
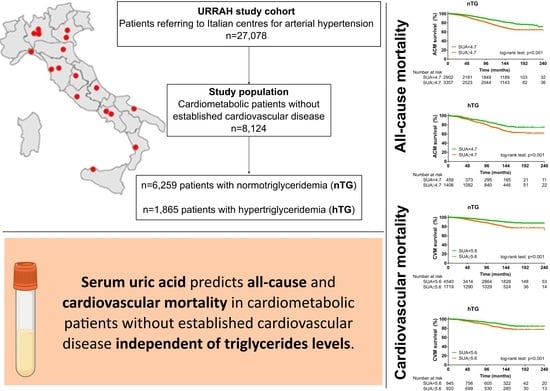
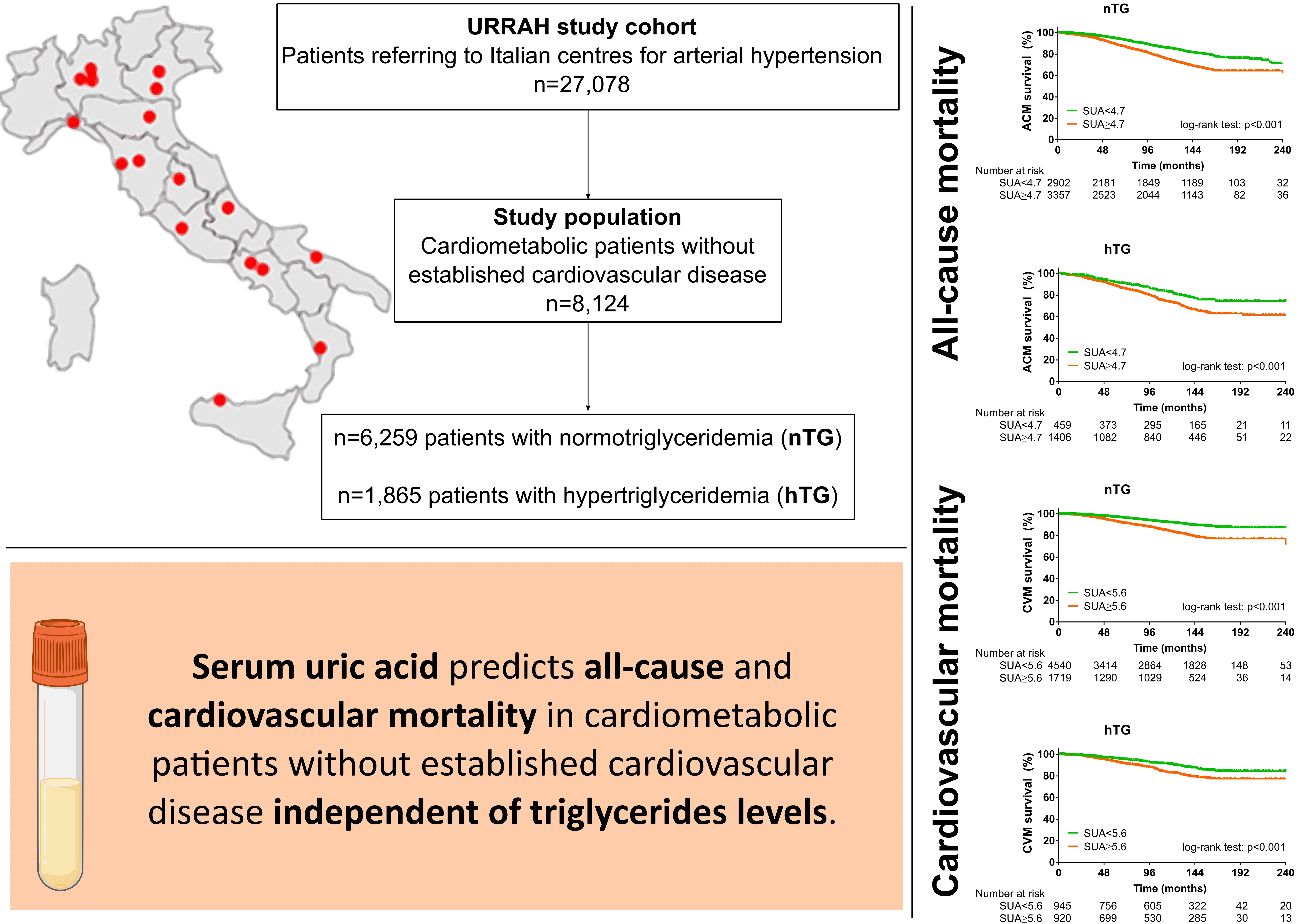
Serum Uric Acid Predicts All-Cause and Cardiovascular Mortality Independently of Hypertriglyceridemia in Cardiometabolic Patients without Established CV Disease: A Sub-Analysis of the URic acid Right for heArt Health (URRAH) Study
 , , , , , , , , , , , , ,
, , , , , , , , , , , , ,  , , , , , , , , , , , , , , and
on behalf of the Working Group on Uric Acid and Cardiovascular Risk of the Italian Society of Hypertension (SIIA)add
Show full author list
, , , , , , , , , , , , , , and
on behalf of the Working Group on Uric Acid and Cardiovascular Risk of the Italian Society of Hypertension (SIIA)add
Show full author list
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Protocol Design
2.2. Adoption of Specific SUA and TG Cut-Offs
2.3. Cardiometabolic Disease Definitions
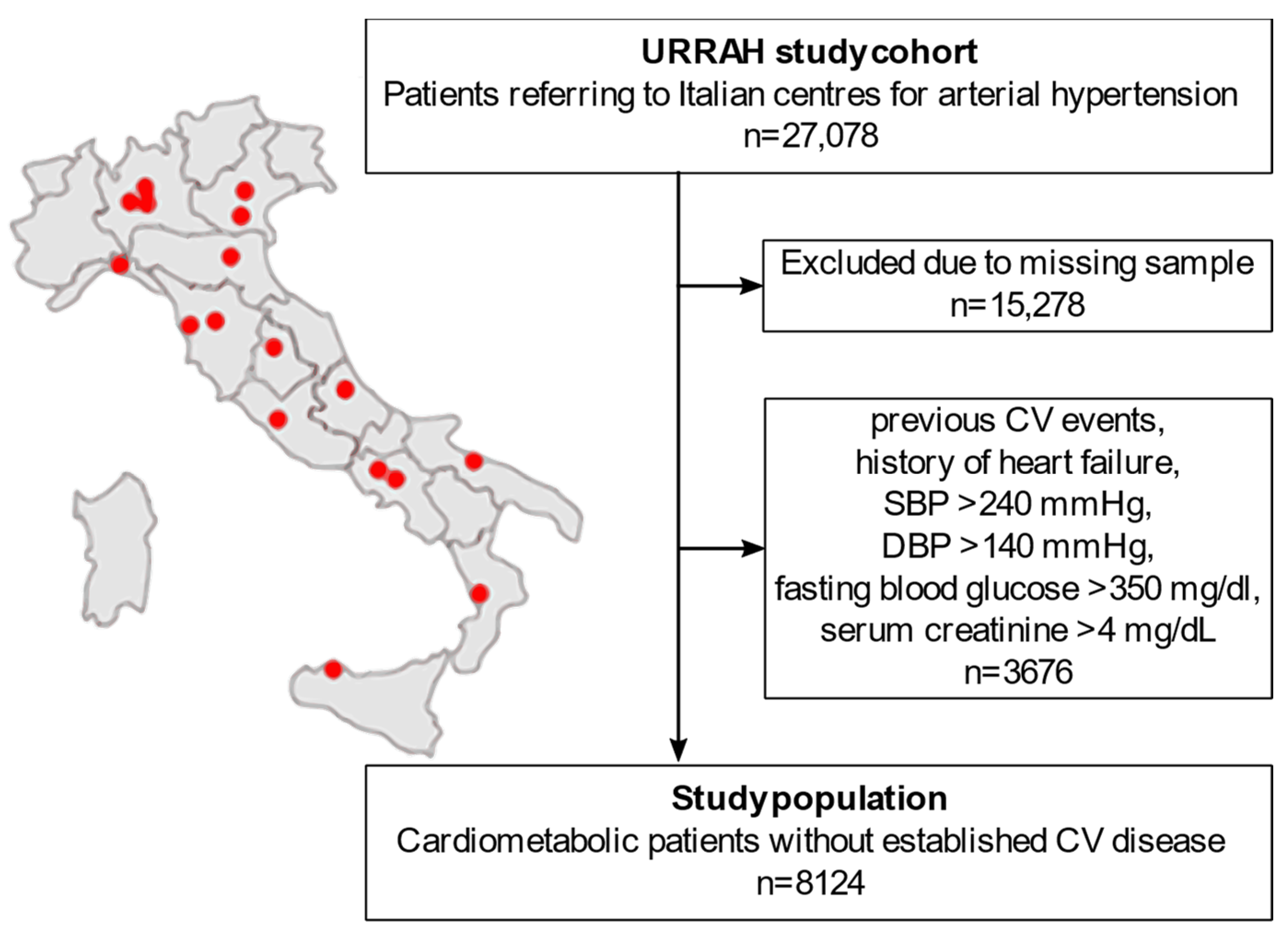
2.4. Study Population Selection from the National Regional-Based Dataset
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Baseline Characterisation of the Study Population Selected from the National Regional-Based Dataset
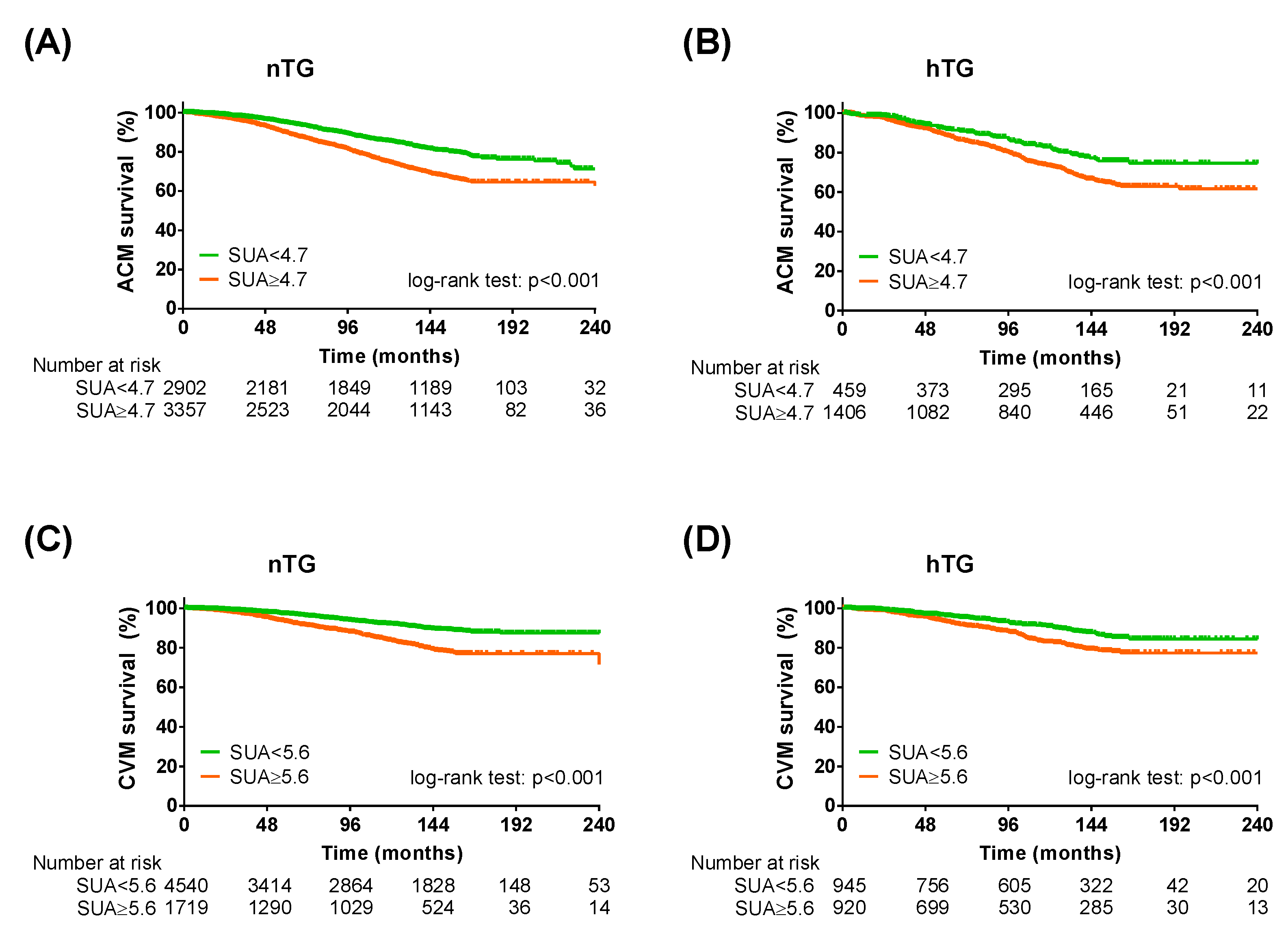
3.2. The Predictive Power of SUA Cut-Offs in Normotriglyceridemia and Hypertriglyceridemia
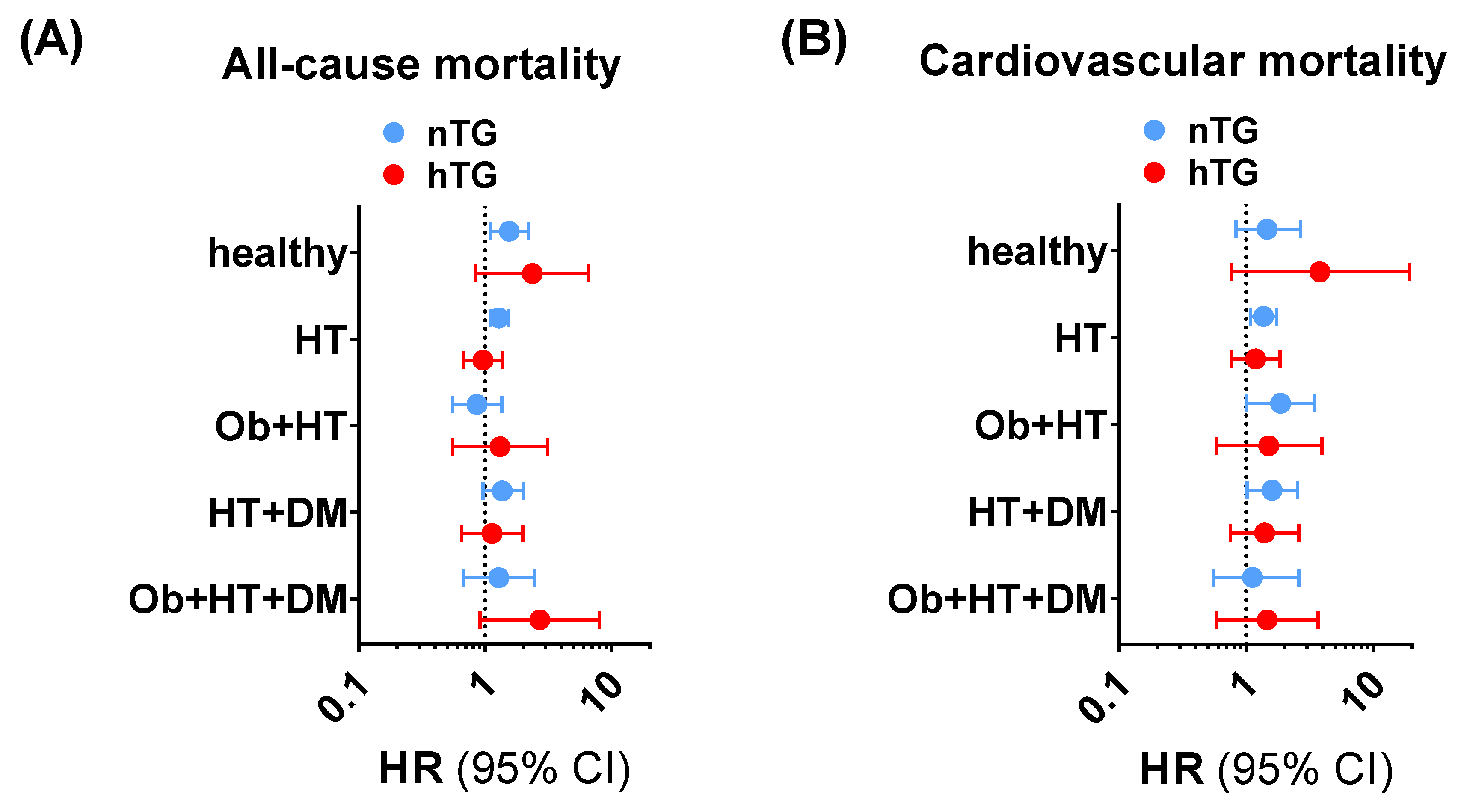
3.3. Predictive Value of SUA across the Cardiometabolic Spectrum
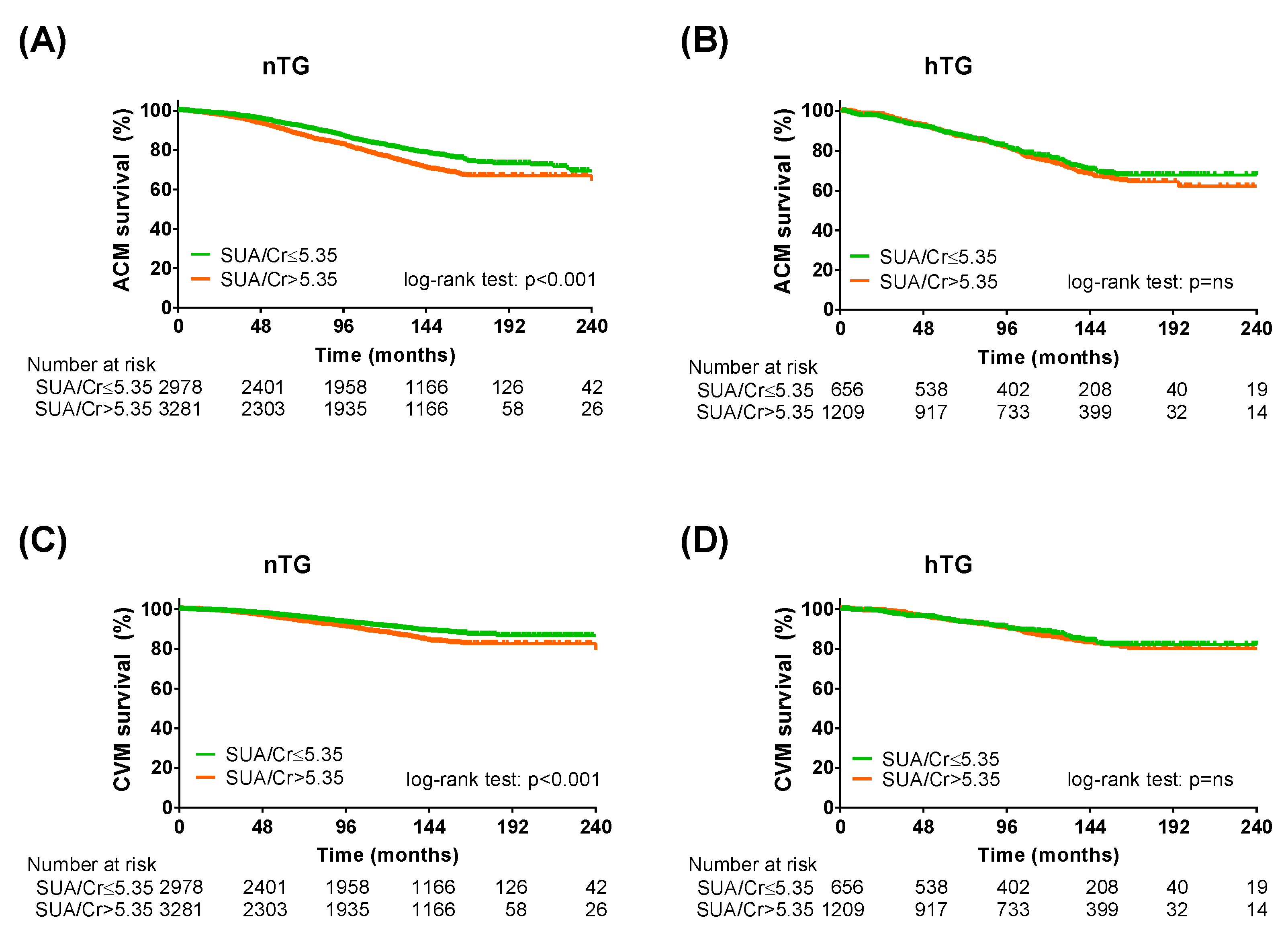
3.4. Sensitivity Analysis Adopting SUA/Serum Creatinine Ratio
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Costantino, S.; Paneni, F.; Cosentino, F. Ageing, metabolism and cardiovascular disease. J. Physiol. 2016, 594, 2061–2073. [Google Scholar] [CrossRef] [PubMed]
- Ward, Z.J.; Bleich, S.N.; Cradock, A.L.; Barrett, J.L.; Giles, C.M.; Flax, C.; Long, M.W.; Gortmaker, S.L. Projected U.S. State-level prevalence of adult obesity and severe obesity. N. Engl. J. Med. 2019, 381, 2440–2450. [Google Scholar] [CrossRef] [PubMed]
- Dunlay, S.M.; Roger, V.L.; Redfield, M.M. Epidemiology of heart failure with preserved ejection fraction. Nat. Rev. Cardiol. 2017, 14, 591–602. [Google Scholar] [CrossRef] [PubMed]
- Paneni, F.; Mocharla, P.; Akhmedov, A.; Costantino, S.; Osto, E.; Volpe, M.; Lüscher, T.F.; Cosentino, F. Gene silencing of the mitochondrial adaptor p66(shc) suppresses vascular hyperglycemic memory in diabetes. Circ. Res. 2012, 111, 278–289. [Google Scholar] [CrossRef]
- Reddy, M.A.; Zhang, E.; Natarajan, R. Epigenetic mechanisms in diabetic complications and metabolic memory. Diabetologia 2015, 58, 443–455. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. 2021 esc guidelines on cardiovascular disease prevention in clinical practice. Eur. J. Prev. Cardiol. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G.; et al. Primary care-led weight management for remission of type 2 diabetes (direct): An open-label, cluster-randomised trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef]
- Mengozzi, A.; Costantino, S.; Paneni, F.; Duranti, E.; Nannipieri, M.; Mancini, R.; Lai, M.; La Rocca, V.; Puxeddu, I.; Antonioli, L.; et al. Targeting sirt1 rescues age- and obesity-induced microvascular dysfunction in ex-vivo human vessels. Circ. Res. 2022, 131, 476–491. [Google Scholar] [CrossRef]
- Drozdz, D.; Alvarez-Pitti, J.; Wójcik, M.; Borghi, C.; Gabbianelli, R.; Mazur, A.; Herceg-Čavrak, V.; Lopez-Valcarcel, B.G.; Brzeziński, M.; Lurbe, E.; et al. Obesity and cardiometabolic risk factors: From childhood to adulthood. Nutrients 2021, 13, 4176. [Google Scholar] [CrossRef]
- Wagner, S.; Lioret, S.; Girerd, N.; Duarte, K.; Lamiral, Z.; Bozec, E.; Van den Berghe, L.; Hoge, A.; Donneau, A.F.; Boivin, J.M.; et al. Association of dietary patterns derived using reduced-rank regression with subclinical cardiovascular damage according to generation and sex in the stanislas cohort. J. Am. Heart Assoc. 2020, 9, e013836. [Google Scholar] [CrossRef]
- Virdis, A.; Masi, S.; Casiglia, E.; Tikhonoff, V.; Cicero, A.F.G.; Ungar, A.; Rivasi, G.; Salvetti, M.; Barbagallo, C.M.; Bombelli, M.; et al. Identification of the uric acid thresholds predicting an increased total and cardiovascular mortality over 20 years. Hypertension 2020, 75, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Masi, S.; Georgiopoulos, G.; Alexopoulos, G.; Pateras, K.; Rosada, J.; Seravalle, G.; De Ciuceis, C.; Taddei, S.; Borghi, C.; Grassi, G.; et al. The complex relationship between serum uric acid, endothelial function and small vessel remodeling in humans. J. Clin. Med. 2020, 9, 2027. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhong, S.; Guo, X. The associations between fasting glucose, lipids and uric acid levels strengthen with the decile of uric acid increase and differ by sex. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 2786–2793. [Google Scholar] [CrossRef] [PubMed]
- Lurbe, E.; Torro, M.I.; Alvarez-Pitti, J.; Redon, J.; Borghi, C.; Redon, P. Uric acid is linked to cardiometabolic risk factors in overweight and obese youths. J. Hypertens. 2018, 36, 1840–1846. [Google Scholar] [CrossRef]
- Tenenbaum, A.; Klempfner, R.; Fisman, E.Z. Hypertriglyceridemia: A too long unfairly neglected major cardiovascular risk factor. Cardiovasc. Diabetol. 2014, 13, 159. [Google Scholar] [CrossRef]
- Alderman, M.H. Podagra, uric acid, and cardiovascular disease. Circulation 2007, 116, 880–883. [Google Scholar] [CrossRef]
- Selvaraj, S.; Claggett, B.L.; Pfeffer, M.A.; Desai, A.S.; Mc Causland, F.R.; McGrath, M.M.; Anand, I.S.; van Veldhuisen, D.J.; Kober, L.; Janssens, S.; et al. Serum uric acid, influence of sacubitril-valsartan, and cardiovascular outcomes in heart failure with preserved ejection fraction: Paragon-hf. Eur. J. Heart Fail. 2020, 22, 2093–2101. [Google Scholar] [CrossRef]
- Kleber, M.E.; Delgado, G.; Grammer, T.B.; Silbernagel, G.; Huang, J.; Krämer, B.K.; Ritz, E.; März, W. Uric acid and cardiovascular events: A mendelian randomization study. J. Am. Soc. Nephrol. 2015, 26, 2831–2838. [Google Scholar] [CrossRef]
- Zhao, G.; Huang, L.; Song, M.; Song, Y. Baseline serum uric acid level as a predictor of cardiovascular disease related mortality and all-cause mortality: A meta-analysis of prospective studies. Atherosclerosis 2013, 231, 61–68. [Google Scholar] [CrossRef]
- Gill, D.; Cameron, A.C.; Burgess, S.; Li, X.; Doherty, D.J.; Karhunen, V.; Abdul-Rahim, A.H.; Taylor-Rowan, M.; Zuber, V.; Tsao, P.S.; et al. Urate, blood pressure, and cardiovascular disease: Evidence from mendelian randomization and meta-analysis of clinical trials. Hypertension 2021, 77, 383–392. [Google Scholar] [CrossRef]
- Borghi, C.; Agnoletti, D.; Cicero, A.F.G.; Lurbe, E.; Virdis, A. Uric acid and hypertension: A review of evidence and future perspectives for the management of cardiovascular risk. Hypertension 2022, 79, 1927–1936. [Google Scholar] [CrossRef] [PubMed]
- Borghi, C.; Agabiti-Rosei, E.; Johnson, R.J.; Kielstein, J.T.; Lurbe, E.; Mancia, G.; Redon, J.; Stack, A.G.; Tsioufis, K.P. Hyperuricaemia and gout in cardiovascular, metabolic and kidney disease. Eur. J. Intern. Med. 2020, 80, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Masulli, M.; D’Elia, L.; Angeli, F.; Barbagallo, C.M.; Bilancio, G.; Bombelli, M.; Bruno, B.; Casiglia, E.; Cianci, R.; Cicero, A.F.G.; et al. Serum uric acid levels threshold for mortality in diabetic individuals: The uric acid right for heart health (urrah) project. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1245–1252. [Google Scholar] [CrossRef]
- Pugliese, N.R.; Mengozzi, A.; Virdis, A.; Casiglia, E.; Tikhonoff, V.; Cicero, A.F.G.; Ungar, A.; Rivasi, G.; Salvetti, M.; Barbagallo, C.M.; et al. The importance of including uric acid in the definition of metabolic syndrome when assessing the mortality risk. Clin. Res. Cardiol. 2021, 110, 1073–1082. [Google Scholar] [CrossRef]
- Casiglia, E.; Tikhonoff, V.; Virdis, A.; Grassi, G.; Angeli, F.; Barbagallo, C.M.; Bombelli, M.; Cicero, A.F.G.; Cirillo, M.; Cirillo, P.; et al. Serum uric acid/serum creatinine ratio as a predictor of cardiovascular events. Detection of prognostic cardiovascular cut-off values. J. Hypertens. 2023, 41, 180–186. [Google Scholar] [CrossRef]
- Muiesan, M.L.; Salvetti, M.; Virdis, A.; Masi, S.; Casiglia, E.; Tikhonoff, V.; Barbagallo, C.M.; Bombelli, M.; Cicero, A.F.G.; Cirillo, M.; et al. Serum uric acid, predicts heart failure in a large italian cohort: Search for a cut-off value the uric acid right for heart health study. J. Hypertens. 2021, 39, 62–69. [Google Scholar] [CrossRef]
- Russo, E.; Viazzi, F.; Pontremoli, R.; Barbagallo, C.M.; Bombelli, M.; Casiglia, E.; Cicero, A.F.G.; Cirillo, M.; Cirillo, P.; Desideri, G.; et al. Serum uric acid and kidney disease measures independently predict cardiovascular and total mortality: The uric acid right for heart health (urrah) project. Front. Cardiovasc. Med. 2021, 8, 713652. [Google Scholar] [CrossRef] [PubMed]
- Ungar, A.; Rivasi, G.; Di Bari, M.; Virdis, A.; Casiglia, E.; Masi, S.; Mengozzi, A.; Barbagallo, C.M.; Bombelli, M.; Bruno, B.; et al. The association of uric acid with mortality modifies at old age: Data from the uric acid right for heart health (urrah) study. J. Hypertens. 2022, 40, 704–711. [Google Scholar] [CrossRef]
- Toth, P.P.; Fazio, S.; Wong, N.D.; Hull, M.; Nichols, G.A. Risk of cardiovascular events in patients with hypertriglyceridaemia: A review of real-world evidence. Diabetes Obes. Metab. 2020, 22, 279–289. [Google Scholar] [CrossRef]
- Tan, H.L.E.; Hure, A.; Peel, R.; Hancock, S.; Attia, J. Prevalence and clinical risk prediction of hypertriglyceridaemia in a community cohort. Int. Med. J. 2021. Online ahead of print. [Google Scholar] [CrossRef]
- Holmes, M.V.; Asselbergs, F.W.; Palmer, T.M.; Drenos, F.; Lanktree, M.B.; Nelson, C.P.; Dale, C.E.; Padmanabhan, S.; Finan, C.; Swerdlow, D.I.; et al. Mendelian randomization of blood lipids for coronary heart disease. Eur. Heart. J. 2015, 36, 539–550. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.M.; O’Neill, L.A.J. Metabolic regulation of nlrp3. Immunol. Rev. 2018, 281, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Schunk, S.J.; Kleber, M.E.; März, W.; Pang, S.; Zewinger, S.; Triem, S.; Ege, P.; Reichert, M.C.; Krawczyk, M.; Weber, S.N.; et al. Genetically determined nlrp3 inflammasome activation associates with systemic inflammation and cardiovascular mortality. Eur. Heart J. 2021, 42, 1742–1756. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Garagnani, P.; Parini, P.; Giuliani, C.; Santoro, A. Inflammaging: A new immune-metabolic viewpoint for age-related diseases. Nat. Rev. Endocrinol. 2018, 14, 576–590. [Google Scholar] [CrossRef]
- Mengozzi, A.; Pugliese, N.R.; Chiriaco, M.; Masi, S.; Virdis, A.; Taddei, S. Microvascular ageing links metabolic disease to age-related disorders: The role of oxidative stress and inflammation in promoting microvascular dysfunction. J. Cardiovasc. Pharmacol. 2021, 78, S78–S87. [Google Scholar] [CrossRef]
- Desideri, G.; Virdis, A.; Casiglia, E.; Borghi, C. Exploration into uric and cardiovascular disease: Uric acid right for heart health (urrah) project, a study protocol for a retrospective observational study. High Blood Press. Cardiovasc. Prev. Off. J. Ital. Soc. Hypertens. 2018, 25, 197–202. [Google Scholar] [CrossRef]
- Inker, L.A.; Eneanya, N.D.; Coresh, J.; Tighiouart, H.; Wang, D.; Sang, Y.; Crews, D.C.; Doria, A.; Estrella, M.M.; Froissart, M.; et al. New creatinine- and cystatin c-based equations to estimate gfr without race. N. Engl. J. Med. 2021, 385, 1737–1749. [Google Scholar] [CrossRef]
- ADA. Classification and diagnosis of diabetes: Standards of medical care in diabetes—2020. Diabetes Care 2020, 43, S14–S31. [Google Scholar] [CrossRef]
- Eckel, N.; Li, Y.; Kuxhaus, O.; Stefan, N.; Hu, F.B.; Schulze, M.B. Transition from metabolic healthy to unhealthy phenotypes and association with cardiovascular disease risk across bmi categories in 90 257 women (the nurses’ health study): 30 year follow-up from a prospective cohort study. Lancet Diabetes Endocrinol. 2018, 6, 714–724. [Google Scholar] [CrossRef]
- Casiglia, E.; Tikhonoff, V.; Virdis, A.; Masi, S.; Barbagallo, C.M.; Bombelli, M.; Bruno, B.; Cicero, A.F.G.; Cirillo, M.; Cirillo, P.; et al. Serum uric acid and fatal myocardial infarction: Detection of prognostic cut-off values: The urrah (uric acid right for heart health) study. J. Hypertens. 2020, 38, 412–419. [Google Scholar] [CrossRef]
- Maloberti, A.; Biolcati, M.; Ruzzenenti, G.; Giani, V.; Leidi, F.; Monticelli, M.; Algeri, M.; Scarpellini, S.; Nava, S.; Soriano, F.; et al. The role of uric acid in acute and chronic coronary syndromes. J. Clin. Med. 2021, 10, 4750. [Google Scholar] [CrossRef]
- Tikhonoff, V.; Casiglia, E.; Spinella, P.; Barbagallo, C.M.; Bombelli, M.; Cicero, A.F.G.; Cirillo, M.; Cirillo, P.; Desideri, G.; D’Elia, L.; et al. Identification of a plausible serum uric acid cut-off value as prognostic marker of stroke: The uric acid right for heart health (urrah) study. J. Hum. Hypertens. 2022, 36, 976–982. [Google Scholar] [CrossRef] [PubMed]
- Palatini, P.; Parati, G.; Virdis, A.; Reboldi, G.; Masi, S.; Mengozzi, A.; Casiglia, E.; Tikhonoff, V.; Cicero, A.F.G.; Ungar, A.; et al. High heart rate amplifies the risk of cardiovascular mortality associated with elevated uric acid. Eur. J. Prev. Cardiol. 2021. Online ahead of print. [Google Scholar] [CrossRef]
- Russo, E.; Viazzi, F.; Pontremoli, R.; Barbagallo, C.M.; Bombelli, M.; Casiglia, E.; Cicero, A.F.G.; Cirillo, M.; Cirillo, P.; Desideri, G.; et al. Association of uric acid with kidney function and albuminuria: The uric acid right for heart health (urrah) project. J. Nephrol. 2022, 35, 211–221. [Google Scholar] [CrossRef]
- Chang, C.C.; Wu, C.H.; Liu, L.K.; Chou, R.H.; Kuo, C.S.; Huang, P.H.; Chen, L.K.; Lin, S.J. Association between serum uric acid and cardiovascular risk in nonhypertensive and nondiabetic individuals: The taiwan i-lan longitudinal aging study. Sci. Rep. 2018, 8, 5234. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Huang, J.Y.; Liu, L.; Lo, K.; Sun, S.; Chen, C.L.; Zhang, B.; Feng, Y.Q.; Huang, Y.Q. Relationship between serum uric acid level and all-cause and cardiovascular mortality in population with obesity. Postgrad. Med. J. 2020, 96, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Ohishi, M.; Takeya, Y.; Onishi, M.; Ito, N.; Yamamoto, K.; Kamide, K.; Rakugi, H. Serum uric acid is an independent risk factor for cardiovascular disease and mortality in hypertensive patients. Hypertens. Res. 2012, 35, 1087–1092. [Google Scholar] [CrossRef]
- Wen, C.P.; David Cheng, T.Y.; Chan, H.T.; Tsai, M.K.; Chung, W.S.; Tsai, S.P.; Wahlqvist, M.L.; Yang, Y.C.; Wu, S.B.; Chiang, P.H.; et al. Is high serum uric acid a risk marker or a target for treatment? Examination of its independent effect in a large cohort with low cardiovascular risk. Am. J. Kidney Dis. 2010, 56, 273–288. [Google Scholar] [CrossRef] [PubMed]
- Maloberti, A.; Vanoli, J.; Finotto, A.; Bombelli, M.; Facchetti, R.; Redon, P.; Mancia, G.; Grassi, G. Uric acid relationships with lipid profile and adiposity indices: Impact of different hyperuricemic thresholds. J. Clin. Hypertens. 2023, 25, 78–85. [Google Scholar] [CrossRef]
- Liu, X.Y.; Wu, Q.Y.; Chen, Z.H.; Yan, G.Y.; Lu, Y.; Dai, H.J.; Li, Y.; Yang, P.T.; Yuan, H. Elevated triglyceride to high-density lipoprotein cholesterol (tg/hdl-c) ratio increased risk of hyperuricemia: A 4-year cohort study in china. Endocrine 2020, 68, 71–80. [Google Scholar] [CrossRef]
- Palatini, P.; Virdis, A.; Masi, S.; Mengozzi, A.; Casiglia, E.; Tikhonoff, V.; Cicero, A.F.G.; Ungar, A.; Parati, G.; Rivasi, G.; et al. Hyperuricemia increases the risk of cardiovascular mortality associated with very high hdl-cholesterol level. Nutr. Metab. Cardiovasc. Dis. 2022. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.D.; Feng, S.; Chen, J.W.; Aihemaiti, M.; Shu, X.Y.; Quan, J.W.; Ding, F.H.; Lu, L.; Shen, W.F.; Zhang, R.Y.; et al. Serum uric acid is associated with the progression of left ventricular diastolic dysfunction in apparently healthy subjects. Dis. Markers 2022, 2022, 9927254. [Google Scholar] [CrossRef] [PubMed]
- Chiang, K.M.; Tsay, Y.C.; Vincent Ng, T.C.; Yang, H.C.; Huang, Y.T.; Chen, C.H.; Pan, W.H. Is hyperuricemia, an early-onset metabolic disorder, causally associated with cardiovascular disease events in han chinese? J. Clin. Med. 2019, 8, 1202. [Google Scholar] [CrossRef] [PubMed]
- Mengozzi, A.; Pugliese, N.R.; Taddei, S.; Masi, S.; Virdis, A. Microvascular inflammation and cardiovascular prevention: The role of microcirculation as earlier determinant of cardiovascular risk. High Blood Press. Cardiovasc. Prev. 2021, 29, 41–48. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Whole Dataset (n = 8124) | nTG (n = 6259) | hTG (n = 1865) | p-Value | |
|---|---|---|---|---|
| Age (years) | 58.8 ± 16.1 | 58.3 ± 16.5 | 60.4 ± 14.9 | <0.001 |
| Male sex (%) | 43.8 | 44.2 | 42.3 | 0.139 |
| BMI (kg/m2) | 26.2 ± 4.2 | 25.7 ± 4.1 | 27.8 ± 4.0 | <0.001 |
| Smokers (%) | 20.3 | 19.0 | 24.5 | <0.001 |
| Alcohol habit (%) | 66.6 | 65.8 | 69.4 | 0.004 |
| Systolic blood pressure (mmHg) | 148 ± 25 | 146 ± 26 | 153 ± 24 | <0.001 |
| Diastolic blood pressure (mmHg) | 88 ± 12 | 87 ± 12 | 91 ± 11 | <0.001 |
| Uric acid (mg/dL) | 5.0 ± 1.4 | 4.9 ± 1.3 | 5.7 ± 1.4 | <0.001 |
| Total cholesterol (mg/dL) | 213 ± 40 | 208 ± 39 | 231 ± 37 | <0.001 |
| HDL cholesterol (mg/dL) | 55.1 ± 15.4 | 57.7 ± 15.3 | 55.1 ± 15.4 | <0.001 |
| Triglycerides (mg/dL) | 104 (76–145) | 90 (69–144) | 190 (167–237) | <0.001 |
| Fasting plasma glucose (mg/dL) | 94 (86–105) | 93 (84–102) | 99 (90–110) | <0.001 |
| eGFR (mL/min/1.73 m2) | 85 ± 20 | 87 ± 20 | 80 ± 20 | <0.001 |
| Hematocrit (%) | 42.5 ± 3.8 | 42.3 ± 3.8 | 43.3 ± 3.8 | <0.001 |
| Obesity (%) | 16.5 | 13.8 | 25.5 | <0.001 |
| Arterial hypertension (%) | 73 | 69.7 | 84.0 | <0.001 |
| Type 2 diabetes (%) | 10.8 | 8.9 | 16.9 | <0.001 |
| Diuretics (%) | 15.6 | 14.3 | 20.2 | <0.001 |
| All-Cause Mortality | ||||
|---|---|---|---|---|
| Univariable | p-value | Multivariable | p-value | |
| SUA ≥ 4.7 | 1.79 [1.61–1.98] | <0.001 | 1.25 [1.12–1.40] | <0.001 |
| TG ≥ 150 | 1.25 [1.12–1.39] | <0.001 | 1.24 [1.09–1.39] | 0.001 |
| Cardiovascular Mortality | ||||
| Univariable | p-value | Multivariable | p-value | |
| SUA ≥ 5.6 | 2.03 [1.77–2.32] | <0.001 | 1.31 [1.11–1.74] | <0.001 |
| TG ≥ 150 | 1.28 [1.10–1.49] | <0.001 | 1.13 [0.95–1.39] | 0.163 |
| All-Cause Mortality (SUA ≥ 4.7) | ||||
|---|---|---|---|---|
| Univariable | p-value | Multivariable | p-value | |
| nTG | 1.31 [1.18–1.47] | <0.001 | 1.26 [1.12–1.43] | <0.001 |
| hTG | 1.60 [1.26–2.02] | <0.001 | 1.31 [1.02–1.68] | 0.033 |
| Cardiovascular Mortality (SUA ≥ 5.6) | ||||
| Univariable | p-value | Multivariable | p-value | |
| nTG | 2.13 [1.81–2.50] | <0.001 | 1.46 [1.23–1.73] | <0.001 |
| hTG | 1.66 [1.28–2.17] | <0.001 | 1.31 [0.99–1.64] | 0.060 |
| All-Cause Mortality | ||||
|---|---|---|---|---|
| Univariable | p-value | Multivariable | p-value | |
| SUA/serum creatinine > 5.35 | 1.33 [1.21–1.47] | <0.001 | 1.18 [1.07–1.31] | 0.001 |
| TG ≥ 150 | 1.25 [1.12–1.39] | <0.001 | 1.29 [1.14–1.45] | <0.001 |
| Cardiovascular Mortality | ||||
| Univariable | p-value | Multivariable | p-value | |
| SUA/serum creatinine > 5.35 | 1.37 [1.19–1.58] | <0.001 | 1.19 [1.03–1.37] | 0.016 |
| TG ≥ 150 | 1.28 [1.10–1.49] | 0.001 | 1.21 [1.02–1.44] | 0.028 |
| All-Cause Mortality | ||||
|---|---|---|---|---|
| Univariable | p-value | Multivariable | p-value | |
| nTG | 1.31 [1.18–1.47] | <0.001 | 1.47 [1.30–1.66] | <0.001 |
| hTG | 1.10 [0.90–1.33] | 0.348 | 1.09 [0.89–1.32] | 0.404 |
| Cardiovascular Mortality | ||||
| Univariable | p-value | Multivariable | p-value | |
| nTG | 1.44 [1.23–1.69] | <0.001 | 1.23 [1.04–1.45] | 0.015 |
| hTG | 1.08 [0.82–1.42] | 0.578 | 1.09 [0.82–1.44] | 0.548 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mengozzi, A.; Pugliese, N.R.; Desideri, G.; Masi, S.; Angeli, F.; Barbagallo, C.M.; Bombelli, M.; Cappelli, F.; Casiglia, E.; Cianci, R.; et al. Serum Uric Acid Predicts All-Cause and Cardiovascular Mortality Independently of Hypertriglyceridemia in Cardiometabolic Patients without Established CV Disease: A Sub-Analysis of the URic acid Right for heArt Health (URRAH) Study. Metabolites 2023, 13, 244. https://doi.org/10.3390/metabo13020244
Mengozzi A, Pugliese NR, Desideri G, Masi S, Angeli F, Barbagallo CM, Bombelli M, Cappelli F, Casiglia E, Cianci R, et al. Serum Uric Acid Predicts All-Cause and Cardiovascular Mortality Independently of Hypertriglyceridemia in Cardiometabolic Patients without Established CV Disease: A Sub-Analysis of the URic acid Right for heArt Health (URRAH) Study. Metabolites. 2023; 13(2):244. https://doi.org/10.3390/metabo13020244
Chicago/Turabian StyleMengozzi, Alessandro, Nicola Riccardo Pugliese, Giovambattista Desideri, Stefano Masi, Fabio Angeli, Carlo Maria Barbagallo, Michele Bombelli, Federica Cappelli, Edoardo Casiglia, Rosario Cianci, and et al. 2023. "Serum Uric Acid Predicts All-Cause and Cardiovascular Mortality Independently of Hypertriglyceridemia in Cardiometabolic Patients without Established CV Disease: A Sub-Analysis of the URic acid Right for heArt Health (URRAH) Study" Metabolites 13, no. 2: 244. https://doi.org/10.3390/metabo13020244