Attitude in Radiographic Post-Operative Assessment of Dental Implants among Italian Dentists: A Cross-Sectional Survey



Abstract
:1. Introduction
2. Results
2.1. Participants
2.2. Type and Frequency of X-ray
2.3. Retrograde Peri-implantitis
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Study Population
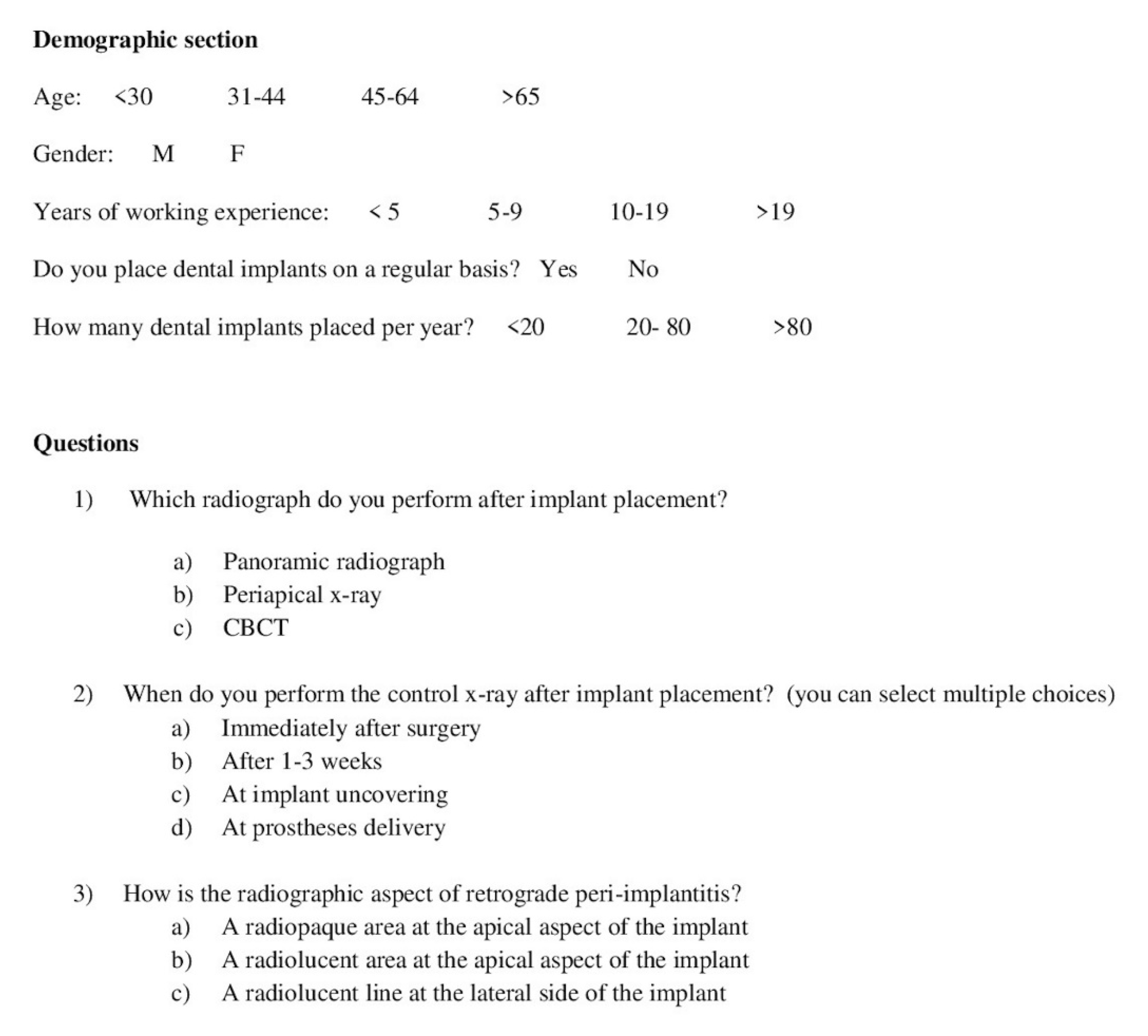
4.3. Survey
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- De Angelis, F.; Papi, P.; Mencio, F.; Rosella, D.; Di Carlo, S.; Pompa, G. Implant survival and success rates in patients with risk factors: Results from a long-term retrospective study with a 10 to 18 years follow-up. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 433–437. [Google Scholar] [PubMed]
- Manicone, P.F.; Passarelli, P.C.; Bigagnoli, S.; Pastorino, R.; Manni, A.; Pasquantonio, G.; D’Addona, A. Clinical and radiographic assessment of implant-supported rehabilitation of partial and complete edentulism: A 2 to 8 years clinical follow-up. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 4045–4052. [Google Scholar] [PubMed]
- Papi, P.; Di Carlo, S.; Mencio, F.; Rosella, D.; De Angelis, F.; Pompa, G. Dental Implants Placed in Patients with Mechanical Risk Factors: A Long-term Follow-up Retrospective Study. J. Int. Soc. Prev. Community Dent. 2017, 7 (Suppl. 1), S48–S51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, Q.; Zhang, L.; Geraets, W.; Wu, W.; Zhou, Y.; Wismeijer, D.; Xie, Q. Association between peri-implant bone morphology and marginal bone loss: A retrospective study on implant-supported mandibular overdentures. Int. J. Oral. Maxillofac. Implant. 2017, 32, 147–155. [Google Scholar] [CrossRef] [Green Version]
- De Bruin, H.; Vandeweghe, S.; Ruyffelaert, C.; Cosyn, J.; Sennerby, L. Radiographic evaluation of modern oral implants with emphasis on crestal bone level and relevance to peri-implant health. Periodontol 2000 2013, 62, 256–270. [Google Scholar] [CrossRef]
- Sirin, Y.; Horasan, S.; Yaman, D.; Basegmez, C.; Tanyel, C.; Aral, A.; Guven, K. Detection of crestal radiolucencies around dental implants: An in vitro experimental study. J. Oral. Maxillofac. Surg. 2012, 70, 1540–1550. [Google Scholar] [CrossRef]
- Pan, Y.H.; Lin, H.K.; Lin, J.C.; Hsu, Y.S.; Wu, Y.F.; Salamanca, E.; Chang, W.J. Evaluation of the Peri-Implant Bone Level around Platform-Switched Dental Implants: A Retrospective 3-Year Radiographic Study. Int. J. Environ. Res. Pub. Health 2019, 18, 2570. [Google Scholar] [CrossRef] [Green Version]
- Kamburoğlu, K.; Murat, S.; Kiliç, C.; Yüksel, S.; Avsever, H.; Farman, A.; Scarfe, W.C. Accuracy of CBCT images in the assessment of buccal marginal alveolar peri-implant defects: Effect of field of view. Dentomaxillofac. Radiol. 2014, 43, 20130332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vadiati Saberi, B.; Khosravifard, N.; Ghandari, F.; Hadinezhad, A. Detection of peri-implant bone defects using cone-beam computed tomography and digital periapical radiography with parallel and oblique projection. Imaging Sci. Dent. 2019, 49, 265–272. [Google Scholar] [CrossRef]
- Omami, G. Cone-Beam Computed Tomography in Implant Dentistry: Back to the Future. J. Oral. Maxillofac. Surg. 2017, 75, 655. [Google Scholar] [CrossRef]
- Graham, J.; Coucke, W.; Roberts, M.; Quirynen, M.; Jacobs, R.; Devlin, H. Prediction of implant loss and marginal bone loss by analysis of dental panoramic radiographs. Int. J. Oral. Maxillofac. Implant. 2015, 30, 372–377. [Google Scholar]
- Aanenson, J.W.; Till, J.E.; Grogan, H.A. Understanding and communicating radiation dose and risk from cone beam computed tomography in dentistry. J. Prosthet. Dent. 2018, 120, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, R.; Quirynen, M. Dental cone beam computed tomography: Justification for use in planning oral implant placement. Periodontol 2000 2014, 66, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, R.; Jacobs, R.; Singer, S.R.; Mupparapu, M. CBCT-based bone quality assessment: Are Hounsfield units applicable? Dentomaxillofac. Radiol. 2015, 44, 20140238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deeb, G.; Antonos, L.; Tack, S.; Carrico, C.; Laskin, D.; Deeb, J.G. Is Cone-Beam Computed Tomography Always Necessary for Dental Implant Placement? J. Oral. Maxillofac. Surg. 2017, 75, 285–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joda, T.; Gallucci, G.O. The virtual patient in dental medicine. Clin. Oral. Implant. Res. 2015, 26, 725–726. [Google Scholar] [CrossRef] [PubMed]
- Vidor, M.M.; Liedke, G.S.; Fontana, M.P.; da Silveira, H.L.D.; Arus, N.A.; Lemos, A.; Vizzotto, M.B. Is cone beam computed tomography accurate for postoperative evaluation of implants? An in vitro study. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2017, 124, 500–505. [Google Scholar] [CrossRef]
- Papi, P.; Brauner, E.; Di Carlo, S.; Musio, D.; Tombolini, M.; De Angelis, F.; Valentini, V.; Tombolini, V.; Polimeni, A.; Pompa, G. Crestal bone loss around dental implants placed in head and neck cancer patients treated with different radiotherapy techniques: A prospective cohort study. Int. J. Oral. Maxillofac. Surg. 2019, 48, 691–696. [Google Scholar] [CrossRef]
- Lurie, A.G. Doses, Benefits, Safety, and Risks in Oral and Maxillofacial Diagnostic Imaging. Health Phys. 2019, 116, 163–169. [Google Scholar] [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. 1), S313–S318. [Google Scholar] [CrossRef]
- Di Murro, B.; Papi, P.; Pompa, G. Surgical management of acute retrograde peri-implantitis: A review of current literature. Ann. Stomatol. 2018, 9, 106–109. [Google Scholar]
- Flanagan, D. Implant placement in failed endodontic sites: A review. J. Oral. Implant. 2016, 42, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Sarmast, N.D.; Wang, H.H.; Soldatos, N.K.; Angelov, N.; Dorn, S.; Yukna, R.; Iacono, V.J. A Novel Treatment Decision Tree and Literature Review of Retrograde Peri-Implantitis. J. Periodontol. 2016, 87, 1458–1467. [Google Scholar] [CrossRef] [PubMed]
- Sarmast, N.D.; Wang, H.H.; Sajadi, A.S.; Angelov, N.; Dorn, S.O. Classification and clinical management of retrograde peri-implantitis associated with apical periodontitis: A proposed classification system and case report. J. Endod. 2017, 43, 1921–1924. [Google Scholar] [CrossRef]
- Peñarrocha-Oltra, D.; Blaya-Tárraga, J.A.; Menéndez-Nieto, I.; Peñarrocha-Diago, M.; Peñarrocha-Diago, M. Factors associated with early apical peri-implantitis: A retrospective study covering a 20-year period. Int. J. Oral. Implantol. 2020, 13, 65–73. [Google Scholar]
- Ramakrishnan, P.; Shafi, F.M.; Subhash, A.; Kumara, A.; Chakkarayan, J.; Vengalath, J. A survey on radiographic prescription practices in dental implant assessment among dentists in Kerala. Oral. Health Dent. Manag. 2014, 13, 826–830. [Google Scholar]
- Sakakura, C.E.; Morais, J.A.; Loffredo, L.C.; Scaf, G. A survey of radiographic prescription in dental implant assessment. Dentomaxillofac. Radiol. 2003, 32, 397–400. [Google Scholar] [CrossRef] [Green Version]
- Bornstein, M.M.; Horner, K.; Jacobs, R. The use of cone beam computed tomography (CBCT) in implant dentistry: Current concepts, indications and limitations for clinical practice and research. Periodontol 2000 2017, 73, 51–72. [Google Scholar] [CrossRef]
- Jacobs, R.; Salmon, B.; Codari, M.; Hassan, B.; Bornstein, M.M. Cone beam computed tomography in implant dentistry: Recommendations for clinical use. BMC Oral. Health 2018, 18, 88. [Google Scholar] [CrossRef] [Green Version]
- Farman, A.G. ALARA still applies. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2005, 100, 395–397. [Google Scholar] [CrossRef]
- Tyndall, D.A.; Price, J.B.; Tetradis, S.; Ganz, S.D.; Hildebolt, C.; Scarfe, W.C. Position statement of the American Academy of Oral and Maxillofacial Radiology on selection criteria for the use of radiology in dental implantology with emphasis on cone beam computed tomography. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2012, 113, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Nagarajan, A.; Perumalsamy, R.; Thyagarajan, R.; Namasivayam, A. Diagnostic imaging for dental implant therapy. J. Clin. Imaging Sci. 2014, 4, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | N | % |
|---|---|---|
| Gender | - | - |
| Male | 386 | 88.9 |
| Female | 48 | 11.1 |
| Age range | - | - |
| < 30 years | 78 | 17.9 |
| 30–44 years | 114 | 26.3 |
| 45–64 years | 218 | 50.3 |
| > 65 years | 24 | 5.5 |
| Years of working experience | - | - |
| < 5 years | 74 | 17.1 |
| 5–9 years | 60 | 13.8 |
| 10–19 years | 106 | 24.5 |
| > 19 years | 194 | 44.6 |
| Number of implants/year | - | - |
| < 20 | 114 | 26.2 |
| 20–80 | 214 | 49.3 |
| > 80 | 106 | 24.5 |
| Variable | PAN | Periapical | CBCT | p Value | Overall p Value | ||
|---|---|---|---|---|---|---|---|
| Gender | |||||||
| Male | 36 | 322 | 28 | 0.701 | 0.158 | < 0.0001 * | 0.524 |
| Female | 2 | 44 | 2 | 0.194 | 0.469 | 0.324 | |
| Age range | |||||||
| < 30 years | 2 | 70 | 6 | 0.039 * | 0.443 | 0.945 | 0.265 |
| 30–44 years | 10 | 100 | 4 | 0.816 | 0.060 | 0.118 | |
| 45–64 years | 26 | 174 | 18 | 0.154 | 0.309 | 0.611 | |
| > 65 years | 0 | 22 | 2 | < 0.0001 * | 0.823 | 0.827 | |
| Years of working experience | |||||||
| < 5 years | 2 | 66 | 6 | 0.048 * | 0.535 | 0.976 | 0.527 |
| 5–9 years | 8 | 50 | 2 | 0.515 | 0.401 | 0.198 | |
| 10–19 years | 6 | 92 | 8 | 0.222 | 0.745 | 0.957 | |
| > 19 years | 22 | 158 | 14 | 0.332 | 0.215 | 0.918 | |
| Number of implants/year | |||||||
| < 20 | 6 | 100 | 8 | 0.157 | 0.543 | 0.813 | 0.687 |
| 20–80 | 18 | 180 | 14 | 0.694 | 0.946 | 0.647 | |
| > 80 | 14 | 84 | 8 | 0.305 | 0.176 | 0.948 | |
| Variable | Other | Correct | p Value | Overall p Value | |
|---|---|---|---|---|---|
| Gender | |||||
| Male | 200 | 186 | 0.996 | 0.702 | 0.545 |
| Female | 28 | 20 | 0.641 | 0.413 | |
| Age range | |||||
| < 30 years | 40 | 36 | 0.891 | 0.826 | 0.316 |
| 30–44 years | 52 | 62 | 0.182 | 0.305 | |
| 45–64 years | 117 | 103 | 0.897 | 0.687 | |
| > 65 years | 18 | 6 | 0.183 | 0.050 * | |
| Years of working experience | |||||
| < 5 years | 40 | 32 | 0.809 | 0.544 | 0.484 |
| 5–9 years | 24 | 36 | 0.098 | 0.208 | |
| 10–19 years | 54 | 52 | 0.697 | 0.942 | |
| > 19 years | 109 | 87 | 0.451 | 0.304 | |
| Number of implants/year | |||||
| < 20 | 64 | 48 | 0.521 | 0.340 | 0.044 * |
| 20–80 | 124 | 92 | 0.191 | 0.114 | |
| > 80 | 40 | 66 | 0.008 * | 0.020 * | |
| Variable | Radiopaque Apical | Radiolucent Apical | Radiolucent Lateral | p Value | Overall p Value | ||
|---|---|---|---|---|---|---|---|
| Gender | |||||||
| Male | 34 | 292 | 60 | 0.747 | 0.498 | 0.067 | 0.248 |
| Female | 2 | 32 | 14 | 0.214 | 0.251 | 0.187 | |
| Age range | |||||||
| < 30 years | 5 | 62 | 11 | 0.267 | 0.355 | 0.328 | 0.310 |
| 30–44 years | 7 | 86 | 19 | 0.222 | 0.111 | 0.691 | |
| 45–64 years | 27 | 154 | 39 | 0.098 | 0.160 | 0.900 | |
| > 65 years | 0 | 16 | 8 | < 0.0001 * | 0.333 | 0.266 | |
| Years of working experience | |||||||
| < 5 years | 7 | 62 | 5 | 0.773 | 0.107 | 0.011 * | 0.081 |
| 5–9 years | 0 | 46 | 10 | < 0.0001 * | 0.070 | 0.890 | |
| 10–19 years | 11 | 72 | 25 | 0.948 | 0.163 | 0.327 | |
| > 19 years | 21 | 138 | 37 | 0.506 | 0.262 | 0.789 | |
| Number of implants/year | |||||||
| < 20 | 5 | 88 | 21 | 0.051 | 0.491 | 0.943 | 0.107 |
| 20–80 | 25 | 141 | 45 | 0.181 | 0.016 * | 0.214 | |
| > 80 | 9 | 89 | 11 | 0.599 | 0.124 | 0.039 * | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Murro, B.; Papi, P.; Passarelli, P.C.; D’Addona, A.; Pompa, G. Attitude in Radiographic Post-Operative Assessment of Dental Implants among Italian Dentists: A Cross-Sectional Survey. Antibiotics 2020, 9, 234. https://doi.org/10.3390/antibiotics9050234
Di Murro B, Papi P, Passarelli PC, D’Addona A, Pompa G. Attitude in Radiographic Post-Operative Assessment of Dental Implants among Italian Dentists: A Cross-Sectional Survey. Antibiotics. 2020; 9(5):234. https://doi.org/10.3390/antibiotics9050234
Chicago/Turabian StyleDi Murro, Bianca, Piero Papi, Pier Carmine Passarelli, Antonio D’Addona, and Giorgio Pompa. 2020. "Attitude in Radiographic Post-Operative Assessment of Dental Implants among Italian Dentists: A Cross-Sectional Survey" Antibiotics 9, no. 5: 234. https://doi.org/10.3390/antibiotics9050234