
Strongyloidiasis in Children Outside the Tropics: Do We Need to Increase Awareness?

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Definitions
2.3. Laboratory Methods
2.4. Statistical Analysis
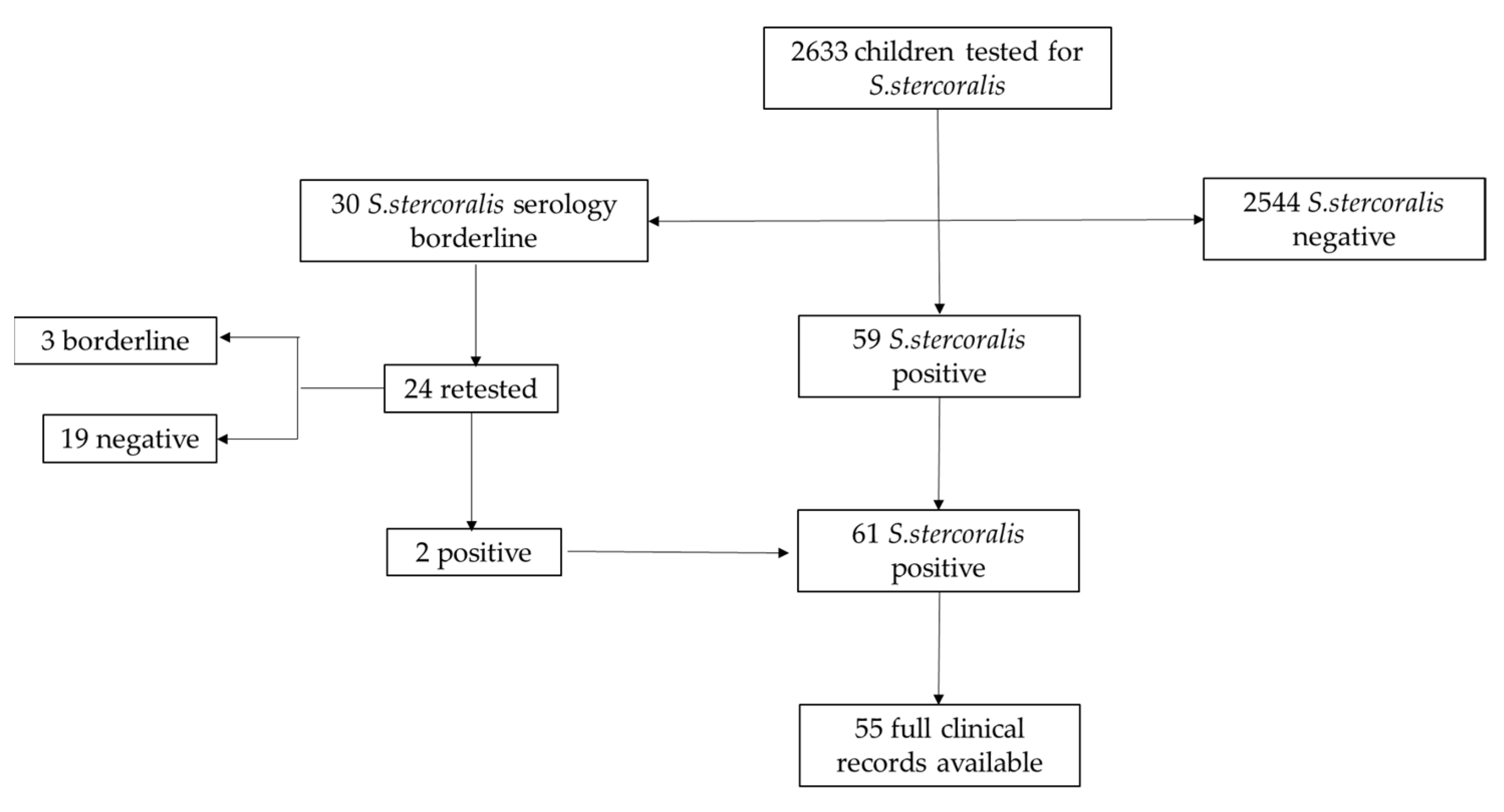
3. Results
3.1. Assessment of Children with Borderline Serology
3.2. Assessment of Children with Positive Index
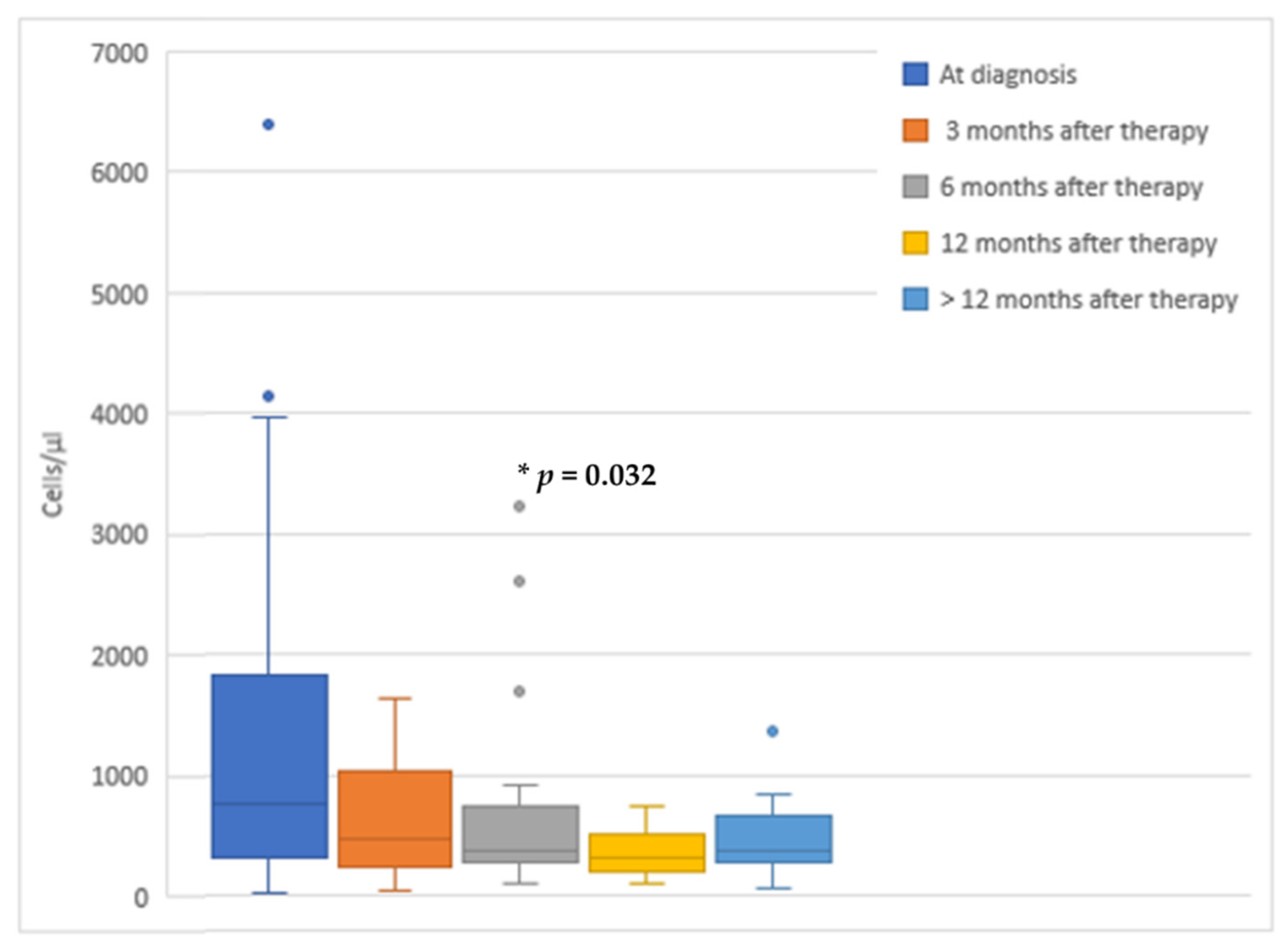
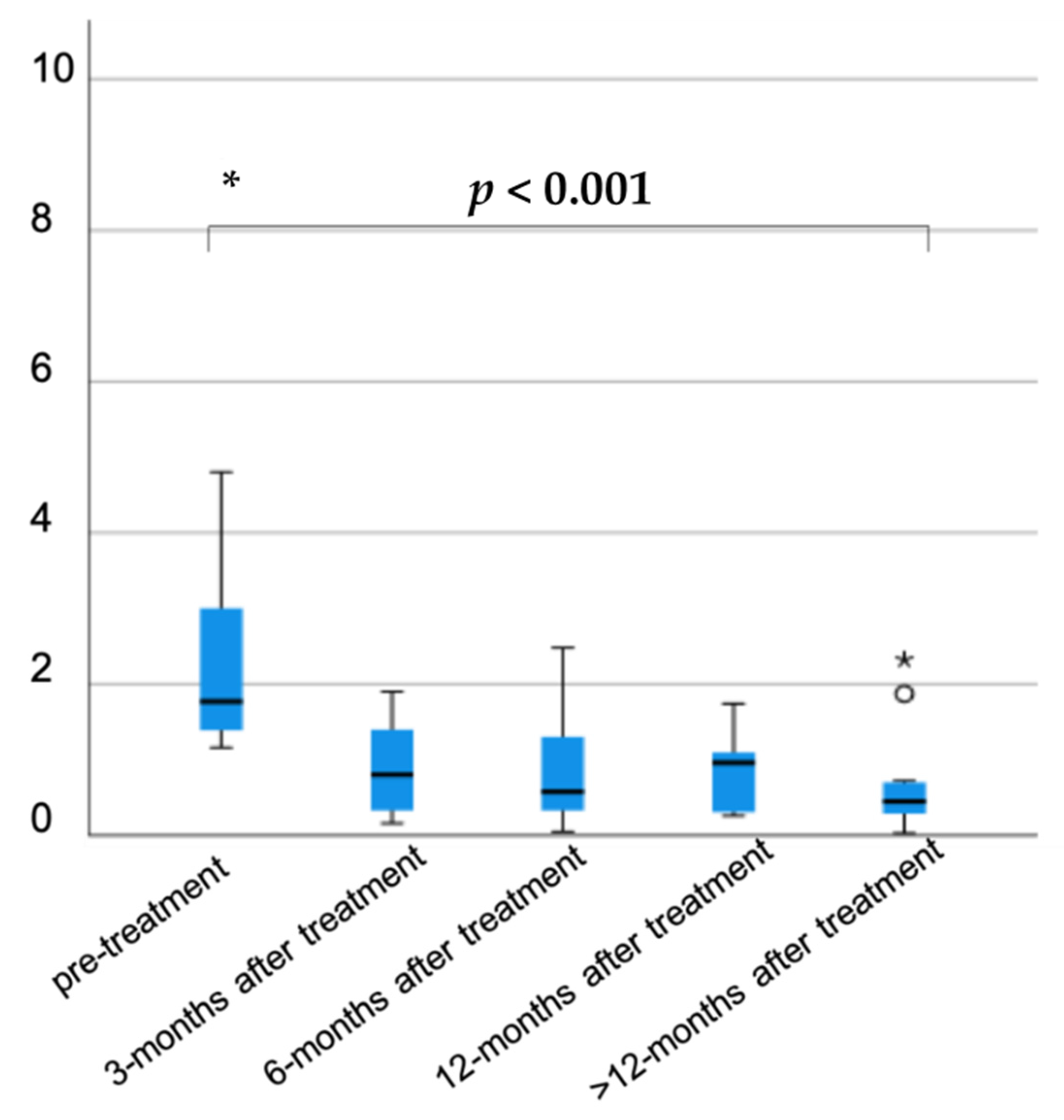
3.3. Assessment of Therapeutic Response of Patients with Positive Serology for S. stercoralis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hotez, P.J.; Aksoy, S.; Brindley, P.J.; Kamhawi, S. What constitutes a neglected tropical disease? PLoS Negl. Trop. Dis. 2020, 14, e0008001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lingscheid, T.; Witzenrath, M.; Bouchaud, O.; Kern, P.; Da Cunha, J.S.; Beltrame, A.; Zammarchi, L.; Paul, M.; Kosina, P.; Marocco, S.; et al. Schistosomiasis in European Travelers and Migrants: Analysis of 14 Years TropNet Surveillance Data. Am. J. Trop. Med. Hyg. 2017, 97, 567–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zammarchi, L.; Gobbi, F.; Angheben, A.; Spinicci, M.; Buonfrate, D.; Calleri, G.; De Paola, M.; Bevilacqua, N.; Carrara, S.; Attard, L.; et al. Schistosomiasis, strongyloidiasis and Chagas disease: The leading imported neglected tropical diseases in Italy. J. Travel Med. 2019, 27. [Google Scholar] [CrossRef] [PubMed]
- Buonfrate, D.; Bisanzio, D.; Giorli, G.; Odermatt, P.; Fürst, T.; Greenaway, C.; French, M.; Reithinger, R.; Gobbi, F.; Montresor, A.; et al. The Global Prevalence of Strongyloides stercoralis Infection. Pathogens 2020, 9, 468. [Google Scholar] [CrossRef] [PubMed]
- Martelli, G.; Di Girolamo, C.; Zammarchi, L.; Angheben, A.; Morandi, M.; Tais, S.; Degani, M.; El Hamad, I.; Caligaris, S.; Ciannameo, A.; et al. Seroprevalence of five neglected parasitic diseases among immigrants accessing five infectious and tropical diseases units in Italy: A cross-sectional study. Clin. Microbiol. Infect. 2017, 23, 335.e1–335.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asundi, A.; Beliavsky, A.; Liu, X.J.; Akaberi, A.; Schwarzer, G.; Bisoffi, Z.; Mendez, A.R.; Shrier, I.; Greenaway, C. Prevalence of strongyloidiasis and schistosomiasis among migrants: A systematic review and meta-analysis. Lancet Glob. Health 2019, 7, e236–e248. [Google Scholar] [CrossRef] [Green Version]
- Khieu, V.; Schaer, F.; Marti, H.; Sayasone, S.; Duong, S.; Muth, S.; Odermatt, P. Diagnosis, Treatment and Risk Factors of Strongyloides stercoralis in Schoolchildren in Cambodia. PLoS Negl. Trop. Dis. 2013, 7, e2035. [Google Scholar] [CrossRef] [Green Version]
- Forrer, A.; Khieu, V.; Schär, F.; Hattendorf, J.; Marti, H.; Neumayr, A.; Char, M.C.; Hatz, C.; Muth, S.; Odermatt, P. Strongyloides stercoralis is associated with significant morbidity in rural Cambodia, including stunting in children. PLoS Negl. Trop. Dis. 2017, 11, e0005685. [Google Scholar] [CrossRef] [Green Version]
- Hailu, T.; Nibret, E.; Amor, A.; Munshea, A.; Anegagrie, M. Efficacy of Single Dose Ivermectin Against Strongyloides stercoralis Infection Among Primary School Children in Amhara National Regional State. Infect. Dis. Res. Treat. 2020, 13. [Google Scholar] [CrossRef]
- Amor, A.; Rodriguez, E.; Saugar, J.M.; Arroyo, A.; López-Quintana, B.; Abera, B.; Yimer, M.; Yizengaw, E.; Zewdie, D.; Ayehubizu, Z.; et al. High prevalence of Strongyloides stercoralis in school-aged children in a rural highland of north-western Ethiopia: The role of intensive diagnostic work-up. Parasites Vectors 2016, 9, 617. [Google Scholar] [CrossRef] [Green Version]
- Zammarchi, L.; Tilli, M.; Botta, A.; Buonfrate, D.; Bartoloni, A.; Boccalini, S. Strategies for management of strongyloidiasis in migrants from Sub-Saharan Africa recently arrived in Italy: A cost-effectiveness analysis. Travel Med. Infect. Dis. 2020, 36, 101561. [Google Scholar] [CrossRef] [PubMed]
- Von Both, U. Children on the move—A call for active screening in migrants. Lancet Child Adolesc. Health 2020, 4, 174–175. [Google Scholar] [CrossRef]
- Schaer, F.; Trostdorf, U.; Giardina, F.; Khieu, V.; Muth, S.; Marti, H.; Vounatsou, P.; Odermatt, P. Strongyloides stercoralis: Global Distribution and Risk Factors. PLoS Negl. Trop. Dis. 2013, 7, e2288. [Google Scholar] [CrossRef] [Green Version]
- Siddiqui, A.A.; Berk, S.L. Diagnosis ofStrongyloides stercoralisInfection. Clin. Infect. Dis. 2001, 33, 1040–1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Requena-Méndez, A.; Chiodini, P.; Bisoffi, Z.; Buonfrate, D.; Gotuzzo, E.; Muñoz, J. The Laboratory Diagnosis and Follow Up of Strongyloidiasis: A Systematic Review. PLoS Negl. Trop. Dis. 2013, 7, e2002. [Google Scholar] [CrossRef] [PubMed]
- Agbata, E.N.; Morton, R.L.; Bisoffi, Z.; Bottieau, E.; Greenaway, C.; Biggs, B.-A.; Montero, N.; Tran, A.; Rowbotham, N.; Arevalo-Rodriguez, I.; et al. Effectiveness of Screening and Treatment Approaches for Schistosomiasis and Strongyloidiasis in Newly-Arrived Migrants from Endemic Countries in the EU/EEA: A Systematic Review. Int. J. Environ. Res. Public Health 2018, 16, 11. [Google Scholar] [CrossRef] [Green Version]
- Olsen, A.; Van Lieshout, L.; Marti, H.; Polderman, T.; Polman, K.; Steinmann, P.; Stothard, R.; Thybo, S.; Verweij, J.J.; Magnussen, P. Strongyloidiasis—The most neglected of the neglected tropical diseases? Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 967–972. [Google Scholar] [CrossRef] [Green Version]
- Buonfrate, D.; Marrone, R.; Silva, R.; Mirisola, C.; Ragusa, A.; Mistretta, M.; Perandin, F.; Bisoffi, Z. Prevalence of Strongyloidiasis in a Cohort of Migrants in Italy and Accuracy of a Novel ELISA Assay for S. stercoralis Infection, a Cross-Sectional Study. Microorganisms 2021, 9, 401. [Google Scholar] [CrossRef]
- Buonfrate, D.; Angheben, A.; Gobbi, F.; Muñoz, J.; Requena-Mendez, A.; Gotuzzo, E.; Mena, M.A.; Bisoffi, Z. Imported Strongyloidiasis: Epidemiology, Presentations, and Treatment. Curr. Infect. Dis. Rep. 2012, 14, 256–262. [Google Scholar] [CrossRef]
- Buonfrate, D.; Requena-Mendez, A.; Angheben, A.; Muñoz, J.; Gobbi, F.; Ende, J.V.D.; Bisoffi, Z. Severe strongyloidiasis: A systematic review of case reports. BMC Infect. Dis. 2013, 13, 78. [Google Scholar] [CrossRef] [Green Version]
- Bisoffi, Z.; Buonfrate, D.; Montresor, A.; Mendez, A.R.; Muñoz, J.; Krolewiecki, A.; Gotuzzo, E.; Mena, M.A.; Chiodini, P.; Anselmi, M.; et al. Strongyloides stercoralis: A Plea for Action. PLoS Negl. Trop. Dis. 2013, 7, e2214. [Google Scholar] [CrossRef] [Green Version]
- Buonfrate, D.; Salas-Coronas, J.; Muñoz, J.; Maruri, B.T.; Rodari, P.; Castelli, F.; Zammarchi, L.; Bianchi, L.; Gobbi, F.; Fernández, I.; et al. Multiple-dose versus single-dose ivermectin for Strongyloides stercoralis infection (Strong Treat 1 to 4): A multicentre, open-label, phase 3, randomised controlled superiority trial. Lancet Infect. Dis. 2019, 19, 1181–1190. [Google Scholar] [CrossRef]
- Gann, P.H.; Neva, F.A.; Gam, A.A. A Randomized Trial of Single- and Two-Dose Ivermectin versus Thiabendazole for Treatment of Strongyloidiasis. J. Infect. Dis. 1994, 169, 1076–1079. [Google Scholar] [CrossRef] [PubMed]
- Henriquez-Camacho, C.; Gotuzzo, E.; Echevarria, J.; Jr, A.C.W.; Terashima, A.; Samalvides, F.; Perez-Molina, J.A.; Plana, M.N. Ivermectin versus albendazole or thiabendazole for Strongyloides stercoralis infection. Cochrane Database Syst. Rev. 2016, 1, CD007745. [Google Scholar] [CrossRef] [Green Version]
- Jittamala, P.; Monteiro, W.; Smit, M.R.; Pedrique, B.; Specht, S.; Chaccour, C.J.; Dard, C.; Del Giudice, P.; Khieu, V.; Maruani, A.; et al. A systematic review and an individual patient data meta-analysis of ivermectin use in children weighing less than fifteen kilograms: Is it time to reconsider the current contraindication? PLoS Negl. Trop. Dis. 2021, 15, e0009144. [Google Scholar] [CrossRef]
- Suputtamongkol, Y.; Premasathian, N.; Bhumimuang, K.; Waywa, D.; Nilganuwong, S.; Karuphong, E.; Anekthananon, T.; Wanachiwanawin, D.; Silpasakorn, S. Efficacy and Safety of Single and Double Doses of Ivermectin versus 7-Day High Dose Albendazole for Chronic Strongyloidiasis. PLoS Negl. Trop. Dis. 2011, 5, e1044. [Google Scholar] [CrossRef] [Green Version]
- Nontasut, P.; Muennoo, C.; Sa-nguankiat, S.; Fongsri, S.; Vichit, A. Prevalence of strongyloides in Northern Thailand and treat-ment with ivermectin vs. albendazole. Southeast Asian J. Trop. Med. Public Health 2005, 36, 442–444. [Google Scholar]
- Datry, A.; Hilmarsdottir, I.; Mayorga-Sagastume, R.; Lyagoubi, M.; Gaxotte, P.; Biligui, S.; Chodakewitz, J.; Neu, D.; Danis, M.; Gentilini, M. Treatment of Strongyloides stercoralis infection with ivermectin compared with albendazole: Results of an open study of 60 cases. Trans. R. Soc. Trop. Med. Hyg. 1994, 88, 344–345. [Google Scholar] [CrossRef]
- Marti, H.; Hatz, C.; Chwaya, H.M.; Haji, H.J.; Mgeni, A.F.; Ameir, J.S.; Savioli, L. A Comparative Trial of a Single-Dose Ivermectin Versus Three Days of Albendazole for Treatment of Strongyloides Stercoralis and Other Soil-Transmitted Helminth Infections in Children. Am. J. Trop. Med. Hyg. 1996, 55, 477–481. [Google Scholar] [CrossRef]
- Kobayashi, J.; Sato, Y.; Toma, H.; Takara, M.; Shiroma, Y. Application of enzyme immunoassay for postchemotherapy evaluation of human strongyloidiasis. Diagn. Microbiol. Infect. Dis. 1994, 18, 19–23. [Google Scholar] [CrossRef]
- Nuesch, R.; Zimmerli, L.; Stockli, R.; Gyr, N.; Hatz, F.C. Imported Strongyloidosis: A Longitudinal Analysis of 31 Cases. J. Travel Med. 2006, 12, 80–84. [Google Scholar] [CrossRef] [Green Version]
- Loutfy, M.R.; Kain, K.; Wilson, M.; Keystone, J.S. Serology and eosinophil count in the diagnosis and management of strongyloidiasis in a non-endemic area. Am. J. Trop. Med. Hyg. 2002, 66, 749–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burris, D.; Rosenberg, C.E.; Schwartz, J.T.; Zhang, Y.; Eby, M.D.; Abonia, J.P.; Fulkerson, P.C. Pediatric Hypereosinophilia: Characteristics, Clinical Manifestations, and Diagnoses. J. Allergy Clin. Immunol. Pract. 2019, 7, 2750–2758.e2. [Google Scholar] [CrossRef]
- Buonfrate, D.; Perandin, F.; Formenti, F.; Bisoffi, Z. A retrospective study comparing agar plate culture, indirect immunofluorescence and real-time PCR for the diagnosis of Strongyloides stercoralis infection. Parasitology 2017, 144, 812–816. [Google Scholar] [CrossRef]
- Al-Mekhlafi, H.M.; Nasr, N.A.; Lim, Y.A.L.; Elyana, F.N.; Sady, H.; Atroosh, W.M.; Dawaki, S.; Anuar, T.S.; Noordin, R.; Mahmud, R. Prevalence and risk factors of Strongyloides stercoralis infection among Orang Asli schoolchildren: New insights into the epidemiology, transmission and diagnosis of strongyloidiasis in Malaysia. Parasitology 2019, 146, 1602–1614. [Google Scholar] [CrossRef]
- Ottino, L.; Buonfrate, D.; Paradies, P.; Bisoffi, Z.; Antonelli, A.; Rossolini, G.M.; Gabrielli, S.; Bartoloni, A.; Zammarchi, L. Autochthonous Human and Canine Strongyloides stercoralis Infection in Europe: Report of a Human Case in An Italian Teen and Systematic Review of the Literature. Pathogens 2020, 9, 439. [Google Scholar] [CrossRef] [PubMed]
- Ross, S.A.; Pintilie, H.; Hatcher, J.; Dosekun, O.; Cooke, G.S.; Bailey, A.C. Strongyloides stercoralis infection in HIV-positive men who have sex with men. Int. J. STD AIDS 2020, 31, 398–401. [Google Scholar] [CrossRef]
- Salvador, F.; Treviño, B.; Chamorro-Tojeiro, S.; Sánchez-Montalvá, A.; Herrero-Martínez, J.M.; Rodríguez-Guardado, A.; Serre-Delcor, N.; Torrús, D.; Goikoetxea, J.; Zubero, Z.; et al. Imported strongyloidiasis: Data from 1245 cases registered in the +REDIVI Spanish Collaborative Network (2009–2017). PLoS Negl. Trop. Dis. 2019, 13, e0007399. [Google Scholar] [CrossRef] [Green Version]
- DaCal, E.; Saugar, J.M.; De Lucio, A.; Hernández-De-Mingo, M.; Robinson, E.; Köster, P.C.; Aznar-Ruiz-De-Alegría, M.L.; Espasa, M.; Ninda, A.; Gandasegui, J.; et al. Prevalence and molecular characterization of Strongyloides stercoralis, Giardia duodenalis, Cryptosporidium spp., and Blastocystis spp. isolates in school children in Cubal, Western Angola. Parasites Vectors 2018, 11, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Bisoffi, Z.; Buonfrate, D.; Sequi, M.; Mejia, R.; Cimino, R.O.; Krolewiecki, A.; Albonico, M.; Gobbo, M.; Bonafini, S.; Angheben, A.; et al. Diagnostic Accuracy of Five Serologic Tests for Strongyloides stercoralis Infection. PLoS Negl. Trop. Dis. 2014, 8, e2640. [Google Scholar] [CrossRef] [Green Version]
- Salvador, F.; Lucas-Dato, A.; Roure, S.; Arsuaga, M.; Pérez-Jacoiste, A.; García-Rodríguez, M.; Pérez-Molina, J.; Buonfrate, D.; Saugar, J.; Molina, I. Effectiveness and Safety of a Single-Dose Ivermectin Treatment for Uncomplicated Strongyloidiasis in Immunosuppressed Patients (ImmunoStrong Study): The Study Protocol. Pathogens 2021, 10, 812. [Google Scholar] [CrossRef]
- Repetto, S.A.; Ruybal, P.; Batalla, E.; López, C.; Fridman, V.; Sierra, M.; Radisic, M.; Bravo, P.M.; Risso, M.G.; Cappa, S.M.G.; et al. Strongyloidiasis Outside Endemic Areas: Long-term Parasitological and Clinical Follow-up After Ivermectin Treatment. Clin. Infect. Dis. 2018, 66, 1558–1565. [Google Scholar] [CrossRef] [PubMed]
- Salim, N.; Schindler, T.; Abdul, U.; Rothen, J.; Genton, B.; Lweno, O.; Mohammed, A.S.; Masimba, J.; Kwaba, D.; Abdulla, S.; et al. Enterobiasis and strongyloidiasis and associated co-infections and morbidity markers in infants, preschool- and school-aged children from rural coastal Tanzania: A cross-sectional study. BMC Infect. Dis. 2014, 14, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Noordin, R.; Yunus, M.H.; Farrizam, S.N.T.; Arifin, N. Serodiagnostic methods for diagnosing larval toxocariasis. Adv. Parasitolo. 2020, 131–152. [Google Scholar] [CrossRef]
- Calleri, G.; Angheben, A.; Albonico, M. Neglected tropical diseases in Europe: Rare diseases and orphan drugs? Infection 2018, 47, 3–5. [Google Scholar] [CrossRef] [Green Version]
- Siddiqui, A.A.; Genta, R.M.; Maguilnik, I.; Berk, S.L. Strongyloidiasis. In Tropical Infectious Diseases: Principles, Pathogens, and Practice, 3rd ed.; Guerrant, R.L., Walker, D.H., Weller, P.F., Eds.; Churchill Livingstone: Philadelphia, PA, USA, 2010; pp. 805–812. [Google Scholar]
- Nielsen, P.B.; Mojon, M. Improved diagnosis of strongyloides stercoralis by seven consecutive stool specimens. Med. Microbiol. Infect. Dis. Virol. Parasitol. 1987, 263, 616–618. [Google Scholar] [CrossRef]
- Monge-Maillo, B.; Norman, F.; Perez-Molina, J.A.; Navarro, M.; Díaz-Menéndez, M.; López-Vélez, R. Travelers visiting friends and relatives (VFR) and imported infectious disease: Travelers, immigrants or both? A comparative analysis. Travel Med. Infect. Dis. 2014, 12, 88–94. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient (Sex, Age) | Home Country | Eosinophil Level (Cells/µL) | Clinical Signs/Symptoms | Comorbidities | Result of S. stercoralis on Stool Samples | Result of S. stercoralis Serology (Second Retesting) |
|---|---|---|---|---|---|---|
| Patient 1 (M/8 years) | Colombia | 225 | No | No | Negative (ME) | Negative |
| Patient 2 (M/10 years) | India | 456 | No | Latent TB | Negative (ME) | Negative |
| Patient 3 (M/2 years) | Mali | 153 | No | Anemia | Negative (ME and AC) | Lost at FU |
| Patient 4 (F/11 years) | Colombia | 1369 | No | No | Negative (ME) | Positive |
| Patient 5 (M/3 years) | Thailand | 1667 | No | Toxocariasis | Negative (ME and AC) | Lost at FU |
| Patient 6 (F/3 months) | Italy | 950 | No | No | Negative (ME) | Negative |
| Patient 7 (M/10 years) | India | 509 | No | Latent TB | Negative (ME) | Negative |
| Patient 8 (M/11 years) | Italy | 1480 | No | No | Not performed | Negative |
| Patient 9 (M/12 years) | Pakistan | 600 | No | No | Negative (ME and AC) | Lost at FU |
| Patient 10 (M/11 years) | Italy | 890 | No | No | Negative (ME) | Negative |
| Patient 11 (M/6 years) | Pakistan | 5000 | No | elevated IgE value | Negative (ME) | Negative |
| Patient 12 (M/14 years) | Russia | 360 | No | No | Negative (ME) | Negative |
| Patient 13 (F/5 months) | Pakistan | 690 | No | No | Negative (ME) | Lost at FU |
| Patient 14 (F/6 years) | India | 227 | No | No | Negative (ME and AC) | Positive |
| Patient 15 (F/10 years) | Colombia | 348 | No | No | Negative (ME and AC) | Negative |
| Patient 16 (M/10 years) | Colombia | 258 | No | No | Negative (ME and AC) | Negative |
| Patient 17 (F/10 years) | Hungary | 209 | No | Giardiasis | Negative (ME and AC) | Negative |
| Patient 18 (F/9 years) | Kosovo | 300 | No | No | Negative (ME and AC) | Borderline |
| Patient 19 (F/10 years) | Chile | 64 | No | Giardiasis | Negative (ME) | Borderline |
| Patient 20 (F/17 years) | Romania | 100 | No | No | Negative (ME) | Negative |
| Patient 21 (M/11 years) | Senegal | 220 | No | Latent TB | Negative (ME) | Negative |
| Patient 22 (M/8 years) | India | 189 | No | No | Negative (ME) | Negative |
| Patient 23 (M/11 years) | Senegal | 6575 | Abdominal pain | S. haematobium infection | Negative (ME) | Borderline |
| Patient 24 (F/12 years) | Philippines | 440 | No | Latent TB | Negative (ME) | Negative |
| Patient 25 (F/16 years) | Nigeria | 25 | No | Latent TB | Negative (ME) | Lost at FU |
| Patient 26 (M/7 years) | Hungary | 95 | No | No | Negative (ME) | Negative |
| Patient 27 (F/15 years) | Romania | 478 | No | Toxocariasis | Negative (ME) | Negative |
| Patient 28 (M/11 years) | Peru | 176 | No | No | Negative (ME and AC) | Negative |
| Patient 29 (M/11 years) | Peru | 510 | No | Pleural TB | Negative (ME) | Negative |
| Patient 30 (F/6 years) | Italy | 280 | Not known | Not known | Negative (ME) | Negative |
| Patient (Sex, Age) | Year of Diagnosis | Parents Home Country | Serology Titer | Eosinophil Count (Cells/µL) | Symptoms | Toxocara canis Serology | Other Co-Infections | Other Anti-Parasite Treatment | S. stercoralis on Stool | Therapy | Serology Negativization | Normalization of Eosinophil Count after Therapy |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient 1 (F/6 years) | 2011 | Italy | 3.1 | 585 | pruritis, nonspecific skin eruption | Negative | Pinworms | Pyrantel pamoate | No (ME) 1 | Ivermectin | Yes | Yes |
| Patient 2 (F/8 months) | 2014 | Italy | 1.6 | 10,673 | Vomiting, anorexia | Negative | No | No | No (ME) | Albendazole | Yes | Yes |
| Patient 3 (M/11 years) | 2015 | Italy | 1.97 | 1128 | Cough and wheezing | Negative | No | No | No (ME) | Ivermectin | Yes | Yes |
| Patient 4 (F/15 years) | 2015 | Italy | 1.54 | 154 | hepato-splenic calcifications | Negative | No | No | No (ME) | No | Yes | |
| Patient 5 (M/10 years) | 2015 | China | 2 | 278 | pruritis, urticaria | Positive | No | No | No (ME) | No | Unknown | |
| Patient 6 (M,9 years) | 2016 | Kosovo | 1.63 | 34 | Cough | Negative | No | No | No (ME and AC) 2 | Ivermectin | Yes | Yes |
| Patient 7 (M,14 years) | 2017 | Italy | 1.81 | 3959 | Eosinophilic pneumonia | Negative | No | No | No (ME and AC) | Ivermectin | Yes | Yes |
| Patient 8 (F/6 years) | 2019 | Perú | 1.46 | 1963 | pruritis, abdominal pain | No | No | No | No (ME) | Ivermectin | Yes | Yes |
| Clinical Signs/Symptoms | n (%) |
|---|---|
| Cough and wheezing | 10 (18.2%) |
| Itch | 10 (18.2%) |
| Nonspecific skin rash | 7 (12.7%) |
| Abdominal pain | 6 (10.9%) |
| Vomiting | 3 (5.5%) |
| Urticaria | 2 (3.6%) |
| Diarrhoea | 2 (3.6%) |
| Larva currens | 1 (1.8%) |
| Anorexia | 1 (1.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Venturini, E.; Fusani, L.; Mantella, A.; Bianchi, L.; Antonelli, A.; Montagnani, C.; Chiappini, E.; Spinicci, M.; Bartoloni, A.; Rossolini, G.M.; et al. Strongyloidiasis in Children Outside the Tropics: Do We Need to Increase Awareness? Microorganisms 2021, 9, 1905. https://doi.org/10.3390/microorganisms9091905
Venturini E, Fusani L, Mantella A, Bianchi L, Antonelli A, Montagnani C, Chiappini E, Spinicci M, Bartoloni A, Rossolini GM, et al. Strongyloidiasis in Children Outside the Tropics: Do We Need to Increase Awareness? Microorganisms. 2021; 9(9):1905. https://doi.org/10.3390/microorganisms9091905
Chicago/Turabian StyleVenturini, Elisabetta, Lara Fusani, Antonia Mantella, Leila Bianchi, Alberto Antonelli, Carlotta Montagnani, Elena Chiappini, Michele Spinicci, Alessandro Bartoloni, Gian Maria Rossolini, and et al. 2021. "Strongyloidiasis in Children Outside the Tropics: Do We Need to Increase Awareness?" Microorganisms 9, no. 9: 1905. https://doi.org/10.3390/microorganisms9091905