Candida albicans Biofilm Heterogeneity and Tolerance of Clinical Isolates: Implications for Secondary Endodontic Infections


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Material and Methods
2.1. Microbial Growth Conditions and Standardisation
2.2. Biofilm Development and Biofilm Forming Ability Characterisation
2.3. Planktonic Minimum Inhibitory Concentration (MIC)
2.4. Biofilm Treatment and Regrowth Assessment
2.5. Statistical Analysis
3. Results
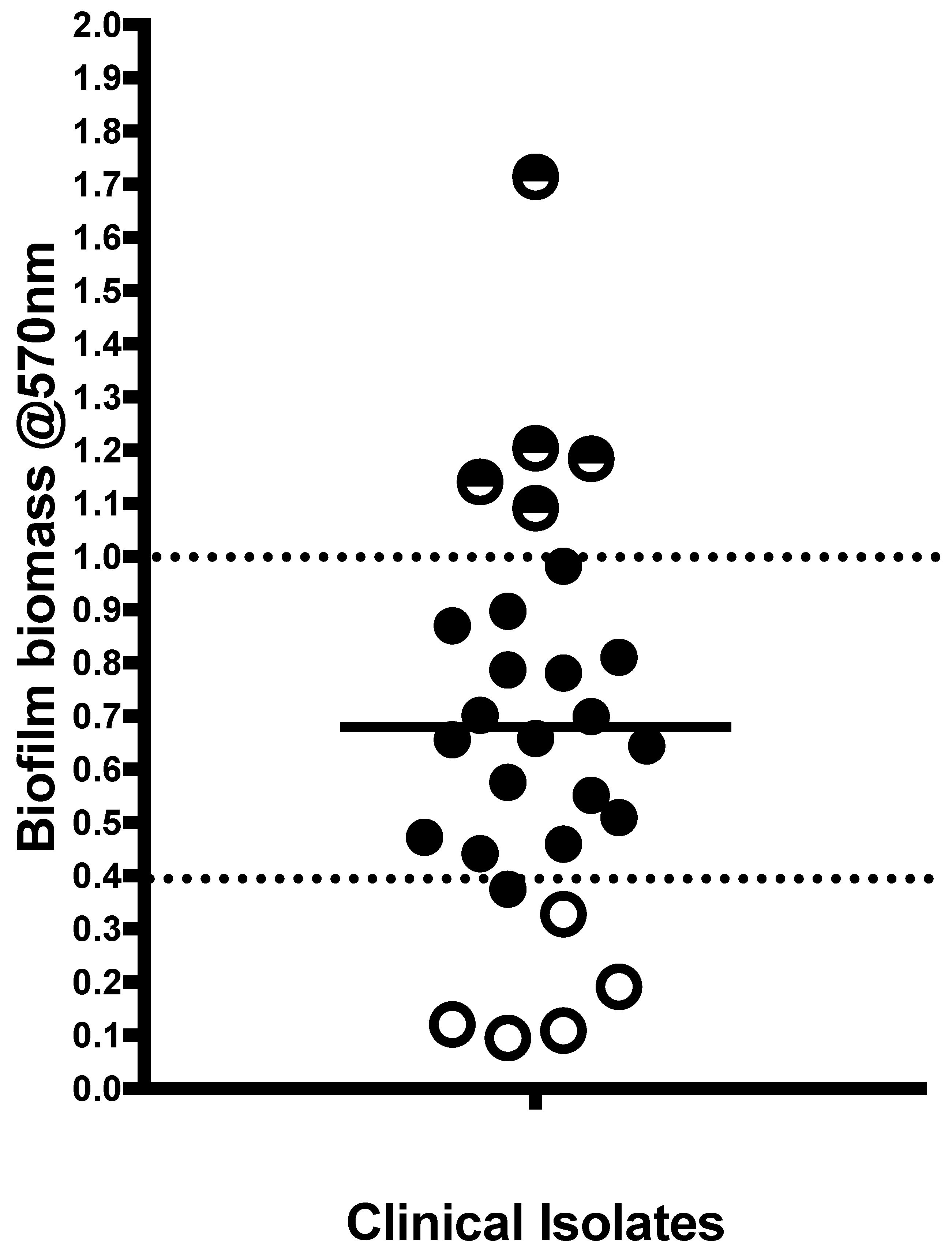
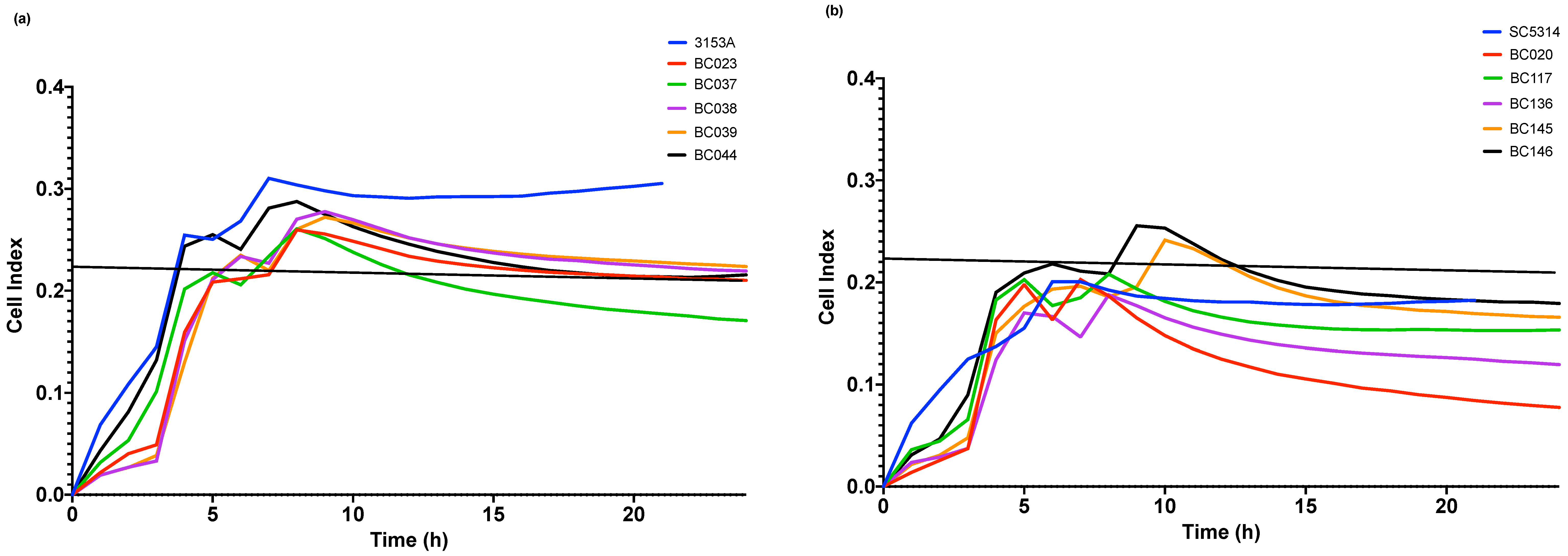
3.1. Oral Candida albicans differentially form biofilms and are NaOCl sensitive
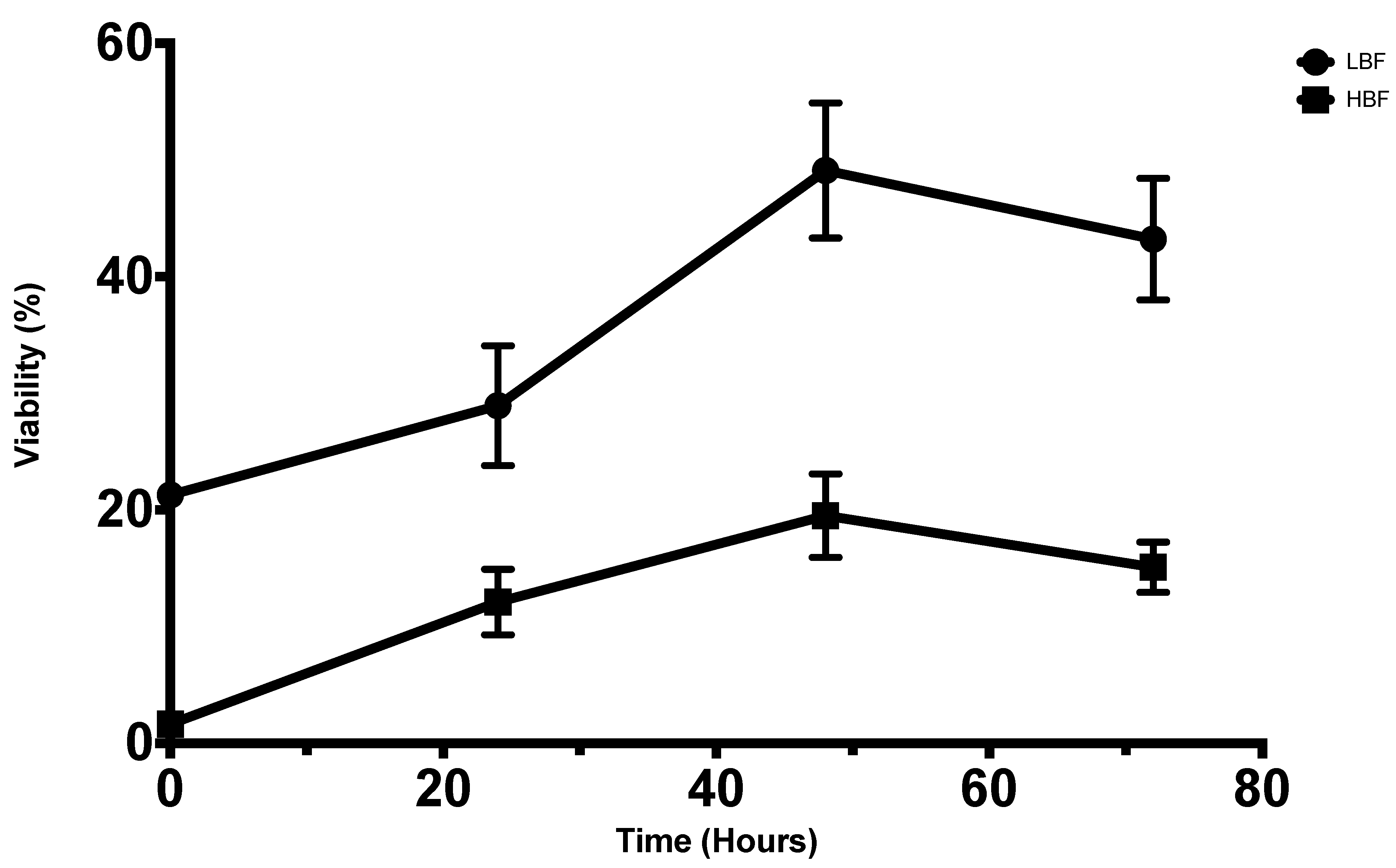
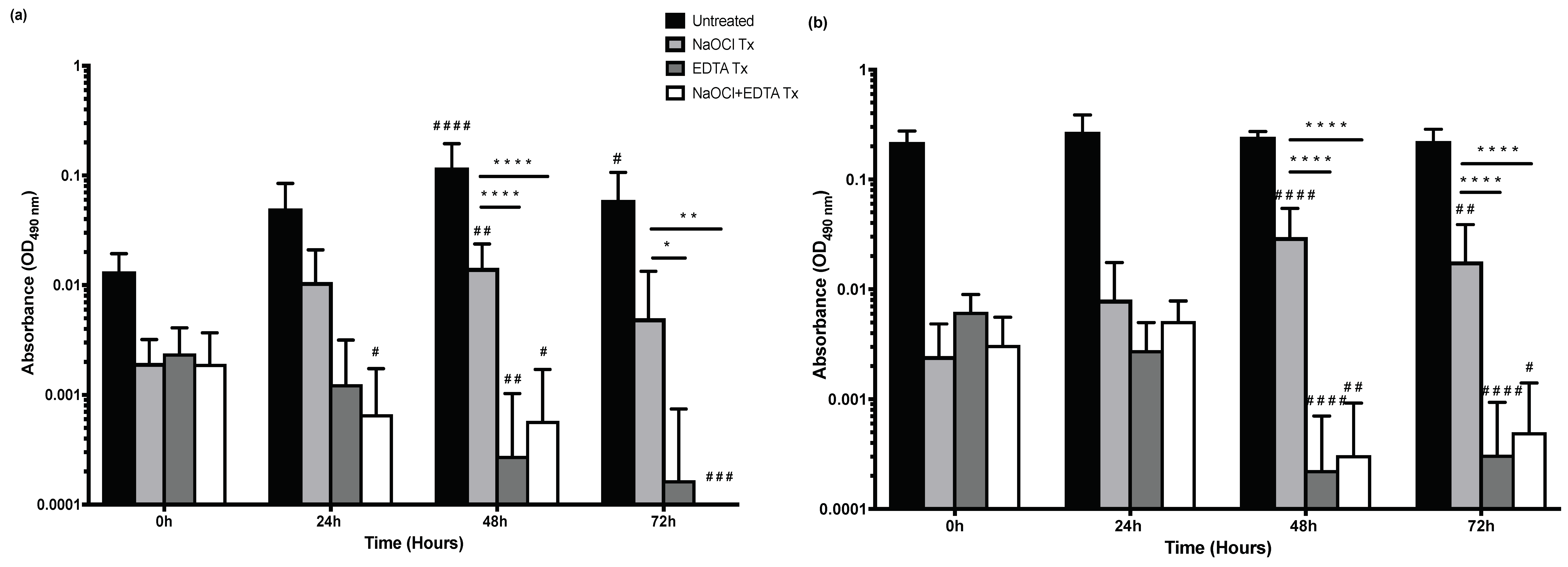
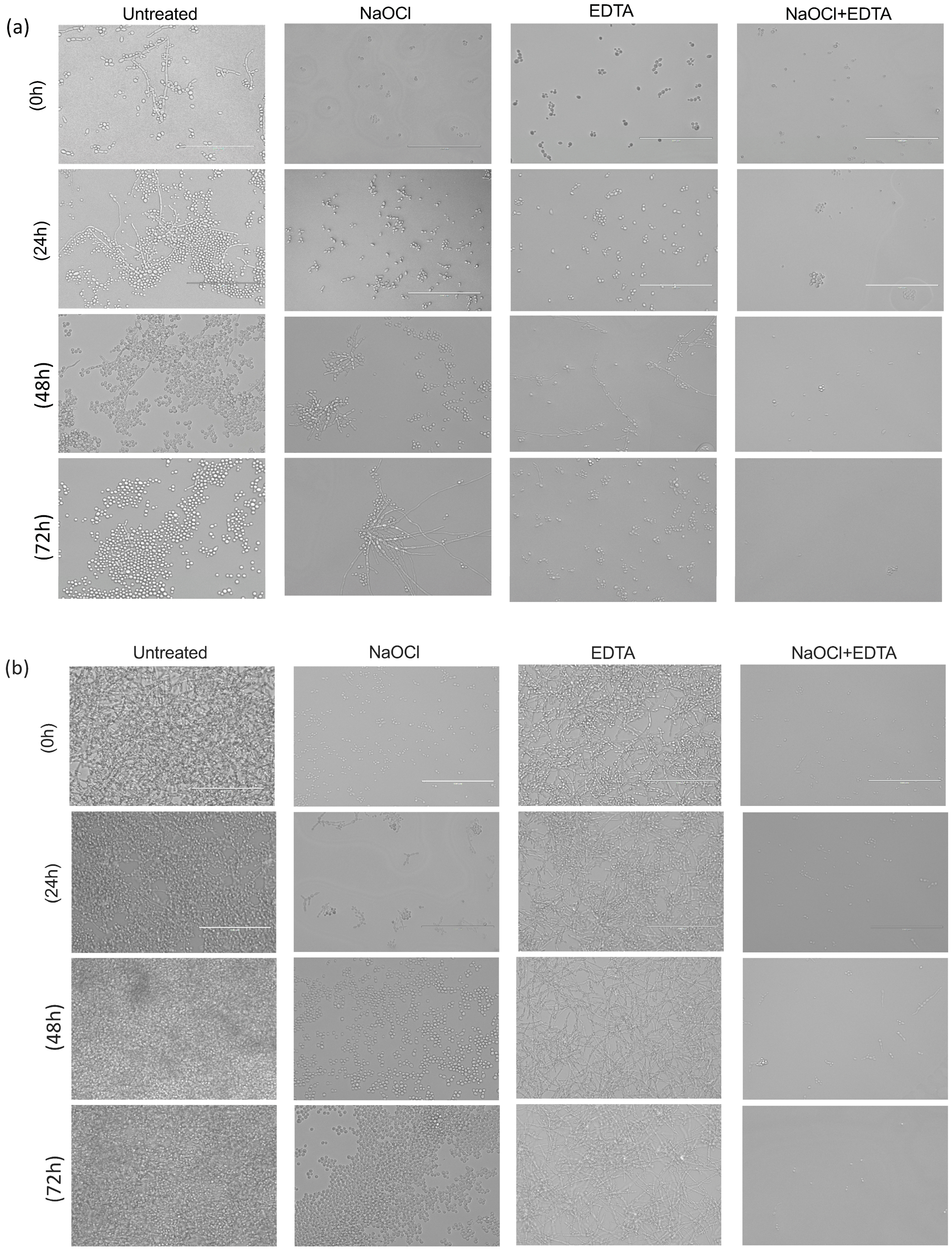
3.2. Oral Candida albicans persistsfFollowing NaOCl treatment
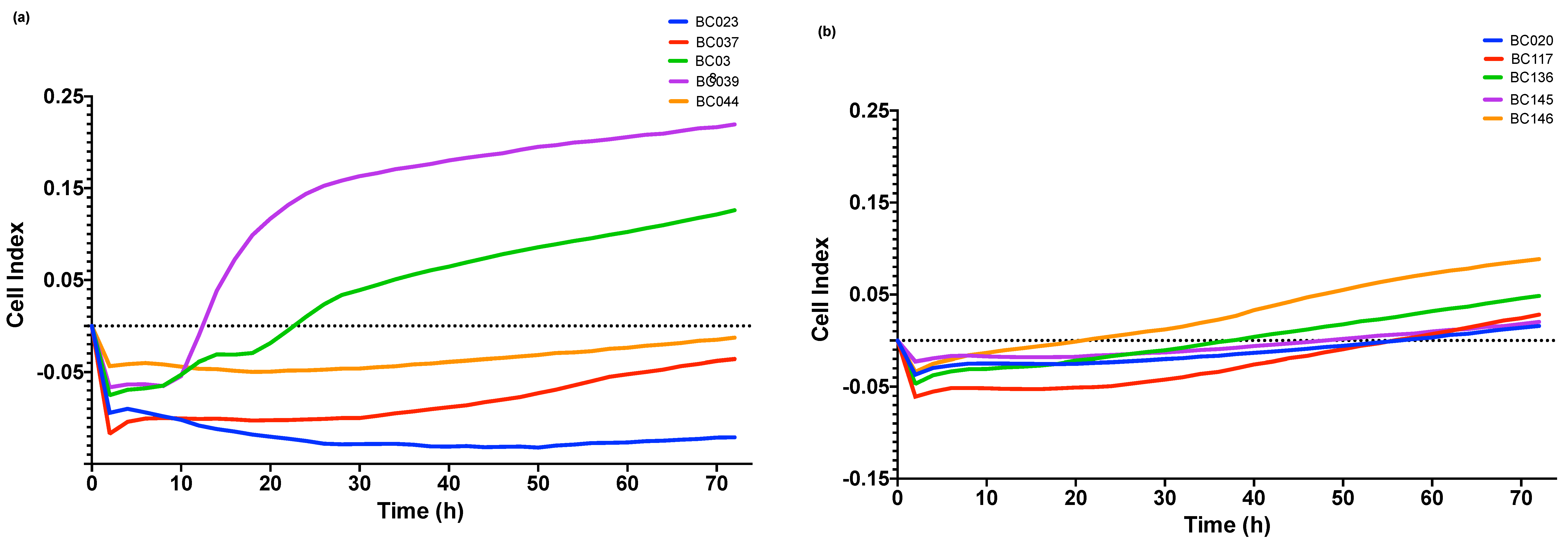
3.3. Oral Candida albicans regrowth after NaOCl treatment is significantly inhibited by EDTA
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gow, N.A.; Netea, M.G. Medical mycology and fungal immunology: New research perspectives addressing a major world health challenge. Philos. Trans. R. Soc. B Biol. Sci. 2016, 371, 20150462. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M.C.; Hawkins, N.J.; Sanglard, D.; Gurr, S.J. Worldwide emergence of resistance to antifungal drugs challenges human health and food security. Science 2018, 360, 739–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramage, G.; Saville, S.P.; Thomas, D.P.; Lopez-Ribot, J.L. Candida biofilms: An update. Eukaryot. Cell 2005, 4, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F., Jr.; Rôças, I.N. Polymerase chain reaction–based analysis of microorganisms associated with failed endodontic treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2004, 97, 85–94. [Google Scholar] [CrossRef]
- Widmer, C.; Skutas, J.; Easson, C.; Lopez, J.V.; Torneck, C.; Flax, M.; Sayin, T.C. Culture-independent Characterization of the Microbiome of Healthy Pulp. J. Endod. 2018, 44, 1132–1139. e2. [Google Scholar] [CrossRef]
- Yu, C.; Abbott, P.V. An overview of the dental pulp: Its functions and responses to injury. Aust. Dent. J. 2007, 52, S4–S16. [Google Scholar] [CrossRef]
- Mergoni, G.; Percudani, D.; Lodi, G.; Bertani, P.; Manfredi, M. Prevalence of Candida Species in Endodontic Infections: Systematic Review and Meta-analysis. J. Endod. 2018, 44, 1616–1625.e9. [Google Scholar] [CrossRef]
- Persoon, I.F.; Crielaard, W.; Ozok, A.R. Prevalence and nature of fungi in root canal infections: A systematic review and meta-analysis. Int. Endod. J. 2017, 50, 1055–1066. [Google Scholar] [CrossRef]
- Sen, B.H.; Safavi, K.E.; Spangberg, L.S. Growth patterns of Candida albicans in relation to radicular dentin. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1997, 84, 68–73. [Google Scholar] [CrossRef]
- Siqueira, J.F.; Rocas, I.N., Jr.; Lopes, H.P.; Elias, C.N.; de Uzeda, M. Fungal infection of the radicular dentin. J. Endod. 2002, 28, 770–773. [Google Scholar] [CrossRef]
- Sevilla, M.J.; Odds, F.C. Development of Candida albicans hyphae in different growth media-variations in growth rates, cell dimensions and timing of morphogenetic events. J. Gen. Microbiol. 1986, 132, 3083–3088. [Google Scholar] [CrossRef] [PubMed]
- Taha, N.A.; Ozawa, T.; Messer, H.H. Comparison of three techniques for preparing oval-shaped root canals. J. Endod. 2010, 36, 532–535. [Google Scholar] [CrossRef] [PubMed]
- Weiger, R.; ElAyouti, A.; Lost, C. Efficiency of hand and rotary instruments in shaping oval root canals. J. Endod. 2002, 28, 580–583. [Google Scholar] [CrossRef] [PubMed]
- Gwinnett, A.J. Smear layer: Morphological considerations. Oper. Dent. Suppl. 1984, 3, 2–12. [Google Scholar]
- Paque, F.; Laib, A.; Gautschi, H.; Zehnder, M. Hard-tissue debris accumulation analysis by high-resolution computed tomography scans. J. Endod. 2009, 35, 1044–1047. [Google Scholar] [CrossRef] [PubMed]
- Sen, B.H.; Chugal, N.M.; Liu, H.; Fleischmann, J. A new method for studying the adhesion of Candida albicans to dentin in the presence or absence of smear layer. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol 2003, 96, 201–206. [Google Scholar] [CrossRef]
- Kokkas, A.B.; Boutsioukis, A.C.; Vassiliadis, L.P.; Stavrianos, C.K. The influence of the smear layer on dentinal tubule penetration depth by three different root canal sealers: An in vitro study. J. Endod. 2004, 30, 100–102. [Google Scholar] [CrossRef]
- Willershausen, I.; Wolf, T.G.; Schmidtmann, I.; Berger, C.; Ehlers, V.; Willershausen, B.; Briseño, B. Survey of root canal irrigating solutions used in dental practices within Germany. Int. Endod. J. 2015, 48, 654–660. [Google Scholar] [CrossRef]
- Ramage, G.; Wickes, B.L.; Lopez-Ribot, J.L. Inhibition on Candida albicans biofilm formation using divalent cation chelators (EDTA). Mycopathologia 2007, 164, 301–306. [Google Scholar] [CrossRef]
- Kean, R.; Delaney, C.; Rajendran, R.; Sherry, L.; Metcalfe, R.; Thomas, R.; McLean, W.; Williams, C.; Ramage, G. Gaining Insights from Candida Biofilm Heterogeneity: One Size Does Not Fit All. J. Fungi (Basel) 2018, 4, 12. [Google Scholar] [CrossRef]
- Sherry, L.; Rajendran, R.; Lappin, D.F.; Borghi, E.; Perdoni, F.; Falleni, M.; Tosi, D.; Smith, K.; Williams, C.; Jones, B.; et al. Biofilms formed by Candida albicans bloodstream isolates display phenotypic and transcriptional heterogeneity that are associated with resistance and pathogenicity. BMC Microbiol. 2014, 14, 182. [Google Scholar] [CrossRef] [PubMed]
- Kean, R.; McKloud, E.; Townsend, E.M.; Sherry, L.; Delaney, C.; Jones, B.L.; Williams, C.; Ramage, G. The comparative efficacy of antiseptics against Candida auris biofilms. Int. J. Antimicrob. Agents 2018, 52, 673–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zehnder, M. Root canal irrigants. J. Endod. 2006, 32, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Fonzi, W.A.; Irwin, M.Y. Isogenic strain construction and gene mapping in Candida albicans. Genetics 1993, 134, 717–728. [Google Scholar]
- Slutsky, B.; Buffo, J.; Soll, D.R. High-frequency switching of colony morphology in Candida albicans. Science 1985, 230, 666–669. [Google Scholar] [CrossRef]
- Coco, B.; Bagg, J.; Cross, L.; Jose, A.; Cross, J.; Ramage, G. Mixed Candida albicans and Candida glabrata populations associated with the pathogenesis of denture stomatitis. Oral Microbiol. Immunol. 2008, 23, 377–383. [Google Scholar] [CrossRef]
- Ramage, G.; Coco, B.; Sherry, L.; Bagg, J.; Lappin, D.F. In vitro Candida albicans biofilm induced proteinase activity and SAP8 expression correlates with in vivo denture stomatitis severity. Mycopathologia 2012, 174, 11–19. [Google Scholar] [CrossRef]
- Ramage, G.; Jose, A.; Coco, B.; Rajendran, R.; Rautemaa, R.; Murray, C.; Lappin, D.F.; Bagg, J. Commercial mouthwashes are more effective than azole antifungals against Candida albicans biofilms in vitro. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011, 111, 456–460. [Google Scholar] [CrossRef]
- Ramage, G.; Walle, K.V.; Wickes, B.L.; López-Ribot, J.L. Standardized method for in vitro antifungal susceptibility testing of Candida albicansbiofilms. Antimicrob. Agents Chemother. 2001, 45, 2475–2479. [Google Scholar] [CrossRef]
- Jose, A.; Coco, B.J.; Milligan, S.; Young, B.; Lappin, D.F.; Bagg, J.; Murray, C.; Ramage, G. Reducing the incidence of denture stomatitis: Are denture cleansers sufficient? J. Prosthodont. Implant. Reconstr. Dent. 2010, 19, 252–257. [Google Scholar] [CrossRef]
- Junka, A.F.; Janczura, A.; Smutnicka, D.; Maczynska, B.; Secewicz, A.; Nowicka, J.; Bartoszewicz, M.; Gościniak, G. Use of the real time xCelligence system for purposes of medical microbiology. Pol. J. Microbiol. 2012, 61, 191–197. [Google Scholar] [PubMed]
- Wayne, P. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts, Approved Standard; CLSI; NCCLS: Wayne, PA, USA, 2002; document M27-A2. [Google Scholar]
- Rajendran, R.; Sherry, L.; Nile, C.J.; Sherriff, A.; Johnson, E.M.; Hanson, M.F.; Williams, C.; Munro, C.A.; Jones, B.J.; Ramage, G. Biofilm formation is a risk factor for mortality in patients with Candida albicans bloodstream infection—Scotland, 2012–2013. Clin. Microbiol. Infect. 2016, 22, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Kandaswamy, D.; Venkateshbabu, N. Root canal irrigants. J. Conserv. Dent. JCD 2010, 13, 256. [Google Scholar] [CrossRef] [PubMed]
- Radcliffe, C.E.; Potouridou, L.; Qureshi, R.; Habahbeh, N.; Qualtrough, A.; Worthington, H.; Drucker, D.B. Antimicrobial activity of varying concentrations of sodium hypochlorite on the endodontic microorganisms Actinomyces israelii, A. naeslundii, Candida albicans and Enterococcus faecalis. Int. Endod. J. 2004, 37, 438–446. [Google Scholar] [CrossRef]
- Mohammadi, Z. Sodium hypochlorite in endodontics: An update review. Int. Dent. J. 2008, 58, 329–341. [Google Scholar] [CrossRef]
- Waltimo, T.M.; Orstavik, D.; Siren, E.K.; Haapasalo, M.P. In vitro susceptibility of Candida albicans to four disinfectants and their combinations. Int. Endod. J. 1999, 32, 421–429. [Google Scholar] [CrossRef]
- Kumamoto, C.A. Candida biofilms. Curr. Opin. Microbiol. 2002, 5, 608–611. [Google Scholar] [CrossRef]
- Mah, T.F.; O’Toole, G.A. Mechanisms of biofilm resistance to antimicrobial agents. Trends Microbiol. 2001, 9, 34–39. [Google Scholar] [CrossRef]
- Roy, M.; Bhaumik, T. Comparative evaluation of effectiveness of 3% Sodium hypochlorite, 17% Ethelene diamine tetra-acetic acid (EDTA) and Fluconazole on Candida Albicans—An in vitro study. Int. J. Innov. Res. Dent. Sci. 2017, 2, 5. [Google Scholar]
- Karale, R.; Odedra, K.M.; Srirekha, A.; Champa, C.; Shetty, A.; Pushpalatha, S.; Sharma, R. Effect of dentin on the antimicrobial efficacy of 3% sodium hypochlorite, 2% chlorhexidine, 17% ethylenediaminetetraacetic acid, and 18% etidronic acid on Candida albicans: An in vitro study. J. Conserv. Dent. JCD 2016, 19, 455–460. [Google Scholar] [CrossRef]
- Siqueira, J.F.; Rôças, I.N.; Favieri, A.; Lima, K.C. Chemomechanical reduction of the bacterial population in the root canal after instrumentation and irrigation with 1%, 2.5%, and 5.25% sodium hypochlorite. J. Endod. 2000, 26, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Sen, B.H.; Akdeniz, B.G.; Denizci, A.A. The effect of ethylenediamine-tetraacetic acid on Candida albicans. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2000, 90, 651–655. [Google Scholar] [CrossRef] [PubMed]
- Delaney, C.; Kean, R.; Short, B.; Tumelty, M.; McLean, W.; Nile, C.J.; Ramage, G. Fungi at the scene of the crime: Innocent bystanders or accomplices in oral infections? Curr. Clin. Microbiol. Rep. 2018, 5, 190–200. [Google Scholar] [CrossRef]







© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshanta, O.A.; Shaban, S.; Nile, C.J.; McLean, W.; Ramage, G. Candida albicans Biofilm Heterogeneity and Tolerance of Clinical Isolates: Implications for Secondary Endodontic Infections. Antibiotics 2019, 8, 204. https://doi.org/10.3390/antibiotics8040204
Alshanta OA, Shaban S, Nile CJ, McLean W, Ramage G. Candida albicans Biofilm Heterogeneity and Tolerance of Clinical Isolates: Implications for Secondary Endodontic Infections. Antibiotics. 2019; 8(4):204. https://doi.org/10.3390/antibiotics8040204
Chicago/Turabian StyleAlshanta, Om Alkhir, Suror Shaban, Christopher J Nile, William McLean, and Gordon Ramage. 2019. "Candida albicans Biofilm Heterogeneity and Tolerance of Clinical Isolates: Implications for Secondary Endodontic Infections" Antibiotics 8, no. 4: 204. https://doi.org/10.3390/antibiotics8040204