
Outcome and Predictors of Treatment Failure in Chronic Osteomyelitis Using Bioactive Glass Granules and Putty Formulations
 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants/Study Subjects
2.3. Variables, Outcome Measures, and Data Sources
2.4. Surgical Management
2.5. Definitions
2.6. Specimen Collection and Microbiology
2.7. Statistical Analysis
3. Results
3.1. Study Population
3.2. Microbiological Findings
3.3. Six-Month Follow-Up Analyses (92 Patients)
3.4. Twelve-Month Follow-Up Analyses (78 Patients)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferguson, J.; Bourget-Murray, J.; Stubbs, D.; McNally, M.; Hotchen, A.J. A Comparison of Clinical and Radiological Outcomes between Two Different Biodegradable Local Antibiotic Carriers Used in the Single-Stage Surgical Management of Long Bone Osteomyelitis. Bone Jt. Res. 2023, 12, 412–422. [Google Scholar] [CrossRef]
- Gimza, B.D.; Cassat, J.E. Mechanisms of Antibiotic Failure During Staphylococcus Aureus Osteomyelitis. Front. Immunol. 2021, 12, 638085. [Google Scholar] [CrossRef]
- Brydone, A.S.; Meek, D.; Maclaine, S. Bone Grafting, Orthopaedic Biomaterials, and the Clinical Need for Bone Engineering. Proc. Inst. Mech. Eng. H 2010, 224, 1329–1343. [Google Scholar] [CrossRef] [PubMed]
- Dimitriou, R.; Jones, E.; McGonagle, D.; Giannoudis, P.V. Bone Regeneration: Current Concepts and Future Directions. BMC Med. 2011, 9, 66. [Google Scholar] [CrossRef]
- Giannoudis, P.V.; Dinopoulos, H.; Tsiridis, E. Bone Substitutes: An Update. Injury 2005, 36 (Suppl. S3), 20–27. [Google Scholar] [CrossRef] [PubMed]
- Athanasiou, V.T.; Papachristou, D.J.; Panagopoulos, A.; Saridis, A.; Scopa, C.D.; Megas, P. Histological Comparison of Autograft, Allograft-DBM, Xenograft, and Synthetic Grafts in a Trabecular Bone Defect: An Experimental Study in Rabbits. Med. Sci. Monit. 2010, 16, 24–31. [Google Scholar]
- Batista Campos, L.; Kurihara, M.N.L.; Santos, I.N.M.; dos Reis, F.B.; Salles, M.J. In Vitro Elution Characteristics of Antibiotic-Loaded Polymethylmethacrylate Cement and a Calcium Sulfate Bone Substitute Using Staphylococci Isolated from Orthopedic Implant-Associated Infections. J. Biomed. Mater. Res.—Part. B Appl. Biomater. 2023, 111, 1318–1327. [Google Scholar] [CrossRef]
- Ferguson, J.; Diefenbeck, M.; McNally, M. Ceramic Biocomposites as Biodegradable Antibiotic Carriers in the Treatment of Bone Infections. J. Bone Jt. Infect. 2017, 2, 38–51. [Google Scholar] [CrossRef] [PubMed]
- Virolainen, P.; Heikkilä, J.; Yli-Urpo, A.; Vuorio, E.; Aro, H.T. Histomorphometric and Molecular Biologic Comparison of Bioactive Glass Granules and Autogenous Bone Grafts in Augmentation of Bone Defect Healing. J. Biomed. Mater. Res. 1997, 35, 9–17. [Google Scholar] [CrossRef]
- Van Gestel, N.A.P.; Geurts, J.; Hulsen, D.J.W.; Van Rietbergen, B.; Hofmann, S.; Arts, J.J. Clinical Applications of S53P4 Bioactive Glass in Bone Healing and Osteomyelitic Treatment: A Literature Review. Biomed. Res. Int. 2015, 2015, 684826. [Google Scholar] [CrossRef]
- Hasan, R.; Schaner, K.; Mulinti, P.; Brooks, A. A Bioglass-Based Antibiotic (Vancomycin) Releasing Bone Void Filling Putty to Treat Osteomyelitis and Aid Bone Healing. Int. J. Mol. Sci. 2021, 22, 7736. [Google Scholar] [CrossRef]
- Van Gestel, N.A.P.; Hulsen, D.J.W.; Geurts, J.; Hofmann, S.; Ito, K.; Arts, J.J.; Van Rietbergen, B. Composition Dependent Mechanical Behaviour of S53P4 Bioactive Glass Putty for Bone Defect Grafting. J. Mech. Behav. Biomed. Mater. 2017, 69, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Hasan, R.; Schaner, K.; Schroeder, M.; Wohlers, A.; Shreffler, J.; Schaper, C.; Subramanian, H.; Brooks, A. Extended Release Combination Antibiotic Therapy from a Bone Void Filling Putty for Treatment of Osteomyelitis. Pharmaceutics 2019, 11, 592. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, R.B.; Salles, M.J. Outcomes and Risk Factors in Prosthetic Joint Infections by Multidrug-Resistant Gram-Negative Bacteria: A Retrospective Cohort Study. Antibiotics 2021, 10, 340. [Google Scholar] [CrossRef]
- Rupp, M.; Walter, N.; Baertl, S.; Lang, S.; Lowenberg, D.W.; Alt, V. Terminology of Bone and Joint Infection. Bone Jt. Res. 2021, 10, 742–743. [Google Scholar] [CrossRef] [PubMed]
- Cierny, G.; Mader, J.T.; Penninck, J.J. The Classic: A Clinical Staging System for Adult Osteomyelitis. Clin. Orthop. Relat. Res. 2003, 414, 7–24. [Google Scholar] [CrossRef]
- Kurien, T.; Pearson, R.G.; Scammell, B.E. Bone Graft Substitutes Currently Available in Orthopaedic Practice: The Evidence for Their Use. Bone Jt. J. 2013, 95B, 583–597. [Google Scholar] [CrossRef] [PubMed]
- Greco, T.; Cianni, L.; Polichetti, C.; Inverso, M.; Maccauro, G.; Perisano, C. Uncoated vs. Antibiotic-Coated Tibia Nail in Open Diaphyseal Tibial Fracture (42 According to AO Classification): A Single Center Experience. BioMed Res. Int. 2021, 2021, 7421582. [Google Scholar] [CrossRef] [PubMed]
- Perisano, C.; Greco, T.; Polichetti, C.; Inverso, M.; Maccauro, G. Antibiotic-Coated Nail in Open Tibial Fracture: A Retrospective Case Series. J. Funct. Morphol. Kinesiol. 2021, 6, 97. [Google Scholar] [CrossRef]
- Bachoura, A.; Guitton, T.G.; Malcolm Smith, R.; Vrahas, M.S.; Zurakowski, D.; Ring, D. Infirmity and Injury Complexity Are Risk Factors for Surgical-Site Infection after Operative Fracture Care. Clin. Orthop. Relat. Res. 2011, 469, 2621–2630. [Google Scholar] [CrossRef]
- Geurts, J.; van Vugt, T.; Thijssen, E.; Arts, J.J. Cost-Effectiveness Study of One-Stage Treatment of Chronic Osteomyelitis with Bioactive Glass S53p4. Materials 2019, 12, 3209. [Google Scholar] [CrossRef]
- Van Vugt, T.A.G.; Heidotting, J.; Arts, J.J.; Ploegmakers, J.J.W.; Jutte, P.C.; Geurts, J.A.P. Mid-Term Clinical Results of Chronic Cavitary Long Bone Osteomyelitis Treatment Using S53P4 Bioactive Glass: A Multi-Center Study. J. Bone Jt. Infect. 2021, 6, 413–421. [Google Scholar] [CrossRef]
- Lindfors, N.C.; Hyvönen, P.; Nyyssönen, M.; Kirjavainen, M.; Kankare, J.; Gullichsen, E.; Salo, J. Bioactive Glass S53P4 as Bone Graft Substitute in Treatment of Osteomyelitis. Bone 2010, 47, 212–218. [Google Scholar] [CrossRef]
- Kankare, J.; Lindfors, N.C. Reconstruction of Vertebral Bone Defects Using an Expandable Replacement Device and Bioactive Glass S53P4 in the Treatment of Vertebral Osteomyelitis: Three Patients and Three Pathogens. Scand. J. Surg. 2016, 105, 248–253. [Google Scholar] [CrossRef]
- dos Reis, G.N.B.; Cuba, G.T.; de Castro Targa, W.H.; Miras, P.S.C.; Bongiovanni, J.C.; Salles, M.J.; dos Reis, F.B.; Dell’Aquila, A.M. S53P4 Bioactive Glass Putty in the Local Treatment of Cavitary Chronic Osteomyelitis. Acta Ortop. Bras. 2023, 31, 2021–2024. [Google Scholar] [CrossRef]
- ElHawary, H.; Baradaran, A.; Abi-Rafeh, J.; Vorstenbosch, J.; Xu, L.; Efanov, J.I. Bone Healing and Inflammation: Principles of Fracture and Repair. Semin. Plast. Surg. 2021, 35, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, K.; Van Den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. (HLS-EU) Consortium Health Literacy Project European Health Literacy and Public Health: A Systematic Review and Integration of Definitions and Models. BMC Public. Health 2012, 12, 80. [Google Scholar] [CrossRef]
- Da Costa, T.S.; De Medeiros, P.J.; Salles, M.J.C. Smoking Increases the Risk of Surgical Site Infection after Hydrocelectomy in Adults: A Retrospective Cohort Study in Brazil. J. Infect. Dev. Ctries. 2018, 11, 950–956. [Google Scholar] [CrossRef]
- Coraça-Huber, D.C.; Fille, M.; Hausdorfer, J.; Putzer, D.; Nogler, M. Efficacy of Antibacterial Bioactive Glass S53P4 against S. Aureus Biofilms Grown on Titanium Discs in Vitro. J. Orthop. Res. 2014, 32, 175–177. [Google Scholar] [CrossRef]
- Drago, L.; Vassena, C.; Fenu, S.; De Vecchi, E.; Signori, V.; Francesco, R.D.; Romanò, C.L. In Vitro Antibiofilm Activity of Bioactive Glass S53P4. Future Microbiol. 2014, 9, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Thi, M.T.T.; Wibowo, D.; Rehm, B.H.A. Pseudomonas Aeruginosa Biofilms. Int. J. Mol. Sci. 2020, 21, 8671. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics, Comorbidities, and Habits | N = 92 (%) |
|---|---|
| Gender | |
| Male | 63 (68.5%) |
| Age (mean (range)) (Years old) | 49 (34–64) |
| <17 years | 5 (5.4%) |
| 18–39 years | 26 (28.3%) |
| 40–59 years | 35 (38.0%) |
| 60–79 years | 18 (19.6%) |
| >80 years | 8 (8.7%) |
| Chronic heart disease and/or hypertension | 22 (23.9%) |
| Diabetes mellitus | 20 (21.7%) |
| Smoking habits | 9 (9.8%) |
| Thrombosis | 4 (4.3%) |
| Paraplegia or quadriplegia | 4 (4.3%) |
| Neoplasia | 3 (3.3%) |
| Immunosuppression condition | 2 (2.2%) |
| Alcoholism | 1 (1.1%) |
| Osteomyelitis | |
| Implant-free | 54 (58.7%) |
| Implant-associated | 38 (41.3%) |
| Pseudarthrosis | 14 (15.2%) |
| Fistula | 15 (16.3%) |
| Bioactive glass formulation | |
| Granules and putty | 33 (35.9%) |
| Putty (only) | 30 (32.6%) |
| Granules (only) | 29 (31.5%) |
| Duration of infection | |
| <3 months | 37 (40.2%) |
| >3 months | 55 (59.8%) |
| Microorganisms | N = 69 (%) |
|---|---|
| Gram-positive cocci | 35 (50.7) |
| Staphylococcus aureus | 19 (27.5) |
| MRSA a | 5 (7.3) |
| MSSA b | 2 (2.9) |
| Coagulase-negative Staphylococci (CNS) | 10 (14.5) |
| Staphylococcus epidermidis | 4 (5.8) |
| Staphylococcus caprae | 1 (1.4) |
| Staphylococcus haemolyticus | 1 (1.4) |
| Staphylococcus xylosus | 1 (1.4) |
| Staphylococcus lugdunensis | 3 (4.3) |
| Enterococcus avium | 1 (1.4) |
| Enterococcus faecalis | 1 (1.4) |
| Enterococcus faecium | 1 (1.4) |
| Streptococcus acidominimus | 1 (1.4) |
| Streptococcus viridans | 1 (1.4) |
| Gram-negative bacilli | 33 (47.8) |
| Pseudomonas aeruginosa | 14 (20.3) |
| Escherichia coli | 5 (7.2) |
| Klebsiella pneumoniae | 6 (8.7) |
| Acinetobacter baumannii | 2 (2.9) |
| Proteus mirabilis | 2 (2.9) |
| Klebsiella oxytoca | 1 (1.4) |
| Morganella morganii | 1 (1.4) |
| Enterobacter aerogenes | 1 (1.4) |
| Enterobacter cloacae | 1 (1.4) |
| Candida albicans | 1 (1.4) |
| MDR c | 26 (37.7) |
| Staphylococcus aureus | 10 (14.5) |
| Pseudomonas aeruginosa | 5 (7.3) |
| Klebsiella pneumoniae | 4 (5.8) |
| Escherichia coli | 2 (2.9) |
| Staphylococcus caprae | 1 (1.4) |
| Staphylococcus epidermidis | 3 (4.3) |
| Staphylococcus xylosus | 1 (1.4) |
| Characteristics | Remission No. (%) (N = 79) | Failure No. (%) (N = 13) | p-Value |
|---|---|---|---|
| Bioactive glass | |||
| Putty (only) | 28 (93.3%) | 2 (6.7%) | 0.058 * |
| Granules and putty | 30 (90.9%) | 3 (9.1%) | |
| Granules (only) | 21 (72.4%) | 8 (27.6%) | |
| Duration of infection | |||
| <3 months | 33 (89.2%) | 4 (10.8%) | 0.453 ** |
| >3 months | 46 (83.6%) | 9 (16.4%) | |
| Gram-positive cocci | |||
| No | 51 (85.0%) | 9 (15.0%) | 1.000 * |
| Yes | 28 (87.5%) | 4 (12.5%) | |
| Staphylococcus spp. | |||
| No | 55 (85.9%) | 9 (14,1%) | 1.000 * |
| Yes | 24 (85.7%) | 4 (14.3%) | |
| Gram-negative bacilli | |||
| No | 57 (89.1%) | 7 (10.9%) | 0.204 * |
| Yes | 22 (78.6%) | 6 (21.4%) | |
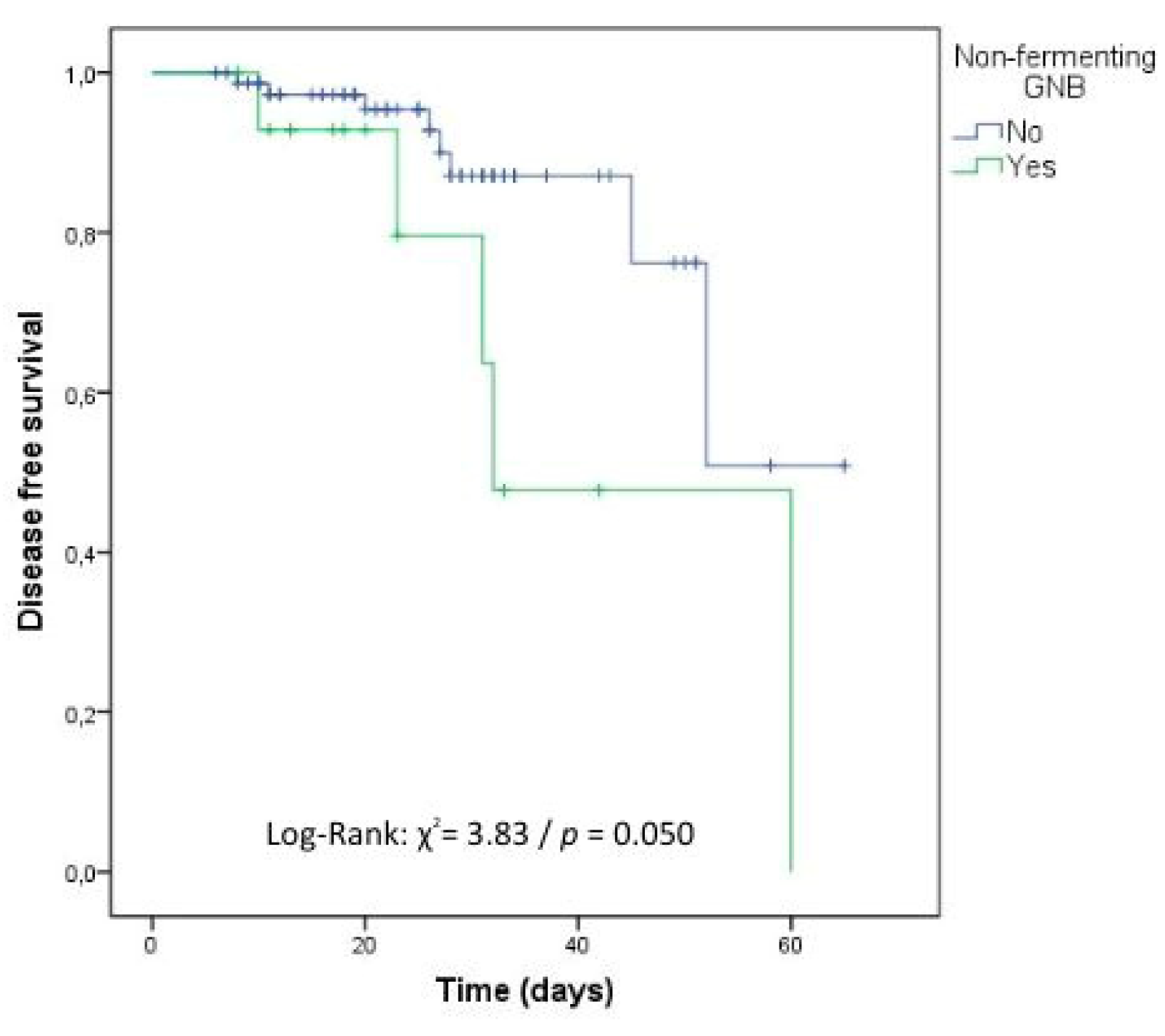
| Nonfermenting Gram-negative bacilli | |||
| No | 69 (89.6%) | 8 (10.4%) | 0.034 * |
| Yes | 10 (66.7%) | 5 (33.3%) |
| Variables | 6 Months | 12 Months | ||
|---|---|---|---|---|
| PR (CI 95%) | p-Value | PR (CI 95%) | p-Value | |
| Smoking | 2.37 (0.55; 10.24) | 0.248 | 4.0 (1.03; 15.52) | 0.045 ** |
| Nonfermenting Gram-negative bacilli | 3.92 (0.45; 33.91) | 0.215 | 3.87 (1.09; 13.73) | 0.036 ** |
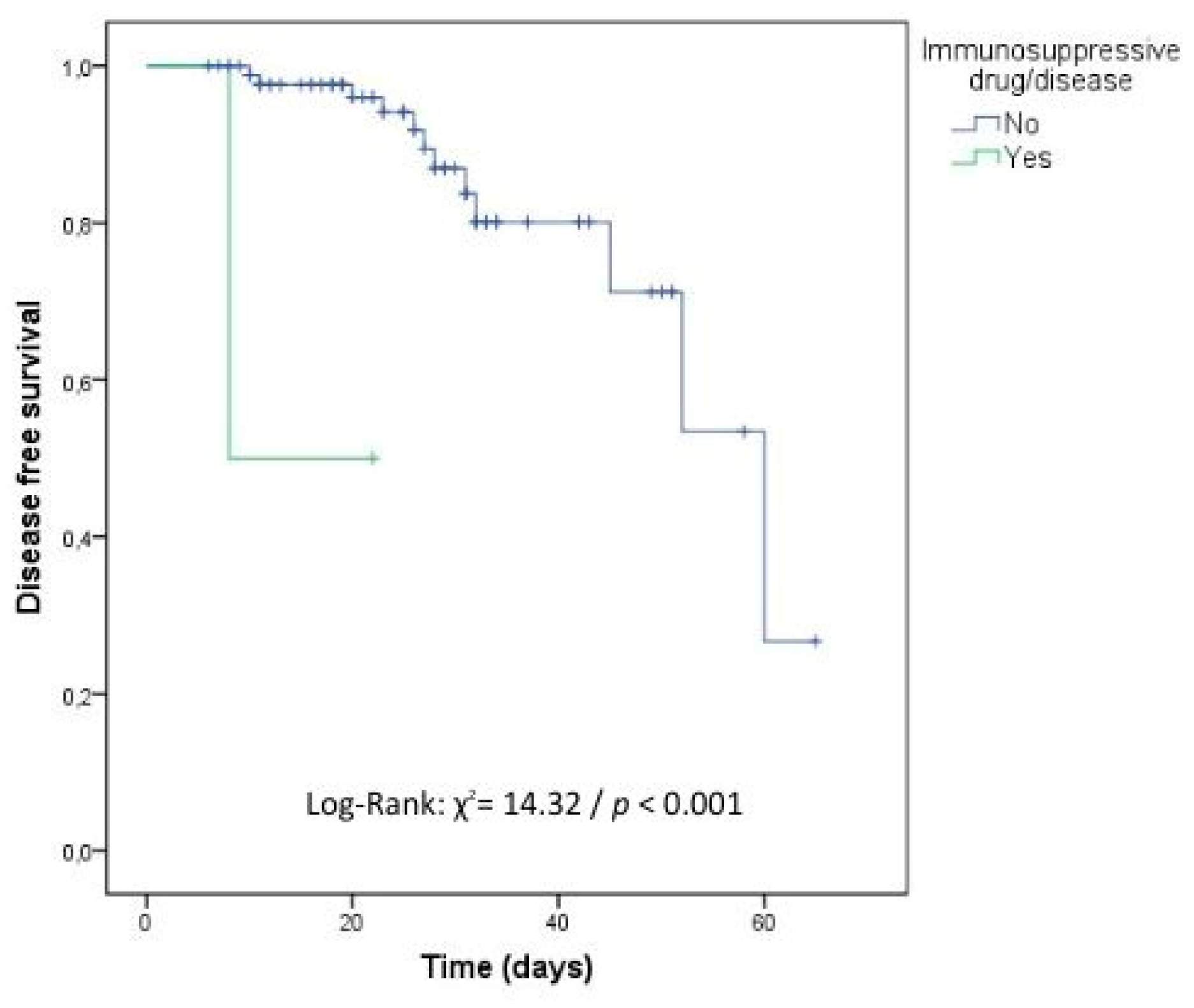
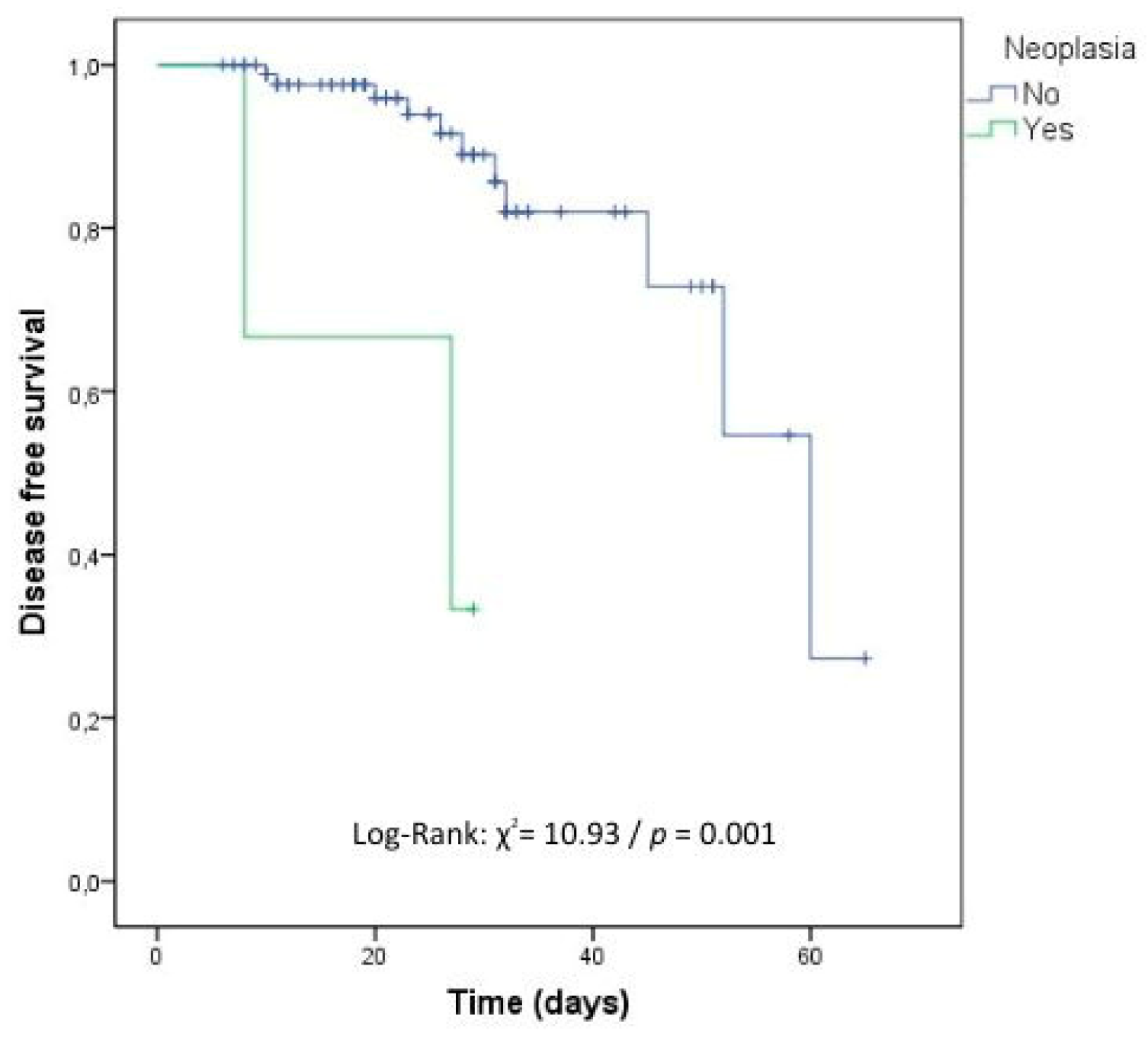
| Neoplasia | 5.26 (1.17; 23.73) | 0.031 ** | 2.64 (0.12; 57.66) | 0.538 |
| Bioglass in granules | 3.44 (1.13; 10.52) | 0.030 ** | 3.04 (0.46; 19.84) | 0.246 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dell’Aquila, A.M.; Reis, G.N.B.d.; Cuba, G.T.; Targa, W.H.d.C.; Bongiovanni, J.C.; Durigon, T.S.; Salles, M.J.; Reis, F.B.d. Outcome and Predictors of Treatment Failure in Chronic Osteomyelitis Using Bioactive Glass Granules and Putty Formulations. Antibiotics 2023, 12, 1720. https://doi.org/10.3390/antibiotics12121720
Dell’Aquila AM, Reis GNBd, Cuba GT, Targa WHdC, Bongiovanni JC, Durigon TS, Salles MJ, Reis FBd. Outcome and Predictors of Treatment Failure in Chronic Osteomyelitis Using Bioactive Glass Granules and Putty Formulations. Antibiotics. 2023; 12(12):1720. https://doi.org/10.3390/antibiotics12121720
Chicago/Turabian StyleDell’Aquila, Adriana Macedo, Gabriela Nagy Baldy dos Reis, Gabriel Trova Cuba, Walter Hamilton de Castro Targa, José Carlos Bongiovanni, Thomas Stravinskas Durigon, Mauro José Salles, and Fernando Baldy dos Reis. 2023. "Outcome and Predictors of Treatment Failure in Chronic Osteomyelitis Using Bioactive Glass Granules and Putty Formulations" Antibiotics 12, no. 12: 1720. https://doi.org/10.3390/antibiotics12121720