Emerging Biomarkers of Oxidative Stress in Acute and Stable Coronary Artery Disease: Levels and Determinants

 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Blood Sampling and Biochemical Analysis
2.3. Statistical Analysis
3. Results
3.1. Study Population Characteristics
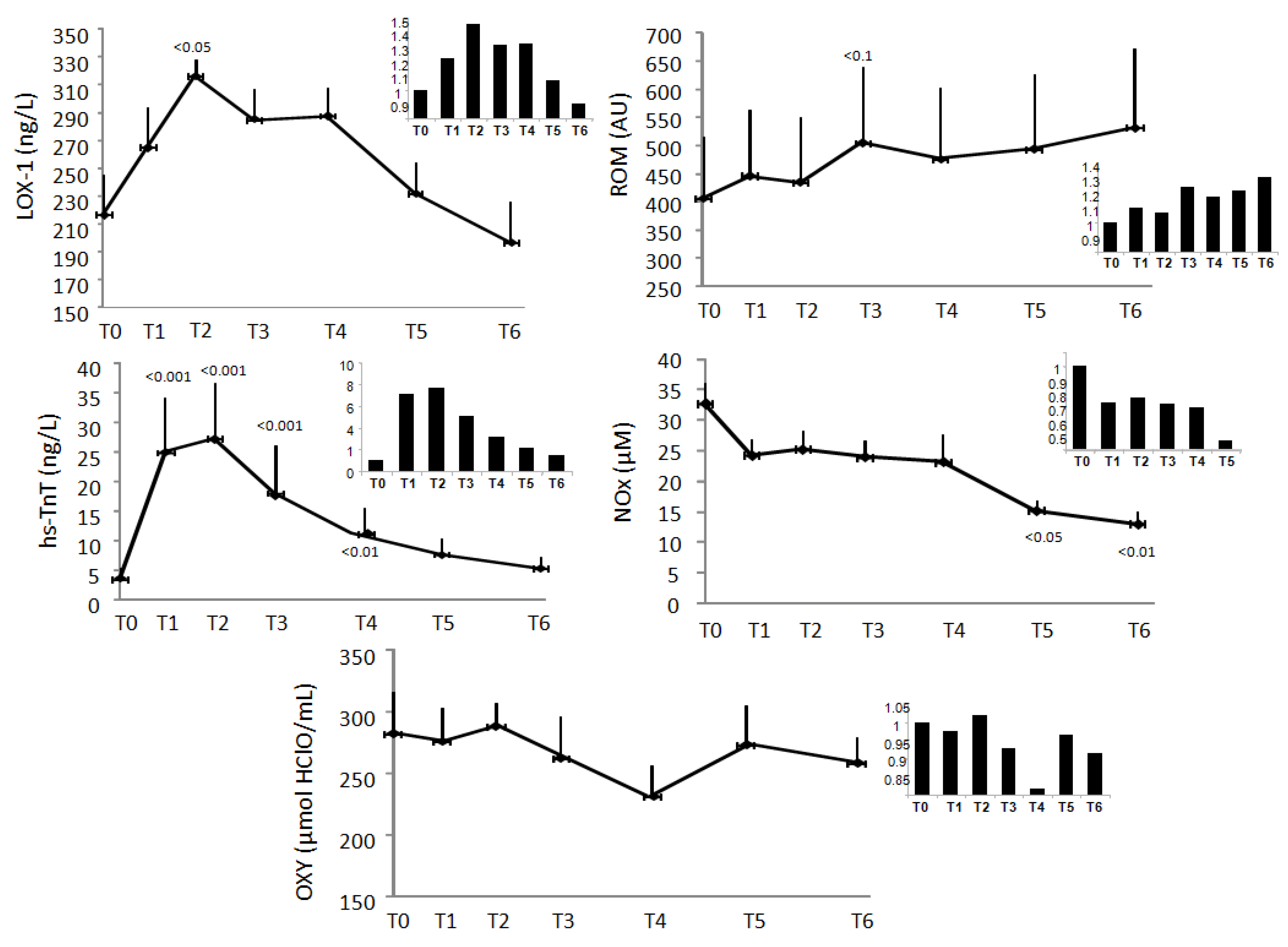
3.2. Response over AMI Time of Oxidative Stress-Related Biomarkers
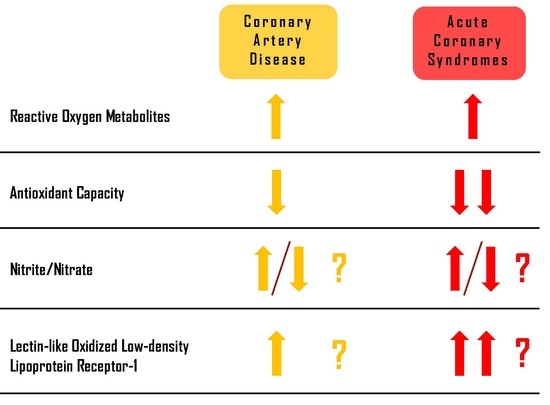
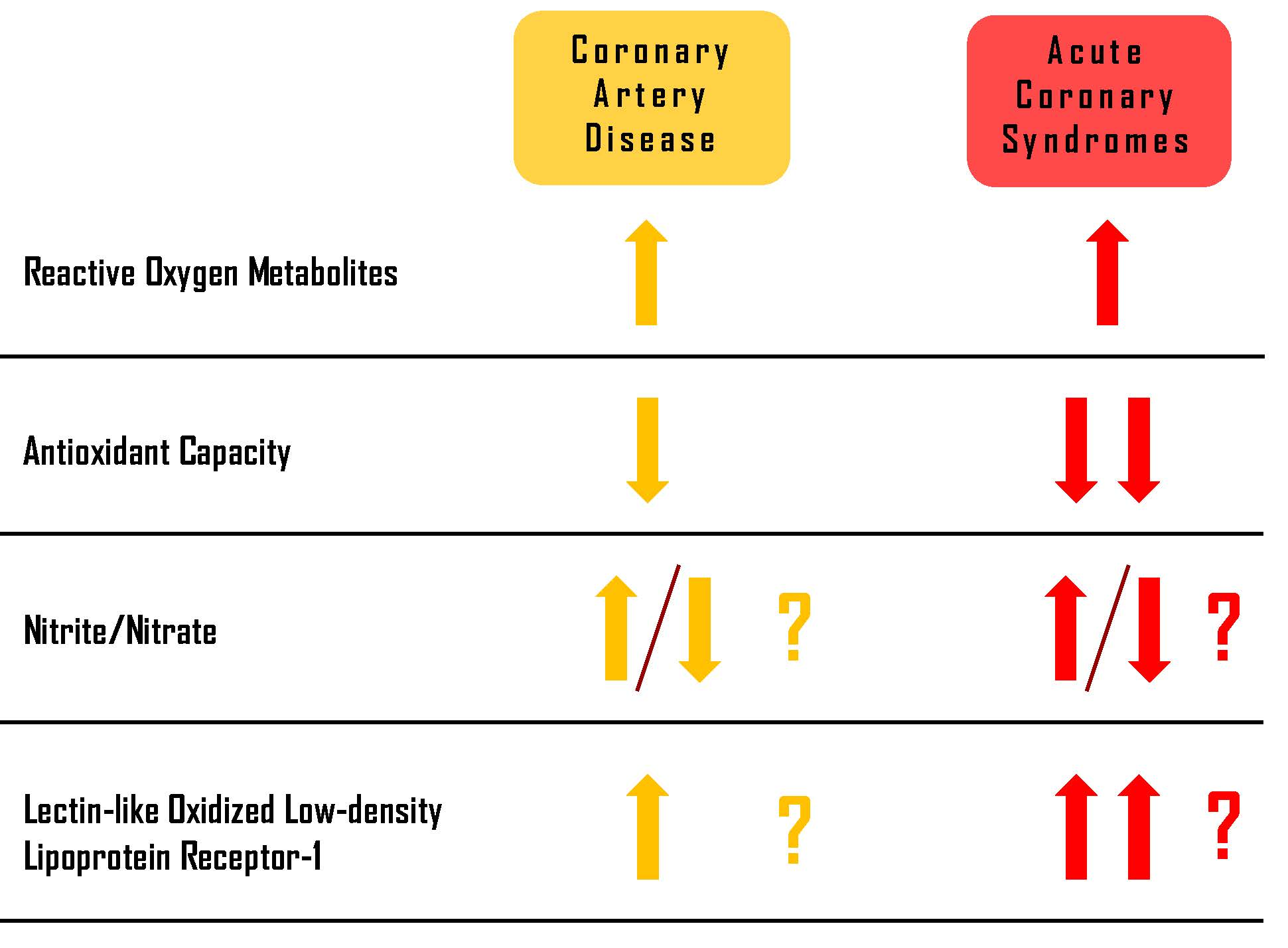
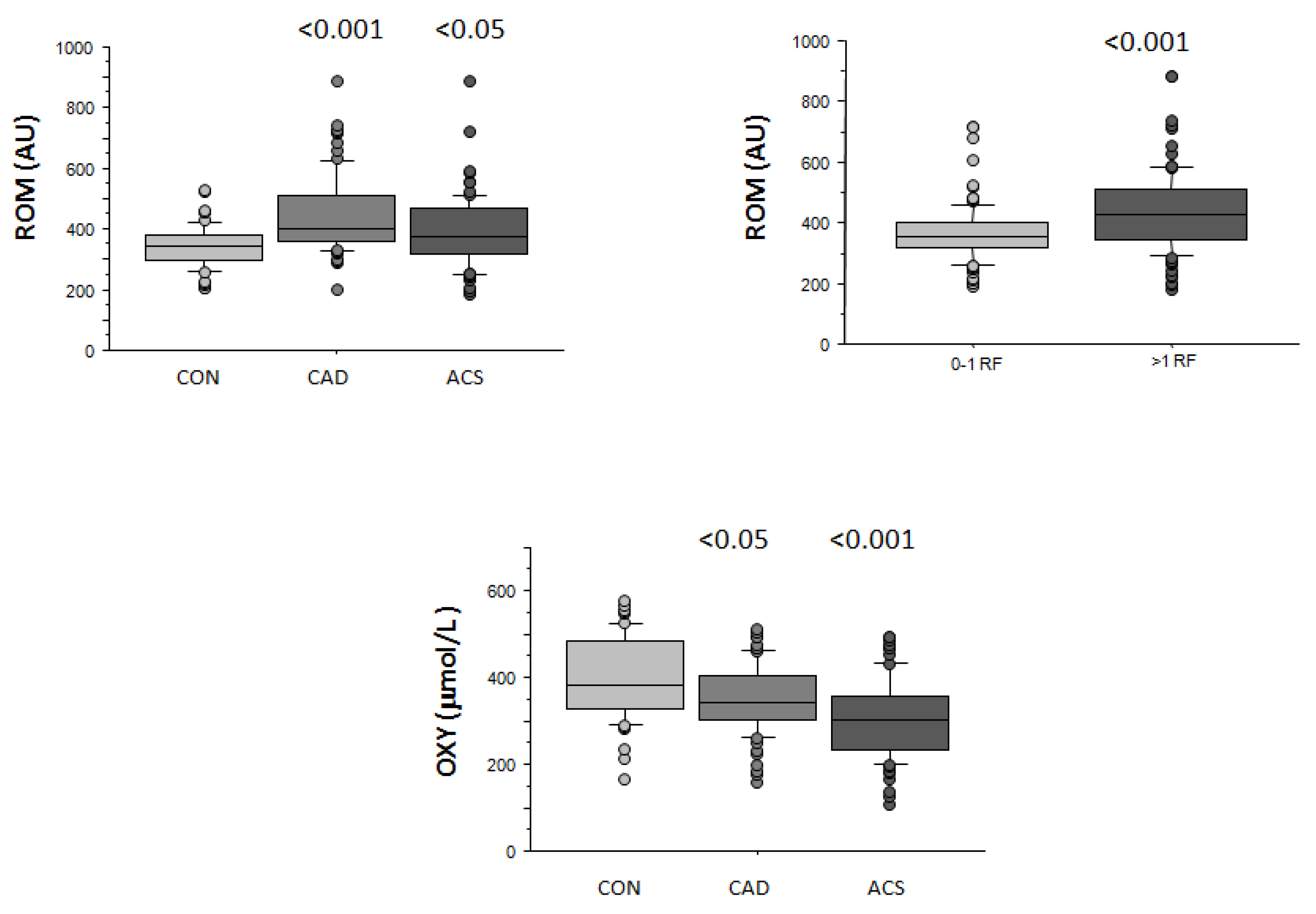
3.3. Reactive Oxygen Metabolites (ROM)
3.4. Antioxidante Capacity (OXY)
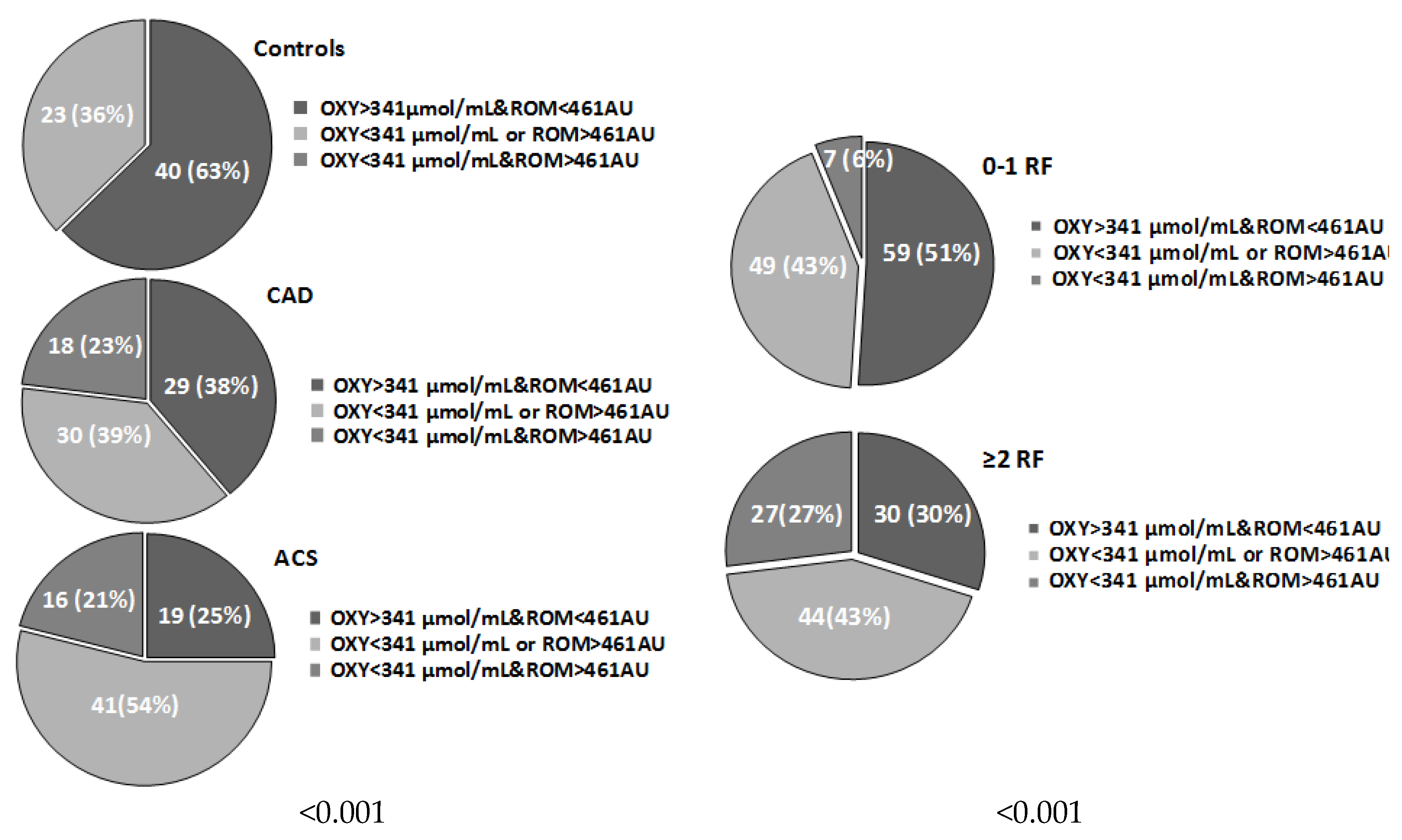
3.5. Systemic Oxidative Stress Status
3.6. Nitrite/Nitrate (NOx)
3.7. Lectin-Like Oxidized Low-Density Lipoprotein Receptor-1 (LOX-1)
4. Discussion
4.1. Reactive Oxygen Metabolites (ROM) and Antioxidant Capacity (OXY)
4.2. Nitrite/Nitrate (NOx)
4.3. Lectin-Like Oxidized Low-Density Lipoprotein Receptor-1 (LOX-1)
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vassalle, C.; Pratali, L.; Boni, C.; Mercuri, A.; Ndreu, R. An oxidative stress score as a combined measure of the pro-oxidant and anti-oxidant counterparts in patients with coronary artery disease. Clin Biochem. 2008, 41, 1162–1167. [Google Scholar] [CrossRef]
- Vassalle, C.; Bianchi, S.; Battaglia, D.; Landi, P.; Bianchi, F.; Carpeggiani, C. Elevated levels of oxidative stress as a prognostic predictor of major adverse cardiovascular events in patients with coronary artery disease. J. Atheroscler. Thromb. 2012, 19, 712–717. [Google Scholar] [CrossRef]
- González-Montero, J.; Brito, R.; Gajardo, A.I.; Rodrigo, R. Myocardial reperfusion injury and oxidative stress: Therapeutic opportunities. World J. Cardiol. 2018, 10, 74–86. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C. Oxidative stress and cardiovascular risk prediction: The long way towards a “radical” perspective. Int. J. Cardiol. 2018, 273, 252–253. [Google Scholar]
- Vassalle, C. New biomarkers and traditional cardiovascular risk scores: Any crystal ball for current effective advice and future exact prediction? Clin. Chem. Lab. Med. 2018, 56, 1803–1805. [Google Scholar] [CrossRef]
- Iamele, L.; Fiocchi, R.; Vernocchi, A. Evaluation of an automated spectrophotometric assay for reactive oxygen metabolites in serum. Clin. Chem. Lab. Med. 2002, 40, 673–676. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C. An easy and reliable automated method to estimate oxidative stress in the clinical setting. Methods Mol. Biol. 2008, 477, 31–39. [Google Scholar] [PubMed]
- Vassalle, C.; Maffei, S.; Boni, C.; Zucchelli, G.C. Gender-related differences in oxidative stress levels among elderly patients with coronary artery disease. Fertil. Steril. 2008, 89, 608–613. [Google Scholar]
- Zhao, Y.; Vanhoutte, P.M.; Leung, S.W. Vascular nitric oxide: Beyond eNOS. J. Pharmacol. Sci. 2015, 129, 83–94. [Google Scholar] [CrossRef] [Green Version]
- Chirinos, J.A.; Akers, S.R.; Trieu, L.; Ischiropoulos, H.; Doulias, P.T.; Tariq, A.; Vasim, I.; Koppula, M.R.; Syed, A.A.; Soto-Calderon, H.; et al. Heart Failure, Left Ventricular Remodeling, and Circulating Nitric Oxide Metabolites. J. Am. Heart Assoc. 2016, 5. [Google Scholar] [CrossRef]
- Maher, A.; Abdel Rahman, M.F.; Gad, M.Z. The Role of Nitric Oxide from Neurological Disease to Cancer. Adv. Exp. Med. Biol. 2017, 1007, 71–88. [Google Scholar]
- Spychalowicz, A.; Wilk, G.; Śliwa, T.; Ludew, D.; Guzik, T.J. Novel therapeutic approaches in limiting oxidative stress and inflammation. Curr. Pharm. Biotechnol. 2012, 13, 2456–2466. [Google Scholar] [CrossRef]
- Vassalle, C.; Lubrano, V.; L’Abbate, A.; Clerico, A. Determination of nitrite plus nitrate and malondialdehyde in human plasma: Analytical performance and the effect of smoking and exercise. Clin. Chem. Lab. Med. 2002, 40, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Moriwaki, H.; Kume, N.; Sawamura, T.; Aoyama, T.; Hoshikawa, H.; Ochi, H.; Nishi, E.; Masaki, T.; Kita, T. Ligand specificity of LOX-1, a novel receptor for oxidized low-density lipoprotein. Arterioscler. Thromb. Vasc. Biol. 1998, 18, 1541–1547. [Google Scholar] [CrossRef]
- Cominacini, L.; Rigoni, A.; Pasini, A.F.; Garbin, U.; Davoli, A.; Campagnola, M.; Pastorino, A.M.; Lo Cascio, V.; Sawamura, T. The binding of oxidized low-density lipoprotein (ox-LDL) to ox-LDL receptor-1 reduces the intracellular concentration of nitric oxide in endothelial cells through an increased production of superoxide. J. Biol. Chem. 2001, 276, 13750–13755. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Mehta, J.L. Antisense to LOX-1 inhibits oxidized LDL-mediated upregulation of monocyte chemoattractant protein-1 and monocyte adhesion to human coronary artery endothelial cells. Circulation 2000, 101, 2889–2895. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, H.; Kume, N.; Miyamoto, S.; Minami, M.; Morimoto, M.; Hayashida, K.; Hashimoto, N.; Kita, T. Oxidized low density lipoprotein (Ox-LDL) modulates Bax/Bcl-2 through lectin-like Ox-LDL receptor-1 in vascular smooth muscle cells. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 955–960. [Google Scholar] [CrossRef]
- Mehta, J.L.; Chen, J.; Hermonat, P.L.; Romeo, F.; Novelli, G. Lectin-like, oxidized low-density lipoprotein receptor-1 (LOX-1): A critical player in the development of atherosclerosis and related disorders. Cardiovasc. Res. 2006, 69, 36–45. [Google Scholar] [CrossRef] [Green Version]
- Kataoka, H.; Kume, N.; Miyamoto, S.; Minami, M.; Moriwaki, H.; Murase, T.; Sawamura, T.; Masaki, T.; Hashimoto, N.; Kita, T. Expression of lectin like oxidized low-density lipoprotein receptor-1 in human atherosclerotic lesions. Circulation 1999, 99, 3110–3117. [Google Scholar] [CrossRef]
- Hayashida, K.; Kume, N.; Murase, T.; Minami, M.; Nakagawa, D.; Inada, T.; Tanaka, M.; Ueda, A.; Kominami, G.; Kambara, H.; et al. Serum soluble lectin-like oxidized low-density lipoprotein receptor-1 levels are elevated in acute coronary syndrome: A novel marker for early diagnosis. Circulation 2005, 112, 812–818. [Google Scholar] [CrossRef]
- Vassalle, C.; Vigna, L.; Bianchi, S.; Maffei, S.; Novembrino, C.; De Giuseppe, R.; de Liso, F.; Vannucci, A.; Tirelli, S.; Maiavacca, R.; et al. A biomarker of oxidative stress as a nontraditional risk factor in obese subjects. Biomark. Med. 2013, 7, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C.; Boni, C.; Di Cecco, P.; Ndreu, R.; Zucchelli, G.C. Automation and validation of a fast method for the assessment of in vivo oxidative stress levels. Clin. Chem. Lab. Med. 2006, 44, 1372–1375. [Google Scholar] [CrossRef]
- Vassalle, C.; Masini, S.; Carpeggiani, C.; L’Abbate, A.; Boni, C.; Zucchelli, G.C. In vivo total antioxidant capacity: Comparison of two different analytical methods. Clin. Chem. Lab. Med. 2004, 42, 84–89. [Google Scholar] [CrossRef]
- Maffei, S.; Mercuri, A.; Zucchelli, G.C.; Vassalle, C. Estrogen therapy effects on different vasoactive factors in recent postmenopausal healthy women. Int. J. Cardiol. 2006, 107, 194–199. [Google Scholar] [CrossRef]
- Vassalle, C.; Lubrano, V.; Domenici, C.; L’Abbate, A. Influence of chronic aerobic exercise on microcirculatory flow and nitric oxide in humans. Int. J. Sports Med. 2003, 24, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Hirata, Y.; Yamamoto, E.; Tokitsu, T.; Kusaka, H.; Fujisue, K.; Kurokawa, H.; Sugamura, K.; Maeda, H.; Tsujita, K.; Kaikita, K.; et al. Reactive oxygen metabolites are closely associated with the diagnosis and prognosis of coronary artery disease. J. Am. Heart Assoc. 2015, 4. [Google Scholar] [CrossRef] [PubMed]
- Kitano, D.; Takayama, T.; Nagashima, K.; Akabane, M.; Okubo, K.; Hiro, T.; Hirayama, A. A comparative study of time-specific oxidative stress after acute myocardial infarction in patients with and without diabetes mellitus. BMC Cardiovasc. Disord. 2016, 16, 102. [Google Scholar] [CrossRef]
- Rodrigo, R.; Libuy, M.; Feliú, F.; Hasson, D. Oxidative stress-related biomarkers in essential hypertension and ischemia-reperfusion myocardial damage. Dis. Markers 2013, 35, 773–790. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, P.; Leone, A.M.; Francis, P.L.; Struthers, A.D.; Moncada, S. The L -arginine:nitric oxide pathway is the major source of plasma nitrite in fasted humans. Biochem. Biophys. Res. Commun. 1995, 209, 590–596. [Google Scholar] [CrossRef]
- Yoon, Y.; Song, J.; Hong, S.H.; Kim, J.Q. Plasma nitric oxide concentrations and nitric oxide synthase gene polymorphisms in coronary artery disease. Clin. Chem. 2000, 46, 1626–1630. [Google Scholar]
- Akiyama, K.; Kimura, A.; Suzuki, H.; Takeyama, Y.; Gluckman, T.L.; Terhakopian, A.; Katagiri, T.; Suh, K.Y.; Roseto, J.; Bing, R.J. Production of oxidative products of nitric oxide in infarcted human heart. J. Am. Coll. Cardiol. 1998, 32, 373–379. [Google Scholar] [CrossRef] [Green Version]
- Higashino, H.; Tabuchi, M.; Yamagata, S.; Kurita, T.; Miya, H.; Mukai, H.; Miya, Y. Serum Nitric Oxide Metabolite Levels in Groups of Patients with Various Diseases in Comparison of Healthy Control Subjects. J. Med. Sci. 2010, 10, 1–11. [Google Scholar] [CrossRef]
- Fan, Q.; Chen, M.; Fang, X.; Lau, W.B.; Xue, L.; Zhao, L.; Zhang, H.; Liang, Y.H.; Bai, X.; Niu, H.Y.; Ye, J.; et al. Aging might augment reactive oxygen species (ROS) formation and affect reactive nitrogen species (RNS) level after myocardial ischemia/reperfusion in both humans and rats. Age 2013, 35, 1017–1026. [Google Scholar] [CrossRef]
- Rusak, T.; Misztal, T.; Piszcz, J.; Tomasiak, M. Nitric oxide scavenging by cell-free hemoglobin may be a primary factor determining hypertension in polycythemic patients. Free Radic. Res. 2014, 48, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Naregal, G.V.; Devaranavadagi, B.B.; Patil, S.G.; Aski, B.S. Elevation of Oxidative Stress and Decline in Endogenous Antioxidant Defense in Elderly Individuals with Hypertension. J. Clin. Diagn. Res. 2017, 11, BC09–BC12. [Google Scholar] [CrossRef] [PubMed]
- Ueda, A.; Kume, N.; Hayashida, K.; Inui-Hayashida, A.; Asai, M.; Kita, T.; Kominami, G. ELISA for soluble form of lectin-like oxidized LDL receptor-1, a novel marker of acute coronary syndrome. Clin. Chem. 2006, 52, 1210–1211. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Ohta, H.; Kume, N.; Hayashida, K.; Tanaka, M.; Mitsuoka, H.; Kaneshige, T.; Misaki, S.; Imagawa, K.; Shimosako, K.; et al. Generation of monoclonal antibodies against a soluble form of lectin-like oxidized low-density lipoprotein receptor-1 and development of a sensitive chemiluminescent enzyme immunoassay. J. Pharm. Biomed. Anal. 2010, 51, 158–163. [Google Scholar] [CrossRef]
- Lubrano, V.; Del Turco, S.; Nicolini, G.; Di Cecco, P.; Basta, G. Circulating levels of lectin-like oxidized low-density lipoprotein receptor-1 are associated with inflammatory markers. Lipids 2008, 43, 945–950. [Google Scholar] [CrossRef]
- Balin, M.; Celik, A.; Kobat, M.A. Circulating soluble lectin-like oxidized low-density lipoprotein receptor-1 levels are associated with proximal/middle segment of the LAD lesions in patients with stable coronary artery disease. Clin. Res. Cardiol. 2012, 101, 247–253. [Google Scholar] [CrossRef]
- Zhao, Z.W.; Xu, Y.W.; Li, S.M.; Guo, J.J.; Yi, T.; Chen, L.L. Higher serum lectin-like oxidized low-density lipoprotein receptor-1 in patients with stable coronary artery disease is associated with major adverse cardiovascular events: A multicentre pilot study. Biochem. Med. (Zagreb). 2019, 29, 010705. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, D.; Higashiyama, A.; Wakabayashi, I.; Kubota, Y.; Adachi, Y.; Hayashibe, A.; Kawamura, K.; Kuwabara, K.; Nishimura, K.; Kadota, A.; et al. The Relationship between Lectin-Like Oxidized Low-Density Lipoprotein Receptor-1 Ligands Containing Apolipoprotein B and the Cardio-Ankle Vascular Index in Healthy Community Inhabitants: The KOBE Study. J. Atheroscler. Thromb. 2015, 22, 499–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokota, C.; Sawamura, T.; Watanabe, M.; Kokubo, Y.; Fujita, Y.; Kakino, A.; Nakai, M.; Toyoda, K.; Miyamoto, Y.; Minematsu, K. High Levels of Soluble Lectin-Like Oxidized Low-Density Lipoprotein Receptor-1 in Acute Stroke: An Age- and Sex-Matched Cross-Sectional Study. J. Atheroscler. Thromb. 2016, 23, 1222–1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | CON (63) | CAD (77) | ACS (76) | p Value |
|---|---|---|---|---|
| Age (Years) | 64 ± 7 | 69 ± 9 | 66 ± 11 | <0.05 |
| Male gender | 25 (40) | 53 (69) | 36 (47) | <0.01 |
| Hypertension | 27 (42) | 45 (59) | 37 (49) | ns |
| Dyslipidemia | 16 (25) | 51 (67) | 39 (51) | <0.001 |
| Type 2 Diabetes | 0 (0) | 27 (35) | 18 (24) | <0.001 |
| Smoking history | 0 (0) | 31 (41) | 32 (42) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lubrano, V.; Pingitore, A.; Traghella, I.; Storti, S.; Parri, S.; Berti, S.; Ndreu, R.; Andrenelli, A.; Palmieri, C.; Iervasi, G.; et al. Emerging Biomarkers of Oxidative Stress in Acute and Stable Coronary Artery Disease: Levels and Determinants. Antioxidants 2019, 8, 115. https://doi.org/10.3390/antiox8050115
Lubrano V, Pingitore A, Traghella I, Storti S, Parri S, Berti S, Ndreu R, Andrenelli A, Palmieri C, Iervasi G, et al. Emerging Biomarkers of Oxidative Stress in Acute and Stable Coronary Artery Disease: Levels and Determinants. Antioxidants. 2019; 8(5):115. https://doi.org/10.3390/antiox8050115
Chicago/Turabian StyleLubrano, Valter, Alessandro Pingitore, Irene Traghella, Simona Storti, Serena Parri, Sergio Berti, Rudina Ndreu, Andrea Andrenelli, Cataldo Palmieri, Giorgio Iervasi, and et al. 2019. "Emerging Biomarkers of Oxidative Stress in Acute and Stable Coronary Artery Disease: Levels and Determinants" Antioxidants 8, no. 5: 115. https://doi.org/10.3390/antiox8050115