Invasive Pneumococcal Disease in Tuscany Region, Italy, 2016–2017: Integrating Multiple Data Sources to Investigate Underreporting

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
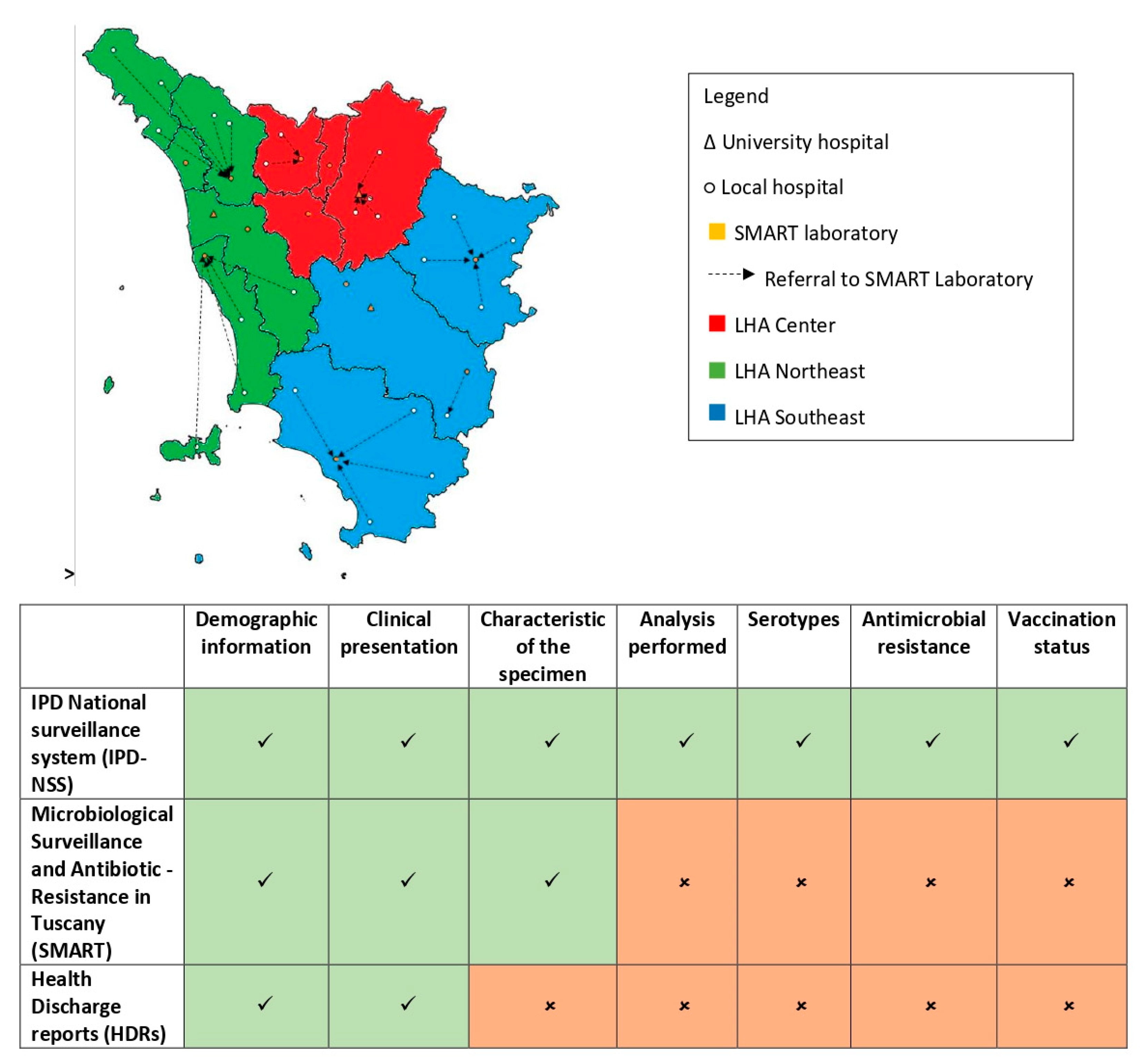
2.1. Description of Data Sources
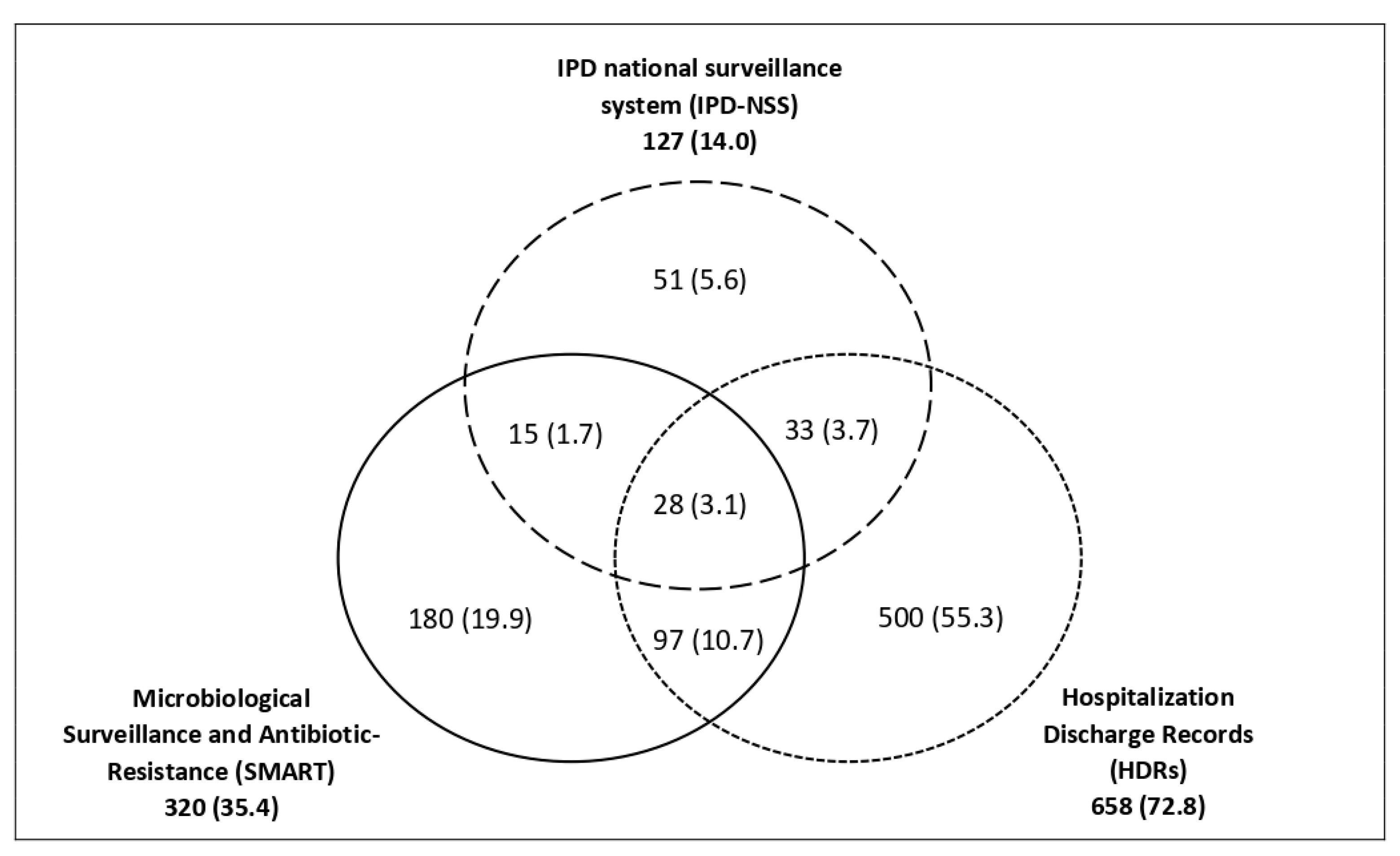
2.2. Identification of Common Cases among Sources
2.3. Description of Surveillance Systems, Calculation of Incidence, and Estimation of Underreporting
2.4. Capture–Recapture Analysis
3. Results
3.1. The Combined Surveillance System (CSS)
3.2. Capture–Recapture Estimates
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- 2012/506/EU: Commission Implementing Decision of 8 August 2012 Amending Decision 2002/253/EC Laying down Case Definitions for Reporting Communicable Diseases to the Community Network under Decision No 2119/98/EC of the European Parliament and of the Council (Notified under Document C(2012) 5538) Text with EEA Relevance, CELEX1; Publications Office of the European Union: Luxembourg, 2012.
- Blasi, F.; Mantero, M.; Santus, P.; Tarsia, P. Understanding the burden of pneumococcal disease in adults. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2012, 18, 7–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ECDC Invasive Pneumococcal Disease—Annual Epidemiological Report for 2017, Annual Epidemiological Report on Communicable Diseases in Europe; ECDC: Stockholm, Sweden, 2019.
- Pilishvili, T.; Bennett, N.M. Pneumococcal disease prevention among adults: Strategies for the use of pneumococcal vaccines. Vaccine 2015, 30, D60–D65. [Google Scholar] [CrossRef] [PubMed]
- Weiser, J.N.; Ferreira, D.M.; Paton, J.C. Streptococcus pneumoniae: Transmission, colonization and invasion. Nat. Rev. Microbiol. 2018, 16, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Desmet, S.; Verhaegen, J.; Van Ranst, M.; Peetermans, W.; Lagrou, K. Switch in a childhood pneumococcal vaccination programme from PCV13 to PCV10: A defendable approach? Lancet Infect. Dis. 2018, 18, 830–831. [Google Scholar] [CrossRef] [Green Version]
- Hulten, K.G. The changing epidemiology of pneumococcal diseases. Lancet Infect. Dis. 2018, 18, 929–930. [Google Scholar] [CrossRef]
- Izurieta, P.; Breuer, T. Interpretation of the switch in a childhood pneumococcal vaccination programme from PCV13 to PCV10 in Belgium. Lancet Infect. Dis. 2018, 18, 831–832. [Google Scholar] [CrossRef] [Green Version]
- Dagan, R.; Klugman, K.P. Impact of conjugate pneumococcal vaccines on antibiotic resistance. Lancet Infect. Dis. 2008, 8, 785–795. [Google Scholar] [CrossRef]
- WHO. Weekly Epidemiological Record; WHO: Geneva, Switzerland, 2019; Volume 94, pp. 85–104. [Google Scholar]
- Ceyhan, M.; Dagan, R.; Sayiner, A.; Chernyshova, L.; Dinleyici, E.Ç.; Hryniewicz, W.; Kulcsár, A.; Mad’arová, L.; Pazdiora, P.; Sidorenko, S.; et al. Surveillance of pneumococcal diseases in Central and Eastern Europe. Hum. Vaccines Immunother. 2016, 12, 2124–2134. [Google Scholar] [CrossRef] [Green Version]
- Torné, A.N.; Dias, J.G.; Quinten, C.; Hruba, F.; Busana, M.C.; Lopalco, P.L.; Gauci, A.J.A.; Pastore-Celentano, L. European enhanced surveillance of invasive pneumococcal disease in 2010: Data from 26 European countries in the post-heptavalent conjugate vaccine era. Vaccine 2014, 32, 3644–3650. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità. La Sorveglianza Nazionale Delle Malattie Invasive da Meningococco, Pneumococco ed Emofilo e Delle Meningiti Batteriche in Italia. Available online: http://old.iss.it/mabi/ (accessed on 1 August 2020).
- Camilli, R.; D’Ambrosio, F.; Del Grosso, M.; Pimentel de Araujo, F.; Caporali, M.G.; Del Manso, M.; Gherardi, G.; D’Ancona, F.; Pantosti, A. Pneumococcal Surveillance Group Impact of pneumococcal conjugate vaccine (PCV7 and PCV13) on pneumococcal invasive diseases in Italian children and insight into evolution of pneumococcal population structure. Vaccine 2017, 35, 4587–4593. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità. Sorveglianza Delle Malattie Batteriche Invasive in Italia. 2018. Available online: http://old.iss.it/binary/mabi/cont/Report2017.pdf (accessed on 1 August 2020).
- Boccalini, S.; Varone, O.; Chellini, M.; Pieri, L.; Sala, A.; Berardi, C.; Bonanni, P.; Bechini, A. Hospitalizations for pneumonia, invasive diseases and otitis in Tuscany (Italy), 2002–2014: Which was the impact of universal pneumococcal pediatric vaccination? Hum. Vaccines Immunother. 2016, 13, 428–434. [Google Scholar] [CrossRef] [Green Version]
- D’Ancona, F.; Caporali, M.G.; Del Manso, M.; Giambi, C.; Camilli, R.; D’Ambrosio, F.; Del Grosso, M.; Iannazzo, S.; Rizzuto, E.; Pantosti, A. Invasive pneumococcal disease in children and adults in seven Italian regions after the introduction of the conjugate vaccine, 2008–2014. Epidemiol. Prev. 2015, 39, 134–138. [Google Scholar]
- Baldovin, T.; Lazzari, R.; Cocchio, S.; Furlan, P.; Bertoncello, C.; Saia, M.; Russo, F.; Baldo, V. Invasive meningococcal disease in the Veneto region of Italy: A capture-recapture analysis for assessing the effectiveness of an integrated surveillance system. BMJ Open 2017, 7, e012478. [Google Scholar] [CrossRef]
- Clothier, H.J.; Vu, T.; Sundararajan, V.; Andrews, R.M.; Counahan, M.; Tallis, G.F.; Lambert, S.B. Invasive pneumococcal disease in Victoria: A better measurement of the true incidence. Epidemiol. Infect. 2008, 136, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Braeye, T.; Verheagen, J.; Mignon, A.; Flipse, W.; Pierard, D.; Huygen, K.; Schirvel, C.; Hens, N. Capture-Recapture Estimators in Epidemiology with Applications to Pertussis and Pneumococcal Invasive Disease Surveillance. PLoS ONE 2016, 11, e0159832. [Google Scholar] [CrossRef] [PubMed]
- Gjini, A.; Stuart, J.M.; George, R.C.; Nichols, T.; Heyderman, R.S. Capture-recapture analysis and pneumococcal meningitis estimates in England. Emerg. Infect. Dis. 2004, 10, 87–93. [Google Scholar] [CrossRef]
- Stock, N.K.; Maly, M.; Sebestova, H.; Orlikova, H.; Kozakova, J.; Krizova, P. The Czech Surveillance System for Invasive Pneumococcal Disease, 2008–2013: A Follow-Up Assessment and Sensitivity Estimation. PLoS ONE 2015, 10, e0131117. [Google Scholar] [CrossRef]
- De Greeff, S.C.; Spanjaard, L.; Dankert, J.; Hoebe, C.J.P.A.; Nagelkerke, N.; de Melker, H.E. Underreporting of meningococcal disease incidence in the Netherlands: Results from a capture-recapture analysis based on three registration sources with correction for false positive diagnoses. Eur. J. Epidemiol. 2006, 21, 315–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hook, E.B.; Regal, R.R. Capture-recapture methods in epidemiology: Methods and limitations. Epidemiol. Rev. 1995, 17, 243–264. [Google Scholar] [CrossRef]
- Gibbons, C.L.; Mangen, M.-J.J.; Plass, D.; Havelaar, A.H.; Brooke, R.J.; Kramarz, P.; Peterson, K.L.; Stuurman, A.L.; Cassini, A.; Fèvre, E.M.; et al. Measuring underreporting and under-ascertainment in infectious disease datasets: A comparison of methods. BMC Public Health 2014, 14, 147. [Google Scholar] [CrossRef] [Green Version]
- Pezzotti, P.; Bellino, S.; Riccardo, F.; Lucaroni, F.; Cerquetti, M.; Pantosti, A.; Rezza, G.; Stefanelli, P. Vaccine preventable invasive bacterial diseases in Italy: A comparison between the national surveillance system and recorded hospitalizations, 2007–2016. Vaccine 2019, 37, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Monali, R.; Vita, E.D.; Mariottini, F.; Privitera, G.; Lopalco, P.L.; Tavoschi, L. Impact of vaccination on invasive pneumococcal disease in Italy 2007–2017: Surveillance challenges and epidemiological changes. Epidemiol. Infect. 2020, 1–21. [Google Scholar] [CrossRef]
- Forni, S.; Toccafondi, G.; Viaggi, B.; Grazzini, M.; D’Arienzo, S.; Gemmi, F.; Vannucci, A.; Tulli, G. Gruppo SMART [The interplay of diagnostic and antimicrobial stewardship for the management of septic patients: The Tuscan model]. Recenti Prog. Med. 2018, 109, 133–136. [Google Scholar] [CrossRef]
- Heffner, A.C.; Horton, J.M.; Marchick, M.R.; Jones, A.E. Etiology of illness in patients with severe sepsis admitted to the hospital from the emergency department. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2010, 50, 814–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azzari, C.; Moriondo, M.; Indolfi, G.; Massai, C.; Becciolini, L.; de Martino, M.; Resti, M. Molecular detection methods and serotyping performed directly on clinical samples improve diagnostic sensitivity and reveal increased incidence of invasive disease by Streptococcus pneumoniae in Italian children. J. Med. Microbiol. 2008, 57, 1205–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmu, A.A.; Jokinen, J.; Nieminen, H.; Syrjänen, R.; Ruokokoski, E.; Puumalainen, T.; Moreira, M.; Schuerman, L.; Borys, D.; Kilpi, T.M. Vaccine effectiveness of the pneumococcal Haemophilus influenzae protein D conjugate vaccine (PHiD-CV10) against clinically suspected invasive pneumococcal disease: A cluster-randomised trial. Lancet Respir. Med. 2014, 2, 717–727. [Google Scholar] [CrossRef] [Green Version]
- Palmu, A.A.; Jokinen, J.; Nieminen, H.; Rinta-Kokko, H.; Ruokokoski, E.; Puumalainen, T.; Moreira, M.; Schuerman, L.; Borys, D.; Kilpi, T.M. Vaccine-preventable disease incidence of pneumococcal conjugate vaccine in the Finnish invasive pneumococcal disease vaccine trial. Vaccine 2018, 36, 1816–1822. [Google Scholar] [CrossRef] [PubMed]
- Van Hest, N.A.H.; Smit, F.; Baars, H.W.M.; De Vries, G.; De Haas, P.E.W.; Westenend, P.J.; Nagelkerke, N.J.D.; Richardus, J.H. Completeness of notification of tuberculosis in The Netherlands: How reliable is record-linkage and capture-recapture analysis? Epidemiol. Infect. 2007, 135, 1021–1029. [Google Scholar] [CrossRef]
- Schrauder, A.; Claus, H.; Elias, J.; Vogel, U.; Haas, W.; Hellenbrand, W. Capture-recapture analysis to estimate the incidence of invasive meningococcal disease in Germany, 2003. Epidemiol. Infect. 2007, 135, 657–664. [Google Scholar] [CrossRef]
- Héraud-Bousquet, V.; Lot, F.; Esvan, M.; Cazein, F.; Laurent, C.; Warszawski, J.; Gallay, A. A three-source capture-recapture estimate of the number of new HIV diagnoses in children in France from 2003–2006 with multiple imputation of a variable of heterogeneous catchability. BMC Infect. Dis. 2012, 12, 251. [Google Scholar] [CrossRef] [Green Version]
- Tilling, K. Capture-recapture methods—Useful or misleading? Int. J. Epidemiol. 2001, 30, 12–14. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| IPD-NSS | SMART | HDRs | CSS | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 2016 | 2017 | 2016 | 2017 | 2016 | 2017 | 2016 | 2017 | ||
| Total | 74 | 53 | 136 | 184 | 322 | 336 | 441 | 463 | |
| Sex | Male | 46 | 24 | 85 | 92 | 187 | 172 | 260 | 228 |
| Female | 28 | 29 | 51 | 92 | 135 | 164 | 181 | 235 | |
| Age (years) | <1 | 0 | 1 | 1 | 1 | 7 | 5 | 8 | 6 |
| 1–4 | 2 | 0 | 4 | 3 | 11 | 5 | 11 | 6 | |
| 5–14 | 0 | 0 | 1 | 5 | 3 | 6 | 3 | 8 | |
| 15–24 | 0 | 0 | 3 | 2 | 8 | 3 | 9 | 4 | |
| 25–44 | 8 | 8 | 15 | 19 | 26 | 30 | 41 | 42 | |
| 45–64 | 23 | 14 | 33 | 36 | 74 | 63 | 103 | 85 | |
| ≥65 | 41 | 30 | 79 | 118 | 193 | 224 | 266 | 312 | |
| Notification rate (n/100,000 inhabitants) | Northwest LHA (835,760 inhabitants) | 1.44 | 2.51 | 4.07 | 6.82 | 14.00 | 17.59 | 17.35 | 21.90 |
| Center LHA (1,627,964 inhabitants) | 3.01 | 1.41 | 5.16 | 6.20 | 7.99 | 7.99 | 12.90 | 11.92 | |
| Southeast LHA (1,278,713 inhabitants) | 1.02 | 0.70 | 1.41 | 2.03 | 5.87 | 4.61 | 6.73 | 6.41 | |
| All regions (3,742,437 inhabitants) | 2.0 | 1.4 | 3.6 | 4.9 | 8.6 | 9.0 | 11.8 | 12.3 | |
| Observed in CSS | Estimated (95% CI) | Underreporting Percentage (95% CI) | |
|---|---|---|---|
| Total | 900 * | 3419 (1364–5474) | 73.7 (34.0–83.6) |
| Year | |||
| 2016 | 441 | 1899 (681–3116) | 76.8 (35.2–85.8) |
| 2017 | 459 | 1520 (617–2424) | 69.8 (25.6–81.1) |
| Place of origin | |||
| University hospitals | 209 | 841 (279–1403) | 75.1 (25.1–85.1) |
| Center | 280 | 1117 (391–1842) | 74.9 (28.4–84.8) |
| Northwest | 269 | 863 (329–1398) | 68.8 (18.2–80.8) |
| Southeast | 142 | 598 (161–1036) | 76.3 (11.8–86.3) |
| Sex | |||
| Male | 487 | 1881 (738–3024) | 74.1 (34.0–83.9) |
| Female | 413 | 1538 (613–2464) | 73.1 (32.6–83.2) |
| Age | |||
| <25 years | 55 | 102 (39–166) | 46.1 (41.0–66.9) |
| 25–65 years | 271 | 888 (324–1435) | 69.5 (16.4–81.1) |
| >65 years | 574 | 2428 (901–3956) | 76.4 (36.3–85.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quattrone, F.; Donzelli, G.; D’Arienzo, S.; Fornili, M.; Innocenti, F.; Forni, S.; Baglietto, L.; Tavoschi, L.; Lopalco, P.L. Invasive Pneumococcal Disease in Tuscany Region, Italy, 2016–2017: Integrating Multiple Data Sources to Investigate Underreporting. Int. J. Environ. Res. Public Health 2020, 17, 7581. https://doi.org/10.3390/ijerph17207581
Quattrone F, Donzelli G, D’Arienzo S, Fornili M, Innocenti F, Forni S, Baglietto L, Tavoschi L, Lopalco PL. Invasive Pneumococcal Disease in Tuscany Region, Italy, 2016–2017: Integrating Multiple Data Sources to Investigate Underreporting. International Journal of Environmental Research and Public Health. 2020; 17(20):7581. https://doi.org/10.3390/ijerph17207581
Chicago/Turabian StyleQuattrone, Filippo, Gabriele Donzelli, Sara D’Arienzo, Marco Fornili, Francesco Innocenti, Silvia Forni, Laura Baglietto, Lara Tavoschi, and Pier Luigi Lopalco. 2020. "Invasive Pneumococcal Disease in Tuscany Region, Italy, 2016–2017: Integrating Multiple Data Sources to Investigate Underreporting" International Journal of Environmental Research and Public Health 17, no. 20: 7581. https://doi.org/10.3390/ijerph17207581