
Intracarotid Infusion of Redox-Active Manganese Porphyrin, MnTnBuOE-2-PyP5+, following Reperfusion Improves Long-Term, 28-Day Post-Stroke Outcomes in Rats

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experiment 1: Effect of BMX-001 on Acute Stroke Outcomes in Young Male Rats
2.2. Experiment 2: Effect of BMX-001 on 28-Day Post-Stroke Outcomes in Young Female Rats
2.3. Experiment 3: Effect of BMX-001 Treatment Duration on 28-Day Post-Stroke Outcomes in Young Male Rats
2.4. Experiment 4: Effects of BMX-001 on Stroke Outcomes in Young Spontaneous Hypertension Rats
2.5. Experiment 5: Effect of BMX-001 on Stroke Outcomes in Aged Female Rats
2.6. Experiment 6: BMX-001 Brain Concentration Measurement
2.7. Experiment 7: Effect of BMX-001 Infused via Carotid Artery on Blood–Brain Barrier Permeability and the Vascular Endothelial Wall
2.8. Experiment 8: Interaction of BMX-001 with t-PA
2.9. Statistical Analysis
3. Results
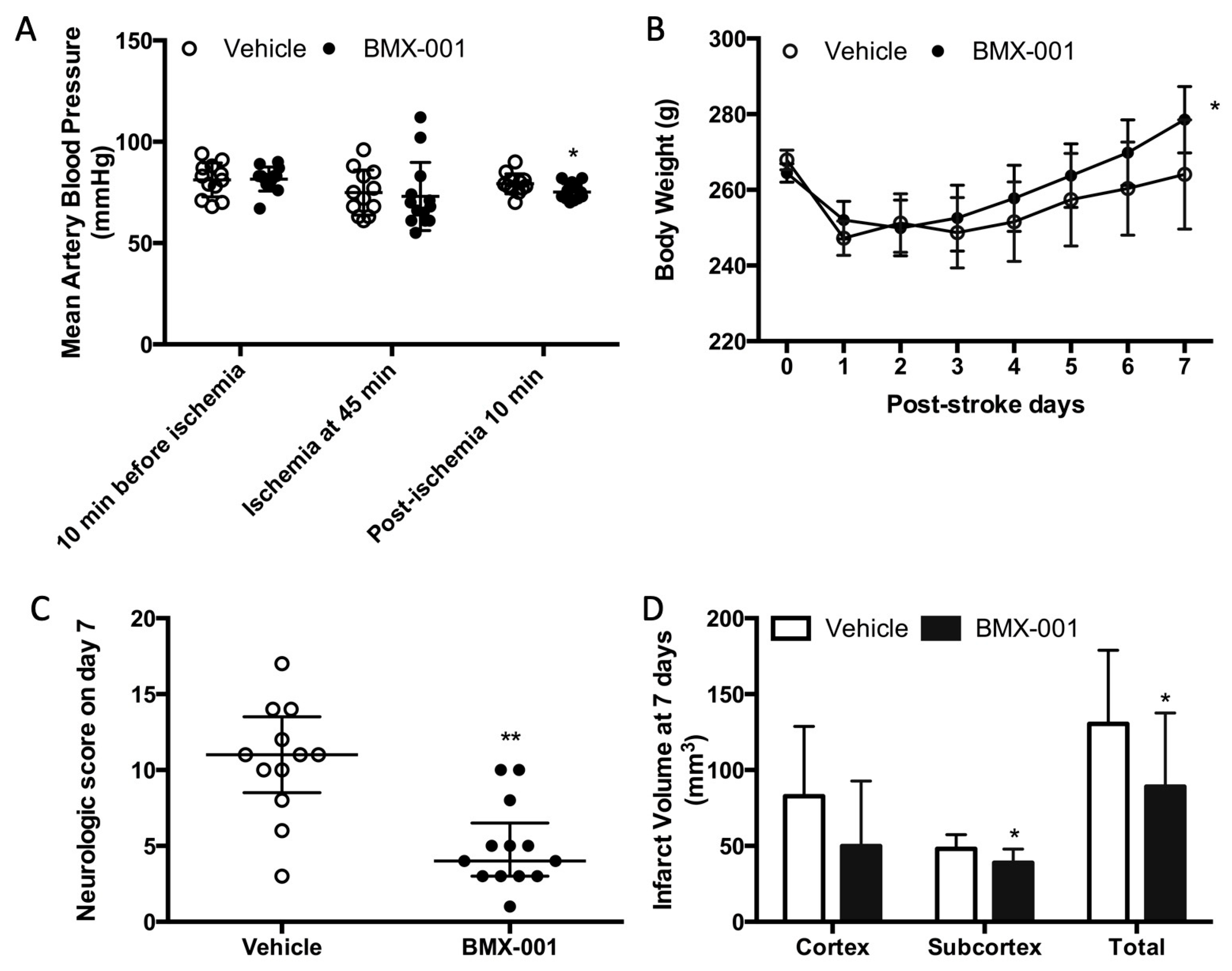
3.1. Experiment 1: BMX-001 Provided Acute Protection in Young Male Stroke Rats
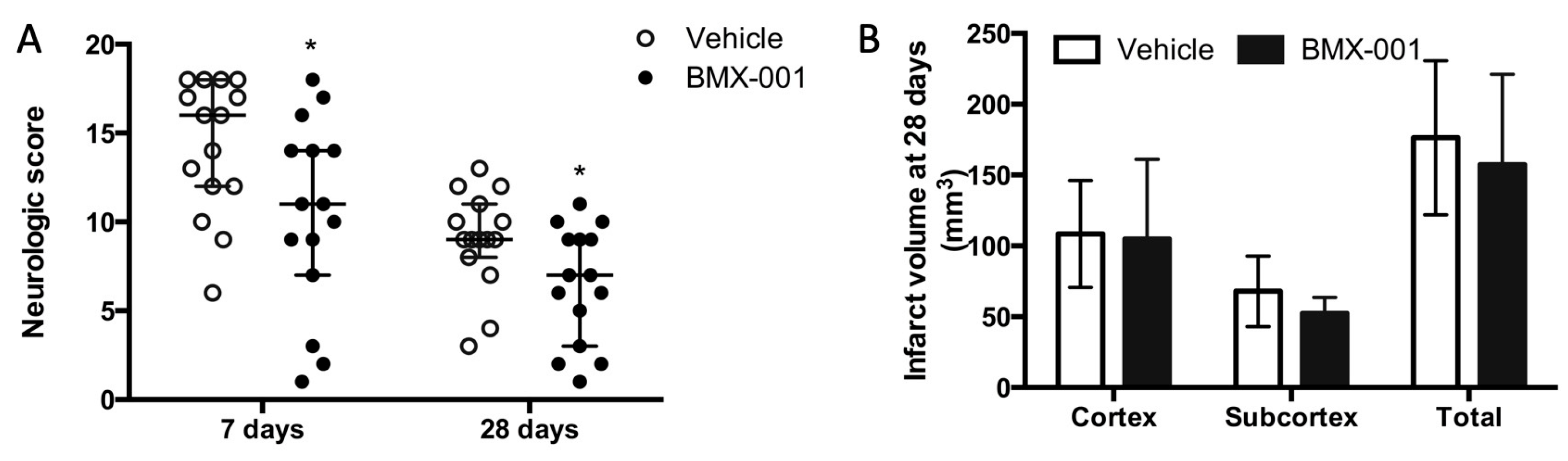
3.2. Experiment 2: BMX-001 Reduced Neurologic Deficits in 28-Day Post-Stroke Survived Young Female Rats
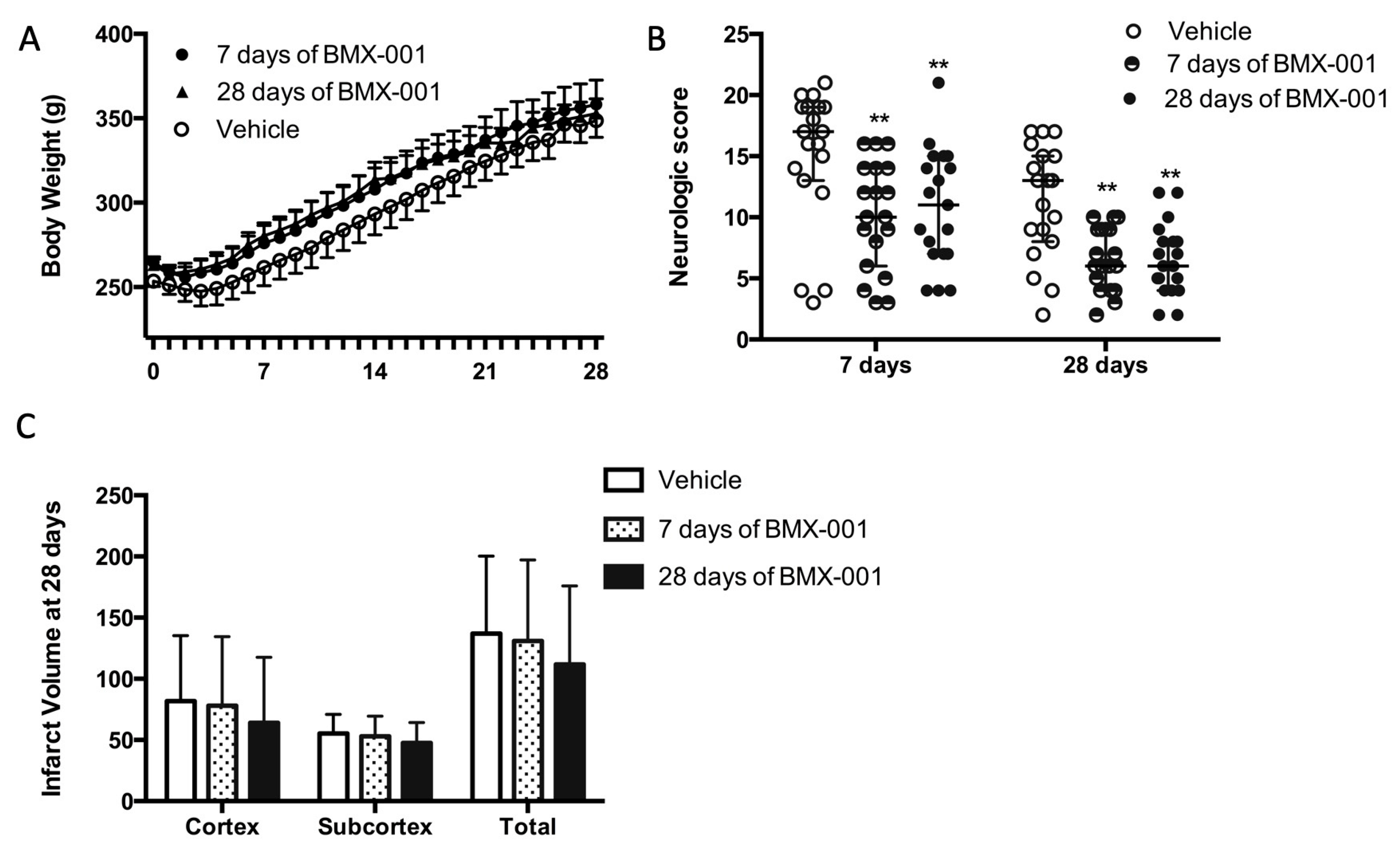
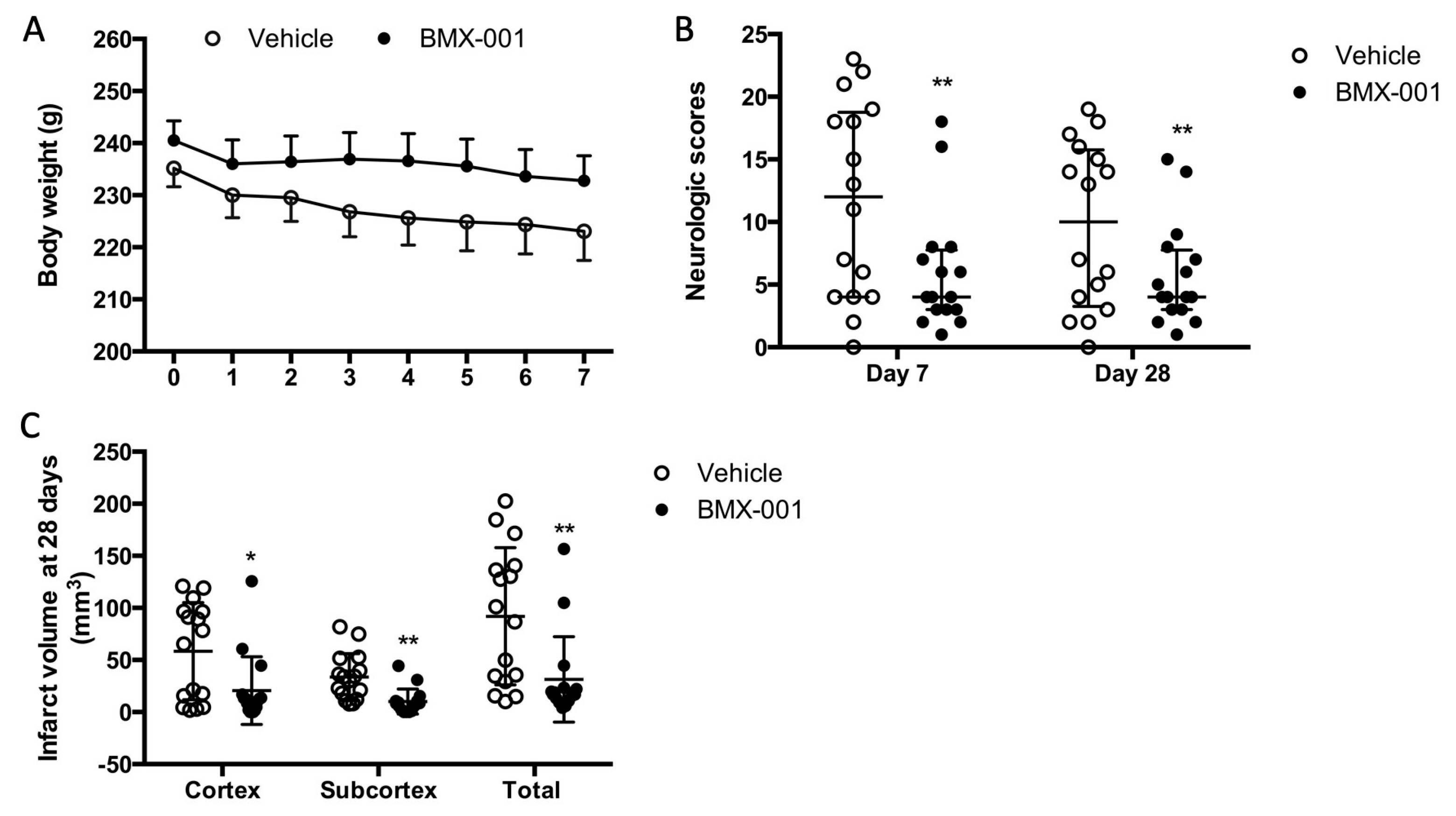
3.3. Experiment 3: Treatment with BMX-001 for 7 Days Provides 28-Day Post-Stroke Protection in Young Male Rats
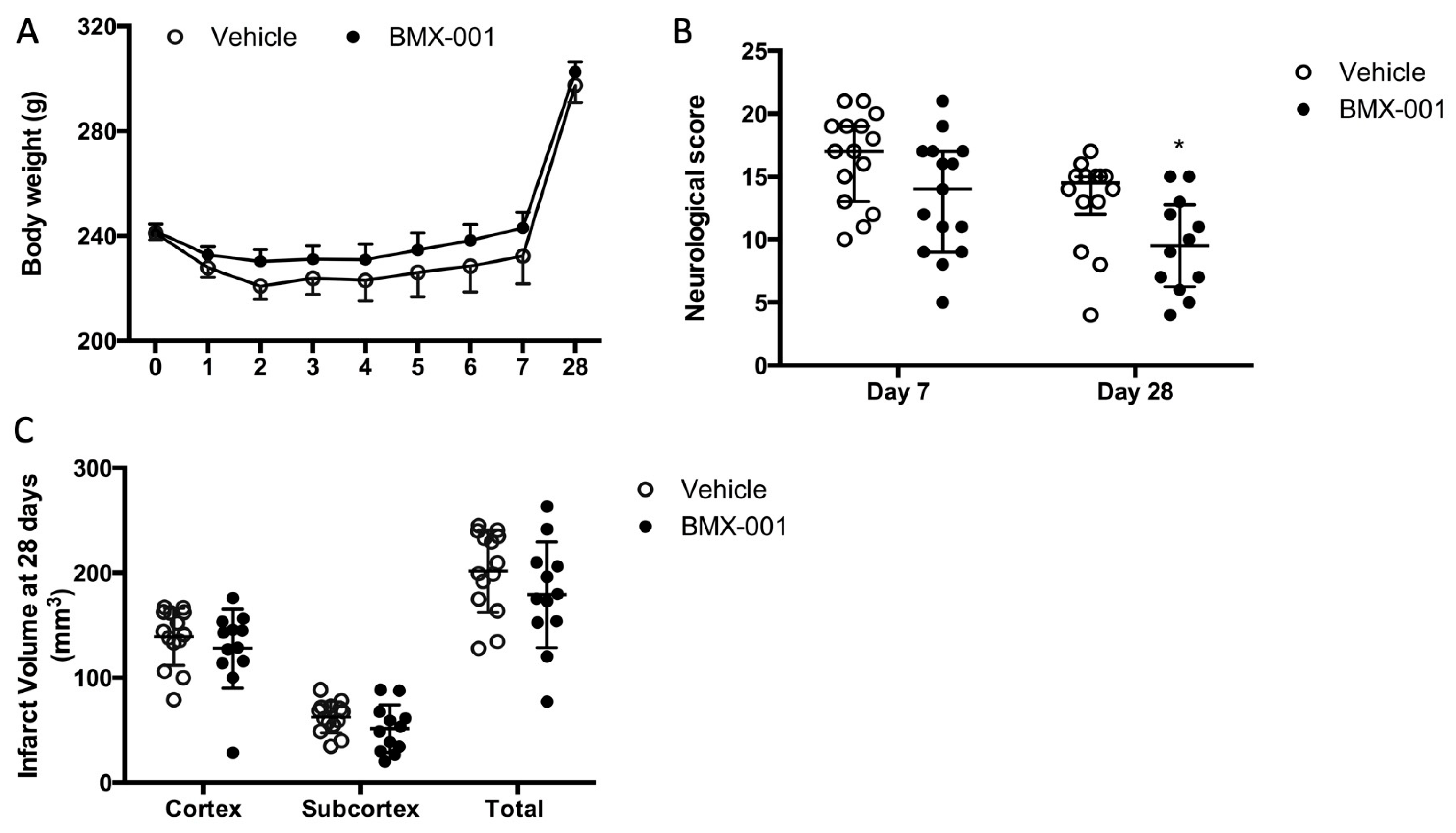
3.4. Experiment 4: BMX-001 Improved 28-Day Post-Stroke Functional Deficits in Spontaneous Hypertension Rats
3.5. Experiment 5: BMX-001 Improved 28-Day Post-Stroke Outcomes in Aged Female Rats
3.6. Experiment 6: BMX-001 Accumulated at the Site of Brain Injury
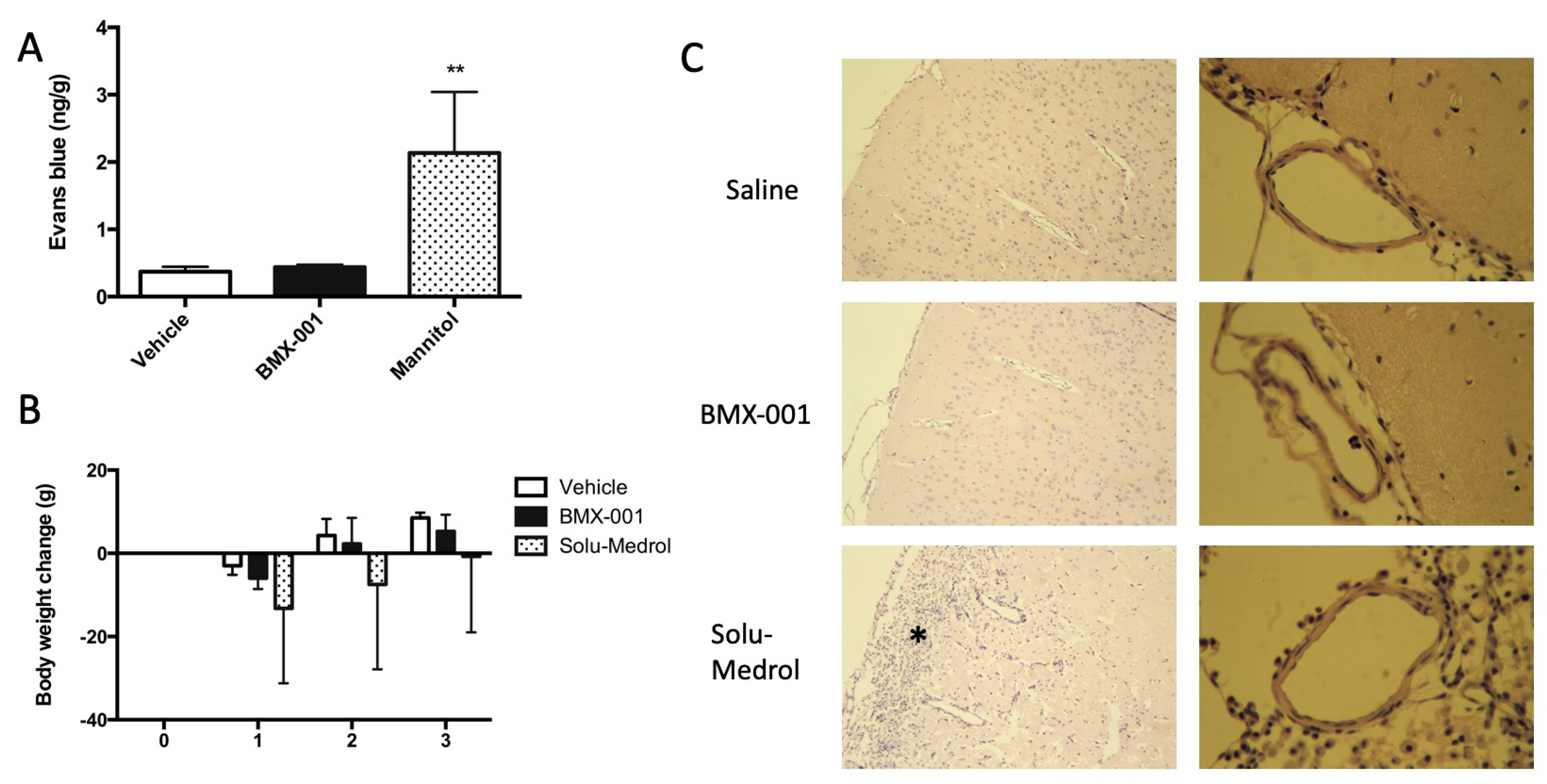
3.7. Experiment 7: Intracarotid BMX-001 Infusion Did Not Affect the Permeability and Vascular Structure of Blood–Brain Barrier
3.8. Experiment 8: No Evidence of an Interaction between BMX-001 and t-PA Was Found
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Grabb, M.C.; Zipfel, G.J.; Choi, D.W. Brain tissue responses to ischemia. J. Clin. Investig. 2000, 106, 723–731. [Google Scholar] [CrossRef] [PubMed]
- Astrup, J.; Siesjo, B.K.; Symon, L. Thresholds in cerebral ischemia—the ischemic penumbra. Stroke 1981, 12, 723–725. [Google Scholar] [CrossRef] [PubMed]
- Kiewert, C.; Mdzinarishvili, A.; Hartmann, J.; Bickel, U.; Klein, J. Metabolic and transmitter changes in core and penumbra after middle cerebral artery occlusion in mice. Brain Res. 2010, 1312, 101–107. [Google Scholar] [CrossRef]
- Shiraishi, K.; Sharp, F.R.; Simon, R.P. Sequential metabolic changes in rat brain following middle cerebral artery occlusion: A 2-deoxyglucose study. J. Cereb. Blood Flow. Metab. 1989, 9, 765–773. [Google Scholar] [CrossRef]
- National Institute of Neurological Disorders and Stroke. Tissue plasminogen activator for acute ischemic stroke. N. Engl. J. Med. 1995, 333, 1581–1587. [Google Scholar] [CrossRef]
- Tanne, D.; Gorman, M.J.; Bates, V.E.; Kasner, S.E.; Scott, P.; Verro, P.; Binder, J.R.; Dayno, J.M.; Schultz, L.R.; Levine, S.R. Intravenous tissue plasminogen activator for acute ischemic stroke in patients aged 80 years and older: The tPA stroke survey experience. Stroke 2000, 31, 370–375. [Google Scholar] [CrossRef]
- Saver, J.L.; Goyal, M.; Bonafe, A.; Diener, H.C.; Levy, E.I.; Pereira, V.M.; Albers, G.W.; Cognard, C.; Cohen, D.J.; Hacke, W.; et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N. Engl. J. Med. 2015, 372, 2285–2295. [Google Scholar] [CrossRef]
- Jovin, T.G.; Nogueira, R.G.; Lansberg, M.G.; Demchuk, A.M.; Martins, S.O.; Mocco, J.; Ribo, M.; Jadhav, A.P.; Ortega-Gutierrez, S.; Hill, M.D.; et al. Thrombectomy for anterior circulation stroke beyond 6 h from time last known well (AURORA): A systematic review and individual patient data meta-analysis. Lancet 2022, 399, 249–258. [Google Scholar] [CrossRef]
- Jovin, T.G.; Chamorro, A.; Cobo, E.; de Miquel, M.A.; Molina, C.A.; Rovira, A.; San Roman, L.; Serena, J.; Abilleira, S.; Ribo, M.; et al. Thrombectomy within 8 Hours after Symptom Onset in Ischemic Stroke. N. Engl. J. Med. 2015, 372, 2296–2306. [Google Scholar] [CrossRef]
- Campbell, B.C.V.; Donnan, G.A.; Mitchell, P.J.; Davis, S.M. Endovascular thrombectomy for stroke: Current best practice and future goals. Stroke Vasc. Neurol. 2016, 1, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Bracard, S.; Ducrocq, X.; Mas, J.L.; Soudant, M.; Oppenheim, C.; Moulin, T.; Guillemin, F.; on behalf of the THRACE investigators. Mechanical thrombectomy after intravenous alteplase versus alteplase alone after stroke (THRACE): A randomised controlled trial. Lancet Neurol. 2016, 15, 1138–1147. [Google Scholar] [CrossRef] [PubMed]
- Saver, J.L.; Chapot, R.; Agid, R.; Hassan, A.; Jadhav, A.P.; Liebeskind, D.S.; Lobotesis, K.; Meila, D.; Meyer, L.; Raphaeli, G.; et al. Thrombectomy for Distal, Medium Vessel Occlusions: A Consensus Statement on Present Knowledge and Promising Directions. Stroke 2020, 51, 2872–2884. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef]
- Albers, G.W.; Lansberg, M.G.; Brown, S.; Jadhav, A.P.; Haussen, D.C.; Martins, S.O.; Rebello, L.C.; Demchuk, A.M.; Goyal, M.; Ribo, M.; et al. Assessment of Optimal Patient Selection for Endovascular Thrombectomy Beyond 6 Hours After Symptom Onset: A Pooled Analysis of the AURORA Database. JAMA Neurol. 2021, 78, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Fonarow, G.C.; Smith, E.E.; Saver, J.L.; Reeves, M.J.; Hernandez, A.F.; Peterson, E.D.; Sacco, R.L.; Schwamm, L.H. Improving door-to-needle times in acute ischemic stroke: The design and rationale for the American Heart Association/American Stroke Association’s Target: Stroke initiative. Stroke 2011, 42, 2983–2989. [Google Scholar] [CrossRef]
- Henninger, N.; Fisher, M. Extending the Time Window for Endovascular and Pharmacological Reperfusion. Transl. Stroke Res. 2016, 7, 284–293. [Google Scholar] [CrossRef]
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.; Mitchell, P.J.; Demchuk, A.M.; Davalos, A.; Majoie, C.B.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- Albers, G.W.; Marks, M.P.; Kemp, S.; Christensen, S.; Tsai, J.P.; Ortega-Gutierrez, S.; McTaggart, R.A.; Torbey, M.T.; Kim-Tenser, M.; Leslie-Mazwi, T.; et al. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N. Engl. J. Med. 2018, 378, 708–718. [Google Scholar] [CrossRef]
- Zaidat, O.O.; Liebeskind, D.S.; Jadhav, A.P.; Ortega-Gutierrez, S.; Nguyen, T.N.; Haussen, D.C.; Yavagal, D.R.; Froehler, M.T.; Jahan, R.; Nogueira, R.G.; et al. Impact of Age and Alberta Stroke Program Early Computed Tomography Score 0 to 5 on Mechanical Thrombectomy Outcomes: Analysis From the STRATIS Registry. Stroke 2021, 52, 2220–2228. [Google Scholar] [CrossRef]
- Sheng, H.; Yang, W.; Fukuda, S.; Tse, H.M.; Paschen, W.; Johnson, K.; Batinic-Haberle, I.; Crapo, J.D.; Pearlstein, R.D.; Piganelli, J.; et al. Long-term neuroprotection from a potent redox-modulating metalloporphyrin in the rat. Free Radic. Biol. Med. 2009, 47, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Sheng, H.; Spasojevic, I.; Tse, H.M.; Jung, J.Y.; Hong, J.; Zhang, Z.; Piganelli, J.D.; Batinic-Haberle, I.; Warner, D.S. Neuroprotective efficacy from a lipophilic redox-modulating Mn(III) N-Hexylpyridylporphyrin, MnTnHex-2-PyP: Rodent models of ischemic stroke and subarachnoid hemorrhage. J. Pharmacol. Exp. Ther. 2011, 338, 906–916. [Google Scholar] [CrossRef] [PubMed]
- Batinic-Haberle, I.; Tovmasyan, A.; Huang, Z.; Duan, W.; Du, L.; Siamakpour-Reihani, S.; Cao, Z.; Sheng, H.; Spasojevic, I.; Alvarez Secord, A. H2O2-Driven Anticancer Activity of Mn Porphyrins and the Underlying Molecular Pathways. Oxid. Med. Cell. Longev. 2021, 2021, 6653790. [Google Scholar] [CrossRef] [PubMed]
- Batinic-Haberle, I.; Tovmasyan, A.; Spasojevic, I. Mn Porphyrin-Based Redox-Active Drugs: Differential Effects as Cancer Therapeutics and Protectors of Normal Tissue Against Oxidative Injury. Antioxid. Redox Signal. 2018, 29, 1691–1724. [Google Scholar] [CrossRef]
- Longa, E.Z.; Weinstein, P.R.; Carlson, S.; Cummins, R. Reversible middle cerebral artery occlusion without craniectomy in rats. Stroke 1989, 20, 84–91. [Google Scholar] [CrossRef]
- Leu, D.; Spasojevic, I.; Nguyen, H.; Deng, B.; Tovmasyan, A.; Weitner, T.; Sampaio, R.S.; Batinic-Haberle, I.; Huang, T.T. CNS bioavailability and radiation protection of normal hippocampal neurogenesis by a lipophilic Mn porphyrin-based superoxide dismutase mimic, MnTnBuOE-2-PyP(5). Redox Biol. 2017, 12, 864–871. [Google Scholar] [CrossRef]
- Badhiwala, J.H.; Nassiri, F.; Alhazzani, W.; Selim, M.H.; Farrokhyar, F.; Spears, J.; Kulkarni, A.V.; Singh, S.; Alqahtani, A.; Rochwerg, B.; et al. Endovascular Thrombectomy for Acute Ischemic Stroke: A Meta-analysis. JAMA 2015, 314, 1832–1843. [Google Scholar] [CrossRef]
- Berkhemer, O.A.; Majoie, C.B.; Dippel, D.W.; Investigators, M.C. Endovascular therapy for ischemic stroke. N. Engl. J. Med. 2015, 372, 2363. [Google Scholar] [CrossRef]
- Broderick, J.P.; Berkhemer, O.A.; Palesch, Y.Y.; Dippel, D.W.; Foster, L.D.; Roos, Y.B.; van der Lugt, A.; Tomsick, T.A.; Majoie, C.B.; van Zwam, W.H.; et al. Endovascular Therapy Is Effective and Safe for Patients with Severe Ischemic Stroke: Pooled Analysis of Interventional Management of Stroke III and Multicenter Randomized Clinical Trial of Endovascular Therapy for Acute Ischemic Stroke in the Netherlands Data. Stroke 2015, 46, 3416–3422. [Google Scholar] [CrossRef]
- Berkhemer, O.A.; van Zwam, W.H.; Dippel, D.W.; Investigators, M.C. Stent-Retriever Thrombectomy for Stroke. N. Engl. J. Med. 2015, 373, 1076. [Google Scholar] [CrossRef]
- Berkhemer, O.A.; Fransen, P.S.; Beumer, D.; van den Berg, L.A.; Lingsma, H.F.; Yoo, A.J.; Schonewille, W.J.; Vos, J.A.; Nederkoorn, P.J.; Wermer, M.J.; et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N. Engl. J. Med. 2015, 372, 11–20. [Google Scholar] [CrossRef]
- Kaesmacher, J.; Bellwald, S.; Dobrocky, T.; Meinel, T.R.; Piechowiak, E.I.; Goeldlin, M.; Kurmann, C.C.; Heldner, M.R.; Jung, S.; Mordasini, P.; et al. Safety and Efficacy of Intra-arterial Urokinase After Failed, Unsuccessful, or Incomplete Mechanical Thrombectomy in Anterior Circulation Large-Vessel Occlusion Stroke. JAMA Neurol. 2020, 77, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Castonguay, A.C.; Jumaa, M.A.; Zaidat, O.O.; Haussen, D.C.; Jadhav, A.; Salahuddin, H.; Zaidi, S.F. Insights Into Intra-arterial Thrombolysis in the Modern Era of Mechanical Thrombectomy. Front. Neurol. 2019, 10, 1195. [Google Scholar] [CrossRef] [PubMed]
- Heiferman, D.M.; Li, D.D.; Pecoraro, N.C.; Smolenski, A.M.; Tsimpas, A.; Ashley, W.W., Jr. Intra-Arterial Alteplase Thrombolysis during Mechanical Thrombectomy for Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2017, 26, 3004–3008. [Google Scholar] [CrossRef] [PubMed]
- Mackensen, G.B.; Patel, M.; Sheng, H.; Calvi, C.L.; Batinic-Haberle, I.; Day, B.J.; Liang, L.P.; Fridovich, I.; Crapo, J.D.; Pearlstein, R.D.; et al. Neuroprotection from delayed postischemic administration of a metalloporphyrin catalytic antioxidant. J. Neurosci. 2001, 21, 4582–4592. [Google Scholar] [CrossRef]
- Rajic, Z.; Tovmasyan, A.; Spasojevic, I.; Sheng, H.; Lu, M.; Li, A.M.; Gralla, E.B.; Warner, D.S.; Benov, L.; Batinic-Haberle, I. A new SOD mimic, Mn(III) ortho N-butoxyethylpyridylporphyrin, combines superb potency and lipophilicity with low toxicity. Free Radic. Biol. Med. 2012, 52, 1828–1834. [Google Scholar] [CrossRef]
- Batinic-Haberle, I.; Tome, M.E. Thiol regulation by Mn porphyrins, commonly known as SOD mimics. Redox Biol. 2019, 25, 101139. [Google Scholar] [CrossRef]
- O’Neill, L.A.; Kaltschmidt, C. NF-κB: A crucial transcription factor for glial and neuronal cell function. Trends Neurosci. 1997, 20, 252–258. [Google Scholar] [CrossRef]
- Harari, O.A.; Liao, J.K. NF-κB and innate immunity in ischemic stroke. Ann. N. Y. Acad. Sci. 2010, 1207, 32–40. [Google Scholar] [CrossRef]
- Schneider, A.; Martin-Villalba, A.; Weih, F.; Vogel, J.; Wirth, T.; Schwaninger, M. NF-κB is activated and promotes cell death in focal cerebral ischemia. Nat. Med. 1999, 5, 554–559. [Google Scholar] [CrossRef]
- Zhang, W.; Potrovita, I.; Tarabin, V.; Herrmann, O.; Beer, V.; Weih, F.; Schneider, A.; Schwaninger, M. Neuronal activation of NF-κB contributes to cell death in cerebral ischemia. J. Cereb. Blood Flow. Metab. 2005, 25, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Dorai, T.; Fishman, A.I.; Ding, C.; Batinic-Haberle, I.; Goldfarb, D.S.; Grasso, M. Amelioration of renal ischemia-reperfusion injury with a novel protective cocktail. J. Urol. 2011, 186, 2448–2454. [Google Scholar] [CrossRef] [PubMed]
- Sheng, H.; Enghild, J.J.; Bowler, R.; Patel, M.; Batinic-Haberle, I.; Calvi, C.L.; Day, B.J.; Pearlstein, R.D.; Crapo, J.D.; Warner, D.S. Effects of metalloporphyrin catalytic antioxidants in experimental brain ischemia. Free Radic. Biol. Med. 2002, 33, 947–961. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Carroll, D.W.; You, Y.; Chaiswing, L.; Wen, R.; Batinic-Haberle, I.; Bondada, S.; Liang, Y.; St Clair, D.K. A novel redox regulator, MnTnBuOE-2-PyP(5+), enhances normal hematopoietic stem/progenitor cell function. Redox Biol. 2017, 12, 129–138. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vehicle n = 19 | 7 Days of BMX-001 n = 19 | 28 Days of BMX-001 n = 19 | |
|---|---|---|---|
| 10 min before stroke | |||
| MAP (mmHg) | 76 ± 7 | 75 ± 9 | 75 ± 7 |
| pH | 7.476 ± 0.034 | 7.481 ± 0.033 | 7.487 ± 0.039 |
| PCO2 | 36 ± 5 | 36 ± 3 | 35 ± 4 |
| PO2 | 157 ± 32 | 168 ± 18 | 172 ± 13 |
| Glucose | 109 ± 17 | 104 ± 19 | 110 ± 17 |
| Hct | 42.6 ± 1.6 | 42.6 ± 1.4 | 42.2 ± 1.3 |
| 45 min after stroke onset | |||
| MAP (mmHg) | 72 ± 9 | 69 ± 7 | 69 ± 7 |
| pH | 7.450 ± 0.035 | 7.462 ± 0.048 | 7.433 ± 0.049 |
| PCO2 | 38 ± 4 | 37 ± 6 | 39 ± 6 |
| PO2 | 162 ± 21 | 162 ± 17 | 162 ± 17 |
| 10 min post-stroke | |||
| MAP (mmHg) | 71 ± 6 | 67 ± 5 | 71 ± 6 |
| Vehicle n = 15 | BMX-001 n = 15 | p | |
|---|---|---|---|
| 10 min before stroke | |||
| MAP (mmHg) | 127 ± 16 | 124 ± 20 | 0.58 |
| pH | 7.402 ± 0.023 | 7.384 ± 0.046 | 0.19 |
| PCO2 | 39 ± 3 | 41 ± 6 | 0.38 |
| PO2 | 173 ± 24 | 175 ± 18 | 0.72 |
| Glucose | 97 ± 31 | 93 ± 30 | 0.71 |
| Hct | 48 ± 3 | 48 ± 3 | 0.76 |
| 45 min after stroke onset | |||
| MAP (mmHg) | 91 ± 13 | 90 ± 9 | 0.93 |
| pH | 7.379 ± 0.027 | 7.375 ± 0.038 | 0.71 |
| PCO2 | 42 ± 4 | 42 ± 5 | 0.83 |
| PO2 | 170 ± 16 | 175 ± 15 | 0.37 |
| 10 min post-stroke | |||
| MAP (mmHg) | 89 ± 9 | 83 ± 11 | 0.15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, X.; Duan, W.; Du, L.; Chu, D.; Wang, P.; Yang, Z.; Qu, X.; Yang, Z.; Batinic-Haberle, I.; Spasojevic, I.; et al. Intracarotid Infusion of Redox-Active Manganese Porphyrin, MnTnBuOE-2-PyP5+, following Reperfusion Improves Long-Term, 28-Day Post-Stroke Outcomes in Rats. Antioxidants 2023, 12, 1861. https://doi.org/10.3390/antiox12101861
Li X, Duan W, Du L, Chu D, Wang P, Yang Z, Qu X, Yang Z, Batinic-Haberle I, Spasojevic I, et al. Intracarotid Infusion of Redox-Active Manganese Porphyrin, MnTnBuOE-2-PyP5+, following Reperfusion Improves Long-Term, 28-Day Post-Stroke Outcomes in Rats. Antioxidants. 2023; 12(10):1861. https://doi.org/10.3390/antiox12101861
Chicago/Turabian StyleLi, Xuan, Weina Duan, Li Du, Dongmei Chu, Peng Wang, Zhong Yang, Xingguang Qu, Zhenxing Yang, Ines Batinic-Haberle, Ivan Spasojevic, and et al. 2023. "Intracarotid Infusion of Redox-Active Manganese Porphyrin, MnTnBuOE-2-PyP5+, following Reperfusion Improves Long-Term, 28-Day Post-Stroke Outcomes in Rats" Antioxidants 12, no. 10: 1861. https://doi.org/10.3390/antiox12101861