The Delayed Neuroprotective Effect of Methylene Blue in Experimental Rat Brain Trauma

 , and
, and 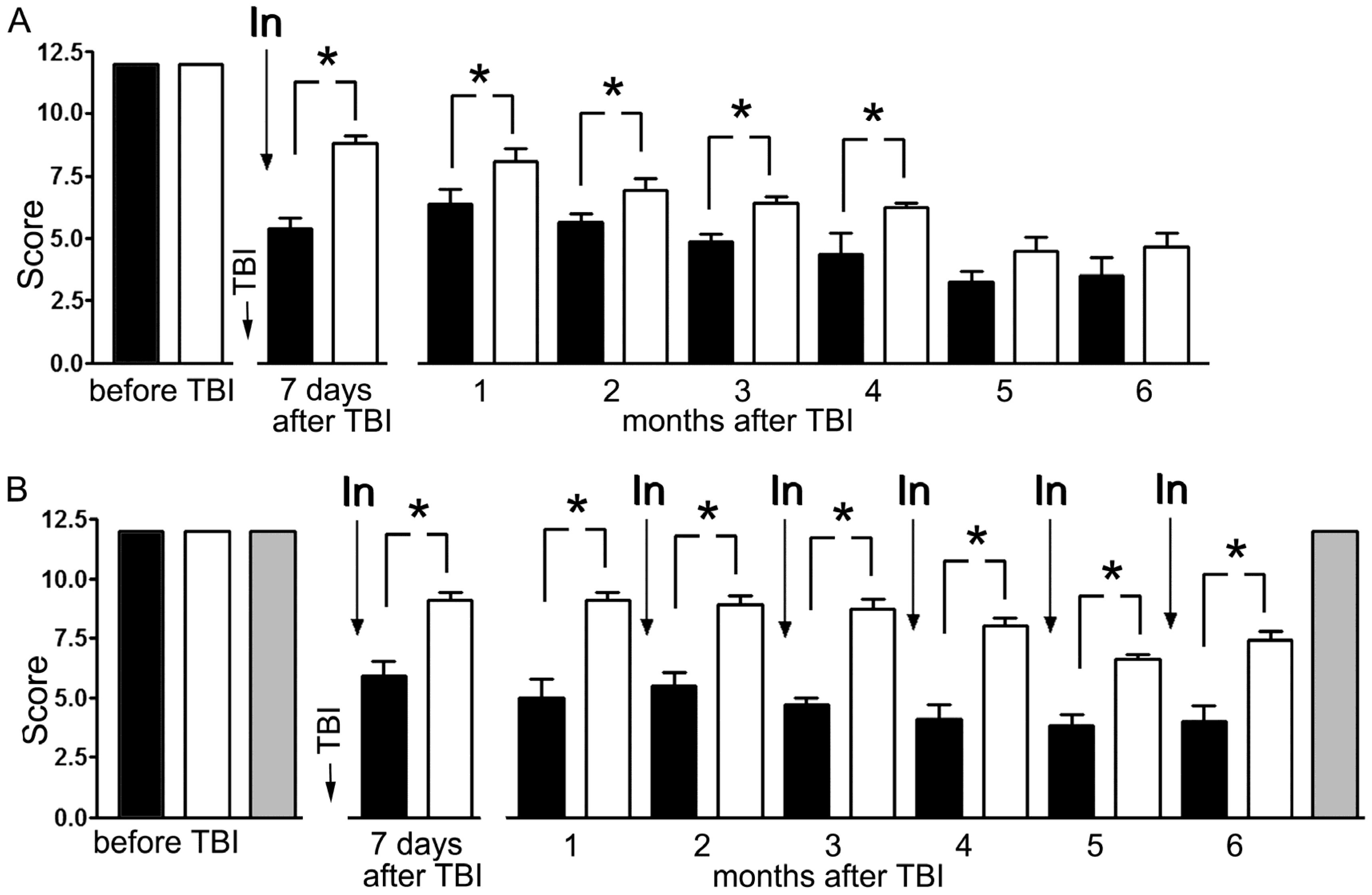{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Modeling Traumatic Brain Injury
2.2. Behavioral Testing
2.3. Morphological Study
2.4. Statistics
3. Results
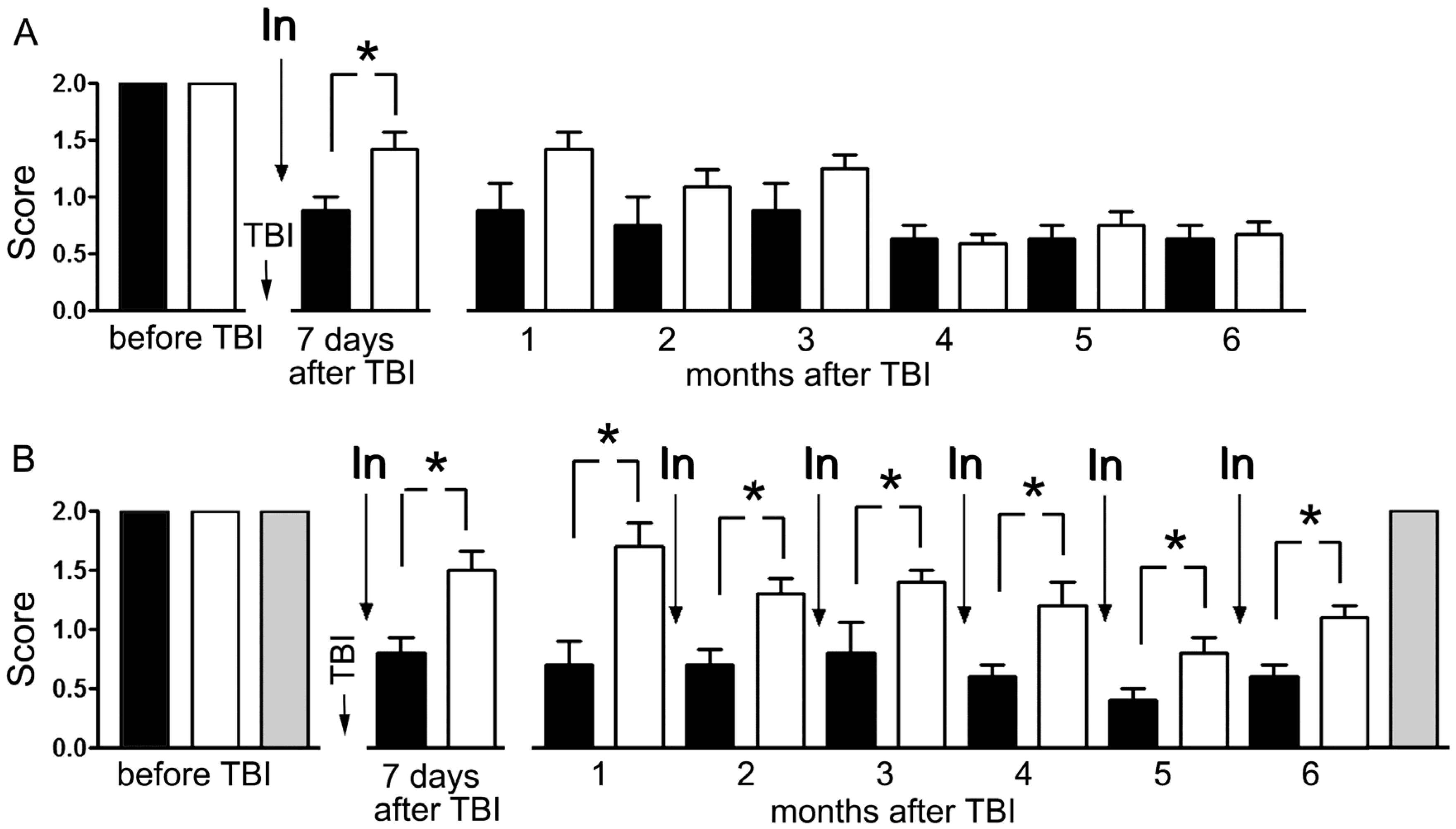
3.1. Effect of Methylene Blue on the Neurological Deficit Caused by Focal Trauma of the Left Sensorimotor Cortex
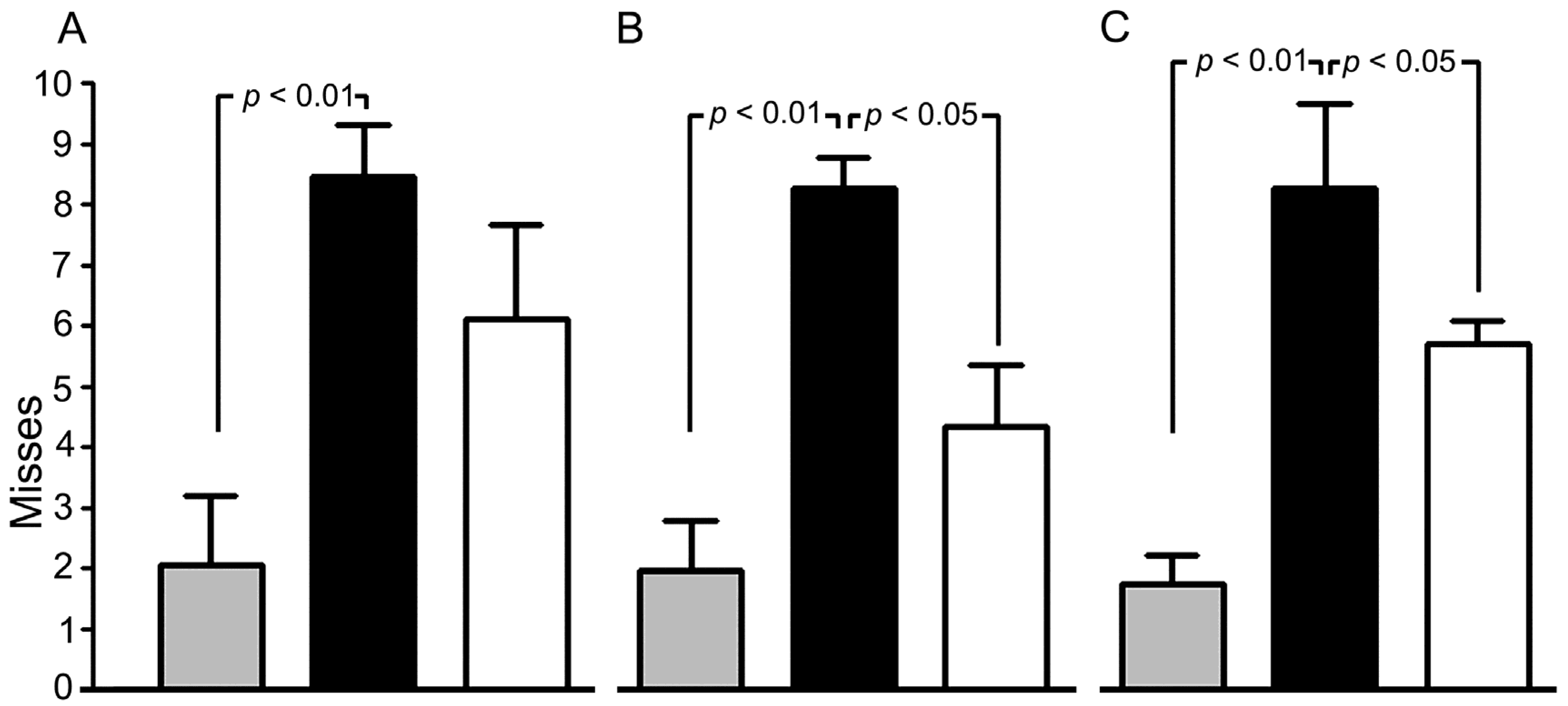
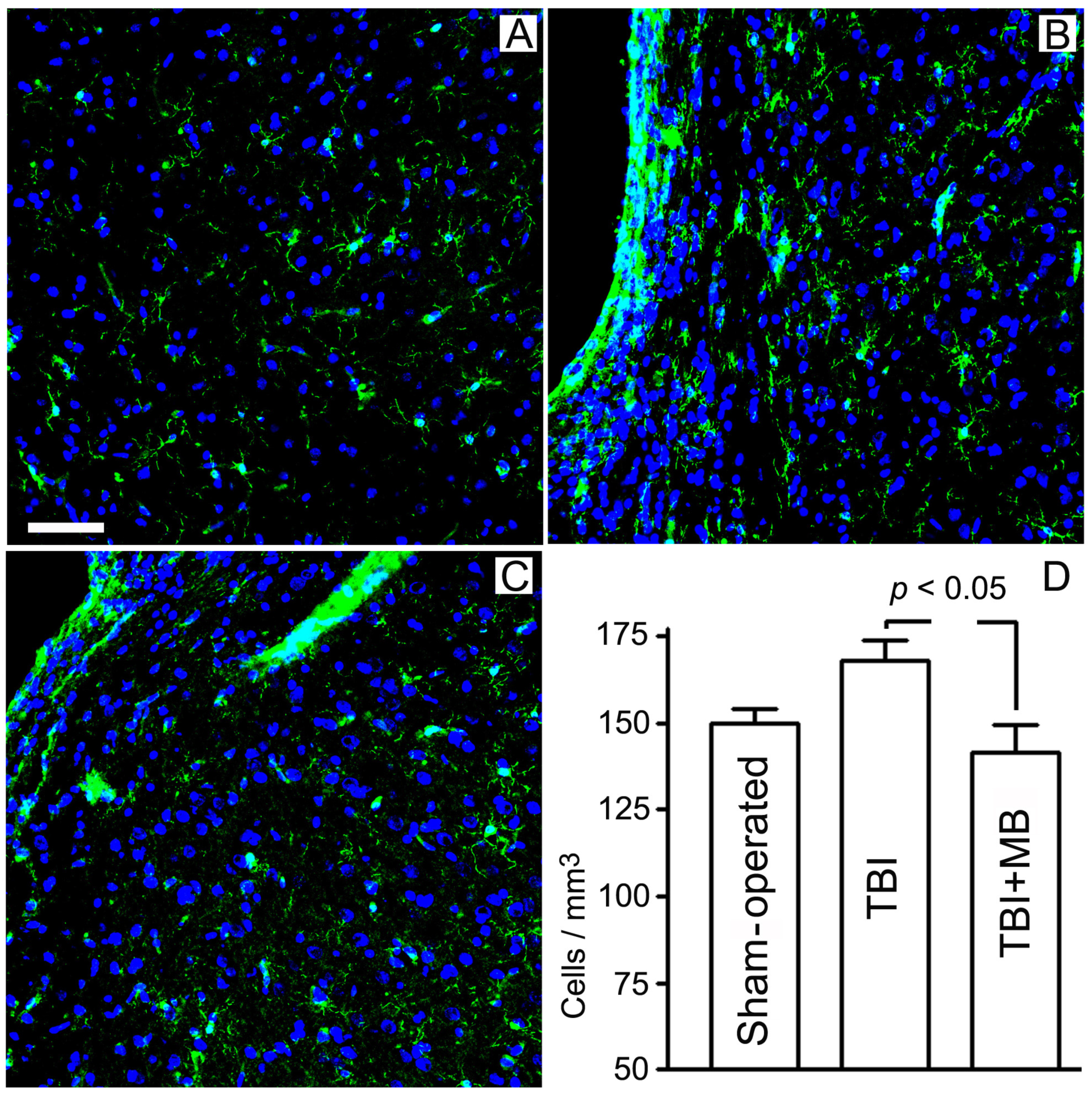
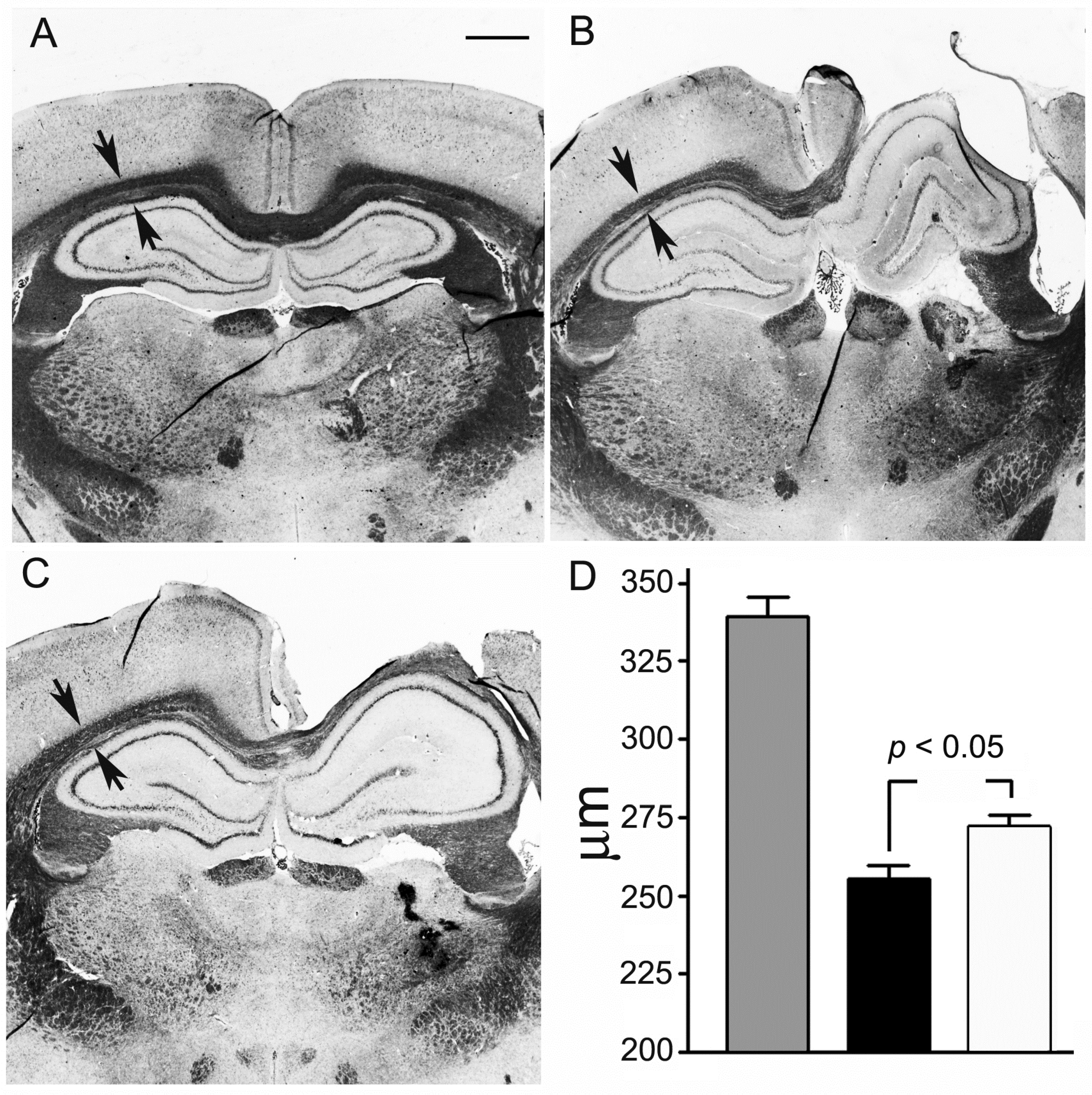
3.2. Effect of Methylene Blue on Microglial Expression and Preservation of Corpus Callosum
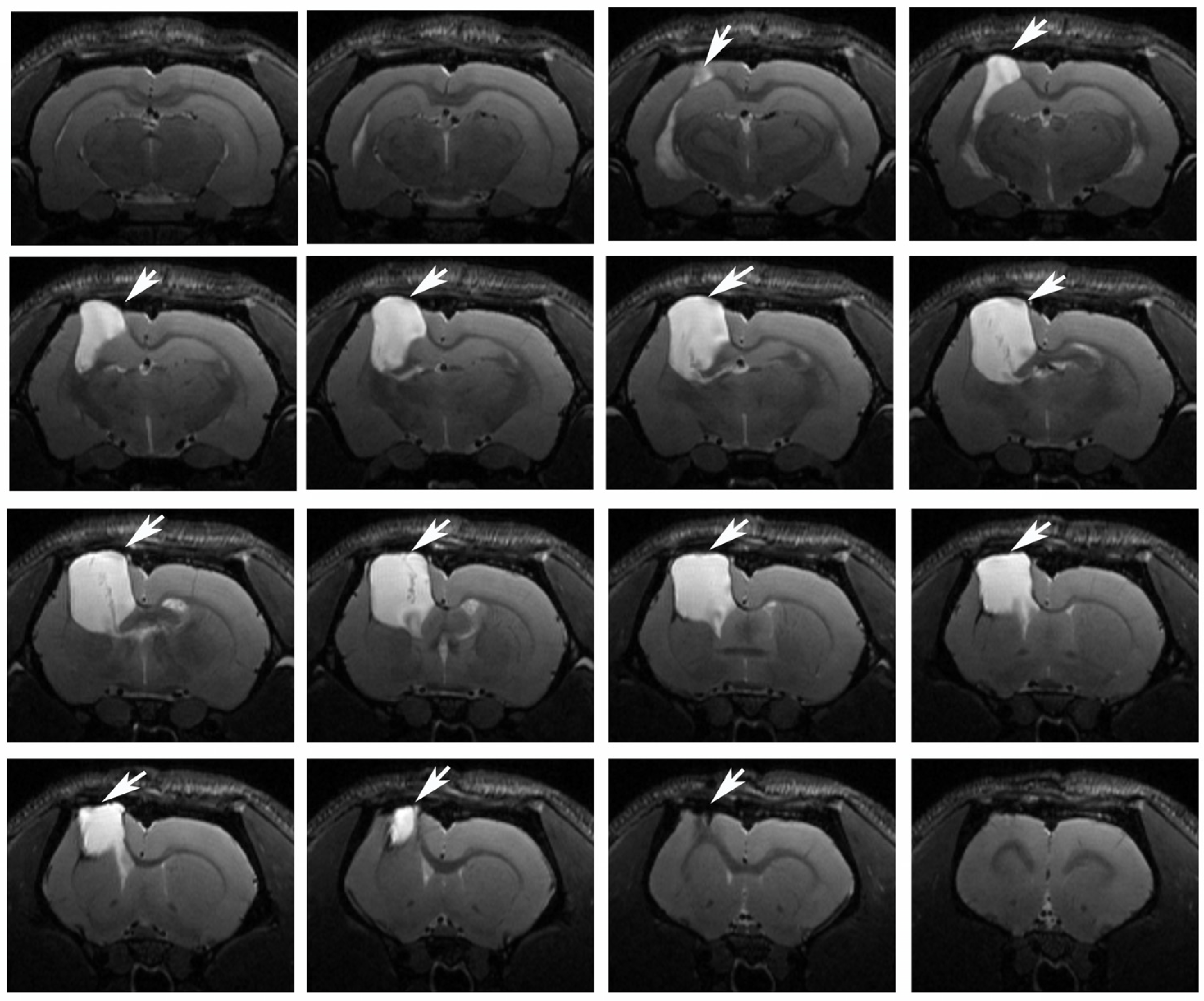
3.3. Brain Magnetic Resonance Imaging
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Vekaria, H.J.; Talley Watts, L.; Lin, A.L.; Sullivan, P.G. Targeting mitochondrial dysfunction in CNS injury using methylene blue; still a magic bullet? Neurochem. Int. 2017, 109, 117–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, A.E. Mechanisms of traumatic brain injury: Biomechanical, structural and cellular considerations. Crit. Care Nurs. Q. 2000, 23, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Impellizzeri, D.; Campolo, M.; Bruschetta, G.; Crupi, R.; Cordaro, M.; Paterniti, I.; Cuzzocrea, S.; Esposito, E. Traumatic brain injury leads to development of Parkinson’s disease related pathology in mice. Front. Neurosci. 2016, 10, 458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glushakova, O.Y.; Johnson, D.; Hayes, R.L. The delayed consequence experimental traumatic brain injury are associated with prolonged inflammation, blood-brain barrier disruption, and progressive white matter damage. J. Neurotraum. 2014, 31, 1180–1193. [Google Scholar] [CrossRef]
- Chen, Z.W.; Liu, A.; Liu, Q.; Chen, J.; Li, W.M.; Chao, X.J.; Yang, Q.; Liu, P.Q.; Mao, Z.X.; Pi, R.B. MEF2D mediates the neuroprotective effect of methylene blue against glutamate-induced oxidative damage in HT22 hippocampal cells. Mol. Neurobiol. 2017, 54, 2209–2222. [Google Scholar] [CrossRef]
- Zhang, X.; Rojas, J.C.; Gonzalez-Lima, F. Methylene blue prevents neurodegeneration caused by rotenone in the retina. Neurotox. Res. 2006, 9, 47–57. [Google Scholar] [CrossRef]
- Stelmashook, E.V.; Genrikhs, E.E.; Mukhaleva, E.V.; Kapkaeva, M.R.; Kondratenko, R.V.; Skrebitsky, V.G.; Isaev, N.K. Neuroprotective effects of methylene blue in vivo and in vitro. Bull. Exp. Biol. Med. 2019, 167, 455–459. [Google Scholar] [CrossRef]
- Zhao, M.; Liang, F.; Xu, H.; Yan, W.; Zhang, J. Methylene blue exerts a neuroprotective effect against traumatic brain injury by promoting autophagy and inhibiting microglial activation. Mol. Med. Rep. 2016, 13, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Shen, J.; Xin, W.; Li, Q.; Gao, Y.; Yuan, L.; Zhang, J. methylene blue reduces neuronal apoptosis and improves blood-brain barrier integrity after traumatic brain injury. Front. Neurol. 2019, 10, 1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peter, C.; Hongwan, D.; Küpfer, A.; Lauterburg, B.H. Pharmacokinetics and organ distribution of intravenous and oral methylene blue. Eur. J. Clin. Pharmacol. 2000, 56, 247–250. [Google Scholar] [CrossRef]
- Talley Watts, L.; Long, J.A.; Chemello, J.; Van Koughnet, S.; Fernandez, A.; Huang, S.; Shen, Q.; Duong, T.Q. Methylene blue is neuroprotective against mild traumatic brain injury. J. Neurotraum. 2014, 31, 1063–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isaev, N.K.; Novikova, S.V.; Stelmashook, E.V.; Barskov, I.V.; Silachev, D.N.; Khaspekov, L.G.; Skulachev, V.P.; Zorov, D.B. Mitochondria-targeted plastoquinone antioxidant SkQR1 decreases trauma-induced neurological deficit in rat. Biochemistry (Mosc). 2012, 77, 996–999. [Google Scholar] [CrossRef] [PubMed]
- Feeney, D.M.; Boyeson, M.G.; Linn, R.T.; Murray, H.M.; Dail, W.G. Responses to cortical injury: I. Methodology and local effects of contusions in the rat. Brain Res. 1981, 211, 67–77. [Google Scholar] [CrossRef]
- Li, L.; Chopp, M.; Ding, G.; Qu, C.; Nejad-Davaran, I.S.P.; Davoodi-Bojd, E.; Li, Q.; Mahmood, A.; Jiang, Q. Diffusion-derived magnetic resonance imaging measures of longitudinal microstructural remodeling induced by marrow stromal cell therapy after traumatic brain injury. J. Neurotraum. 2017, 34, 182–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paxinos, G.; Watson, C. Atlas of anatomy of rat brain. In The Rat Brain in Stereotaxic Coordinates, 3rd ed.; Academic Press: Cambridge, MA, USA, 1997. [Google Scholar]
- Genrikhs, E.E.; Stelmashook, E.V.; Popova, O.V.; Kapay, N.A.; Korshunova, G.A.; Sumbatyan, N.V.; Skrebitsky, V.G.; Skulachev, V.P.; Isaev, N.K. Mitochondria-targeted antioxidant SKQT1 decreases trauma-induced neurological deficit in rat and prevents amyloid-β-induced impairment of long-term potentiation in rat hippocampal slices. J. Drug Targ. 2015, 23, 347–352. [Google Scholar] [CrossRef]
- Jolkkonen, J.; Puurunen, K.; Rantakomi, S.; Harkonen, A.; Haapalinna, A.; Sivenius, J. Behavioral effects of the alpha(2)-adrenoceptor antagonist, atipamezole, after focal cerebral ischemia in rats. Eur. J. Pharmacol. 2000, 400, 211–219. [Google Scholar] [CrossRef]
- Genrikhs, E.E.; Stelmashook, E.V.; Isaev, N.K. Method of Assessment of Neurological Deficits of the Limbs of the Experimental Rats. Patent RU 2697791, 19 August 2019. [Google Scholar]
- Genrikhs, E.E.; Stelmashook, E.V.; Alexandrova, O.P.; Novikova, S.V.; Voronkov, D.N.; Glibka, Y.A.; Skulachev, V.P.; Isaev, N.K. The single intravenous administration of mitochondria-targeted antioxidant SkQR1 after traumatic brain injury attenuates neurological deficit in rats. Brain Res. Bull. 2019, 148, 100–108. [Google Scholar] [CrossRef]
- Genrikhs, E.E.; Stelmashook, E.V.; Isaev, N.K. Method for Evaluating the Performance of the Forelimbs in Experimental Animal. Patent RU 2714479, 17 February 2020. [Google Scholar]
- Giacanelli, F.; Moretti, E. On a new technic for the combined staining of nerve cells and fibers: The Kluver-Barrera method. Riv. Patol. Nerv. Ment. 1959, 80, 467–469. [Google Scholar]
- Shively, S.; Scher, A.I.; Perl, D.P.; Diaz-Arrastia, R. Dementia resulting from traumatic brain injury: What is the pathology? Arch. Neurol. 2012, 69, 1245–1251. [Google Scholar] [CrossRef]
- Gardner, R.C.; Yaffe, K. Epidemiology of mild traumatic brain injury and neurodegenerative disease. Mol. Cell Neurosci. 2015, 66(Pt B), 75–80. [Google Scholar] [CrossRef] [Green Version]
- Gupta, R.; Sen, N. Traumatic brain injury: A risk factor for neurodegenerative diseases. Rev. Neurosci. 2016, 27, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Shishido, H.; Kishimoto, Y.; Kawai, N.; Toyota, Y.; Ueno, M.; Kubota, T.; Kirino, Y.; Tamiya, T. Traumatic brain injury accelerates amyloid-β deposition and impairs spatial learning in the triple-transgenic mouse model of Alzheimer’s disease. Neurosci. Lett. 2016, 629, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Genrikhs, E.E.; Voronkov, D.N.; Kapkaeva, M.R.; Isaev, N.K.; Stelmashook, E.V. Focal unilateral traumatic brain injury causes delayed neurodegenerative changes in the brain of Rats. Bull. Exp. Biol. Med. 2017, 164, 211–213. [Google Scholar] [CrossRef] [PubMed]
- Acosta, S.A.; Tajiri, N.; Shinozuka, K.; Ishikawa, H.; Grimmig, B.; Diamond, D.M.; Sanberg, P.R.; Bickford, P.C.; Kaneko, Y.; Borlongan, C.V. Long-term upregulation of inflammation and suppression of cell proliferation in the brain of adult rats exposed to traumatic brain injury using the controlled cortical impact model. PLoS ONE 2013, 8, e53376. [Google Scholar] [CrossRef]
- Kumar Sahel, D.; Kaira, M.; Raj, K.; Sharma, S.; Singh, S. Mitochondrial dysfunctioning and neuroinflammation: Recent highlights on the possible mechanisms involved in Traumatic Brain Injury. Neurosci. Lett. 2019, 710, 134347. [Google Scholar] [CrossRef]
- Siopi, E.; Cho, A.H.; Homsi, S.; Croci, N.; Plotkine, M.; Marchand-Leroux, C.; Jafarian-Tehrani, M. Minocycline restores sAPPα levels and reduces the late histopathological consequences of traumatic brain injury in mice. J. Neurotraum. 2011, 28, 2135–2143. [Google Scholar] [CrossRef]
- Genrikhs, E.E.; Voronkov, D.N.; Kapkaeva, M.R.; Gudasheva, T.A.; Glibka, Y.A.; Isaev, N.K.; Stelmashook, E.V. The delayed protective effect of GK-2, a dipeptide mimetic of Nerve Growth Factor, in a model of rat traumatic brain injury. Brain Res. Bull. 2018, 140, 148–153. [Google Scholar] [CrossRef]
- Cheng, J.P.; Shaw, K.E.; Monaco, C.M.; Hoffman, A.N.; Sozda, C.N.; Olsen, A.S.; Kline, A.E. A relatively brief exposure to environmental enrichment after experimental traumatic brain injury confers long-term cognitive benefits. J. Neurotraum. 2012, 29, 2684–2688. [Google Scholar] [CrossRef] [Green Version]
- Mamere, A.E.; Saraiva, L.A.; Matos, A.L.; Carneiro, A.A.; Santos, A.C. Evaluation of delayed neuronal and axonal damage secondary to moderate and severe traumatic brain injury using quantitative MR imaging techniques. AJNR Am. J. Neuroradiol. 2009, 30, 947–952. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Wang, B.; Huang, T.; Guo, X.; Yang, Z.; Song, J.; Zhang, M. Glial response in early stages of traumatic brain injury. Neurosci. Lett. 2019, 708, 134335. [Google Scholar] [CrossRef]
- Perry, V.H.; Nicoll, J.A.; Holmes, C. Microglia in neurodegenerative disease. Nat. Rev. Neurol. 2010, 6, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Genrikhs, E.E.; Stelmashook, E.V.; Voronkov, D.N.; Novikova, S.V.; Alexandrova, O.P.; Fedorov, A.V.; Isaev, N.K. The single intravenous administration of methylene blue after traumatic brain injury diminishes neurological deficit, blood-brain barrier disruption and decrease in the expression of S100 protein in rats. Brain Res. 2020, 1740, 146854. [Google Scholar] [CrossRef] [PubMed]
- Poteet, E.; Winters, A.; Yan, L.J.; Shufelt, K.; Green, K.N.; Simpkins, J.W.; Wen, Y.; Yang, S.H. Neuroprotective actions of methylene blue and its derivatives. PLoS ONE 2012, 7, e48279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haouzi, P.; Gueguinou, M.; Sonobe, T.; Judenherc-Haouzi, A.; Tubbs, N.; Trebak, M.; Cheung, J.; Bouillaud, F. Revisiting the physiological effects of methylene blue as a treatment of cyanide intoxication. Clin. Toxicol. 2018, 56, 828–840. [Google Scholar] [CrossRef]
- Clifton, J.; Leikin, J.B. Methylene blue. Am. J. Ther. 2003, 10, 289–291. [Google Scholar] [CrossRef] [PubMed]
- Ginimuge, P.R.; Jyothi, S.D. Methylene blue: Revisited. J. Anaesthesiol. Clin. Pharmacol. 2010, 26, 517–520. [Google Scholar] [PubMed]
- Zhang, L.; Liu, Y.; Huang, Z.; Nan, L.; Wang, F.; Zhou, S.; Wang, J.; Feng, X. Toxicity effects of methylene blue on rat intervertebral disc annulus fibrosus cells. Pain Physician 2019, 22, 155–164. [Google Scholar] [PubMed]
- Talley Watts, L.; Long, J.A.; Boggs, R.C.; Manga, H.; Huang, S.; Shen, Q.; Duong, T.Q. Delayed methylene blue improves lesion volume, multi-parametric quantitative magnetic resonance imaging measurements, and behavioral outcome after traumatic brain injury. J Neurotraum. 2016, 33, 194–202. [Google Scholar] [CrossRef]
- Liu, Y.R.; Cardamone, L.; Hogan, R.E.; Gregoire, M.C.; Williams, J.P.; Hicks, R.J.; Binns, D.; Koe, A.; Jones, N.C.; Myers, D.E.; et al. Progressive metabolic and structural cerebral perturbations after traumatic brain injury: An in vivo imaging study in the rat. J. Nucl. Med. 2010, 51, 1788–1795. [Google Scholar] [CrossRef] [Green Version]
- Loane, D.J.; Kumar, A.; Stoica, B.A.; Cabatbat, R.; Faden, A.I. Progressive neurodegeneration after experimental brain trauma: Association with chronic microglial activation. J. Neuropathol. Exp. Neurol. 2014, 73, 14–29. [Google Scholar] [CrossRef] [Green Version]
- Colton, C.; Wilt, S.; Gilbert, D.; Chernyshev, O.; Snell, J.; Dubois-Dalcq, M. Species differences in the generation of reactive oxygen species by microglia. Mol. Chem. Neuropathol. 1996, 28, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.Y.; Lee, A.Y.W. Traumatic brain injuries: Pathophysiology and potential therapeutic targets. Front. Cell Neurosci. 2019, 13, 528. [Google Scholar] [CrossRef] [PubMed]






© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Genrikhs, E.E.; Stelmashook, E.V.; Voronkov, D.N.; Novikova, S.V.; Alexandrova, O.P.; Gulyaev, M.V.; Isaev, N.K. The Delayed Neuroprotective Effect of Methylene Blue in Experimental Rat Brain Trauma. Antioxidants 2020, 9, 377. https://doi.org/10.3390/antiox9050377
Genrikhs EE, Stelmashook EV, Voronkov DN, Novikova SV, Alexandrova OP, Gulyaev MV, Isaev NK. The Delayed Neuroprotective Effect of Methylene Blue in Experimental Rat Brain Trauma. Antioxidants. 2020; 9(5):377. https://doi.org/10.3390/antiox9050377
Chicago/Turabian StyleGenrikhs, Elizaveta E., Elena V. Stelmashook, Dmitriy N. Voronkov, Svetlana V. Novikova, Olga P. Alexandrova, Mikhail V. Gulyaev, and Nickolay K. Isaev. 2020. "The Delayed Neuroprotective Effect of Methylene Blue in Experimental Rat Brain Trauma" Antioxidants 9, no. 5: 377. https://doi.org/10.3390/antiox9050377