Early Renal Involvement in Cats with Natural Feline Morbillivirus Infection

 , , ,
, , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. FeMV Infection Diagnosis and Serological Evaluation
2.2. Clinical and Clinicopathological Evaluation
2.3. Renal Histopathology and Immunohistochemistry
2.4. Statistical Analysis
3. Results
3.1. Hematology, Chemistry and Urinalysis Results
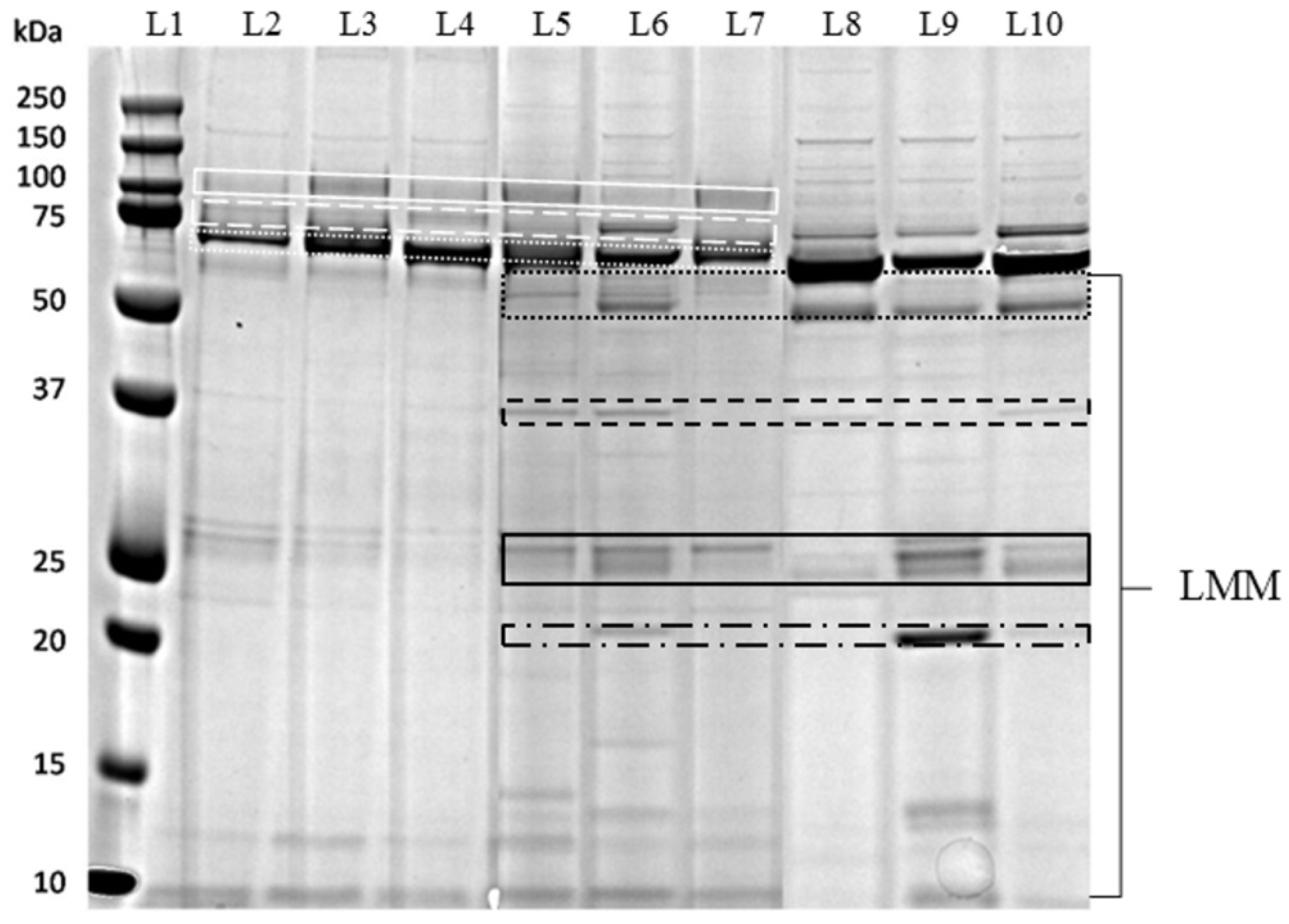
3.2. Quantitative and Qualitative Urine Analysis
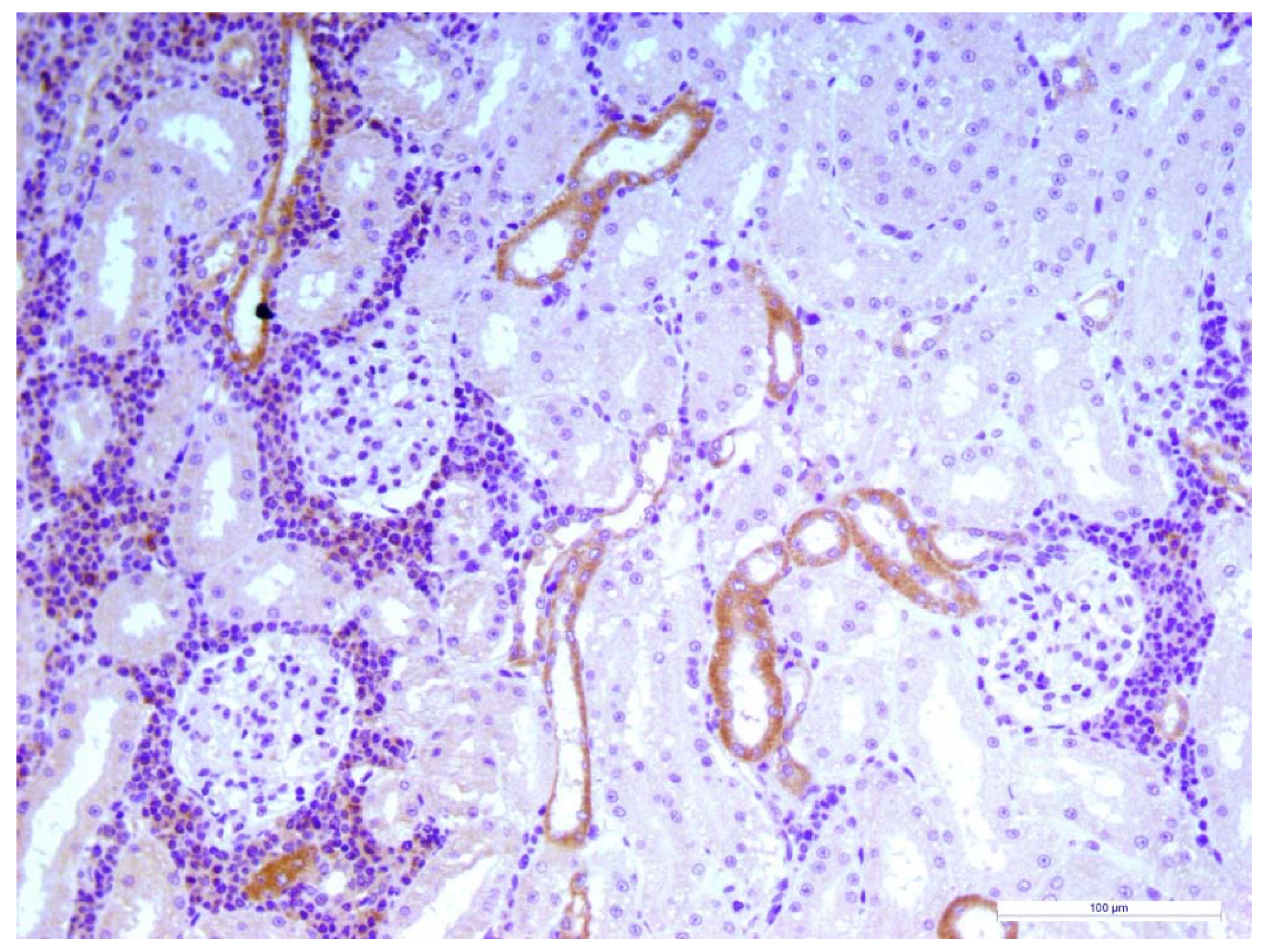
3.3. Renal Histopathology
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Woo, P.C.Y.; Lau, S.K.P.; Wong, B.H.L.; Fan, R.Y.Y.; Wong, A.Y.P.; Zhang, A.J.X.; Wu, Y.; Choi, G.K.Y.; Li, K.S.M.; Hui, J.; et al. Feline morbillivirus, a previously undescribed paramyxovirus associated with tubulointerstitial nephritis in domestic cats. Proc. Natl. Acad. Sci. USA 2012, 109, 5435–5440. [Google Scholar] [CrossRef] [Green Version]
- Furuya, T.; Sassa, Y.; Omatsu, T.; Nagai, M.; Fukushima, R.; Shibutani, M.; Yamaguchi, T.; Uematsu, Y.; Shirota, K.; Mizutani, T. Existence of feline morbillivirus infection in Japanese cat populations. Arch. Virol. 2014, 159, 371–373. [Google Scholar] [CrossRef]
- Park, E.-S.; Suzuki, M.; Kimura, M.; Mizutani, H.; Saito, R.; Kubota, N.; Hasuike, Y.; Okajima, J.; Kasai, H.; Sato, Y.; et al. Epidemiological and pathological study of feline morbillivirus infection in domestic cats in Japan. BMC Vet. Res. 2016, 12, 228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorusso, A.; Di Tommaso, M.; Di Felice, E.; Zaccaria, G.; Luciani, A.; Marcacci, M.; Aste, G.; Boari, A.; Savini, G. First report of feline morbillivirus in Europe. Vet. Ital. 2015, 51, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Marcacci, M.; De Luca, E.; Zaccaria, G.; Di Tommaso, M.; Mangone, I.; Aste, G.; Savini, G.; Boari, A.; Lorusso, A. Genome characterization of feline morbillivirus from Italy. J. Virol. Methods 2016, 234, 160–163. [Google Scholar] [CrossRef] [PubMed]
- De Luca, E.; Crisi, P.E.; Marcacci, M.; Malatesta, D.; Di Sabatino, D.; Cito, F.; D’Alterio, N.; Puglia, I.; Berjaoui, S.; Colaianni, M.L.; et al. Epidemiology, pathological aspects and genome heterogeneity of feline morbillivirus in Italy. Vet. Microbiol. 2019, 108484. [Google Scholar] [CrossRef]
- Sieg, M.; Heenemann, K.; Rückner, A.; Burgener, I.; Oechtering, G.; Vahlenkamp, T.W. Discovery of new feline paramyxoviruses in domestic cats with chronic kidney disease. Virus Genes 2015, 51, 294–297. [Google Scholar] [CrossRef]
- Sharp, C.R.; Nambulli, S.; Acciardo, A.S.; Rennick, L.J.; Drexler, J.F.; Rima, B.K.; Williams, T.; Duprex, W.P. Chronic Infection of Domestic Cats with Feline Morbillivirus, United States. Emerg. Infect. Dis. 2016, 22, 760–762. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, H.; Tekelioglu, B.K.; Gurel, A.; Bamac, O.E.; Ozturk, G.Y.; Cizmecigil, U.Y.; Altan, E.; Aydin, O.; Yilmaz, A.; Berriatua, E.; et al. Frequency, clinicopathological features and phylogenetic analysis of feline morbillivirus in cats in Istanbul, Turkey. J. Feline Med. Surg. 2017, 19, 1206–1214. [Google Scholar] [CrossRef]
- Darold, G.M.; Alfieri, A.A.; Muraro, L.S.; Amude, A.M.; Zanatta, R.; Yamauchi, K.C.I.; Alfieri, A.F.; Lunardi, M. First report of feline morbillivirus in South America. Arch. Virol. 2017, 162, 469–475. [Google Scholar] [CrossRef]
- McCallum, K.E.; Stubbs, S.; Hope, N.; Mickleburgh, I.; Dight, D.; Tiley, L.; Williams, T.L. Detection and seroprevalence of morbillivirus and other paramyxoviruses in geriatric cats with and without evidence of azotemic chronic kidney disease. J. Vet. Intern. Med. 2018, 32, 1100–1108. [Google Scholar] [CrossRef] [PubMed]
- Chakrabarti, S.; Syme, H.M.; Brown, C.A.; Elliott, J. Histomorphometry of feline chronic kidney disease and correlation with markers of renal dysfunction. Vet. Pathol. 2013, 50, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Bartges, J.W. Chronic kidney disease in dogs and cats. Vet. Clin. N. Am. Small Anim. Pract. 2012, 42, 669–692. [Google Scholar] [CrossRef] [PubMed]
- Finch, N. Measurement of glomerular filtration rate in cats: Methods and advantages over routine markers of renal function. J. Feline Med. Surg. 2014, 16, 736–748. [Google Scholar] [CrossRef]
- Polzin, D.J. Chronic kidney disease. In Textbook of Veterinary Internal Medicine: Disease of the Dog and the Cat; Elsevier: St. Louis, MO, USA, 2017; pp. 1938–1959. [Google Scholar]
- Vaden, S.L.; Levine, J.F.; Lees, G.E.; Groman, R.P.; Grauer, G.F.; Forrester, S.D. Renal biopsy: A retrospective study of methods and complications in 283 dogs and 65 cats. J. Vet. Intern. Med. 2005, 19, 794–801. [Google Scholar] [CrossRef]
- Sparkes, A.H.; Caney, S.; Chalhoub, S.; Elliott, J.; Finch, N.; Gajanayake, I.; Langston, C.; Lefebvre, H.P.; White, J.; Quimby, J. ISFM Consensus Guidelines on the Diagnosis and Management of Feline Chronic Kidney Disease. J. Feline Med. Surg. 2016, 18, 219–239. [Google Scholar] [CrossRef]
- IRIS Staging of CKD. Available online: http://www.xn--iriskidney-ru6e.com/guidelines/staging.html (accessed on 26 January 2020).
- Hall, J.A.; Yerramilli, M.; Obare, E.; Yerramilli, M.; Jewell, D.E. Comparison of serum concentrations of symmetric dimethylarginine and creatinine as kidney function biomarkers in cats with chronic kidney disease. J. Vet. Intern. Med. 2014, 28, 1676–1683. [Google Scholar] [CrossRef] [Green Version]
- Jepson, R.E.; Coulton, G.R.; Cowan, M.L.; Markwell, P.; Syme, H.M.; Elliott, J. Evaluation of mass spectrometry of urinary proteins and peptides as biomarkers for cats at risk of developing azotemia. Am. J. Vet. Res. 2013, 74, 333–342. [Google Scholar] [CrossRef]
- Ferlizza, E.; Campos, A.; Neagu, A.; Cuoghi, A.; Bellei, E.; Monari, E.; Dondi, F.; Almeida, A.M.; Isani, G. The effect of chronic kidney disease on the urine proteome in the domestic cat (Felis catus). Vet. J. 2015, 204, 73–81. [Google Scholar] [CrossRef] [Green Version]
- Martorelli, C.R.; Kogika, M.M.; Chacar, F.C.; Caragelasco, D.S.; de Campos Fonseca Pinto, A.C.B.; Lorigados, C.A.B.; Andrade, L.C. Urinary Fractional Excretion of Phosphorus in Dogs with Spontaneous Chronic Kidney Disease. Vet. Sci. 2017, 4, 67. [Google Scholar] [CrossRef] [Green Version]
- Miyazaki, M.; Soeta, S.; Yamagishi, N.; Taira, H.; Suzuki, A.; Yamashita, T. Tubulointerstitial nephritis causes decreased renal expression and urinary excretion of cauxin, a major urinary protein of the domestic cat. Res. Vet. Sci. 2007, 82, 76–79. [Google Scholar] [CrossRef] [PubMed]
- De Luca, E.; Crisi, P.E.; Di Domenico, M.; Malatesta, D.; Vincifori, G.; Di Tommaso, M.; Di Guardo, G.; Di Francesco, G.; Petrini, A.; Savini, G.; et al. A real-time RT-PCR assay for molecular identification and quantitation of feline morbillivirus RNA from biological specimens. J. Virol. Methods 2018, 258, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.S.; Sparkes, A.H.; Briscoe, K.; Carter, J.; Sala, S.C.; Jepson, R.E.; Reynolds, B.S.; Scansen, B.A. ISFM Consensus Guidelines on the Diagnosis and Management of Hypertension in Cats. J. Feline Med. Surg. 2017, 19, 288–303. [Google Scholar] [CrossRef] [PubMed]
- Hokamp, J.A.; Leidy, S.A.; Gaynanova, I.; Cianciolo, R.E.; Nabity, M.B. Correlation of electrophoretic urine protein banding patterns with severity of renal damage in dogs with proteinuric chronic kidney disease. Vet. Clin. Pathol. 2018, 47, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.A.; Elliott, J.; Schmiedt, C.W.; Brown, S.A. Chronic Kidney Disease in Aged Cats: Clinical Features, Morphology, and Proposed Pathogeneses. Vet. Pathol. 2016, 53, 309–326. [Google Scholar] [CrossRef]
- Rizzo, F.; Tappin, S.W.; Tasker, S. Thrombocytosis in cats: A retrospective study of 51 cases (2000–2005). J. Feline Med. Surg. 2007, 9, 319–325. [Google Scholar] [CrossRef]
- Chikazawa, S.; Dunning, M.D. A review of anaemia of inflammatory disease in dogs and cats. J. Small Anim. Pract. 2016, 57, 348–353. [Google Scholar] [CrossRef]
- Relford, R.; Robertson, J.; Clements, C. Symmetric Dimethylarginine: Improving the Diagnosis and Staging of Chronic Kidney Disease in Small Animals. Vet. Clin. N. Am. Small Anim. Pract. 2016, 46, 941–960. [Google Scholar] [CrossRef] [Green Version]
- Littman, M.P. Protein-losing nephropathy in small animals. Vet. Clin. N. Am. Small Anim. Pract. 2011, 41, 31–62. [Google Scholar] [CrossRef]
- Hokamp, J.A.; Nabity, M.B. Renal biomarkers in domestic species. Vet. Clin. Pathol. 2016, 45, 28–56. [Google Scholar] [CrossRef]
- Beatty, J.A.; Sharp, C.R.; Duprex, W.P.; Munday, J.S. Novel feline viruses: Emerging significance of gammaherpesvirus and morbillivirus infections. J. Feline Med. Surg. 2019, 21, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Lawler, D.F.; Evans, R.H.; Chase, K.; Ellersieck, M.; Li, Q.; Larson, B.T.; Satyaraj, E.; Heininger, K. The aging feline kidney: A model mortality antagonist? J. Feline Med. Surg. 2006, 8, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Sutummaporn, K.; Suzuki, K.; Machida, N.; Mizutani, T.; Park, E.-S.; Morikawa, S.; Furuya, T. Association of feline morbillivirus infection with defined pathological changes in cat kidney tissues. Vet. Microbiol. 2019, 228, 12–19. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Healthy (n = 22) | FeMV (n = 14) | CKD (n = 21) | p Value |
|---|---|---|---|---|
| Median body weight (kg) | 5.0 (2.6–7.6) | 3.8 (3.0–6.0) | 4.0 (2.1–7.4) | 0.005 * |
| Median BCS | 6 (5–8) | 5 (2–7) | 5 (3–6) | 0.001 * |
| Poor coat conditions n (%) | – | 8 (57%) | 4 (19%) | 0.003 |
| Gingivostomatitis n (%) | – | 4 (29%) | 8 (38%) | 0.721 |
| Diarrhea n (%) | – | 3 (21%) | 2 (9%) | 0.369 |
| Hyporexia/Anorexia n (%) | – | 2 (14%) | 12 (57%) | 0.016 |
| FeLV n (%) | – | 2 (14%) | 0 | 0.153 |
| FIV n (%) | – | 0 | 0 | 1.000 |
| Weight loss n (%) | – | 1 (7%) | 11 (52%) | 0.009 |
| Vomiting n (%) | – | 1 (7%) | 6 (29%) | 0.203 |
| Pale mucous n (%) | – | 1 (7%) | 6 (29%) | 0.203 |
| Lethargy n (%) | – | 1 (7%) | 3 (14%) | 0.635 |
| Enlarged abdomen n (%) | – | 1 (7%) | 0 | 0.400 |
| Dehydration n (%) | – | 1 (7%) | 7 (33%) | 0.108 |
| PU/PD n (%) | – | 0 | 10 (48%) | 0.002 |
| Heart murmur n (%) | – | 0 | 3 (14%) | 0.259 |
| Constipation n (%) | – | 0 | 2 (9%) | 0.506 |
| Abnormal renal palpation n (%) | – | 1 (7%) | 7 (33%) | 0.108 |
| Hypertension (SBP > 160 mmHg) n (%) | – | 0 | 9 (43%) | 0.005 |
| Ultrasound abnormalities n (%) | 3 (14%) | 2 (14%) | 21 (100%) | <0.001 |
| Hyperechoic cortex | 3 (14%) | 2 (7%) | 21 (100%) | <0.001 |
| Decreased corticomedullar distinction | – | 0 | 13 (62%) | <0.001 |
| Small kidneys | – | 0 | 5 (24%) | 0.063 |
| Irregular kidney shape | – | 0 | 10 (48%) | 0.002 |
| Variable | RI | Healthy (n = 22) | FeMV (n = 14) | CKD (n = 21) | p Value |
|---|---|---|---|---|---|
| Hct % | 32–48 | 38.3 (33.3–48.7) | 32.0 (19.9–41.4) | 27.0 (17.7–40.1) | <0.001 * |
| WBCs cells/mm³ | 4800–14,900 | 8600 (4980–18,830) | 16,345 (7990–23,340) | 9660 (5480–27,970) | <0.001 ¶ |
| Neutrophils cells/mm³ | 1600–10,000 | 4710 (1570–13,520) | 9320 (4080–16,870) | 6270 (2740–24,790) | <0.001 * |
| Lymphocytes cells/mm³ | 900–5600 | 3050 (1150–4610) | 4530 (1660–9700) | 1760 (800– 7770) | <0.001 * |
| Monocytes cells/mm³ | 0–650 | 135.0 (50.0–490.0) | 470.0 (0.0–920.0) | 240.0 (70.0–870.0) | <0.001 * |
| Eosinophils cells/mm³ | 60–1470 | 645 (60–1260) | 955 (330–3910) | 490 (200–1060) | 0.009 ¶ |
| Platelets cells/mm³ | 150,000–500,000 | 208,000 (45,000–563,000) | 362,000 (58,000–615,000) | 332,000 (95,000–618,000) | 0.033 † |
| Basophils cells/mm³ | 0–60 | 20 (0–40) | 20 (10–60) | 10 (0–30) | <0.001 ‡ |
| Creatinine mg/dL | 0.8–1.6 | 1.46 (0.78–1.90) | 0.82 (0.67–2.13) | 2.98 (1.52–9.49) | <0.001 * |
| Creatinine > 1.6 mg/dL, n (%) | – | – | 1/14 (7%) | 19/21 (90%) | <0.001 |
| Urea mg/dL | 30–65 | 46.48 (31.47–73.01) | 45.35 (30.20–63.30) | 99.4 (41.51–318.82) | <0.001 ‡ |
| SDMA µg/dL | <18 | 12.5 (7.0–18.0) | 10.0 (6.0–15.0) | 21.5 (7.0–50.0) | <0.001 ‡ |
| SDMA ≥ 18 µg/dL, n (%) | – | – | 0/14 | 12/18 (67%) | <0.001 * |
| Total calcium mg/dL | 8.5–10.5 | 9.75 (8.80–10.80) | 9.20 (8.24–10.38) | 10.10 (8.30–11.60) | 0.004 ¶ |
| Ionized calcium mmol/L | 1.19–1.38 | 1.27 (1.07–1.34) | 1.25 (0.80–1.40) | 1.32 (1.07–1.50) | 0.001 ‡ |
| Phosphate mg/dL | 2.5–6.2 | 4.4 (3.0–6.1) | 5.43 (3.79–6.50) | 4.9 (4.0–12.3) | 0.010 † |
| Sodium mEq/L | 145–155 | 151.0 (147.0–155.0) | 149.0 (147.0–154.0) | 151.0 (143.0–157.0) | 0.299 |
| Chloride mEq/L | 110–123 | 119.0 (113.0–129.0) | 120.5 (117.0–125.0) | 116.6 (108.4–125.0) | 0.022 † |
| Potassium mEq/L | 3.4–5.1 | 4.2 (3.4–4.9) | 4.93 (4.08–5.38) | 4.2 (3.1–4.8) | <0.001 ¶ |
| Magnesium mg/dL | 1.9–2.8 | 2.30 (2.12–2.48) | 2.32 (2.04–2.72) | 2.27 (1.80–3.66) | 0.952 |
| Total proteins g/dL | 6.5–8.8 | 7.72 (7.06–8.89) | 7.87 (7.05–9.12) | 7.51 (5.36–9.97) | 0.790 |
| Albumin g/dL | 2.6–4.0 | 3.6 (2.0–4.0) | 3.1 (2.5–3.7) | 3.0 (2.3–3.4) | <0.001 † |
| A:G | 0.52–1.20 | 0.85 (0.58–1.28) | 0.63 (0.37–0.87) | 0.67 (0.37–0.90) | 0.001 † |
| Glucose mg/dL | 65–148 | 99.5 (71.0–240.0) | 85.0 (62.0–193.0) | 106.0 (72.0–148.0) | 0.055 |
| AST U/L | 9–40 | 25.5 (16.0–157.0) | 23.5 (5.0–65.0) | 28.0 (17.0–79.0) | 0.419 |
| ALT U/L | 20–72 | 47.5 (33.0–92.0) | 55.0 (20.0–117.0) | 58.0 (20.0–224.0) | 0.309 |
| GGT U/L | 0–4 | 0.1 (0.1–0.6) | 0.1 (0.0–1.3) | 0.1 (0.1–2.3) | 0.590 |
| ALP U/L | 20–140 | 69.0 (22.0–163.0) | 26.5 (13.0–120.0) | 45.0 (16.0–128.0) | <0.001 * |
| Total bilirubin mg/dL | 0–0.35 | 0.18 (0.10–0.31) | 0.08 (0.05–0.20) | 0.19 (0.14–0.32) | <0.001 ¶ |
| Total cholesterol mg/dL | 59–230 | 130.5 (45.0–370.0) | 86.0 (55.0–142.0) | 195.0 (81.0–478.0) | <0.001 * |
| Variable | RI | Healthy (n = 22) | FeMV (n = 14) | CKD (n = 21) | p Value |
|---|---|---|---|---|---|
| USG | >1035 | 1067 (1040–1080) | 1054 (1022–1060) | 1017 (1008–1040) | <0.001 * |
| USG < 1035, n (%) | – | – | 1/14 (7 %) | 19/21 (90 %) | <0.001 |
| uCreatinine mg/dL | 120–593 | 406.5 (117.8–575.6) | 227.2 (83.0–489.8) | 112.7 (48.4–489.6) | <0.001 * |
| uUrea mg/dL | 1500–10700 | 7597.8 (3650.6–9235.1) | 5174.9 (1625.2–6508.3) | 2225.8 (967.6–6478.8) | <0.001 * |
| uTP mg/dL | 21–134 | 41.14 (22.09–151.24) | 41.97 (16.44–172.74) | 33.42 (5.96–337.90) | 0.244 |
| UPC | 0.01–0.4 | 0.1 (0.04–0.25) | 0.20 (0.08–1.03) | 0.23 (0.10–0.80) | <0.001 † |
| UPC 0.2–0.4, n (%) | – | – | 5/13 (38%) | 9/21 (43%) | 0.803 |
| UPC > 0.4, n (%) | – | – | 1/13 (8%) | 6/21 (29%) | 0.149 |
| uGlucose mg/dL | 4.0–14.0 | 8.0 (5.0–16.1) | 9.9 (3.3–139.0) | 2 (0–1408.0) | <0.001 ‡ |
| uNa mEq/L | 49.0–375.0 | 210.40 (20.40–296.0) | 83.10 (16.20–217.10) | 78.80 (13.10–298.20) | <0.001 † |
| uNa/uCrea | 0.15–1.0 | 0.51 (0.10–0.72) | 0.31 (0.07–1.23) | 0.76 (0.11–1.20) | 0.040 ‡ |
| FE Na% | 0–0.97 | 0.49 (0.08–0.88) | 0.19 (0.04–0.78) | 1.13 (0.21–6.11) | <0.001 ‡ |
| uK mEq/L | 60–231 | 134.30 (62.50–230.40) | 149.95 (85.0–200.40) | 53.50 (19.0–169.30) | <0.001 ‡ |
| uK/uCrea | 0.16–0.66 | 0.34 (0.15–0.64) | 0.68 (0.22–1.30) | 0.47 (0.16–0.76) | <0.001 * |
| FE K% | 7.0–22.0 | 11.87 (6.20–22.79) | 12.69 (8.63–27.12) | 38.96 (7.91–128.76) | <0.001 ‡ |
| uCa mg/dL | 1.0–10.0 | 2.40 (1.0–11.60) | 2.05 (1.10–3.50) | 2.40 (0.80–9.40) | 0.586 |
| uCa/uCrea | 0–0.03 | 0.01 (0–0.03) | 0.01 (0–0.03) | 0.02 (0–0.14) | <0.001 ‡ |
| FE Ca% | 0–0.26 | 0.09 (0.05–0.45) | 0.10 (0.04–0.26) | 0.72 (0.10–11.15) | <0.001 ‡ |
| uP mg/dL | 90.0–385.0 | 187.70 (105.20–381.30) | 230.0 (103.50–377.30) | 58.10 (9.7–268.20) | <0.001 ‡ |
| uP/uCrea | 0.25–1.13 | 0.51 (0–0.89) | 1.16 (0.32–2.26) | 0.55 (0.04–0.87) | <0.001 ¶ |
| FE P% | 0–40 | 16.51 (8.28–37.32) | 17.20 (9.54–38.15) | 31.55 (3.02–54.99) | 0.002 ‡ |
| uCl mEq/L | 51–366 | 179.40 (85.0–330.0) | 87.0 (10.50–133.0) | 190.50 (56.0–386.0) | <0.001 ‡ |
| uCl/uCrea | 0.13–1.10 | 0.43 (0.15–1.08) | 1.02 (0.14–2.47) | 0.64 (0.09–1.29) | 0.004 † |
| FE Cl% | 0.18–1.26 | 0.55 (0.20–1.08) | 0.80 (0.26–1.97) | 1.42 (0.21–9.15) | <0.001 ‡ |
| uMg mg/dL | 0.76–17 | 11.06 (3.0–19.40) | 8.07(1.04–14.64) | 4.15 (0.76–9.70) | 0.001 ‡ |
| uMg/uCrea | 0–0.05 | 0.03 (0.01–0.06) | 0.05 (0–0.09) | 0.04 (0–0.11) | 0.051 † |
| FE Mg% | 0.05–3.23 | 1.92 (0.41–3.22) | 1.72 (0.21–3.87) | 6.38 (0.15–31.61) | <0.001 ‡ |
| Total bands number | – | 13 (9–15) | 17 (5–24) | 15 (6–21) | 0.016 ∞ |
| HMM number | – | 6 (5–7) | 6 (2–8) | 4 (1–9) | 0.049 ‡ |
| LMM number | – | 7 (3–10) | 11 (3–17) | 9 (5–16) | 0.024 † |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crisi, P.E.; Dondi, F.; De Luca, E.; Di Tommaso, M.; Vasylyeva, K.; Ferlizza, E.; Savini, G.; Luciani, A.; Malatesta, D.; Lorusso, A.; et al. Early Renal Involvement in Cats with Natural Feline Morbillivirus Infection. Animals 2020, 10, 828. https://doi.org/10.3390/ani10050828
Crisi PE, Dondi F, De Luca E, Di Tommaso M, Vasylyeva K, Ferlizza E, Savini G, Luciani A, Malatesta D, Lorusso A, et al. Early Renal Involvement in Cats with Natural Feline Morbillivirus Infection. Animals. 2020; 10(5):828. https://doi.org/10.3390/ani10050828
Chicago/Turabian StyleCrisi, Paolo Emidio, Francesco Dondi, Eliana De Luca, Morena Di Tommaso, Kateryna Vasylyeva, Enea Ferlizza, Giovanni Savini, Alessia Luciani, Daniela Malatesta, Alessio Lorusso, and et al. 2020. "Early Renal Involvement in Cats with Natural Feline Morbillivirus Infection" Animals 10, no. 5: 828. https://doi.org/10.3390/ani10050828