
Characterization of Autoimmune Thyroid Disease in a Cohort of 73 Paediatric Patients Affected by 22q11.2 Deletion Syndrome: Longitudinal Single-Centre Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Disease Definition
- (a)
- Positive serum thyroid autoantibodies against TPOAb, TGAb, and/or TRAb;
- (b)
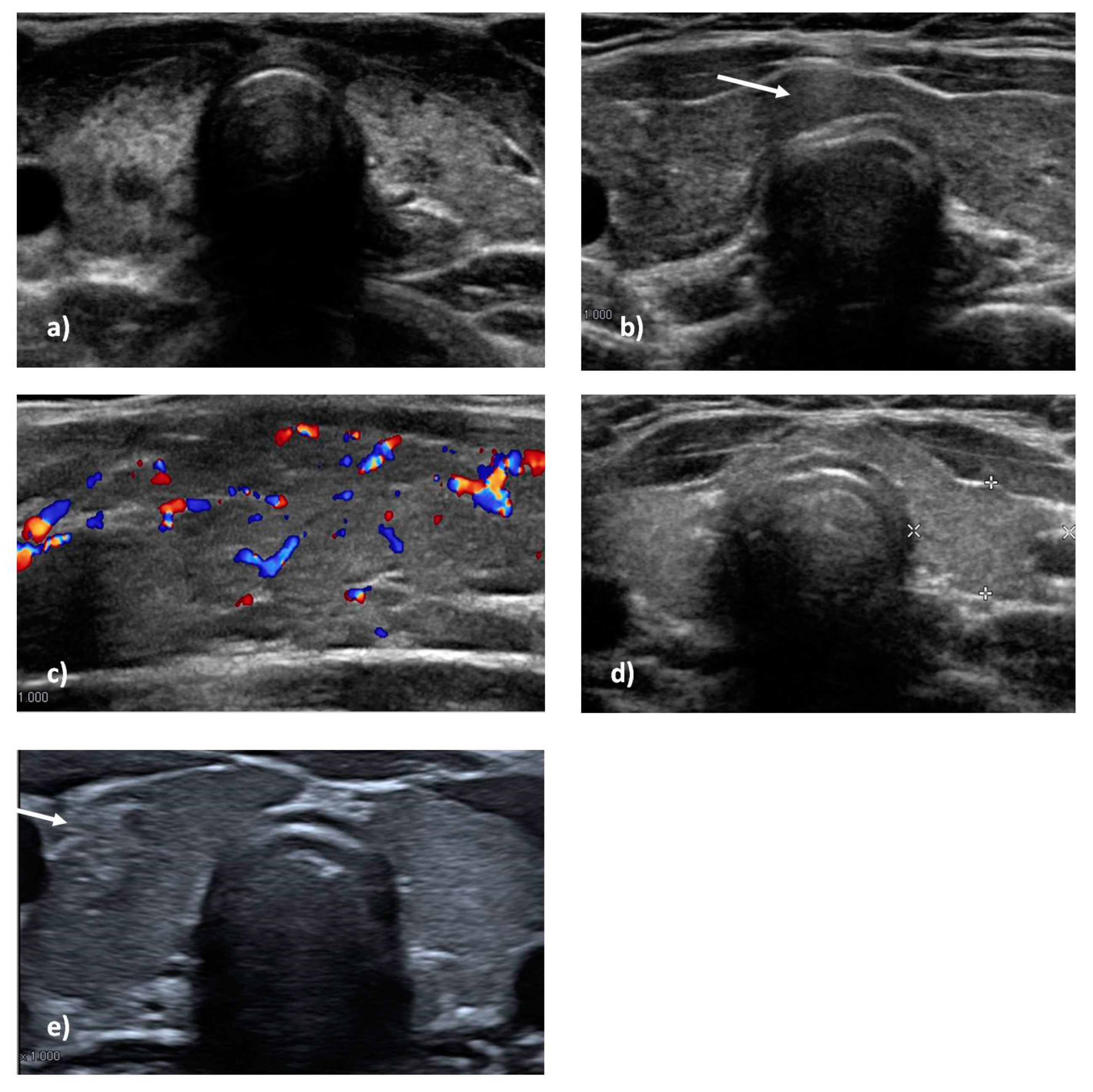
- Characteristic ultrasound scan with inhomogeneous echotexture, diffuse or irregular hypo-echogenicity (typical for thyroiditis);
- (c)
- Hormonal alteration on blood essays or clinical manifestations suggestive of hormonal alteration.
2.2. Statistical Analyses
3. Results
3.1. Thyroid Ultrasound Scan
3.2. Thyroid Function and Autoantibodies
3.3. Risk Factors Analysis for ATD in the 22q11.2 Pediatric Population
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kyritsi, E.M.; Kanaka-Gantenbein, C. Autoimmune Thyroid Disease in Specific Genetic Syndromes in Childhood and Adolescence. Front. Endocrinol. 2020, 11, 543. [Google Scholar] [CrossRef] [PubMed]
- Goodship, J.; Cross, I.; Liling, J.; Wren, C. A population study of chromosome 22q11 deletions in infancy. Arch. Dis. Child. 1998, 79, 348–351. [Google Scholar] [CrossRef] [PubMed]
- Roby, B.B.; Broderick, M.; Bohm, L.A. 22q11.2 Deletion Syndrome. In Cummings Pediatric Otolaryngology, 2nd ed.; Lesperance, M., Ed.; Elsevier: Amsterdam, The Netherlands, 2021; pp. 154–163. [Google Scholar] [CrossRef]
- McLean-Tooke, A.; Spickett, G.P.; Gennery, A.R. Immunodeficiency and autoimmunity in 22q11.2 deletion syndrome. Scand. J. Immunol. 2007, 66, 1–7. [Google Scholar] [CrossRef]
- Jerome, L.A.; Papaioannou, V.E. DiGeorge syndrome phenotype in mice mutant for the T-box gene, Tbx1. Nat. Genet. 2001, 27, 286–291. [Google Scholar] [CrossRef]
- de Almeida, J.R.; James, A.L.; Papsin, B.C.; Weksburg, R.; Clark, H.; Blaser, S. Thyroid gland and carotid artery anomalies in 22q11.2 deletion syndromes. Laryngoscope 2009, 119, 1495–1500. [Google Scholar] [CrossRef]
- Stagi, S.; Lapi, E.; Gambineri, E.; Salti, R.; Genuardi, M.; Colarusso, G.; Conti, C.; Jenuso, R.; Chiarelli, F.; Azzari, C.; et al. Thyroid function and morphology in subjects with microdeletion of chromosome 22q11 (del(22)(q11)). Clin. Endocrinol. 2010, 72, 839–844. [Google Scholar] [CrossRef]
- Jawad, A.F.; McDonald-McGinn, D.M.; Zackai, E.; Sullivan, K.E. Immunologic features of chromosome 22q11.2 deletion syndrome (DiGeorge syndrome/velocardiofacial syndrome). J. Pediatr. 2001, 139, 715–723. [Google Scholar] [CrossRef]
- Simmonds, M.J.; Gough, S.C.L. Genetic insights into disease mechanisms of autoimmunity. Br. Med. Bull. 2005, 71, 93–113. [Google Scholar] [CrossRef]
- Dejaco, C.; Duftner, C.; Grubeck-Loebenstein, B.; Schirmer, M. Imbalance of regulatory T cells in human autoimmune diseases. Immunology 2006, 117, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Simmonds, M.J.; Gough, S.C.L. Unravelling the genetic complexity of autoimmune thyroid disease: HLA, CTLA-4 and beyond. Clin. Exp. Immunol. 2004, 136, 1–10. [Google Scholar] [CrossRef]
- Dayan, C.M.; Daniels, G.H. Chronic autoimmune thyroiditis. N. Engl. J. Med. 1996, 335, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Dittmar, M.; Libich, C.; Brenzel, T.; Kahaly, G.J. Increased familial clustering of autoimmune thyroid diseases. Horm. Metab. Res. 2011, 43, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Shugar, A.L.; Shapiro, J.M.; Cytrynbaum, C.; Hedges, S.; Weksberg, R.; Fishman, L. An increased prevalence of thyroid disease in children with 22q11.2 deletion syndrome. Am. J. Med. Genet. A 2015, 167, 1560–1564. [Google Scholar] [CrossRef]
- Caturegli, P.; de Remigis, A.; Rose, N.R. Hashimoto thyroiditis: Clinical and diagnostic criteria. Autoimmun. Rev. 2014, 13, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Menconi, F.; Marcocci, C.; Marinò, M. Diagnosis and classification of Graves’ disease. Autoimmun. Rev. 2014, 13, 398–402. [Google Scholar] [CrossRef]
- Ueda, D. Sonographic measurement of the volume of the thyroid gland in healthy children. Acta Paediatr. Jpn. 1989, 31, 352–354. [Google Scholar] [CrossRef]
- Ohta, T.; Nishioka, M.; Nakata, N.; Fukuda, K.; Shirakawa, T. Significance of Perithyroidal Lymph Nodes in Benign Thyroid Diseases. J. Med. Ultrason. 2018, 45, 81–87. [Google Scholar] [CrossRef]
- Hakim, F.T.; Gress, R.E. Reconstitution of the lymphocyte compartment after lymphocyte depletion: A key issue in clinical immunology. Eur. J. Immunol. 2005, 35, 3099–3102. [Google Scholar] [CrossRef]
- Brent, G.A. Environmental exposures and autoimmune thyroid disease. Thyroid 2010, 20, 755–761. [Google Scholar] [CrossRef] [Green Version]
- Brown, R.S. Autoimmune thyroiditis in childhood. J. Clin. Res. Pediatr. Endocrinol. 2013, 5 (Suppl. 1), 45–49. [Google Scholar] [CrossRef]
- Morshed, S.A.; Latif, R.; Davies, T.F. Delineating the autoimmune mechanisms in Graves’ disease. Immunol. Res. 2012, 54, 191–203. [Google Scholar] [CrossRef] [PubMed]
- Zaletel, K.; Gaberšček, S. Hashimoto’s Thyroiditis: From Genes to the Disease. Curr. Genom. 2011, 12, 576–588. [Google Scholar] [CrossRef] [PubMed]
- Cappa, M.; Bizzarri, C.; Crea, F. Autoimmune thyroid diseases in children. J. Thyroid Res. 2010, 2011, 675703. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, D.A.; Spinner, N.B.; Budarf, M.L.; McDonald-McGinn, D.M.; Zackai, E.H.; Goldberg, R.B.; Shprintzen, R.J.; Saal, H.M.; Zonana, J.; Jones, M.C.; et al. Deletions and microdeletions of 22q11.2 in velo-cardio-facial syndrome. Am. J. Med. Genet. 1992, 44, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.I.; Burn, J.; Scambler, P.; Goodship, J. DiGeorge syndrome: Part of CATCH 22. J. Med. Genet. 1993, 30, 852–856. [Google Scholar] [CrossRef]
- Ryan, A.K.; Goodship, J.A.; Wilson, D.I.; Philip, N.; Levy, A.; Seidel, H.; Schuffenhauer, S.; Oechsler, H.; Belohradsky, B.; Prieur, M.; et al. Spectrum of clinical features associated with interstitial chromosome 22q11 deletions: A European collaborative study. J. Med. Genet. 1997, 34, 798–804. [Google Scholar] [CrossRef]
- Stagi, S.; Giani, T.; Simonini, G.; Falcini, F. Thyroid function, autoimmune thyroiditis and coeliac disease in juvenile idiopathic arthritis. Rheumatology 2005, 44, 517–520. [Google Scholar] [CrossRef]
- Gleeson, P.A.; Toh, B.H.; van Driel, I.R. Organ-specific autoimmunity induced by lymphopenia. Immunol. Rev. 1996, 149, 97–125. [Google Scholar] [CrossRef]
- Khoruts, A.; Fraser, J.M. A causal link between lymphopenia and autoimmunity. Immunol. Lett. 2005, 98, 23–31. [Google Scholar] [CrossRef]
- Min, B.; McHugh, R.; Sempowski, G.D.; Mackall, C.; Foucras, G.; Paul, W.E. Neonates support lymphopenia-induced proliferation. Immunity 2003, 18, 131–140. [Google Scholar] [CrossRef]
- Mackall, C.L.; Hakim, F.T.; Gress, R.E. Restoration of T-cell homeostasis after T-cell depletion. Semin. Immunol. 1997, 9, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Ricci, S.; Masini, M.; Valleriani, C.; Casini, A.; Cortimiglia, M.; Grisotto, L.; Canessa, C.; Indolfi, G.; Lippi, F.; Azzari, C. Reduced frequency of peripheral CD4+CD45RA+CD31+ cells and autoimmunity phenomena in patients affected by Del22q11 syndrome. Clin. Immunol. 2018, 188, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Tison, B.E.; Nicholas, S.K.; Abramson, S.L.; Hanson, I.C.; Paul, M.E.; Seeborg, F.O.; Shearer, W.; Perez, M.D.; Noroski, L.M.; Chinen, J. Autoimmunity in a cohort of 130 pediatric patients with partial DiGeorge syndrome. J. Allergy Clin. Immunol. 2011, 128, 1115–1117.e1-3. [Google Scholar] [CrossRef] [PubMed]
- Montin, D.; Marolda, A.; Licciardi, F.; Robasto, F.; Di Cesare, S.; Ricotti, E.; Ferro, F.; Scaioli, G.; Giancotta, C.; Amodio, D.; et al. Immunophenotype Anomalies Predict the Development of Autoimmune Cytopenia in 22q11.2 Deletion Syndrome. J. Allergy Clin. Immunol. Pract. 2019, 7, 2369–2376. [Google Scholar] [CrossRef]
- Stożek, K.; Grubczak, K.; Marolda, V.; Eljaszewicz, A.; Moniuszko, M.; Bossowski, A. Lower proportion of CD19+IL-10+ and CD19+CD24+CD27+ but not CD1d+CD5+CD19+CD24+CD27+ IL-10+ B cells in children with autoimmune thyroid diseases. Autoimmunity 2020, 53, 46–55. [Google Scholar] [CrossRef]
- Frommer, L.; Kahaly, G.J. Type 1 Diabetes and Autoimmune Thyroid Disease—The Genetic Link. Front. Endocrinol. 2021, 12, 618213. [Google Scholar] [CrossRef]


{kind=link}
| Clinical Features | All 22q11.2DS Patients |
|---|---|
| Hypocalcemia (mild and severe) | 53/73 (72%) |
| Cardiac anomalies | 46/73 (63%) |
| Combined cardiac defect (e.g., Fallot) | 25/73 (34%) |
| Isolated cardiac defect (e.g., IVD) | 21/73 (29%) |
| Developmental delay | 11/73 (15%) |
| Neuropsychiatric disorders | 10/73 (13.7%) |
| Failure to thrive | 8/73 (11%) |
| Feeding difficulties due to palatal defect | 7/73 (9.5%) |
| 22q11.2DS and ATD | All | Female | Male | F:M Ratio | Mean Age at Diagnosis (Years and DS) |
|---|---|---|---|---|---|
| All ATD under 18 | 16/73 (21.9%) | 13 | 3 | 4.33 | 10.34 ± 2.87 |
| HT | 15/73 (20.5%) | 13 | 2 | 6 | 10.28 ± 2.96 |
| GD | 1/73 (1.4%) | 0 | 1 | - | 11.29 |
| Morphologic Feature on US | 22q11.2DS ATD+ | 22q11.2DS ATD- | p-Value | RR Value | 95% CI |
|---|---|---|---|---|---|
| Overflow | 9/16 | 1/42 | <0.0001 | 6.171 | 3.031 to 12.67 |
| Nodules/pseudonodules | 3/16 | 4/42 | 0.3813 | 1.681 | 0.5714 to 3.744 |
| Inhomogeneity | 13/16 | 14/42 | 0.014 | 4.975 | 1.752 to 15.18 |
| Hypoecogenity | 10/16 | 8/42 | 0.032 | 3.704 | 1.624 to 8.531 |
| Perithyroidal lymphoadenopathy | 4/16 | 2/42 | 0.043 | 2.889 | 1.163 to 5.568 |
| Structural anomalies | 7/16 | 7/42 | 0.0096 | 3.278 | 1.433 to 6.986 |
| Lymphocyte Subset | 22q11.2DS ATD+ (Mean and DS) | 22q11.2DS ATD− (Mean and DS) | T-Student (p < 0.05) |
|---|---|---|---|
| CD3+ | 982.88 ± 319.1 | 1044.52 ± 398.79 | p = 0.287244 |
| CD3+CD4+ | 537 ± 213.8 | 603.65 ± 237.03 | p = 0.159249 |
| CD3+CD8+ | 329.25 ± 63.46 | 341.46 ± 171.24 | p = 0.396863 |
| CD19+ | 312.13 ± 152.14 | 461.38 ± 305.28 | p = 0.03239 |
| CD4+CD45RA+ % | 46.56 ± 15.51 | 47.72 ± 18.59 | p = 0.412255 |
| CD4+CD45RO+ % | 52.19 ± 16.17 | 51.80 ± 12.36 | p = 0.471045 |
| CD4+CD45RA+CD31+ % | 81.43 ± 15.21 | 77.59 ± 12.36 | p = 0.174093 |
| CD27+IgM+IgD− % | 8.16 ± 4.94 | 7.62 ± 9.45 | p = 0.399932 |
| 22q11.2DS Cohort Prevalence | Shugar et al. [14]. Prevalence | Pediatric Italian General Population Prevalence [28] | z-Score for One Proportion (95% CI) | |
|---|---|---|---|---|
| All ATD | 21.9% | 9.5% | 1.2% | p < 0.00001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ricci, S.; Sarli, W.M.; Lodi, L.; Canessa, C.; Lippi, F.; Azzari, C.; Stagi, S. Characterization of Autoimmune Thyroid Disease in a Cohort of 73 Paediatric Patients Affected by 22q11.2 Deletion Syndrome: Longitudinal Single-Centre Study. Genes 2022, 13, 1552. https://doi.org/10.3390/genes13091552
Ricci S, Sarli WM, Lodi L, Canessa C, Lippi F, Azzari C, Stagi S. Characterization of Autoimmune Thyroid Disease in a Cohort of 73 Paediatric Patients Affected by 22q11.2 Deletion Syndrome: Longitudinal Single-Centre Study. Genes. 2022; 13(9):1552. https://doi.org/10.3390/genes13091552
Chicago/Turabian StyleRicci, Silvia, Walter Maria Sarli, Lorenzo Lodi, Clementina Canessa, Francesca Lippi, Chiara Azzari, and Stefano Stagi. 2022. "Characterization of Autoimmune Thyroid Disease in a Cohort of 73 Paediatric Patients Affected by 22q11.2 Deletion Syndrome: Longitudinal Single-Centre Study" Genes 13, no. 9: 1552. https://doi.org/10.3390/genes13091552