
Nuclear Expression of β-Catenin Is Associated with Improved Outcomes in Endometrial Cancer

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population and Study Design
2.2. Immunohistochemistry and Specificity of Immunostaining
2.3. β Catenin Scoring
2.4. DNA Analysis
2.5. Statistical Analysis
3. Results
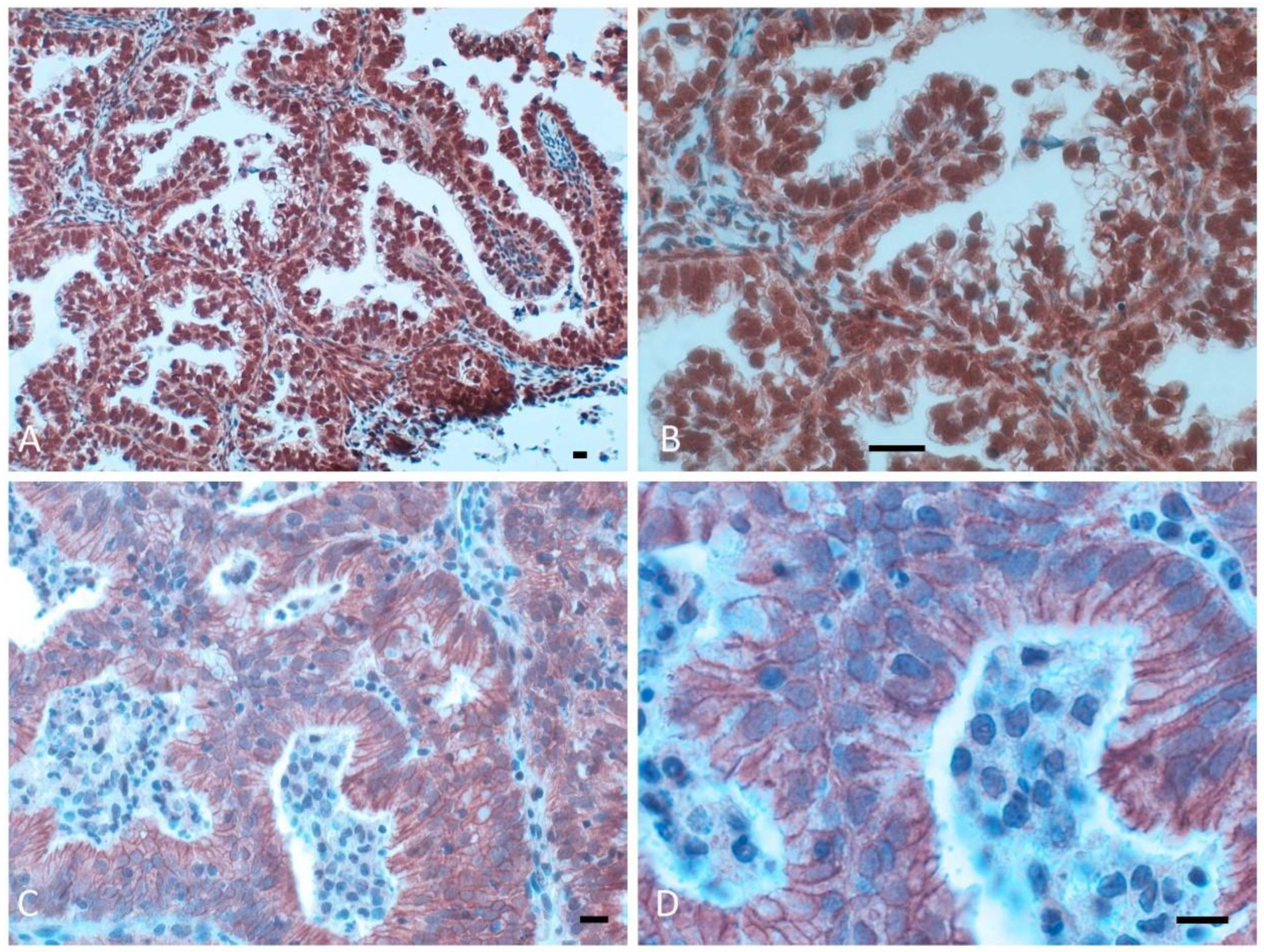
3.1. β-Catenin Protein Expression in Normal Human Endometrium, Simple and Complex Hyperplasia and Cystic Atrophy
3.2. β-Catenin Expression in Endometrial Adenocarcinomas and Correlations with Clinicopathological Features
3.3. β-Catenin Gene Mutations
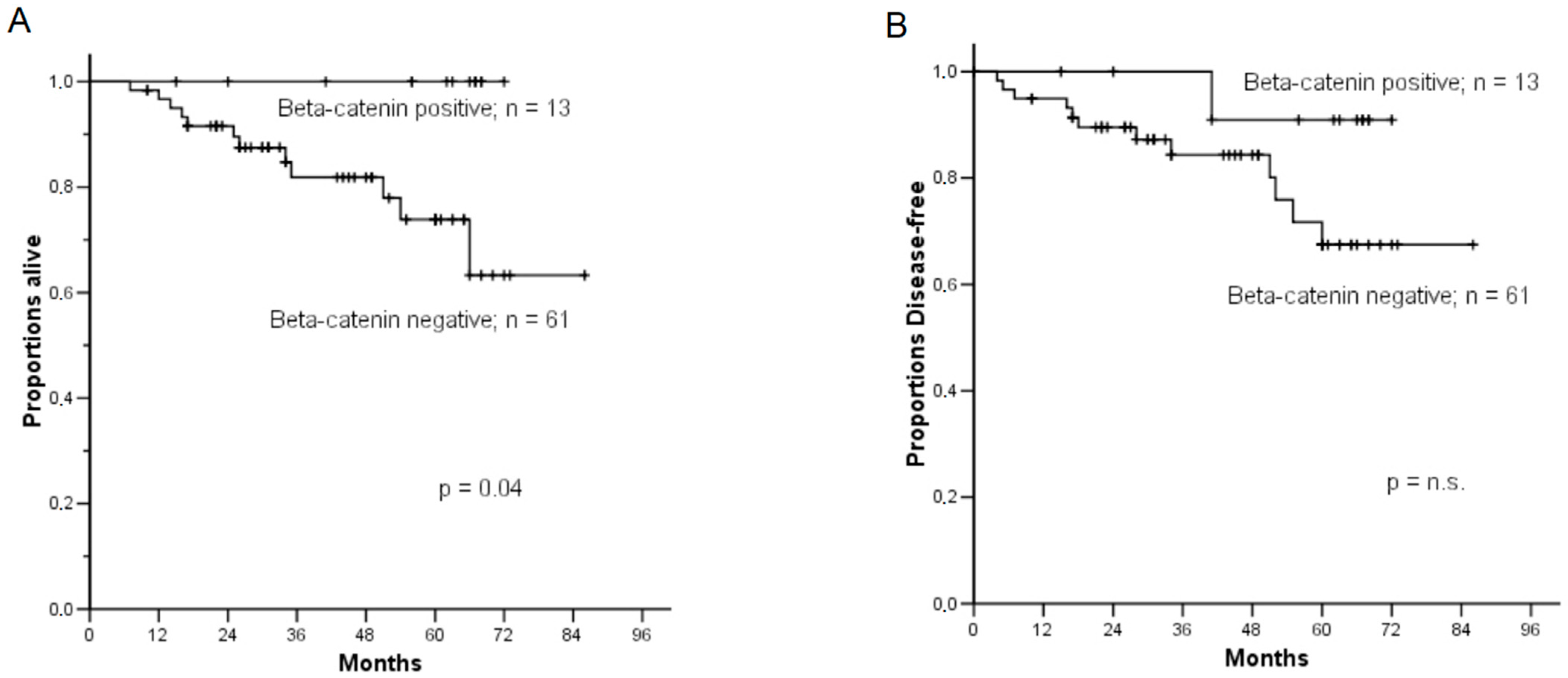
3.4. Correlation of β-Catenin Expression with Clinicopathological Parameters and Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Urick, M.E.; Bell, D.W. Clinical actionability of molecular targets in endometrial cancer. Nat. Rev. Cancer 2019, 19, 510–521. [Google Scholar] [CrossRef] [PubMed]
- van den Heerik ASV, M.; Horeweg, N.; de Boer, S.M.; Bosse, T.; Creutzberg, C.L. Adjuvant therapy for endometrial cancer in the era of molecular classification: Radiotherapy, chemoradiation and novel targets for therapy. Int. J. Gynecol. Cancer 2021, 31, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Kommoss, S.; McConechy, M.K.; Kommoss, F.; Leung, S.; Bunz, A.; Magrill, J.; Britton, H.; FKommoss, F.; Grevenkamp, F.; Karnezis, A.; et al. Talhouk A Final validation of the ProMisE molecular classifier for endometrial carcinoma in a large population-based case series. Ann. Oncol. 2018, 29, 1180–1188. [Google Scholar] [CrossRef]
- Castellone, M.D.; Teramoto, H.; Gutkind, J.S. Cyclooxygenase-2 and Colorectal Cancer chemoprevention: The β-Catenin Connection. Cancer Res. 2006, 66, 11085–11088. [Google Scholar] [CrossRef] [Green Version]
- Gammons, M.; Bienz, M. Multiprotein complexes governing Wnt signal transduction. Curr. Opin. Cell Biol. 2018, 51, 42–49. [Google Scholar] [CrossRef]
- Valenta, T.; Hausmann, G.; Basler, K. The many faces and functions of β-catenin. EMBO J. 2012, 31, 2714–2736. [Google Scholar] [CrossRef] [Green Version]
- Kikuchi A: Tumor formation by genetic mutations in the components of the Wnt signaling pathway. Cancer Sci. 2003, 94, 225–229. [CrossRef]
- Fukuchi, T.; Sakamoto, M.; Tsuda, H.; Maruyama, K.; Nozawa, S.; Hirohashi, S. Beta-catenin mutation in carcinoma of the uterine endometrium. Cancer Res. 1998, 58, 3526–3528. [Google Scholar]
- Machin, P.; Catasus, L.; Pons, C.; Muñoz, J.; Matias-Guiu, X.; Prat, J. CTNNB1 mutations and beta-catenin expression in endometrial carcinomas. Hum. Pathol. 2002, 33, 206–212. [Google Scholar] [CrossRef]
- Kurnit, K.C.; Kim, G.N.; Fellman, B.M.; Urbauer, D.L.; Mills, G.B.; Zhang, W.; Broaddus, R.R. CTNNB1 (beta-catenin) mutation identifies low grade, early stage endometrial cancer patients at increased risk of recurrence. Mod. Pathol. 2017, 30, 1032–1041. [Google Scholar] [CrossRef] [PubMed]
- Scholten, A.N.; Creutzberg, C.L.; van den Broek, L.J.; Noordijk, E.M.; Smit, V.T. Nuclear beta-catenin is a molecular feature of type I endometrial carcinoma. J. Pathol. 2003, 201, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Bueno, G.; Hardisson, D.; Sarrio, D.; Sanchez, C.; Cassia, R.; Prat, J.; Herman, J.G.; Esteller, M.; Matias-Guiu, X.; Palacios, J. Abnormalities of E- and P-cadherin and catenin (beta-, gamma-catenin, and p120ctn) expression in endometrial cancer and endometrial atypical hyperplasia. J. Pathol. 2003, 199, 471–478. [Google Scholar] [CrossRef]
- Stefansson, I.M.; Salvesen, H.B.; Akslen, L.A. Prognostic impact of alterations in P-Cadherin expression and related cell adhesion markers in endometrial cancer. J. Clin. Oncol. 2004, 22, 1242–1252. [Google Scholar] [CrossRef] [PubMed]
- Pijnenborg, J.M.; Kisters, N.; van Engeland, M.; Dunselman, G.A.; de Haan, J.; de Goeij, A.F.; Groothuis, P.G. APC, beta-catenin, and E-cadherin and the development of recurrent endometrial carcinoma. Int. J. Gynecol. Cancer 2004, 14, 947–956. [Google Scholar] [CrossRef] [PubMed]
- Irving, J.A.; Catasus, L.; Gallardo, A.; Bussaglia, E.; Romero, M.; Matias-Guiu, X.; Prat, J. Synchronous endometrioid carcinomas of the uterine corpus and ovary: Alterations in the beta-catenin (CTNNB1) pathway are associated with independent primary tumors and favorable prognosis. Hum. Pathol. 2005, 36, 605–619. [Google Scholar] [CrossRef]
- Athanassiadou, P.; Athanassiades, P.; Grapsa, D.; Gonidi, M.; Athanassiadou, A.M.; Stamati, P.N.; Patsouris, E. The prognostic value of PTEN, p53, and beta-catenin in endometrial carcinoma: A prospective immunocytochemical study. Int. J. Gynecol. Cancer 2007, 17, 697–704. [Google Scholar] [CrossRef]
- Schulten, H.-J.; Al-Maghrabi, J.; Al-Ghamdi, K.; Salama, S.; Al-Muhayawi, S.; Chaudhary, A.; Hamour, O.; Abuzenadah, A.; Gari, M.; Al-Qahtani, M. Mutational screening of RET, HRAS, KRAS, NRAS, BRAF, AKT1, and CTNNB1 in medullary thyroid carcinoma. Anticancer Res. 2011, 31, 4179–4183. [Google Scholar]
- Sal, V.; Demirkiran, F.; Erenel, H.; Tokgozoglu, N.; Kahramanoglu, I.; Bese, T.; Turan, H.; Sofiyeva, N.; Calay, Z.; Arvas, M.; et al. Expression of PTEN and β-Catenin and Their Relationship With Clinicopathological and Prognostic Factors in Endometrioid Type Endometrial Cancer. Int. J. Gynecol. Cancer 2016, 26, 512–520. [Google Scholar] [CrossRef]
- Vizza, E.; Cutillo, G.; Bruno, V.; Sperduti, I.; Mancini, E.; Baiocco, E.; Chiofalo, B.; Cicchillitti, L.; Certelli, C.; Zampa, A.; et al. Pattern of recurrence in patients with endometrial cancer: A retrospective study. Eur. J. Surg. Oncol. 2020, 46, 1697–1702. [Google Scholar] [CrossRef]
- Maretzky, T.; Reiss, K.; Ludwig, A.; Buchholz, J.; Scholz, F.; Proksch, E.; de Strooper, B.; Hartmann, D.; Saftig, P. ADAM10 mediates E-cadherin shedding and regulates epithelial cell-cell adhesion, migration, and β-catenin translocation. Proc. Natl. Acad. Sci. USA 2005, 102, 9182–9187. [Google Scholar] [CrossRef] [Green Version]
- Reiss, K.; Maretzky, T.; Ludwig, A.; Tousseyn, T.; de Strooper, B.; Hartmann, D.; Saftig, P. ADAM10 cleavage of N-cadherin and regulation of cell-cell adhesion and beta-catenin nuclear signalling. EMBO J. 2005, 24, 742–752. [Google Scholar] [CrossRef]
- Tabibzadeh, A.; Tameshkel, F.S.; Moradi, Y.; Soltani, S.; Moradi-Lakeh, M.; Ashrafi, G.H.; Motamed, N.; Zamani, F.; Motevalian, S.A.; Panahi, M.; et al. Signal transduction pathway mutations in gastrointestinal (GI) cancers: A systematic review and meta-analysis. Sci. Rep. 2020, 10, 1–24. [Google Scholar] [CrossRef]
- Gallagher, S.J.; Rambow, F.; Kumasaka, M.; Champeval, D.; Bellacosa, A.; Delmas, V.; Larue, L. Beta-catenin inhibits melanocyte migration but induces melanoma metastasis. Oncogene 2012, 32, 2230–2238. [Google Scholar] [CrossRef] [Green Version]
- McLean, T.D.; Duchi, S.; Di Bella, C. Molecular Pathogenesis of Sporadic Desmoid Tumours and Its Implications for Novel Therapies: A Systematised Narrative Review. Target. Oncol. 2022, 17, 223–252. [Google Scholar] [CrossRef] [PubMed]
- Glanz, S.M.; Kessler, D.H.P.; Eskin, T.A.; Liu, C.; Hassanein, A.M. b-Catenin Is Expressed Aberrantly in Tumors Expressing Shadow Cells Pilomatricoma, Craniopharyngioma, and Calcifying Odontogenic Cyst. Am. J. Clin. Pathol. 2003, 120, 732–736. [Google Scholar] [CrossRef]
- Saegusa, M.; Hashimura, M.; Kuwata, T.; Hamano, M.; Wani, Y.; Okayasu, I. A functional role of Cdx2 in β-catenin signaling during transdifferentiation in endometrial carcinomas. Carcinogenesis 2007, 28, 1885–1892. [Google Scholar] [CrossRef] [Green Version]
- Monaghan, H.; MacWhinnie, N.; Williams, A.R.W. The role of matrix metalloproteinases-2, -7 and -9 and β-catenin in high grade endometrial carcinoma. Histopathology 2007, 50, 348–357. [Google Scholar] [CrossRef]
- De, P.; Aske, J.C.; Dale, A.; Rojas Espaillat, L.; Starks, D.; Dey, N. Addressing activation of WNT beta-catenin pathway in diverse landscape of endometrial carcinogenesis. Am. J. Transl. Res. 2021, 13, 12168–12180. [Google Scholar] [PubMed]
- Travaglino, A.; Raffone, A.; Saccone, G.; De Luca, C.; Mollo, A.; Mascolo, M.; De Placido, G.; Insabato, L.; Zullo, F. Immunohistochemical Nuclear Expression of β-Catenin as a Surrogate of CTNNB1 Exon 3 Mutation in Endometrial Cancer. Am. J. Clin. Pathol. 2019, 151, 529–538. [Google Scholar] [CrossRef]
- Geyer, F.C.; Lacroix-Triki, M.; Savage, K.; Arnedos, M.; Lambros, M.B.; MacKay, A.; Natrajan, R.; Reis-Filho, J.S. b-catenin pathway activation in breast cancer is associated with triple-negative phenotype, but not with CTNNB1 mutation. Mod. Pathol. 2011, 24, 209–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, L.; Chen, S.; Jiang, H.; Huang, J.; Jin, W.; Yao, S. The expression of S100P increases and promotes cellular proliferation by increasing nuclear translocation of β-catenin in endometrial cancer. Int. J. Clin. Exp. Pathol. 2014, 7, 2102–2112. [Google Scholar] [PubMed]
- Liu, Y.; Patel, L.; Mills, G.B.; Lu, K.H.; Sood, A.K.; Ding, L.; Kucherlapati, R.; Mardis, E.R.; Levine, D.A.; Shmulevich, I.; et al. Clinical Significance of CTNNB1 Mutation and Wnt Pathway Activation in Endometrioid Endometrial Carcinoma. JNCI J. Natl. Cancer Inst. 2014, 106, dju245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sch, A.; Aliredjo, R.; Creutzberg, C.; Smit, V. Combined E-cadherin, alpha-catenin, and beta-catenin expression is a favorable prognostic factor in endometrial carcinoma. Int. J. Gynecol. Cancer 2006, 16, 1379–1385. [Google Scholar]
- Wang, L.; Rambau, P.F.; Kelemen, L.E.; Aglesio, M.S.; Leung, S.; Talhouk, A.; Kobel, M. Nuclear β-catenin and CDX2 expression in ovarian endometrioid carcinoma identify patients with favourable outcome. Histopathology 2019, 74, 452–462. [Google Scholar] [CrossRef]
- Garg, K.; Soslow, R.A. Strategies for Distinguishing Low-grade Endometrioid and Serous Carcinomas of Endometrium. Adv. Anat. Pathol. 2012, 19, 1–10. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total n. | Nuclear Pattern | Membranous Pattern | p | |
|---|---|---|---|---|
| Age | 74 | |||
| ≤65 year (44) | 6 (8%) | 38 (51%) | N.S. | |
| >65 year (30) | 7 (10%) | 23 (31%) | ||
| FIGO stage | 74 | |||
| I (49) | 10 (13%) | 39 (53%) | N.S. | |
| II (14) | 1 (1.4%) | 13 (17.5%) | ||
| III (8) | 1 (1.4%) | 7 (9.5%) | ||
| IV (3) | 1 (1.4%) | 2 (2.8%) | ||
| Histological type | 74 | 13 | 61 | |
| Adenocarcinoma endom (55) | 8 (10.8%) | 47 (63.5%) | N.S. | |
| Adenosquamous (13) | 4 (5.5%) | 9 (12.2%) | ||
| Clear cell (4) | 1 (1.4%) | 3 (4%) | ||
| Adenoacanthoma (2) | 0 | 2 (2.6%) | ||
| Grading | 74 | |||
| G1 (35) | 8 (10.9%) | 27 (36.4%) | 0.08 | |
| G2 (20) | 1 (1.4%) | 19 (25.8%) | ||
| G3 (19) | 4 (5.4%) | 15 (20.1%) | ||
| Myometrial invasion | 74 | |||
| <50% of depth (32) | 6 (8.1%) | 26 (35.1%) | N.S. | |
| >50% of depth (42) | 7 (9.5%) | 35 (47.3%) | ||
| Adjuvant treatment | 74 | |||
| None (42) | 6 (8.1%) | 36 (48.7%) | N.S. | |
| Radiotherapy (27) | 6 (8.1%) | 21 (28.3%) | ||
| Chemotherapy (5) | 1 (1.4%) | 4 (5.4%) |
| Total n. | Reduced β-Catenin | Preserved β-Catenin | p | |
|---|---|---|---|---|
| Age | 74 | |||
| ≤65 year (44) | 35 (47.3%) | 10 (13.5%) | N.S. | |
| >65 year (29) | 25 (34%) | 4 (5.2%) | ||
| FIGO stage | 74 | |||
| I (49) | 39 (53%) | 11 (15%) | N.S. | |
| II (14) | 11 (15%) | 3 (4%) | ||
| III (8) | 7 (9.5%) | 0 | ||
| IV (3) | 3 (4%) | 0 | ||
| Histological type | 74 | |||
| Adenocarcinoma endom (69) | 54 (74%) | 14 (19%) | N.S. | |
| Other hystotypes (5) | 5 (7%) | 0 | ||
| Grading | 74 | |||
| G1 (35) | 25 (34%) | 10 (13.5%) | 0.036 | |
| G2 (20) | 16 (21%) | 4 (6.5%) | ||
| G3 (19) | 18 (24%) | -- | ||
| Myometrial invasion | 74 | |||
| <50% of depth (32) | 24 (32%) | 8 (11%) | N.S. | |
| >50% of depth (42) | 36 (49%) | 6 (8%) | ||
| Adjuvant treatment | 74 | |||
| None (42) | 7 (10%) | 35 (47%) | N.S. | |
| Radiotherapy (27) | 5 (8%) | 22 (30%) | ||
| Chemotherapy (5) | 2 (3.5%) | 3 (1.5%) |
| Variable | RR of Death | 95% CI | p Value | RR of Recurrence | 95% CI | p Value |
|---|---|---|---|---|---|---|
| β catenin expression | ||||||
| nuclear | 1 | 1 | ||||
| membranous | 33.9 | 1.11–771.34 | 0.04 | 3.95 | 0.5–30.62 | n.s. |
| FIGO stage | ||||||
| I | 1 | 1 | ||||
| >I | 3.87 | 1.18–12.66 | 0.02 | 4.91 | 1.56–15.42 | 0.0006 |
| Age | ||||||
| ≤65 year | 1 | 1 | ||||
| >65 year | 1.81 | 0.58–5.67 | n.s | 1.56 | 0.52–4.69 | N.S. |
| Histotype | ||||||
| Not Aggressive | 1 | 1 | ||||
| Aggressive | 2.24 | 0.28–17.78 | n.s. | 5.65 | 1.15–27.73 | 0.003 |
| Grading | ||||||
| 1 | 1 | 1 | ||||
| 2–3 | 14.5 | 1.83–115.39 | 0.01 | 7.89 | 1.71–36.45 | 0.008 |
| Myometrial Invasion. | ||||||
| <50% of depth | 1 | 1 | ||||
| >50% of depth | 1.80 | 0.53–6.07 | n.s. | 2.25 | 0.68–7.41 | N.S. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masciullo, V.; Susini, T.; Corrado, G.; Stepanova, M.; Baroni, A.; Renda, I.; Castiglione, F.; Minimo, C.; Bellacosa, A.; Chiofalo, B.; et al. Nuclear Expression of β-Catenin Is Associated with Improved Outcomes in Endometrial Cancer. Diagnostics 2022, 12, 2401. https://doi.org/10.3390/diagnostics12102401
Masciullo V, Susini T, Corrado G, Stepanova M, Baroni A, Renda I, Castiglione F, Minimo C, Bellacosa A, Chiofalo B, et al. Nuclear Expression of β-Catenin Is Associated with Improved Outcomes in Endometrial Cancer. Diagnostics. 2022; 12(10):2401. https://doi.org/10.3390/diagnostics12102401
Chicago/Turabian StyleMasciullo, Valeria, Tommaso Susini, Giacomo Corrado, Marina Stepanova, Alessandro Baroni, Irene Renda, Francesca Castiglione, Corrado Minimo, Alfonso Bellacosa, Benito Chiofalo, and et al. 2022. "Nuclear Expression of β-Catenin Is Associated with Improved Outcomes in Endometrial Cancer" Diagnostics 12, no. 10: 2401. https://doi.org/10.3390/diagnostics12102401