct current (DC) motors, ultrasonic sensors for the safe movement of the stand, a tracking system with a camera (TAG) for monitoring patient movement, force and flow sensors for detecting fluid levels in the IV bag, and an IR LED sensor for detecting blood if returned to infusion via cannula, after which the valve closes automatically and alarms are sent to the medical staff.
The advantages of the described systems are continuous detection of IV bottle/bag fluid level [4,5,6,7,8,9,11,12,13,14], sound alarm in the patient’s room [4,5,6,8,9,11,13,14], LCD for text alarms in the patient’s room [4,6,9,11,13,14], alarm (sound, SMS or LCD) at the nurse room [6,7,9,12], and additional sensors for fluid level detection or monitoring of the patient’s condition [6,9,12,14].
The disadvantages of the described systems are that there is no alarm at the nurse room [4,5,8,11,13,14]; it is not tested on IV bottle/bag [5,6,7,9,11]; the data are only in the controller, with no backup [4,5,8,9,11,12,13,14]; there is no monitoring application [4,5,6,7,8,9,11,12,13,14] and it has not been tested in hospitals [4,5,6,7,8,9,11,12,13].
2.2. Automated Systems for Regulating and Closing the Flow of IV Infusion
This subsection presents the papers dealing with various fluid level detection systems in IV bottle/bag; however, the focus is on the systems for regulating or closing the infusion flow by using a shut-off valve, directional control valve, or pump.
A system for detecting and regulating the flow of an IV infusion using an optical sensor and an electrically operated valve is presented in [15]. The sensor detects drops through the drip chamber, while each drop activates a timer. After the droplet detection stops or the time between the two-drop detection expires, the timer activates the solenoid valve, which closes the fluid flow. A vision system for detecting and measuring the flow of IV infusion, based on a color background in the form of a matrix, behind a drip chamber, and a digital/webcam to monitor the movement of the droplet, in front, is shown in [16]. Upon the detection of a droplet in the matrix, the corresponding alarm is activated. The IV infusion flow detection and control systems are presented in [17]. The sensor detects the weight of the IV bag and sends signals to the Arduino controller. When the bag is emptied, the controller closes the valve and the return of blood to the infusion is disabled. A method of controlling IV infusion flow by using a sensor module to detect liquid droplets through the drip chamber is shown in [18]. On the basis of the number of drops, the microcontroller calculates the liquid flow and the remaining time for emptying the IV bag, while the actuator regulates the liquid flow, if necessary. A clinical study confirming the efficacy and safety of the use of IV infusion flow monitoring and control devices is presented in [19].
The advantages of the described systems are continuous detection of IV bottle/bag fluid level [15,16,17,18,19], alarm in the patient room or at the nurse room [17,18,19], flow control valve for infusion fluid [16], pump control [18], shut-off valve [15,17], patient monitoring system [18,19], and being tested in hospitals [17,18,19].
The disadvantages of the described systems are that there is no backflow solution [18,19], that there is no alarm in the patient room or at the nurse room [15,16,17,18], the data are only in the controller [15,16,17,18,19], there is no monitoring application [15,16,17,19], and that it was not tested in hospitals [15,16].
2.3. Wireless Communication Systems
This subsection presents wireless communication between (i) the sensor for detecting the fluid level in the IV bottle/bag and the controller that receives the data from the sensor, (ii) the controller that receives the data from the sensor and the user interface on the computer in the nurse room, and (iii) the controller that receives data from sensors and the user interfaces on medical staff smartphones.
The Internet of Things (IoT) system for monitoring IV infusion using an ultrasound and temperature sensor to detect fluid levels in the IV bag, as well as an IR sensor to count liquid drops from the IV bag through the drip chamber, is shown in [20]. The sensors send information to the microcontroller, which, via Global System for Mobile communications (GSM), sends SMS messages, i.e., alarms to medical staff. Monitoring of infusion fluid levels using a humidity sensor is shown in [21]. The humidity sensor, together with sensors for detecting the patient’s temperature and pulse via a microcontroller and Bluetooth connection, sends real-time data to medical staff mobile devices. The IoT infusion monitoring system which comprises a temperature sensor for infusion flow detection, a microcontroller, and a Wireless-Fidelity (Wi-Fi) module is presented in [22]. Liquid level data is transmitted wirelessly from the microcontroller to the IoT cloud, the mobile application, and to the medical staff mobile phones. The use of a wireless flexible capacitive sensor to detect fluid levels in the IV bag by changing the capacitance when the fluid level in the bag decreases is shown in [23]. The sensor communicates wirelessly with a microcontroller that produces an alarm at the appropriate time. A system which involves an optical sensor with a lens for measuring the number of drops of liquid through the drip chamber is presented in [24]. The LED emits light of a predetermined light length and color through different lenses. The electrical signal, which indicates the passage of the droplet, is sent via Bluetooth communication to the microcontroller, and then to the medical staff. The IoT system for monitoring IV infusion, based on the load sensor—detection of the liquid level of the IV bag by measuring its weight—and the IR sensor—counting liquid drips through the drip chamber—is shown in [25]. When the IV bag is emptied, the controller produces an audible and visual alarm to the patient, and the data about this are collected on a server that wirelessly forwards the information to the medical staff. The detection of IV bag weight change using a load cell sensor is shown in [26]. If the IV bag empties, the microcontroller sends the data to the mobile application and medical staff mobile phones via Wi-Fi connection. An infusion monitoring system using artificial intelligence is presented in [27]. It is based on an IR sensor for measuring the number of infusion drops, and the system is designed to monitor the patient’s temperature, blood pressure, pulse, and respiration parameters. These data, along with infusion fluid flow data, are sent to a central processing unit (CPU) that forwards the data to the cloud. A system for monitoring IV infusion flow using two electrodes above and below the drip chamber, used for counting drops of liquid sends signals to the microcontroller, while the display shows the remaining liquid level in the IV bag as a percentage, as is shown in [28]. In addition, data from the microcontroller are forwarded to the nurse room via a Bluetooth module. The use of weight sensors for monitoring the emptiness of the IV bag—measuring the weight of the IV liquid—is shown in [29]. When the fluid level is low, the processor activates an alarm and sends the data to the server and personal digital assistants (PDAs) located in the patient monitoring room. In addition, the authors suggest the use of a bar code or radio-frequency identification (RFID) to generate patient data, IV infusion, etc. A real-time IV infusion monitoring system using a weight sensor to detect fluid levels in the IV bag is shown in [30]. The processor receives signals from the sensor and sends them to the cloud server via a communication module that compares the current and initial liquid level in the IV bag, on the basis of which it generates the remaining time until the IV bag is emptied, and after discharging, the alarm is activated. A wireless patient–nurse communication system is shown in [31]. When an alarm sounds, on the basis of the data collected from hardware and RFID devices, the software connects the patient to the nurse via the voice over internet protocol (VoIP). A system for monitoring a patient’s blood glucose level using a sensor attached to the patient’s body that measures glucose levels and wirelessly sends a signal to the doctor’s phone application and monitoring devices in the nurse room is shown in [32]. If the blood glucose level is outside the range, the alarm in the application is activated. The system for monitoring energy consumption on a test machine using a sensor for measuring the change in current and a module for wireless communication is shown in [33]. The data from the sensor are sent to the cloud server and interpreted to calculate the total operating time of the machine. A robotic system for monitoring a patient with lower limb paralysis using exoskeletons and a cloud server is shown in [34]. The information from the sensor is sent to the cloud server where it is interpreted and, if necessary, the exoskeleton control is adjusted.
The advantages of the described systems are wireless communication between sensor and controller [20,23,24], wireless communication between controller and computer at nurse room [21,22,23,25,26,27,28], the use of IoT technologies [21,22,29,30], mobile application for IV therapy monitoring [21,22,25,26,27,29,30], personal computer (PC) monitoring application [28], continuous detection of IV bottle/bag fluid level [20,21,22,23,24,25,26,27,28,29,30], alarm at the patient or in the nurse room [20,21,22,23,25,26,28,29,30], flow control valve or pump for infusion fluid [20,25,27], and monitoring system in patient’s room [20].
The disadvantages of the described systems are that there is no backflow solution [21,22,23,24,26,28,29,30], there is no IV therapy monitoring application [20,23,24], there is no wireless between communication controller and control panel [20,24], there is no usage of IoT technology [20,23,24,25,26,27,28], and it has not been tested in hospitals [20,21,22,23,24,25,26,27,28,29,30].
2.4. Department Configuration, Room Layout, and Efficiency of Medical Staff
This subsection presents how the configuration of the department—rectangular, centralized or hybrid—as well as the position of the patient rooms in relation to the medical staff room, affect the efficiency and response time of medical staff to alarms.
According to [35], if the rooms for medicaments and medical staff are positioned centrally with regard to the patient rooms surrounding them, then the path to the farthest patient is shorter and the efficiency of the medical staff is higher. The influence of the department configuration, room layout, and the number of beds in the rooms on the walking distance and the response time of the medical staff is shown in [36]. The medical staff walking distance in the rectangular configuration department is longer than in the circular configuration. In addition, the efficiency of medical staff is affected by the existence of a unified system for monitoring the patients’ conditions, the layout of rooms in the department, the distribution of work tasks among nurses, as well as good cooperation and exchange of information between medical staff [37]. According to [38], the room for medical staff should be a modern and dynamic environment with new technologies where a good exchange of information is imperative. Moreover, the centralization of the room for medical staff enables better communication between the staff, a shorter path to the patients, and thus a shorter response time to alarms. An analysis of nurses’ movements using PedSim software in a total of eight departments with different room and bed layouts is presented in [39]. The nurse response time is shorter by 15% in the centralized arrangement of patient rooms with regard to the nurse room. According to [40], hybrid room layout—a combination of rectangular and centralized room layout—reduces the maximum distance and response time of medical staff by 60%. The impact of decentralized room layout on the communication between medical staff is presented in [41]. The medical staff was stationed in front of the patient rooms, which implies a significantly shorter response time, but because of that, the communication between the medical staff was minimized. The influence of the daycare center structure in nursing homes on the communication between staff and patients is presented in [42]. Acoustics affect the quality of verbal communication, especially in patients who have speech difficulties as a result of a stroke or in patients with dementia for whom even a minimal noise level affects the ability to communicate. An analysis of the distance that medical staff should travel depending on the layout of the rooms in the department is presented in [43]. Although it initially seemed different, the distance that staff has to travel is actually not longer in departments with a larger number of patient rooms when the layout of the rooms in the department is centralized. With a straight-line layout, as the number of patient rooms increases, the distance that staff needs to cover increases. According to [44], the use of the Pepid mobile application does not reduce the distance that nurses have to travel or the response times. However, medical staff has increasing confidence in mobile applications intended for hospitals, which is significant.
2.5. Medical Staff Response Time to Alarms
The last subsection presents the response time of medical staff to alarms (for different scenarios) in order to obtain feedback from patients on the response speed of medical staff, which greatly affects patient satisfaction.
An analysis of the response time of medical staff using a stopwatch and surveying a total of 30 patients at the Indonesian National Hospital is presented in [45]. The response time of medical staff is within the legitimate values, with female patients being more satisfied with the service (in terms of response time) than male patients. An analysis of the response time of medical staff in monitoring pulse oximetry in a total of 103 patients is presented in [46]. When any of the oxygen parameters is outside the allowable values, a green light alarm is activated in front of the patient’s room. The medical staff on duty have 15 s to react to that alarm, otherwise a flashing green light in front of the patient’s room and an audible alarm in the monitoring room are activated for another medical worker to react. If the staff does not react even after 3 min and 15 s, an emergency alarm is activated in the medical staff room—a louder alarm of stronger intensity and a flashing green and white light in front of the patient’s room. As many as 26% of missed initial alarms were recorded—40% of missed alarms generated after 2 min and 27% of missed alarms generated after 3 min. An analysis of the response time of medical staff to light alarms in four nursing homes is presented in [47]. There were light signals in front of each patient’s room, where the red light indicates that the patient needs help in the bathroom, while the white light indicates the necessary help when moving in the room. Due to frequent alarms, the response time was outside the defined standards, while in as many as 50% of cases, the staff responded only after 5 min. According to [48], the medical staff diminish the importance of light alarms, especially when the patient is not endangered, and therefore either do not respond to light alarms or react very slowly. An analysis of alarm response time via video recordings of patients connected to ventilators in a children’s hospital is presented in [49]. Each of the 36 nurses was assigned two or four patients, resulting in a total of 5070 on-call alarms. With the increase in the number of alarms that do not require an urgent response, the response time of nurses has increased significantly. A study which analyzed the response time of medical staff in the emergency department using a questionnaire completed by the patients found that they considered the response time of the medical staff to be unsatisfactory [50]. An analysis of nurses’ response times to patient calls by canceling alarms is presented in [51]. In this experiment, after deactivation of the existing alarms in the department, each nurse was assigned one patient per day. With frequent changes of nurses and the exchange of key information about patients during short team meetings, the response time of nurses has decreased, but with the importance of engagement and effort of nurses, which is impossible for a longer period and a larger number of patients.
2.6. Summary
On the basis of the analysis of the literature review, we conclude that there is no comprehensive research that represents a unique solution to the problem of detection, monitoring, and control of an automated system for IV infusion therapy, taking into account the response time of medical staff. In addition, remote control, as an Industry 4.0 technology, is particularly suitable for hospital systems because it allows medical staff to easily and quickly, wirelessly, change system parameters in real time, manage the entire process, and access and download data about patients hosted on a cloud server, which is our goal.
3. Problem Description
Non-automated IV infusion systems are most commonly found in hospitals around the world. Figure 1 shows a traditional IV infusion therapy set consisting of four main elements: a pole/stand (1) on which one or more IV bottles/bags (2) of appropriate content are placed and an IV tubing set (5–8) for connection and transfer of fluid from the IV bottle/bag to the cannula (9), allowing fluid to be infused directly into the patient’s vein. The IV tubing set consists of a drip chamber (5) whose role is multiple, a piggyback port (6) for connecting an additional IV bottle/bag if necessary, IV tubing (7), and a roller clamp (8) for manual adjustment of the infusion flow. The drip chamber, at one end has spikes (3) for connection to the IV bottle/bag by penetration, while on the opposite side it is connected to the IV tubing. Moreover, laterally, there is an air valve (4) to prevent the appearance of a vacuum. In addition, the drip chamber prevents the transfer of air into the patient’s bloodstream, which is extremely important, because otherwise an arterial gas embolism occurs with dramatic consequences.
According to [52], the most common reasons for receiving IV infusion are replacement of lost fluid and electrolytes; for chemotherapy, anesthesia, or drugs that the patient cannot receive orally; for transfusion of blood or blood plasma during or after surgery as a result of heavy bleeding; and for the intake of vitamins, minerals, and other trace elements. Numerous complications are possible, such as pulmonary edema that causes breathing problems; the appearance of air plugs, which is manifested by shortness of breath, neck pain, and dizziness; and catheter embolism when part of the cannula breaks off and enters the bloodstream. Moreover, local and systemic infections cause sepsis by penetrating the patient’s bloodstream, leading to the presence of pyrogenic substances in the infusion as a result of non-sterile preparation of the drug; rupture of veins and bleeding; artery puncture; phlebitis manifested by pain along the cannula; redness; locally elevated skin temperature; and extravasation of the drug that causes pain, tingling, and swelling along the vein.
Some IV therapies have a prescribed infusion time due to the full effect of the drug. However, the infusion rate directly depends on the pressure produced by the height of the liquid column in the IV bottle/bag, as well as on the position of the bottle/bag in relation to the cannula (see Figure 1, distance L). In addition, partial or complete closure of the IV tubing due to bending by moving the patient’s arm—e.g., the patient falls asleep—as well as the deposition of various components of fluid in the vessel such as blood cells, can have negative effects on fluid flow. Nevertheless, the condition of the veins remains crucial, especially in oncology patients. Therefore, the analysis of one of the most common malignant diseases of young men—testicular cancer—whose treatment requires several months of IV infusion chemotherapy, is presented briefly.
3.1. Testicular Cancer
Although the COVID-19 virus is a burning problem in the world, with currently over 52 million cases and 1.29 million deaths [53], cardiovascular and malignant diseases are still the leading causes of death worldwide, with close to 18 and 10 million deaths in 2017, respectively [54,55]. However, in malignant diseases, this number increases dramatically [56,57,58]. In testicular cancers, which are the most common malignant disease in men between 14–44 years of age [59,60], with a peak incidence at 30–34 years of age [61,62], a sudden increase in the number of patients half a century ago was recorded [63,64], which was equally influenced by hereditary factors and environmental conditions [59]. Developed countries such as New Zealand [65], Norway [66], Canada [67], Denmark [68], Great Britain [69], Israel [70], Czech Republic [71], Australia [72], Croatia [73], the USA [74], France [62], Germany [75], and Switzerland [76], saw a significant increase in testicular cancer. According to [77,78], this type of cancer affects the populations of Europe and Australia the most, and Asia and Africa the least. In addition, the highest incidence in the world is in the Scandinavian countries [79]. It is also estimated that the number of people with testicular cancer will increase in almost all European countries by 2035 [80]. However, in the case of timely diagnosis and beginning of treatment, the cure rate in European countries is as high as 95–97% [81,82].
3.2. IV Chemotherapy
Testicular cancer most often arises from germ cells—seminoma- and non-seminoma-type. At diagnosis, approximately 70% of cases are detected in the first stage of the disease when the cure rate is extremely high. The success of the treatment is also attributed to the fact that this type of cancer is very sensitive to IV chemotherapy and radiotherapy, which is why these treatment modalities are widely used in clinical practice [83]. Platinum-based chemotherapy is most commonly used [84]. The combination of cytostatics, cisplatin/etoposide/bleomycin, the so-called PEB protocol, is the standard in treatment after the initial surgical procedure for seminoma- and non-seminoma-type tumors. When there are poor prognostic parameters, 1–2 cycles of chemotherapy are applied, while for metastatic disease, 3–4 cycles are used [85,86]. However, if the disease relapses or is refractory to the PEB protocol, then another combination of cytostatics, cisplatin/etoposide/ifosfamide, the so-called PEI protocol, is used.
The PEB protocol involves the intravenous administration of cisplatin and etoposide in the appropriate dose, from the first to the fifth day of the cycle, as well as the intravenous administration of bleomycin in the form of an intravenous bolus on the 1st, 8th, and 15th days of the cycle. The PEI cycle involves the intravenous administration of cisplatin, etoposide, and ifosfamide in the appropriate dose, from the first to the fifth day of the cycle [87]. In addition, before and after the IV infusion, the patients receive appropriate premedication as an intravenous bolus using corticosteroids and antiemetics. One cycle of chemotherapy lasts a total of 21 days, after which the therapy is repeated.
Table 1 shows the parameters of daily IV chemotherapy for both protocols. In addition to the order of administration of IV bottles and the appropriate cytostatics, the recommended drip times for each IV bottle are shown separately. Therefore, the total recommended infusion drip time for the PEB protocol is 195–220 min, while for the PEI protocol it is slightly longer at 245–270 min.
On the basis of this, we conclude that the treatment of patients with testicular cancer using cytostatics is intravenous, very long, complex, and exhausting, but largely a known process, which is unthinkable without the use of IV infusion, whose properties we want to improve. In addition, the time of IV infusion drip required for the full effect of chemotherapy, despite its length and regardless of the number of cycles, should be imperative, which is only possible by using modern systems for detection, monitoring, regulation, and stop of IV infusion flow.
4. Case Study: Oncology Department
The efficiency of medical staff depends on a number of factors; however, the response time is crucial. According to [35,36,37,40,43], the response time of medical staff directly depends on the configuration of the department and the layout of the rooms. If the rooms for medical staff are positioned centrally in relation to the patient rooms surrounding them, then the path to the farthest patient is the shortest and thus the efficiency is the highest. On the other hand, the distance traveled by medical staff in a rectangular configuration department is longer, and thus as the number of patient rooms increases, the distance that the staff needs to cover increases as well. However, a combination of centralized and rectangular configurations reduces the maximum distance and response time of medical staff by as much as 60%. In addition, the efficiency of medical staff is affected by the existence of a unique system for monitoring the condition of patients. The distribution of work tasks and good cooperation and exchange of information between medical staff also has a positive effect on reducing the overall response time, which results in greater efficiency.
Bearing in mind that IV chemotherapy is inconceivable without the use of IV infusion, an analysis of the medical staff response time (depending on the staff’s gender and age), for a typical oncology department with rectangular configuration was performed. It should be emphasized that oncology patients, due to cytostatics, have a very low number of leukocytes, which causes a decline in the immune system, leaving the body unprotected from many bacteria and viruses, which is why strict control at the entrance of the department is crucial, especially today, due to the COVID-19 pandemic. Although it increases the medical staff response time, the rectangular configuration is of exceptional importance in oncology departments, which implies the use of modern systems for detection and monitoring of IV infusion therapy at a remote location.
Figure 2 shows the rectangular oncology department for the treatment of patients with testicular cancer. The left side of the department comprises (viewed from the bottom up) the nurse room (R-A1), where two nurses work all the time, 24 h a day, with a shift lasting 12 h; cytostatic and other medical supplies room (R-A2); sterile bed linens room (R-A3); hospital staff bathroom (R-A4); doctor’s room (R-A5); head nurse and administration room (R-A6); electrocardiogram (ECG) and other minor diagnostics room (R-A7); and additional medical materials and equipment room (R-A8), such as mobile and stationary devices and instruments, oxygen tanks, IV stands, etc.
The right side of the departments consists of (viewed from the bottom up) a housekeeping room (R-B1); sanitary and disinfection material room (R-B2); and a total of eight patient rooms (PR-1, PR-2, PR-3, PR-4, PR-5, PR-6, PR-7, PR-8), of which the first five are double, and the remaining three have seven beds, allowing the admission of a total of 31 patients. All rooms are intended for inpatient treatment according to PEB or PEI protocol, however, double rooms are most often for patients with extremely weak immunity or those in the terminal phase, which is less common. From the arrangement of beds in the rooms, it can be noticed that the path to each patient is largely straight, allowing easier access to the infusion stand, which, according to [43], has a positive effect on reducing the medical staff response time.
The head nurse is in the department from 7:00 a.m. to 3:00 p.m. every work day, and her role is to plan and manage the organization, as well as to supervise the nurses, technicians, and support staff. Although she is not in charge of constant monitoring and visiting of patients, she does so as needed, or at the invitation of the patient or the nurse on call. Therefore, the head nurse should react if neither of the two nurses in charge of patients responds to alarms in a timely manner. The attending doctors work in shifts—there are more of them in the morning, and at night there is one on duty, with the shift lasting 12 h. Their role is to prescribe therapy on the basis of the patient’s anamnesis and monitor the course of treatment, as well as to react urgently in case of unforeseen circumstances. The cytostatic room contains cytostatics and other medications that all patients should receive that day. This room is not classic storage of cytostatics, but their requirements are performed daily. Every morning, after the visit, the doctor issues an order for IV chemotherapy. On the basis of this, the staff in charge of storing medicaments delivers the necessary cytostatics as soon as possible. After that, the nurses on duty within the cytostatic room prepare premedication and IV bottles in accordance with the prescribed doses for each patient individually. According to the daily schedule, the nurses take the IV bottles to the patient, after which they apply a cannula if it has not already been placed, give appropriate premedication and then place the IV bottle on a stand, activating IV chemotherapy. Upon completion, the nurses return to the nurse room (R-A1).
Experiment and Results
The average medical staff response time in the example of the oncology department from Figure 2 at full capacity when a total of 31 patients receive IV chemotherapy according to PEB or PEI protocol, was determined experimentally. Therefore, the total number of IV bottles to be placed, turned on and off, was 165. In addition, the trajectory of the medical staff from the cytostatic room (R-A2) is shown in Figure 2 in the form of black arrows for each individual patient. Thus, the distance from the cytostatic room to the farthest patient (P4 or P5) was calculated to be 53 m.
Within the experiment, a total of 50 healthy and adult subjects participated, of which 40 (80%) were women (nurses) and 10 (20%) were men (medical technicians) in four age groups: a total of 27 subjects (54%) were from 18 to 25 years old; a total of 8 subjects (16%) were from 25 to 30; a total of 8 subjects (16%) were from 35 to 45 and a total of 7 subjects (14%) were from 45 to 55 years old. All the subjects performed the task of crossing a straight path with a total length of 53 m for two different scenarios—spontaneous and fast walking. Times were measured using a stopwatch.
Table 2 shows the results of the experiment for the female, male, and total sample. In addition, for each age group, depending on the scenario, data for minimum, main, and maximum walking times as well as standard deviation are given.
The first part of the table refers to female subjects representing 80% of the total number of subjects in the experiment. The first age group included a total of 21 subjects (52.5%), the second a total of 7 subjects (17.5%), while the third and fourth groups had a total of 6 subjects (15.0%) each. Therefore, the response time of female subjects during the spontaneous and fast walk was in the intervals of 24.05–35.34 s and 21.69–31.46 s, respectively. The shortest main reaction time was recorded in the first group and the longest in the fourth group. In addition, the major times of all female subjects in the spontaneous and fast walk were 30.61 ± 2.22 s and 25.33 ± 2.04 s, respectively.
The second part of the table refers to male subjects representing 20% of the total number of subjects in the experiment. The first age group includes a total of 6 subjects (52.5%), the second and fourth a total of 1 subject each (10%), while the third group a total of 2 subjects (20%). Therefore, the reaction times of male subjects during spontaneous and fast walking were in the range of 25.24–31.84 s and 20.25–25.64 s, respectively. The shortest main reaction time was recorded in the second group, while the longest was in the fourth group. In addition, the major times of all male subjects at spontaneous and fast walk were 27.95 ± 2.06 s and 22.54 ± 1.91 s, respectively.
The third part of the table refers to all 50 subjects of both sexes. The first age group includes a total of 27 subjects (54%), the second and third a total of 8 subjects (16%) each, while the fourth group a total of 7 subjects (14%). Therefore, the reaction times of all subjects during spontaneous and fast walking were in the intervals of 24.05–35.34 s and 20.25–31.46 s, respectively. The shortest main reaction time was recorded in the first group and the longest in the fourth group. In addition, the main times of all 50 subjects, both in spontaneous and fast walking, were 30.08 ± 2.43 s and 24.77 ± 2.31 s, respectively.
On the basis of the analysis of the results, we conclude that with increasing age, the response time increased in both sexes. In addition, the response time of male subjects was approximately 10% shorter than that of female subjects. It should be noted that the response time also depended on the height and weight of the subject.
Finally, on the basis of the data in Table 2, the average response time of the entire sample of a total of 50 subjects of both sexes was found to be 27.42 s. Accordingly, the response times of the medical staff for each patient individually, according to the paths in Figure 2, were determined by interpolation, as shown in Table 3. The arrangement of the columns in the table is as follows. The first column refers to the number of patient rooms, while the second shows the number of beds in the room. The third column represents the distance from the cytostatic room to the patient. On the basis of this, in the fourth column, the response time of the medical staff for each patient is shown. The fifth column shows the daily number of IV bottles according to the PEB/PEI protocol. The sixth column refers to the minimum number of visual checks of IV bottles during daily IV chemotherapy, which implies one check per placed IV bottle. The seventh and eighth columns show the total response time of the medical staff and the total distance that the medical staff travels per patient during IV chemotherapy per day, respectively. It should be noted that the number of visual controls is not easy to prescribe, having in mind the daily number of IV bottles and the recommended drip times, which differ. In addition, there are no two patients with the same clinical manifestation, which is why patients respond differently to IV chemotherapy and, instead of lasting several hours a day, sometimes the process lasts significantly longer. This largely depends on the condition of the patient’s veins—after several cycles of IV chemotherapy, the patient’s veins become porous and weak, which is why the reactions of the medical staff are much more frequent than during the first cycle.
On the basis of the data from Table 3, we conclude that for the placement, inclusion/exclusion of IV bottles and visual control for the timely and continuous change of bottles, in the example of the oncology department of rectangular configuration with a capacity of 31 patients, in the treatment of patients with testicular cancer according to PEB and PEI protocol, the total daily response time of the medical staff during IV chemotherapy, was approximately 106 min, and the total distance traveled was as much as 12.335 m. However, by using a modern IV infusion system for detection and monitoring of liquid levels in the IV bottle at a remote location, we can minimize visual controls, and thus the total distance traveled by medical staff is shortened by half, and therefore the total response time is halved as well. Then, having in mind that there are two nurses in the department all the time, the total reaction time for one nurse and the total distance traveled were found to be approximately 26.5 min and 3080 m, respectively.
5. Smart IV Infusion Dosing System
Figure 3 shows the proposed smart IV infusion dosing system (SIVIDS) consisting of three essential parts: (i) sensing and computation layer, (ii) communication layer and (iii) user layer. The first layer refers to the detection and signaling of liquid levels in the IV bottle, and consists of input elements such as sensors, buttons, and controllers for signal interpretation, as well as output elements, such as an audible signal (buzzer), flow regulation valve, and a device for displaying the current state of the system (display). The second layer refers to communication by enabling coupling between the first and third layers using a wireless communication module on one side and a wireless router on the other. In addition, the communication layer allows internet access, and thus data from the devices of the other two layers can be stored directly on the cloud server. The third and final layer allows the medical staff to monitor and visually display the infusion reception in real time for each patient individually but also features a visual display of possible alarms at the nurse room (R-A1) for monitoring. It should be noted that all layers are of the modular type, allowing, if necessary, the upgrade and improvement of the entire system, including the replacement or addition of components or the use of another computer or mobile application.
5.1. System Configuration
Figure 4 shows the system for detecting and signaling the liquid level in the infusion bottle—sensing and computation layer. It consists of a pole/stand (1), IV bottle (2), infusion set containing drip chamber (3), roller clamp (4), IV tubing (5), valve (6) with step motor (7) for interruption of liquid flow, and cannula (8), as well as capacitive sensors (9) for detecting the level of liquid in the bottle, color sensors (10) for detecting the color of the liquid in the bottle, microcontroller with wireless communication module (11), motor driver (12), and display (13). Table 4 shows the configuration of the liquid level detection and signaling system in the infusion bottle.
A saline bottle (2) with a volume of 500 mL is placed on a stand (1). The infusion set (3–8) is connected at the opposite end of the bottle. The sensor holders, within which the capacitive sensors (9) for detecting the liquid level are located, are fixed on the outside of the bottle. In addition, the sensor holders are shaped so that they can be easily, quickly, and simply attached to any bottle. It should be noted that the price of this sensor together with the holder is below 5 EUR. At the same time, the connector with the cable for connecting the sensor is always on the infusion stand, enabling a quick and easy connection to a new IV bottle. Moreover, within the stand, a color sensor (10) for detecting different colors of liquid in the IV bottle is attached—the sensor recognizes the color of light using 8 × 8 series of photodiodes containing three different color filters, of which 16 photodiodes have red filters, 16 have green, and 16 have blue, while the remaining 16 photodiodes are without filters. With the appropriate combination of sensor pins, it is possible to detect red, blue, green, and transparent colors. At the end of the infusion hose, just before the cannula connection, a valve (6) for interrupting and regulating the infusion flow is installed. The valve has two connections and is placed inline. The hose coming from the bottle is connected on the one side of the valve, and on the opposite side is at the outlet of the valve is the hose going towards the cannula. The control of the valve is automated using a stepper motor (7) whose operating voltage is 5 V DC, transmission ratio is 1:64 and has 4075 step/rev., as well as through the use of a driver (12). The control of the liquid level detection and signaling system in the IV bottle is enabled by the use of the Arduino Uno microcontroller (11), whose operating voltage is 5 V DC, which has 14 digital pins that can be used as inputs/outputs and 6 analog pins. A visual display of system parameters from the microcontroller is enabled close to the patient, using the LCD (13). To power the microcontroller, we adopted the Phaseo ABL8 12V DC power supply in the testing of the proposed system. Although the Arduino Uno can operate at 6–20 V DC, voltages above 12 V DC can overheat the voltage regulator and damage the board. Moreover, if the voltage is below 7 V DC, a 5 V pin can give less than 5 V and then the board becomes unstable. Due to all this, it is recommended that a voltage of 7–12 V DC be used, and thus we adopted a power supply of 12 V DC. The current output is 2.1 A, and the power supply is 30 W. In real conditions, i.e., in hospitals, due to the mobility of the device, we suggest power supply using batteries. For communication between the microcontroller and remote devices, we used the NodeMcu ESP8266 CP2102 V3 wireless module.
5.2. Operating Principle
Two capacitive sensors (9) are attached to the saline bottle (2), one below the other, enabling the detection of liquid levels in the bottle. The upper sensor detects the MAX fluid level, while the lower detects the MIN 1 and MIN 2 levels. The height of the liquid column in the bottle is 145 mm. Accordingly, the capacitive sensors are positioned to cover a liquid column height of 140 mm, which is 5 mm less than the maximum. Thus, this 5 mm height in the bottle cap zone is approximately 25 mL of saline, which drains from the bottle at maximum flow for approximately 30 s. This time was taken into account when forming the alarm states. The sensors (9) for detecting the level of liquid in the bottle are connected to the microcontroller (11), sending signals about the current level of liquid in the bottle all the time. On the other hand, the color sensor (10) enables the detection of the color of the fluid in the IV bottle, indicating the type of fluid—saline, blood or plasma, or urine if the system is used to collect urine or drain the patient in postoperative days. On the basis of the type and volume of fluid contained in the IV bottle, the condition of the patient’s veins, and the flow of the selected cannula, the medical staff manually adjusts the infusion flow using a roller clamp (4). All the above parameters directly affect the time the bottle empties, i.e., the time of occurrence of the alarm that gives the signal for the emptied IV bottle. If the bottle is completely emptied and the medical staff does not respond to the alarm for any reason, then the stepper motor (7) is activated by closing the valve (6), and thus the return of blood through the cannula to the IV tubing is prevented, which is essential.
Figure 5 shows the algorithm of the smart IV infusion dosing system, which is a combination of a system for detecting and signaling liquid levels in an IV bottle and a web application for monitoring and displaying the state of IV infusion in real time at a remote location. After starting the device, the RESET button must be activated in order to set the system to the initial values. The microcontroller then reads the values from both capacitive sensors and compares them with the predefined ones. De facto, the microcontroller first analyzes the signals from the upper capacitive sensor that sends data for the MAX liquid level in the IV bottle and, if this value does not match the defined value for the MAX level, then the buzzer is activated, and the alarm is displayed. On the other hand, if this value corresponds to the value defined in the microcontroller as the MAX level, then the infusion is enabled and the status of the liquid level in the bottle is displayed. The microcontroller further analyzes the signals from the lower capacitive sensor that sends data for the MIN 1 and MIN 2 levels.
If this sensor detects the liquid level defined as MIN 1, the alarm is activated, but the system continues to work. On the other hand, if the sensor detects the fluid level defined as MIN 2, then there is 5 mL of liquid left in the bottle. The microcontroller then activates a continuous buzzer alarm, showing the alarm condition on the display, and the infusion flow to the patient automatically stops. Finally, it is necessary to replace the empty bottle with a new one, after which the procedure is repeated or the IV administration is terminated if the therapy is over.
5.3. Web Application
A web application for monitoring and displaying the state of IV infusion in real time at a remote location, for PEB and PEI chemotherapy protocol was developed. It is used to simulate the functioning of the automated system for detection and signaling of fluid levels in IV bottle from Figure 4. All patients’ data are located in a centralized database on the cloud server. Thanks to this, client devices (smart mobile phones, computers, tablets, etc.) can access the data by connecting to the server via hypertext transfer protocol (HTTP). However, if the communication between the cloud server and the client is interrupted for any reason, the data is not lost but is still on the server. In addition, it is not necessary to install the application on the client to access the data, but only to enter the internet protocol (IP) address in the browser.
A computer system for monitoring and displaying the current state of the IV infusion for each patient individually is located at the nurse room. The system is started after the doctor’s visit, when an instruction for administering IV chemotherapy is issued and the preparation of cytostatics, accompanying drugs, and other actions such as placing IV bottles on stands near the patient are performed. Upon activation of the application, the representation of the oncology department with buttons showing patient rooms is displayed on the computer screen, as shown in Figure 6a. By selecting the appropriate button/room, a new window opens and new buttons representing patient beds in the room are displayed. The button/patient is then selected to access data on daily IV chemotherapy, as shown in Figure 6b. The left side of the screen displays the information about the selected patient and the type of chemotherapy he is receiving. For the PEB protocol, the IV bottles that the patient should receive are shown in the form of icons with numbers from 1 to 5. After the first IV bottle is emptied, the icon with number 1 turns yellow, and so on. On the right side of the screen, there is a system reset button, a scale that shows the current state of the liquid in the IV bottle and possible alarms. If the internet communication between the server and the client is interrupted, the smart IV infusion dosing system will continue working, regardless. In doing so, the data are stored on the server all the time, and after the establishment of communication, it can be accessed again.
Figure 7 shows the cloud infrastructure related to patient data protection. A multi-layered client/server application consists of a user interface (UI), an application programming interface (API), and a structured query language (SQL) server on which the database is located. The IU is located on the computer at the nurse room, while the API layer allows communication between the UI and the SQL server.
In order to protect the data, it is necessary to set the UI network settings to allow only incoming traffic on port 443 (standard port for hypertext transfer protocol secure (HTTPS) traffic) from the public IP address of the hospital using the virtual private network (VPN) gateway. In addition, it is necessary to include minimum transport layer security (TLS) 1.2 encryption, as well as protection against distributed denial-of-service (DDoS) attack. Moreover, logging in to the web application should only be allowed via two-factor authentication (2FA) using a universal serial bus (USB) token or an official smartphone. The UI communicates with the SQL database via API that receives HTTP GET and POST commands, thus protecting the database from attacks in case someone takes over the UI server. The API communicates with the UI via the REST API call, and with the database via the database (DB) contained user. An additional level of security applies to network API settings. Therefore, the API should only be visible to the UI server by port 443 (HTTPS), and to the database by port 1433 (default port for SQL server). Moreover, the SQL server communicates directly and exclusively with the API service, while indirectly with the binary large object (Blob) storage, which is used to store on-demand DB backups. The SQL server itself is placed in georeplying redundancy with the secondary server at another location. In Serbia, the same general data protection regulation (GDPR) applies as for European Union (EU) countries. Access to the described infrastructure is possible through the cloud service portal, with 2FA also configured. It should be noted that the formation and maintenance of the proposed cloud infrastructure is below 65 EUR per month.
6. Results and Discussion
The system for detection, signaling, and regulation of IV infusion flow was developed on the basis of available components. The use of two capacitive sensors allows for the detection of MAX and MIN liquid levels in a plastic IV bottle but provides no data on the amount of liquid between these two sensors. Therefore, the idea is to use one flexible capacitive sensor along the entire bottle instead of two capacitive sensors, allowing for data on the remaining amount of liquid in the IV bottle, all the time, during the infusion drip. In addition, the flexible capacitive sensor enables the detection of liquids regardless of the material and shape of the IV bottle—plastic or glass. It is also suitable for IV plastic bags or urine bags, regardless of the change in the shape of the bag during emptying and filling, respectively. Detection of liquid levels in an IV bottle would work on the same principle. The use of color sensors for liquid color detection in IV bottles is insufficiently reliable due to signal interference as a consequence of changes in ambient light intensity. In addition, the distance between the sensor and the IV bottle significantly affects the reliability of the sensor. Nevertheless, the use of modern color sensors can be extremely useful for the detection of blood in the urine bags in immobile patients, especially in the postoperative days, enabling a quick reaction of the medical staff, which is crucial. For greater reliability of the entire IV dosing system, we suggest the use of another sensor for detecting liquid levels in the IV bottle—a flow sensor, type SMC PF2D504-11-1, which is acceptable in medicine.
The monitoring and management of the smart IV infusion dosing system is enabled by creating a client and server web application. By placing the database on the cloud server, the storing of data on all patients and their received IV therapies is enabled even when the internet connection between the hardware part of the system, the server, and the client is interrupted. In such a case the hardware part functions independently, and the data are stored in the microcontroller. After establishing an internet connection, the data are sent to the server and the client, independently. On the basis of the data from the cloud server, we can perform various statistical analyses, such as monitoring the success of therapy or the amount of cytostatics and other medications consumed and make daily, weekly, or monthly review of used IV bottles and other equipment. However, it should be noted that patient data protection is extremely important, and that is why the cloud security infrastructure is configured.
A standard industrial valve was used to regulate and stop the flow of IV infusion. However, in order to prevent IV liquid contamination, we recommend the SMC valve from the XT34 series. It should be noted that the regulation of IV infusion flow is of exceptional importance, especially in oncology patients. Depending on the chemotherapy protocol, due to the full effect of the drug, the drip time of only one IV bottle can be prescribed for up to 24 h. Then, continuous dripping of IV infusion, all the time during chemotherapy, is imperative. The manual valve, i.e., roller clamp, which is most often used to regulate the flow of IV infusion, has low reliability and requires constant monitoring and too frequent adjustment of the flow, which is unacceptable. Therefore, on the basis of the defined drip time of the IV infusion (which, for example, the medical staff selects according to the therapy via the display) and the current flow of IV fluid to the patient, the system would automatically regulate the flow to reach the prescribed drip time, which is very important.
The smart IV dosing system requires a constant power supply. However, for mobility it is necessary to install batteries to power the hardware. In this case, the battery capacity to power the proposed system is determined by
where Q (mAh) is battery capacity, E (Wh) is energy stored in the battery, and U (V) is battery voltage. If the system needs to operate for 24 h at the voltage of 9 V DC (max consumption 45 mA), a rechargeable NIMH battery of 3000 (2667) mAh is required.
Q = E/U
The accuracy of the data from the capacitive sensors was tested using an ultrasonic sensor HC-SR04. The ultrasonic sensor was placed on the opposite side of the IV bottle, above the IV liquid. It should be noted that the IV bottle was previously opened because this sensor is not able to detect drops of liquid directly through the drip chamber or the IV bottle. By simultaneously detecting the liquid level in the IV bottle using ultrasound and capacitive sensors, and by comparing the obtained data, we concluded that the capacitive sensors reliably and accurately detect the liquid level in the IV bottle.
Functional test of the liquid detection and signaling system in IV bottle was performed by measuring the time from the moment of activation of the upper capacitive sensor on IV bottle (MAX level) to the moment of infusion expiration (MIN 2 level), and the signal for closing the flow valve. Testing was performed using an IV bottle with 500 mL of saline, with the distance from the bottle to the cannula being L = 1 m (see Figure 1). In addition, for the purposes of this test, the roller clamp was fully open to measure the drip time at maximum IV fluid flow. The cannula that is most often used in IV therapy or blood transfusion was chosen—it is pink for identification and has a flow rate of 65 mL/min [88]. A total of 10 measurements were performed. Table 5 shows the measurement results.
As can be seen from Table 5, the drip time of all 10 IV bottles was in the interval 6.78–7.40 min, while the main time was 7.01 ± 0.15 min. During the sixth and seventh measurements, a short stoppage of the infusion flow was noticed due to the deformation of the IV bottle, but without much influence on the final drip time. If the shortest and longest time is excluded from the analysis, the results are very close, and thus the main time is 6.99 ± 0.05. Therefore, the rate of dripping of liquid from the IV bottle is influenced by the type and diameter of the cannula, the position of the IV bottle in relation to the cannula, the appearance of vacuum in the IV bottle, but also the type of IV liquid—e.g., blood plasma also affects the flow rate; however, the condition of the veins is crucial, especially in oncology patients using cytostatics intravenously. After several months of IV chemotherapy, the patient’s veins are no longer able to withstand daily IV therapy and then become weak and porous. Therefore, during daily IV chemotherapy, it is often necessary to remove the cannula and apply a new one to another vein, often from several attempts. Thinner cannulas are then used—usually blue with a flow rate of 35 mL/min [88]. Therefore, the duration of IV chemotherapy is significantly prolonged, which has negative effects on the full effect of the drug. The proposed smart IV dosing system should help patients and preserve their veins by preventing blood from returning to the IV tubing and clogging the cannula during IV chemotherapy.
Finally, Table 6 presents a comparison of modern IV infusion detection, signaling, and monitoring systems with the system we proposed. The comparison was made on the basis of the presence/absence of the following elements: (i) a system for detecting fluid levels in the IV bottle, (ii) signaling—any type of alarm, (iii) a system for regulating and closing the infusion flow, (iv) monitoring system in patient rooms, (v) remote monitoring system at the nurse room, (vi) database, and (vi) IoT technology.
On the basis of the analysis of the results from Table 6, we conclude that only the SIVIDS system we proposed in this paper has a score of 7/7, representing a comprehensive solution for detection, signaling, regulation, and monitoring of IV infusion at a remote location.
7. Conclusions
The paper presents a smart IV infusion dosing system that enables the detection and signaling of liquid level in an IV bottle. In addition, it allows monitoring and visualization of the IV infusion process in real time from a remote location, such as a nurse room. It also enables automatic regulation and stopping of infusion flow through IV tubing. It consists of three key parts: (i) the sensing and computation layer, (ii) the communication layer, and (iii) the user layer.
The sensing and computation layer encompasses two systems. The first system is used for detecting and signaling the liquid level in the IV bottle. It is based on two capacitive sensors where the upper sensor detects the MAX liquid level in the IV bottle, while the lower detects the MIN 1 and MIN 2 levels. It should be noted that the price of this sensor together with the holder is below 5 EUR. The second system is based on a valve that is used to regulate and close the flow of IV infusion. Its role is to provide the prescribed time of IV therapy drip for the full effect of the drug, as well as to automatically close the flow of fluid through the IV tubing after the dripping of liquid from the IV bottle has stopped, preventing the return of blood and the clogging of the cannula.
The communication layer enables the coupling and exchange of information between the first and third layers using a wireless communication module. In addition, it provides internet access, and thus enables the data from the devices of the other two layers to be stored directly on the cloud server. Moreover, placing the database on the cloud server enables the data on all patients and received IV therapies to be stored. However, if the internet connection is lost, the hardware part of the system functions separately, and thus the data is stored in the microcontroller. After the connection is reestablished, the data are sent to the cloud server and to the client (user layer).
The user layer enables monitoring and visualization of the reception of IV infusion therapy for each patient individually in real time at a remote location. In addition, it allows a visual display of possible alarms in the monitoring room. Client devices, such as smartphones, computers, and tablets, can access the data by connecting to a server over the Internet. However, if communication between the cloud server and the client is interrupted, the data are not lost but are still on the server. In addition, to access the data, it is not necessary to install the application for the client, but only to enter the IP address in the browser.
It should be noted that all the layers are of the modular type, which allows upgrading and improving the entire system by adding or replacing components or using another computer or mobile application. The smart IV infusion dosing system can be used not only for the detection and signaling of saline in the IV bottle/bag but also for the blood and some of its components. In addition, it can be applied to urine bags in immobile patients or drainage bags in postoperative care. It can also be installed in any hospital room, ambulance, or mobile hospital.
Remote control, as an Industry 4.0 technology, is particularly suitable for hospital systems because it allows medical staff to easily, quickly, and wirelessly change some system parameters in real time, manage the process, and access and retrieve patient data placed on the cloud server. However, patient data protection is extremely important. Accordingly, the security cloud infrastructure is configured, and its implementation and monthly maintenance costs below 65 EUR.
By using a modern IV infusion system for detection, signaling, and monitoring of fluid levels in the IV bottle/bag at a remote location, we can minimize visual controls during the IV therapy, and thus the total distance traveled by medical staff is much shorter, which implies greater efficiency and better organization of medical staff. In addition, the system alerts staff to continuous and timely IV bottle changes, which can have positive effects on increasing the success of IV therapy, especially in oncology patients, where IV bottle drip times are strictly prescribed. The prescribed drip time of IV chemotherapy for the full effect of cytostatics should be imperative, which is only possible with the use of modern systems for detection, monitoring, regulation, and closure of IV infusion flow such as the one proposed in this paper. To conclude, the proposed system can overcome a number of problems during the IV therapy, which implies less patient concern and greater efficiency of medical staff with less effort and greater satisfaction.
Finally, we should note that due to the appearance of the COVID-19 virus, it is currently impossible to perform clinical testing of the proposed smart IV infusion dosing system, which will be done in the future in accordance with the legislation of the Republic of Serbia.
8. Patents
The smart intravenous infusion dosing system described in this paper is patent pending.
Author Contributions
Conceptualization, methodology, software, writing—original draft preparation: D.O., M.P., and J.Š.; data curation, validation: M.Č., G.O., and O.I.; supervision, writing—review and editing: S.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
This research has been supported by the Ministry of Education, Science and Technological Development, Government of the Republic of Serbia, through the project “Innovative scientific and artistic research from the FTN activity domain”.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fraunhofer-Gesellschaft: Research News. Safe. IV Therapies in Developing Countries–Reducing Mortality with an Electronically Controlled Infusion Set; Fraunhofer: Munich, Germany, 2020; pp. 1–4. Available online: https://www.fraunhofer.de/en/press/research-news/2020/september/reducing-mortality-with-an-electronically-controlled-infusion-set.html (accessed on 12 November 2020).
- Hindley, G. Infection control in peripheral cannulae. Nurs. Stand. 2004, 18, 37–40. [Google Scholar] [CrossRef]
- Millam, D.A. Managing complications of i.v. therapy (continuing education credit). Nursing 1988, 18, 34–43. [Google Scholar] [CrossRef]
- Ajibola, O.O.E.; Sunday, O.O.; Eyehorua, D.O. Development of automated intravenous blood infusion monitoring system using load cell sensor. J. Appl. Sci. Environ. Manag. 2018, 22, 1557–1561. [Google Scholar] [CrossRef]
- Shelishiyah, R.; Suma, S.; Reji, J.R.M. A system to prevent blood backflow in intravenous infusions. In Proceedings of the 2nd International Conference on Innovations in Information, Embedded and Communication Systems (ICIIECS), Coimbatore, India, 19–20 March 2015; pp. 1–4. [Google Scholar] [CrossRef]
- Bhavasaar, M.K.; Nithya, M.; Praveena, R.; Bhuvaneswari, N.S.; Kalaiselvi, T. Automated intravenous fluid monitoring and alerting system. In Proceedings of the IEEE Technological Innovations in ICT for Agriculture and Rural Development (TIAR), Chennai, India, 15–16 July 2016; pp. 77–80. [Google Scholar] [CrossRef]
- Ramisha, R.K.; Shabana, N.; Tanmayee, P.; Loganathan, S.; Velmathi, G. Smart drip infusion monitoring system for instant alert-through nRF24L01. In Proceedings of the International Conference on Nextgen Electronic Technologies: Silicon to Software (ICNETS2), Chennai, India, 23–25 March 2017; pp. 452–455. [Google Scholar] [CrossRef]
- Cohen, L.; Rose, R.A. Capacitance-Type Fluid Level Sensor for I.V., and Catheter Bags. U.S. Patent No. US5135485, 4 August 1992. [Google Scholar]
- Anand, M.; Pradeep, M.; Manoj, S.; Arockia Raj, L.M.; Thamaraikani, P. Intravenous drip monitoring system. Indo-Iran. J. Sci. Res. 2018, 2, 106–113. [Google Scholar] [CrossRef]
- Pratim, R.P.; Thapa, N. A systematic review on real-time automated measurement of IV fluid level: Status and challenges. Measurement 2018, 129, 343–348. [Google Scholar] [CrossRef]
- Priyadharshini, R.; Mithuna, S.; Vasanth, K.U.; Kalpana, D.S.; Suthanthira, V.N. Automatic intravenous fluid level indication system for hospitals. Int. J. Res. Appl. Sci. Eng. Technol. 2015, 3, 427–432. [Google Scholar]
- Ogawa, H.; Maki, H.; Tsukamoto, S.; Yonezawa, Y.; Amano, H.; Caldwell, W.M. A new drip infusion solution monitoring system with a free-flow detection function. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 1214–1217. [Google Scholar] [CrossRef]
- Makobore, P.N.; Mulerwa, M. An electronically controlled gravity feed infusion set for intravenous fluids. In Biomedical Engineering for Africa; Douglas, T.S., Ed.; University of Cape Town Libraries: Cape Town, South Africa, 2019; pp. 125–138. [Google Scholar] [CrossRef]
- Sayed-Kassem, A.; Kozah, N.; Hajj-Moussa, G.; Harb, R.; Zaylaa, A.J. BMIVPOT, a fully automated version of the intravenous pole: Simulation, design, and evaluation. J. Healthc. Eng. 2020, 2020, 7963497. [Google Scholar] [CrossRef] [PubMed]
- LeFevre, R.J.; Thomas, R.E. Electronically Controlled Intravenous Infusion Set. U.S. Patent No. US4038981, 2 August 1977. [Google Scholar]
- Cheng, T.-Y. Intravenous Drip Monitoring Method and Related Intravenous Drip Monitoring System. U.S. Patent No. US2011/0144595A1, 16 June 2011. [Google Scholar]
- Moorthy, J.; Karunakaran, K.; Senthik, K.S.V. An automated locking system to prevent backflow of blood in an intravenous setup. Glob. J. Res. Eng. 2020, 20, 27–34. [Google Scholar]
- Mulerwa, M.; Makobore, P.; Kagoda, H. Clinician engagement and training on an electronically controlled gravity feed infusion set as a precursor for clinical studies. CMBES Proc. 2019, 42, 1–3. [Google Scholar]
- Makobore, P.N.; Mulerwa, M.; Kagoda, H.; Ocheng, M.; Niyitanga, P.; Wegoye, M.; Muhanguzi, D.; Rutakingirwa, M.; Meya, D. Early feasibility study of an electronically controlled gravity feed infusion set for intravenous fluids in adults. CMBES Proc. 2019, 42, 1–5. [Google Scholar]
- Raghavendra, R.K.; Evangili, S.K. Design and development of IoT based intravenous infusion system. In Emerging Trends in Electrical, Communications, and Information Technologies: ICECIT 2018; Hitendra, S.T., Sankar, V., Shaik, R., Eds.; Springer: Singapore, 2020; Volume 569, pp. 487–499. [Google Scholar] [CrossRef]
- Joseph, S.; Francis, N.; John, A.; Farha, B.; Baby, A. Intravenous drip monitoring system for smart hospital using IoT. In Proceedings of the 2nd International Conference on Intelligent Computing, Instrumentation and Control Technologies (ICICICT), Kannur, Kerala, India, 5–6 July 2019; pp. 835–839. [Google Scholar] [CrossRef]
- Pratim, R.P.; Thapa, N.; Dash, D.; De, D. Novel implementation of IoT based non-invasive sensor system for real-time monitoring of intravenous fluid level for assistive e-healthcare. Circuit World 2019, 3, 109–123. [Google Scholar] [CrossRef]
- Wei, Q.; Lee, J.H.; Seong, K.W.; Kim, M.N.; Cho, J.H. The design of a wireless flexible capacitive sensor detection system to detect liquid level in plastic bag intravenous drip sets. Biomed. Eng. Lett. 2011, 1, 247–253. [Google Scholar] [CrossRef]
- Tseng, W.-H.; Juan, D.; Hsiao, W.-C.; Chan, C.-H.; Wang, K.-C.; Ma, H.-Y.; Lee, H.-Y. Optical design and study of a wireless IV drip detection device. Microelectron. Reliab. 2019, 102, 113325. [Google Scholar] [CrossRef]
- Feng, J.; Miao, X. Method for Determining the Empty State of an IV Bottle in an IV Infusion Monitoring Device. U.S. Patent No. US9752913B2, 5 September 2017. [Google Scholar]
- Binti, R.S.N.; Chin, K.L. The development of intravenous drip detector based on wireless application. In E-Proceedings of the 4th International Conference on Research in TVET Studies (ICOR-TVET), Pamulang, Indonesia, 9 September 2019; Temerloh Community College Press: Mentakab, Pahang, 2019; pp. 188–193. [Google Scholar]
- Dinesh, K.J.R.; Ganesh, B.C.; Soundari, D.V.; Priyadharsini, K.; Karthi, S.P. A novel system design for intravenous infusion system monitoring for betterment of health monitoring system using ML-AI. Int. J. Innov. Technol. Explor. Eng. 2020, 9, 2649–2655. [Google Scholar] [CrossRef]
- Amano, H.; Ogawa, H.; Maki, H.; Tsukamoto, S.; Yonezawa, Y.; Caldwell, W.M. A remote drip infusion monitoring system employing Bluetooth. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 2029–2032. [Google Scholar] [CrossRef]
- Feng, J.; Miao, X. IV Infusion Monitoring Device. U.S. Patent No. US2011/0205074A1, 25 August 2011. [Google Scholar]
- Yang, C.W. Intravenous Drip Real-Time Monitoring System and Method. U.S. Patent No. US2019/0365994A1, 5 December 2019. [Google Scholar]
- Unluturk, M.S.; Ozcanhan, M.H.; Dalkilic, G. Improving communication among nurses and patients. Comput. Meth. Prog. Bio. 2015, 120, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Rghioui, A.; Lloret, J.; Parra, L.; Sendra, S.; Oumnad, A. Glucose data classification for diabetic patient monitoring. Appl. Sci. 2019, 9, 4459. [Google Scholar] [CrossRef] [Green Version]
- Jung, W.-K.; Park, Y.-C.; Lee, J.-W.; Suh, E.S. Remote sensing of sewing work levels using a power monitoring system. Appl. Sci. 2020, 10, 3104. [Google Scholar] [CrossRef]
- Lee, H.-W.; Lee, K.-O.; Kang, I.-A.; Kye, J.-E.; Park, Y.-Y. Design of a generic wearable-robot monitoring system (GWRMS) for patients with lower limb paralysis. Appl. Sci. 2020, 10, 5566. [Google Scholar] [CrossRef]
- Yi, L.; Seo, H.-B. The effect of hospital unit layout on nurse walking behavior. HERD-Health Env. Res. 2012, 6, 66–82. [Google Scholar] [CrossRef]
- Shepley, M.M.; Davies, K. Nursing unit configuration and its relationship to noise and nurse walking behavior: An AIDS/HIV unit case study. AIA Academy J. 2013, 6, 12–14. [Google Scholar]
- Chiang, Y. Design Dilemma: Nurses’ Stations; Cornell University: Ithaca, NY, USA, 2010; pp. 1–32. Available online: https://www.iwsp.human.cornell.edu/files/2013/09/Nurses-stations-qr3u4x.pdf (accessed on 12 November 2020).
- Adams, R. Nursing Unit Design: Staff Interaction and Communication Patterns; Cornell University: Ithaca, NY, USA, 2013; pp. 1–30. Available online: https://www.iwsp.human.cornell.edu/files/2013/09/Nursing-Unit-Design-Staff-Interac-tion-Com-munication-patterns-u8f0lw.pdf (accessed on 12 November 2020).
- Lee, J.; Lee, H.; Shepley, M.M. Exploring the spatial arrangement of patient rooms for minimum nurse travel in hospital nursing units in Korea. Front. Archit. Res. 2020, 9, 711–725. [Google Scholar] [CrossRef]
- Ullah, U.; Park, J.S. A comparative analysis of patient visibility, spatial configuration and nurse walking distance in Korean intensive care units (ICUs)–focused on single corridor, pod and composite type units. J. Korea Inst. Health Archit. 2016, 22, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Real, K.; Bardach, S.H.; Bardach, D.R. The role of the built environment: How decentralized nurse stations shape communication, patient care processes, and patient outcomes. Health Commun. 2017, 32, 1557–1570. [Google Scholar] [CrossRef] [PubMed]
- Devos, P.; Aletta, F.; Thomas, P.; Vander Mynsbrugge, T.; Petrovic, M.; Van de Velde, D.; De Vriendt, P.; Botteldooren, D. Application of a prediction model for ambient noise levels and acoustical capacity for living rooms in nursing homes hosting older people with dementia. Appl. Sci. 2020, 10, 4205. [Google Scholar] [CrossRef]
- Seo, H.-B.; Choi, Y.-S.; Zimring, C. Impact of hospital unit design for patient-centered care on nurses’ behavior. Environ. Behav. 2011, 43, 443–468. [Google Scholar] [CrossRef]
- Sedgwick, M.; Awosoga, O.; Grigg, L. A pilot study exploring the relationship between the use of mobile technologies, walking distance, and clinical decision making among rural hospital nurses. Health Inform. J. 2019, 25, 1163–1169. [Google Scholar] [CrossRef]
- Mutiarasari, D.; Miranti, M.; Puspasari, K.D.I. Response times and patient satisfaction in emergency room at Anutapura General Hospital, city of Palu. J. Curr. Med. Res. Opin. 2019, 2, 152–157. [Google Scholar] [CrossRef]
- Voepel-Lewis, T.; Parker, M.L.; Burke, C.N.; Hemberg, J.; Perlin, L.; Kai, S.; Ramachandran, S.K. Pulse oximetry desaturation alarms on a general postoperative adult unit: A prospective observational study of nurse response time. Int. J. Nurs. Stud. 2013, 50, 1351–1358. [Google Scholar] [CrossRef]
- Ali, H.; Li, H. Use of notification and communication technology (call light systems) in nursing homes: Observational study. J. Med. Internet Res. 2020, 22, e16252. [Google Scholar] [CrossRef]
- Ali, H.; Cole, A.; Sienkiewicz, A.; Ho, T. Perspectives of nursing homes staff on the nature of residents-initiated call lights. SAGE Open Nurs. 2020, 6, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Bonafide, C.P.; Lin, R.; Zander, M.; Graham, C.S.; Paine, C.W.; Rock, W.; Rich, A.; Roberts, K.E.; Fortino, M.; Nadkarni, V.M.; et al. Association between exposure to nonactionable physiologic monitor alarms and response time in a children’s hospital. J. Hosp. Med. 2015, 10, 345–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martasari, Y.; Zakiyah, A.; Santoso, W. The differences of patient’s families perceptions with BPJS insurance and general about response time nurse’s based on triage in the emergency room. Int. J. Nurs. Midwifery Sci. 2020, 4, 22–28. [Google Scholar] [CrossRef]
- Chapman, C.B. Improving communication among nurses, patients, and physicians. Am. J. Nurs. 2009, 109, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Doyle, G.R.; McCutcheon, J.A. Intravenous therapy. In Clinical Procedures for Safer Patient Care; BCcampus: Victoria, BC, Canada, 2015; pp. 463–542. [Google Scholar]
- Worldometers. Available online: https://www.worldometers.info/coronavirus/ (accessed on 12 November 2020).
- Ritchie, H.; Roser, M. Causes of Death. Available online: https://ourworldindata.org/causes-of-death (accessed on 12 November 2020).
- GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Cheng, L.; Albers, P.; Berney, D.M.; Feldman, D.R.; Daugaard, G.; Gilligan, T.; Looijenga, L.H.J. Testicular cancer. Nat. Rev. Dis. Primers 2018, 4, 1–24. [Google Scholar] [CrossRef]
- De Toni, L.; Šabovic, I.; Cosci, I.; Ghezzi, M.; Foresta, C.; Garolla, A. Testicular cancer: Genes, environment, hormones. Front. Endocrinol. 2019, 10, 408. [Google Scholar] [CrossRef]
- Baird, D.C.; Meyers, G.J.; Hu, J.S. Testicular cancer: Diagnosis and treatment. Am. Fam. Physician 2018, 97, 261–268. [Google Scholar]
- Kudjawu, Y.C.; de Maria, F.; Beltzer, N. Trends in rates of inpatients treated for testicular cancer in France, 2000–2014. Andrology 2018, 6, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Huyghe, E.; Matsuda, T.; Thonneau, P. Increasing incidence of testicular cancer worldwide: A review. J. Urol. 2003, 170, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Garner, M.J.; Turner, M.C.; Ghadirian, P.; Krewski, D. Epidemiology of testicular cancer: An overview. Int. J. Cancer 2005, 116, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Pearce, N.; Sheppard, R.A.; Howard, J.K.; Fraser, J.; Lilley, B.M. Time trends and occupational differences in cancer of the testis in New Zealand. Cancer 1987, 59, 1677–1682. [Google Scholar] [CrossRef]
- Wanderås, E.H.; Tretli, S.; Fosså, S.D. Trends in incidence of testicular cancer in Norway 1955–1992. Eur. J. Cancer 1995, 31A, 2044–2048. [Google Scholar] [CrossRef]
- Weir, H.K.; Marrett, L.D.; Moravan, V. Trends in the incidence of testicular germ cell cancer in Ontario by histologic subgroup, 1964–1996. Can. Med. Assoc. J. 1999, 160, 201–205. [Google Scholar]
- Møller, H. Trends in incidence of testicular cancer and prostate cancer in Denmark. Hum. Reprod. 2001, 16, 1007–1011. [Google Scholar] [CrossRef] [Green Version]
- Toledano, M.B.; Jarup, L.; Best, N.; Wakefield, J.; Elliott, P. Spatial variation and temporal trends of testicular cancer in Great Britain. Br. J. Cancer 2001, 84, 1482–1487. [Google Scholar] [CrossRef] [Green Version]
- Beri, A.; Matzkin, H.; Liphshitz, I.; Barchana, M. Epidemiological characteristics and trends of testicular cancer in Israel 1992–2002. Harefuah 2007, 146, 515–519. [Google Scholar]
- Dusek, L.; Abrahamova, J.; Lakomy, R.; Vyzula, R.; Koptikova, J.; Pavlik, T.; Muzik, J.; Klimes, D. Multivariate analysis of risk factors for testicular cancer: A hospital-based case-control study in the Czech Republic. Neoplasma 2008, 55, 356–368. [Google Scholar]
- Baade, P.; Carrière, P.; Fritschi, L. Trends in testicular germ cell cancer incidence in Australia. Cancer Causes Control 2008, 19, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Sincic, N.; Kulis, T.; Znaor, A.; Bray, F. Time trends in testicular cancer in Croatia 1983–2007: Rapid increases in incidence, no declines in mortality. Cancer Epidemiol. 2012, 36, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Ghazarian, A.A.; Trabert, B.; Devesa, S.S.; McGlynn, K.A. Recent trends in the incidence of testicular germ cell tumors in the United States. Andrology 2015, 3, 13–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandt, M.P.; Gust, K.M.; Bon, D.; Tsaur, I.; Thomas, C.; Neisius, A.; Haferkamp, A.; Herrmann, E.; Bartsch, G. Trend analysis and regional tumor incidence in Germany for testicular cancer between 2003 and 2014. Andrology 2019, 7, 408–414. [Google Scholar] [CrossRef]
- Schaffar, R.; Pant, S.; Bouchardy, C.; Schubert, H.; Rapiti, E. Testicular cancer in Geneva, Switzerland, 1970–2012: Incidence trends, survival and risk of second cancer. BMC Urol. 2019, 19, 64. [Google Scholar] [CrossRef]
- Rosen, A.; Jayram, G.; Drazer, M.; Eggener, S.E. Global trends in testicular cancer incidence and mortality. Eur. Urol. 2011, 60, 374–379. [Google Scholar] [CrossRef]
- Kalan, F.K.H.; Mahdavifar, N.; Mohammadian-Hafshejani, A.; Salehiniya, H. Testicular cancer in the world: An epidemiological review. WCRJ 2018, 5, e1180-1–e1180-5. [Google Scholar]
- Gurney, J.K.; Florio, A.A.; Znaor, A.; Ferlay, J.; Laversanne, M.; Sarfati, D.; Bray, F.; McGlynn, K.A. International trends in the incidence of testicular cancer: Lessons from 35 years and 41 countries. Eur. Urol. 2019, 76, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Znaor, A.; Skakkebaek, N.E.; Rajpert-De Meyts, E.; Laversanne, M.; Kuliš, T.; Gurney, J.; Sarfati, D.; McGlynn, K.A.; Bray, F. Testicular cancer incidence predictions in Europe 2010-2035: A rising burden despite population ageing. Int. J. Cancer 2020, 147, 820–828. [Google Scholar] [CrossRef]
- Hanna, N.H.; Einhorn, L.H. Testicular cancer–discoveries and updates. N. Engl. J. Med. 2014, 371, 2005–2016. [Google Scholar] [CrossRef] [Green Version]
- Albers, P.; Albrecht, W.; Algaba, F.; Bokemeyer, C.; Cohn-Cedermark, G.; Fizazi, K.; Horwich, A.; Laguna, M.P.; Nicolai, N.; Oldenburg, J. EAU guidelines on testicular cancer: 2015 update. Eur. Urol. 2015, 68, 1054–1068. [Google Scholar] [CrossRef] [PubMed]
- Albers, P.; Albrecht, W.; Algaba, F.; Bokemeyer, C.; Cohn-Cedermark, G.; Fizazi, K.; Horwich, A.; Laguna, M.P. EAU guidelines on testicular cancer: 2011 update. Eur. Urol. 2011, 60, 304–319. [Google Scholar] [CrossRef] [PubMed]
- Travis, L.B.; Beard, C.; Allan, J.M.; Dahl, A.A.; Feldman, D.R.; Oldenburg, J.; Daugaard, G.; Kelly, J.L.; Dolan, M.E.; Hannigan, R.; et al. Testicular cancer survivorship: Research strategies and recommendations. J. Natl. Cancer Inst. 2010, 102, 1114–1130. [Google Scholar] [CrossRef] [PubMed]
- Krege, S. PEB beim hodentumor [PEB treatment of testicular cancer]. Aktuelle Urol. 2012, 43, 342–345. [Google Scholar] [CrossRef] [PubMed]
- Cullen, M.H.; Stenning, S.P.; Parkinson, M.C.; Fossa, S.D.; Kaye, S.B.; Horwich, A.H.; Harland, S.J.; Williams, M.V.; Jakes, R. Short-course adjuvant chemotherapy in high-risk stage I nonseminomatous germ cell tumors of the testis: A Medical Research Council report. J. Clin. Oncol. 1996, 14, 1106–1113. [Google Scholar] [CrossRef] [PubMed]
- Loehrer, P.J., Sr.; Lauer, R.; Roth, B.J.; Williams, S.D.; Kalasinski, L.A.; Einhorn, L.H. Salvage therapy in recurrent germ cell cancer: Ifosfamide and cisplatin plus either vinblastine or etoposide. Ann. Intern. Med. 1988, 109, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Braun, B. Healthcare Company. Available online: https://www.bbraun.com/content/dam/catalog/bbraun/bbraunProductCatalog/S/AEM2015/en-01/b9/patient-access-ininfusiontherapy.pdf (accessed on 12 November 2020).
Figure 1.
Traditional intravenous (IV) infusion therapy set: 1—pole/stand, 2—IV bottle/bag, 3—spike, 4—air valve, 5—drip chamber, 6—piggyback port, 7—IV tubing, 8—roller clamp, and 9—cannula.
Figure 1.
Traditional intravenous (IV) infusion therapy set: 1—pole/stand, 2—IV bottle/bag, 3—spike, 4—air valve, 5—drip chamber, 6—piggyback port, 7—IV tubing, 8—roller clamp, and 9—cannula.

Figure 2.
An example of an oncology department: room for nurses (R-A1), room for cytostatics preparation and other medical supplies (R-A2), room for clean linen (R-A3), bathroom for hospital staff (R-A4), room for doctors (R-A5), room for head nurse (R-A6), room for ECG and other minor diagnostics (R-A7), room for medical equipment including mobile and stationary devices and instruments (R-A8), room for housekeeping staff (R-B1), room with material for hospital cleaning and disinfection (R-B2), rooms for patients with two beds each in which there are isolated or immobile patients (PR-1, PR-2, PR-3, PR-4, PR-5), and rooms for patients with seven beds each in which there are mobile patients (PR-6, PR-7, PR-8).
Figure 2.
An example of an oncology department: room for nurses (R-A1), room for cytostatics preparation and other medical supplies (R-A2), room for clean linen (R-A3), bathroom for hospital staff (R-A4), room for doctors (R-A5), room for head nurse (R-A6), room for ECG and other minor diagnostics (R-A7), room for medical equipment including mobile and stationary devices and instruments (R-A8), room for housekeeping staff (R-B1), room with material for hospital cleaning and disinfection (R-B2), rooms for patients with two beds each in which there are isolated or immobile patients (PR-1, PR-2, PR-3, PR-4, PR-5), and rooms for patients with seven beds each in which there are mobile patients (PR-6, PR-7, PR-8).

Figure 3.
Smart IV infusion dosing system layers.

Figure 4.
IV infusion dosing system.

Figure 5.
Smart IV infusion dosing system algorithm.

Figure 6.
Web application: (a) home screen layout; (b) screen layout for the selected patient.

Figure 7.
Cloud infrastructure: 1—https; 2—https, representational state transfer (REST) application programming interface (API); 3—EF connection; 4—SQL query; 5—backup database (DB).
Figure 7.
Cloud infrastructure: 1—https; 2—https, representational state transfer (REST) application programming interface (API); 3—EF connection; 4—SQL query; 5—backup database (DB).


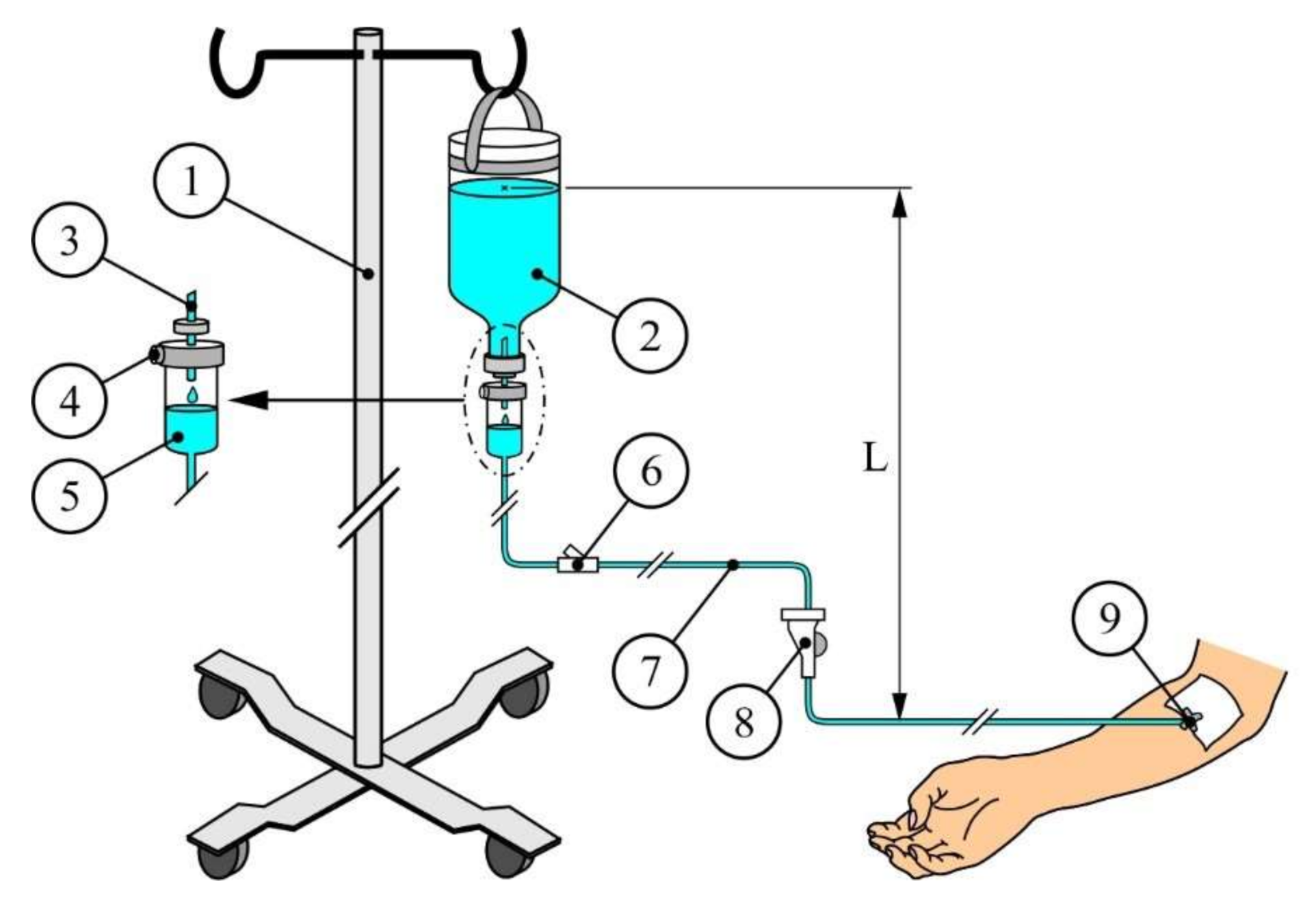{kind=link}
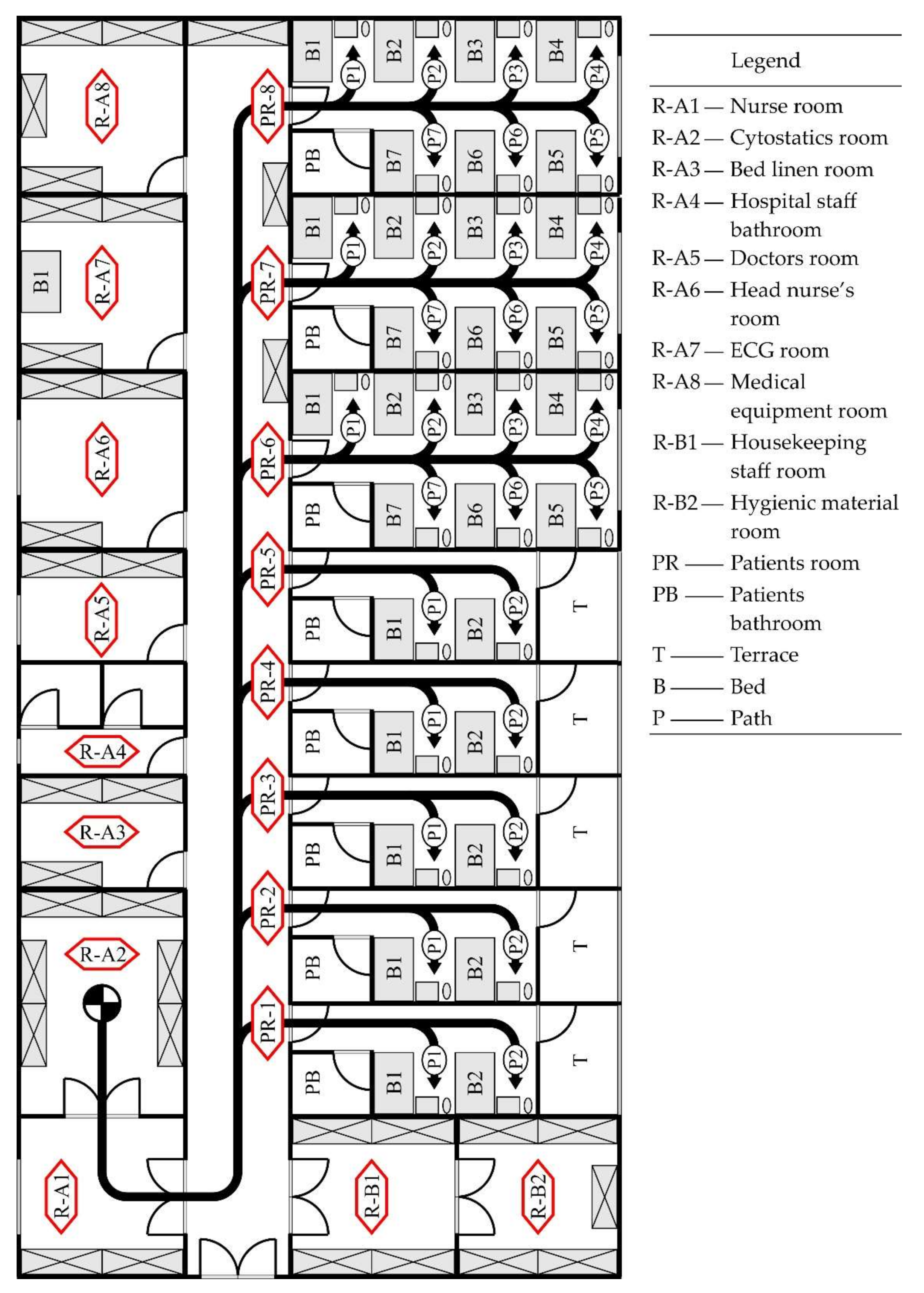{kind=link}
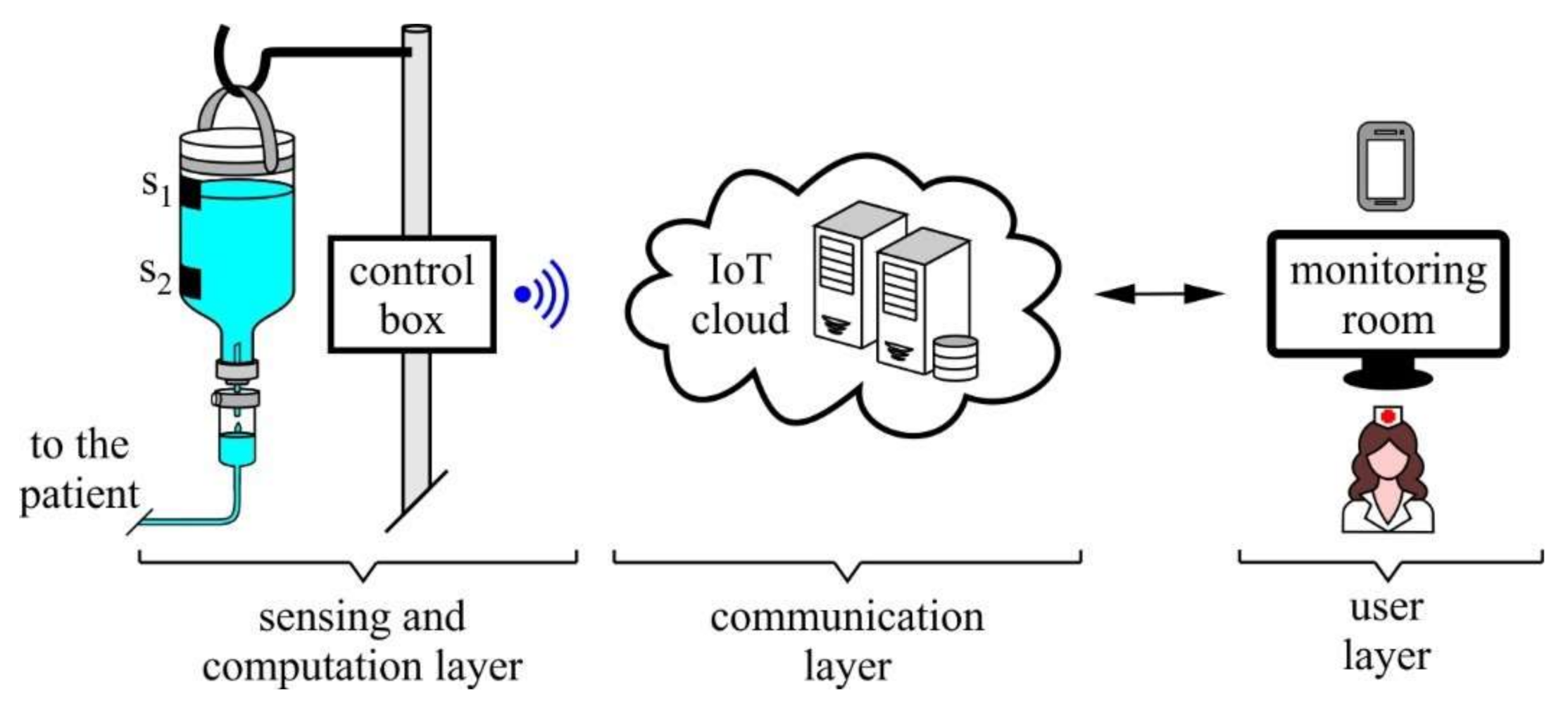{kind=link}
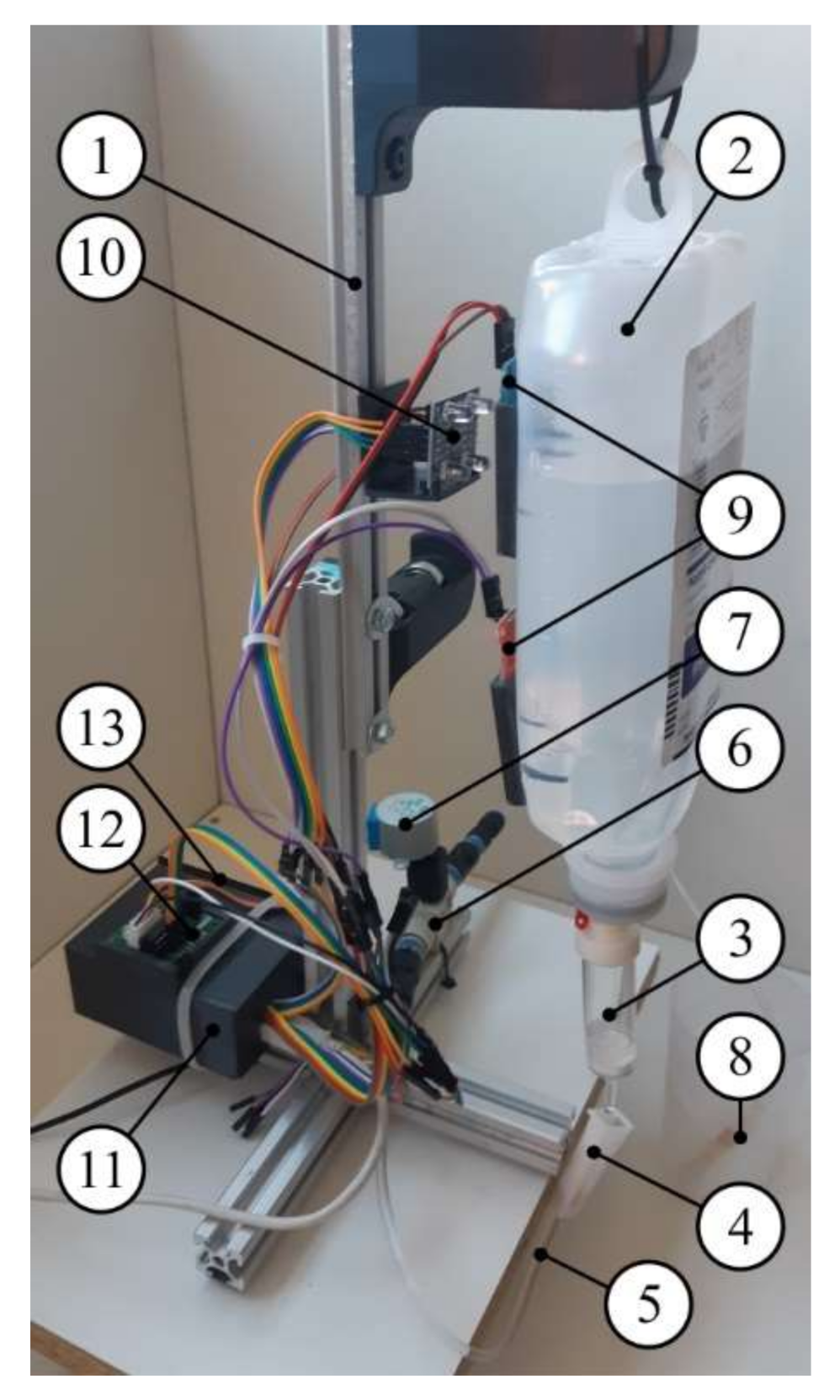{kind=link}
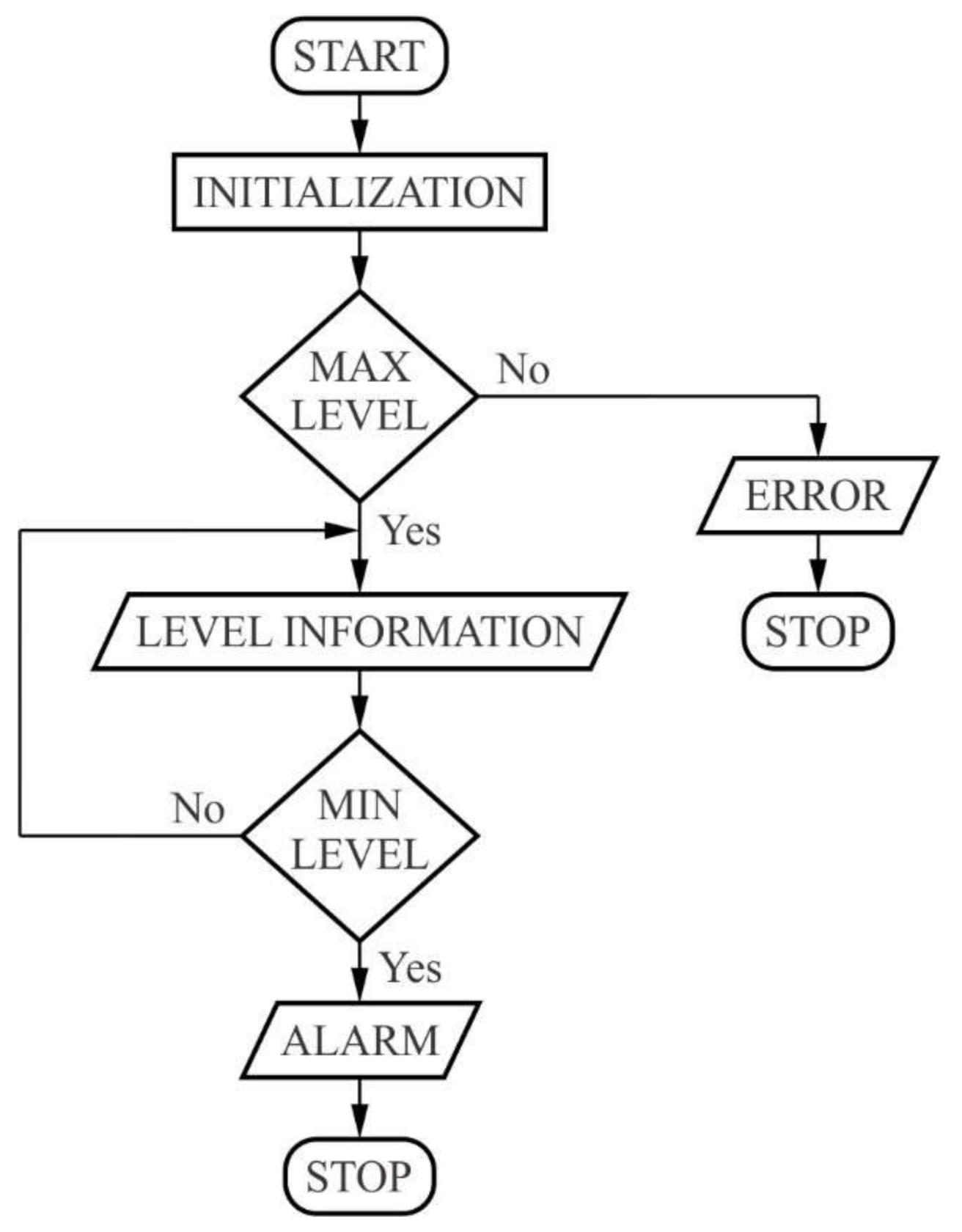{kind=link}
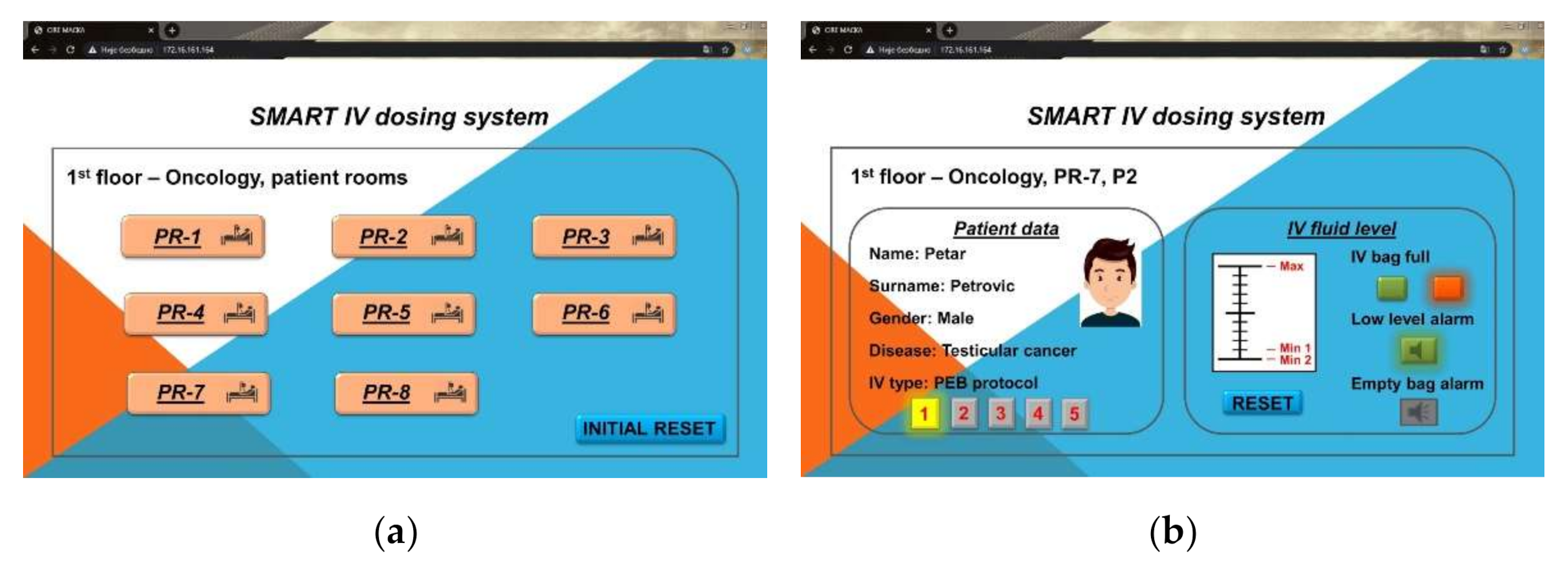{kind=link}
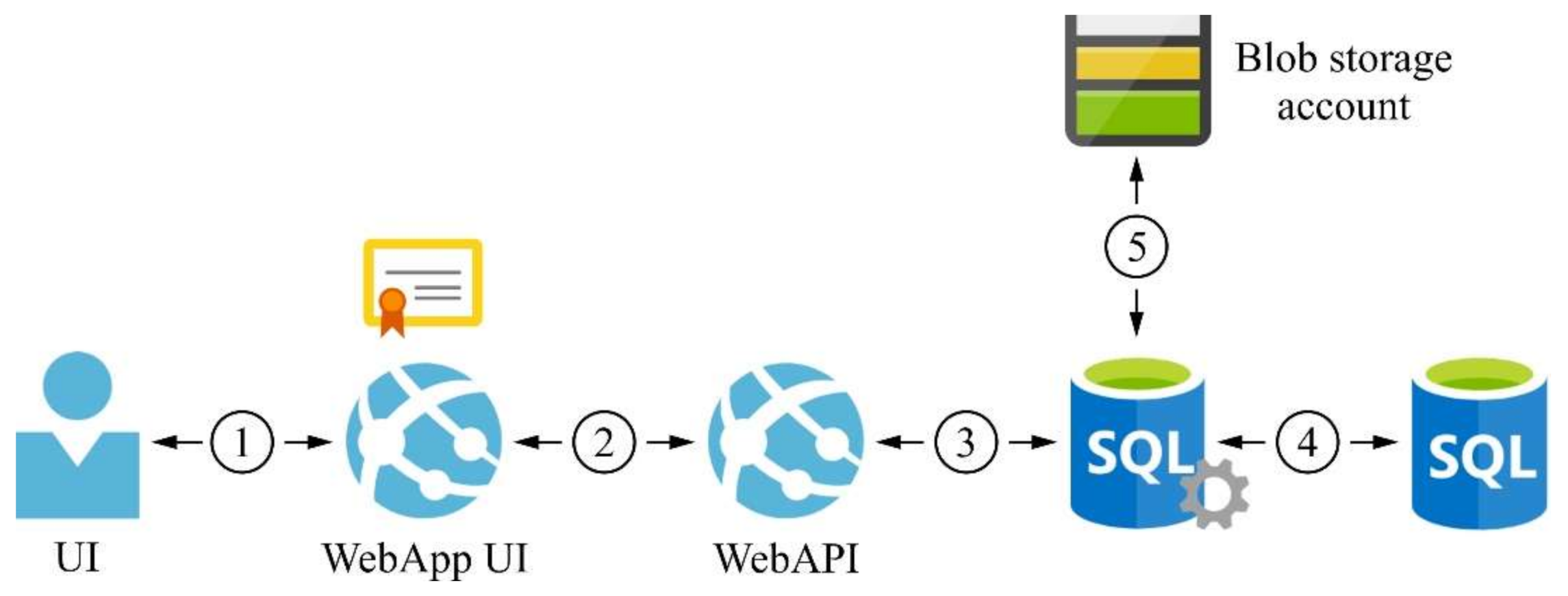{kind=link}
Table 1.
Daily IV chemotherapy in the treatment of testicular cancer according to cisplatin/etoposide/bleomycin (PEB) and cisplatin/etoposide/ifosfamide (PEI) protocols: order of receiving IV bottles and recommended drip times (RDT) of infusion for each IV bottle.
Table 1.
Daily IV chemotherapy in the treatment of testicular cancer according to cisplatin/etoposide/bleomycin (PEB) and cisplatin/etoposide/ifosfamide (PEI) protocols: order of receiving IV bottles and recommended drip times (RDT) of infusion for each IV bottle.
| Protocol | IV Bottle 500 (mL) | IV Bottle Label | Cytostatic | RDT (min) | Total RDT (min) |
|---|---|---|---|---|---|
| PEB (5 bottles) | 1st | Glucosi infundibile 5% or Natrii chloridi infundibile 0.9% | Etoposide | 45–60 | 195–220 |
| 2nd | Natrii chloridi infundibile 0.9% | Cisplatin | 120 | ||
| 3rd | Manitol HF 10% | / | 10 | ||
| 4th | Natrii chloridi infundibile 0.9% | / | 10–15 | ||
| 5th | / | 10–15 | |||
| PEI (5 bottles) | 1st | Natrii chloridi infundibile 0.9% | Cisplatin | 120 | 245–270 |
| 2nd | Glucosi infundibile 5% or Natrii chloridi infundibile 0.9% | Etoposide | 45–60 | ||
| 3rd | Natrii chloridi infundibile 0.9% | Ifosfamide | 60 | ||
| 4th | / | 10–15 | |||
| 5th | / | 10–15 |
Table 2.
Response time of medical staff depending on gender and age group.
| Gender | Group | Age (Years) | No. (%) | Spontaneous Walking Time (s) | Fast Walking Time (s) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| min | main | max | SD | min | main | max | SD | ||||
| Female | I | 18–25 | 21 (52.5) | 28.28 | 30.24 | 33.89 | 1.60 | 21.69 | 24.45 | 27.50 | 1.45 |
| II | 25–35 | 7 (17.5) | 24.05 | 29.76 | 32.25 | 2.68 | 22.55 | 25.90 | 31.46 | 2.60 | |
| III | 35–45 | 6 (15.0) | 27.19 | 31.70 | 34.06 | 2.57 | 22.66 | 25.47 | 27.39 | 1.80 | |
| IV | 45–55 | 6 (15.0) | 29.05 | 31.77 | 35.34 | 2.27 | 26.05 | 27.60 | 29.14 | 1.05 | |
| Total | 40 (100) | 24.05 | 30.61 | 35.34 | 2.22 | 21.69 | 25.33 | 31.46 | 2.04 | ||
| Male | I | 18–25 | 6 (60.0) | 25.72 | 28.08 | 30.76 | 1.72 | 20.62 | 22.39 | 24.01 | 1.40 |
| II | 25–35 | 1 (10.0) | 26.81 | 26.81 | 26.81 | 0 | 20.36 | 20.36 | 20.36 | 0 | |
| III | 35–45 | 2 (20.0) | 25.24 | 26.20 | 27.16 | 0.96 | 20.25 | 22.94 | 25.64 | 2.70 | |
| IV | 45–55 | 1 (10.0) | 31.84 | 31.84 | 31.84 | 0 | 24.79 | 24.79 | 24.79 | 0 | |
| Total | 10 (100) | 25.24 | 27.95 | 31.84 | 2.06 | 20.25 | 22.54 | 25.64 | 1.91 | ||
| Female + Male | I | 18–25 | 27 (54.0) | 25.72 | 29.76 | 33.89 | 1.86 | 20.62 | 23.99 | 27.50 | 1.67 |
| II | 25–35 | 8 (16.0) | 24.05 | 29.39 | 32.25 | 2.69 | 20.36 | 25.21 | 31.46 | 3.05 | |
| III | 35–45 | 8 (16.0) | 25.24 | 30.33 | 34.06 | 3.30 | 20.25 | 24.84 | 27.39 | 2.33 | |
| IV | 45–55 | 7 (14.0) | 29.05 | 31.78 | 35.34 | 2.10 | 24.79 | 27.20 | 29.14 | 1.38 | |
| Total | 50 (100) | 24.05 | 30.08 | 35.34 | 2.43 | 20.25 | 24.77 | 31.46 | 2.31 | ||
Table 3.
Nurse response time (NRT).
| Room | Patient | Distance (m) | NRT (s) | IV Bottles | Visual Control | Total Time 1 (s) | Total Distance 2 (m) |
|---|---|---|---|---|---|---|---|
| PR-1 | P1 | 21 | 10.87 | 5 | 5 | 108.70 | 210 |
| P2 | 23 | 11.90 | 5 | 5 | 119.00 | 230 | |
| PR-2 | P1 | 24.5 | 12.68 | 5 | 5 | 126.80 | 245 |
| P2 | 26.5 | 13.71 | 5 | 5 | 137.10 | 265 | |
| PR-3 | P1 | 28 | 14.49 | 5 | 5 | 144.90 | 280 |
| P2 | 30 | 15.52 | 5 | 5 | 155.20 | 300 | |
| PR-4 | P1 | 31.5 | 16.30 | 5 | 5 | 163.00 | 315 |
| P2 | 33.5 | 17.33 | 5 | 5 | 173.30 | 335 | |
| PR-5 | P1 | 35 | 18.11 | 5 | 5 | 181.10 | 350 |
| P2 | 37 | 19.14 | 5 | 5 | 191.40 | 370 | |
| PR-6 | P1 | 36 | 18.63 | 5 | 5 | 186.30 | 360 |
| P2 | 38 | 19.66 | 5 | 5 | 196.60 | 380 | |
| P3 | 40 | 20.70 | 5 | 5 | 207.00 | 400 | |
| P4 | 42 | 21.73 | 5 | 5 | 217.30 | 420 | |
| P5 | 42 | 21.73 | 5 | 5 | 217.30 | 420 | |
| P6 | 40 | 20.70 | 5 | 5 | 207.00 | 400 | |
| P7 | 38 | 19.66 | 5 | 5 | 196.60 | 380 | |
| PR-7 | P1 | 41.5 | 21.47 | 5 | 5 | 214.70 | 415 |
| P2 | 43.5 | 22.51 | 5 | 5 | 225.10 | 435 | |
| P3 | 45.5 | 23.54 | 5 | 5 | 235.40 | 455 | |
| P4 | 47.5 | 24.58 | 5 | 5 | 245.80 | 475 | |
| P5 | 47.5 | 24.58 | 5 | 5 | 245.80 | 475 | |
| P6 | 45.5 | 23.54 | 5 | 5 | 235.40 | 455 | |
| P7 | 43.5 | 22.51 | 5 | 5 | 225.10 | 435 | |
| PR-8 | P1 | 47 | 24.32 | 5 | 5 | 243.20 | 470 |
| P2 | 49 | 25.35 | 5 | 5 | 253.50 | 490 | |
| P3 | 51 | 26.39 | 5 | 5 | 263.90 | 510 | |
| P4 | 53 | 27.42 | 5 | 5 | 274.20 | 530 | |
| P5 | 53 | 27.42 | 5 | 5 | 274.20 | 530 | |
| P6 | 51 | 26.39 | 5 | 5 | 263.90 | 510 | |
| P7 | 49 | 25.35 | 5 | 5 | 253.50 | 490 | |
| Sum 3 | 31 | 1233.5 | 638.23 | 155 | 155 | 6382.30 | 12335 |
1 Total time is the product of NRT and the total number of connections/disconnections of IV bottles together with visual controls; 2 total distance is the product of the distance and the total number of connections/disconnections of IV bottles together with visual controls; 3 sum refers to columns only and represents statistics.
Table 4.
IV infusion dosing system configuration.
| No. | Part |
|---|---|
| 1 | pole/stand |
| 2 | saline bottle |
| 3 | drip chamber |
| 4 | roller clamp |
| 5 | IV tubing |
| 6 | valve VHK2–08f–08f |
| 7 | stepper motor 28BYJ–48 |
| 8 | cannula |
| 9 | capacitive levelsensor for Arduino |
| 10 | color sensor TCS230 |
| 11 | microcontroller Arduino Uno and Wi-Fi module NodeMcu ESP8266 |
| 12 | motor driver 2PH64011A |
| 13 | display LCD 12864 |
Table 5.
Drip time of 500 mL IV saline bottle using smart IV dosing system.
| No. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Time (min) | 6.90 | 6.78 | 6.93 | 6.96 | 7.03 | 7.40 | 7.10 | 6.98 | 7.02 | 7.03 |
Table 6.
Comparison of modern detection, signaling, and monitoring IV infusion systems.
| System | IV Liquid Level Detection | Alarms | Regulation or On/Off Valve | Monitoring (At the Patient) | Remote Monitoring | Database | IoT | Score |
|---|---|---|---|---|---|---|---|---|
| [10] | yes | yes | no | yes | no | no | no | 3/7 |
| [17] | yes | no | yes | yes | no | no | no | 3/7 |
| [19] | yes | yes | no | yes | yes | no | no | 4/7 |
| [23] | yes | yes | no | no | yes | yes | yes | 5/7 |
| [27] | yes | yes | no | no | yes | no | no | 3/7 |
| [29] | yes | yes | no | no | yes | yes | no | 4/7 |
| [31] | yes | yes | no | no | yes | no | yes | 4/7 |
| SIVIDS | yes | yes | yes | yes | yes | yes | yes | 7/7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Oros, D.; Penčić, M.; Šulc, J.; Čavić, M.; Stankovski, S.; Ostojić, G.; Ivanov, O. Smart Intravenous Infusion Dosing System. Appl. Sci. 2021, 11, 513. https://doi.org/10.3390/app11020513
AMA Style
Oros D, Penčić M, Šulc J, Čavić M, Stankovski S, Ostojić G, Ivanov O. Smart Intravenous Infusion Dosing System. Applied Sciences. 2021; 11(2):513. https://doi.org/10.3390/app11020513
Chicago/Turabian StyleOros, Dragana, Marko Penčić, Jovan Šulc, Maja Čavić, Stevan Stankovski, Gordana Ostojić, and Olivera Ivanov. 2021. "Smart Intravenous Infusion Dosing System" Applied Sciences 11, no. 2: 513. https://doi.org/10.3390/app11020513
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.