
Laparoscopic Compared with Open D2 Gastrectomy on Perioperative and Long-Term, Stage-Stratified Oncological Outcomes for Gastric Cancer: A Propensity Score-Matched Analysis of the IMIGASTRIC Database


 , ,
, ,  , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Overall Objective and Type of Study
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection and Outcomes
2.4. Statistical Analysis
3. Results
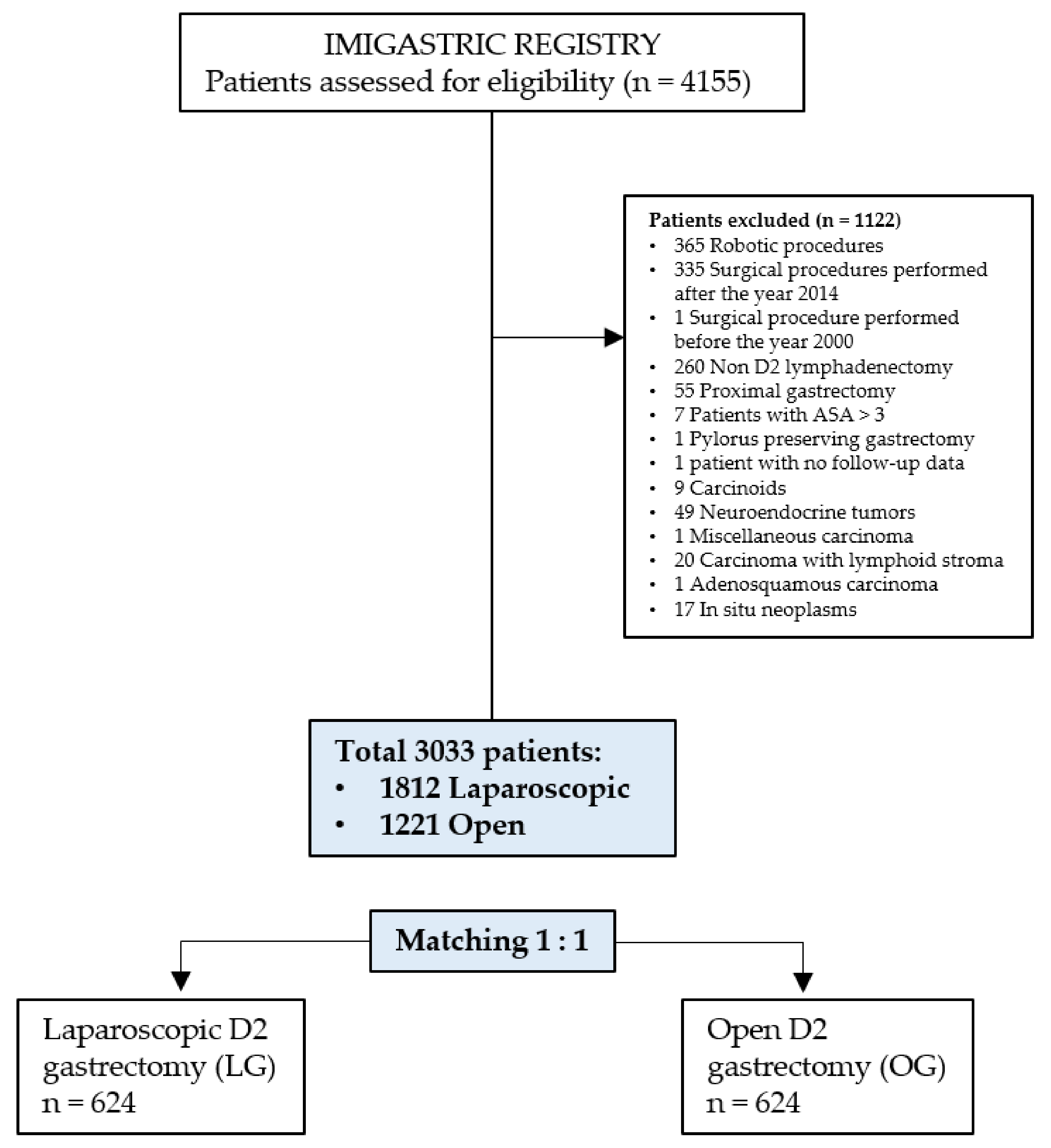
3.1. Patient Selection
3.2. Patient Characteristics
3.3. Operative Outcomes
3.4. Histology
3.5. Post-Operative Outcomes
3.6. Survival Analysis
4. Discussion
4.1. Study Findings (Short-Term Outcomes)
4.2. Operative Time
4.3. Hospital Stay and Complications
4.4. Lymphadenectomy
4.5. Long-Term Survival and Related Factors
4.6. Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer 2021, 24, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitano, S.; Iso, Y.; Moriyama, M.; Sugimachi, K. Laparoscopy-assisted Billroth I gastrectomy. Surg. Laparosc. Endosc. 1994, 4, 146–148. [Google Scholar] [PubMed]
- Zhu, Z.; Li, L.; Xu, J.; Ye, W.; Zeng, J.; Chen, B.; Huang, Z. Laparoscopic versus open approach in gastrectomy for advanced gastric cancer: A systematic review. World J. Surg. Oncol. 2020, 18, 126. [Google Scholar] [CrossRef] [PubMed]
- Inaki, N.; Etoh, T.; Ohyama, T.; Uchiyama, K.; Katada, N.; Koeda, K.; Yoshida, K.; Takagane, A.; Kojima, K.; Sakuramoto, S.; et al. A Multi-institutional, Prospective, Phase II Feasibility Study of Laparoscopy-Assisted Distal Gastrectomy with D2 Lymph Node Dissection for Locally Advanced Gastric Cancer (JLSSG0901). World J. Surg. 2015, 39, 2734–2741. [Google Scholar] [CrossRef]
- Wang, Z.; Xing, J.; Cai, J.; Zhang, Z.; Li, F.; Zhang, N.; Wu, J.; Cui, M.; Liu, Y.; Chen, L.; et al. Short-term surgical outcomes of laparoscopy-assisted versus open D2 distal gastrectomy for locally advanced gastric cancer in North China: A multicenter randomized controlled trial. Surg. Endosc. 2019, 33, 33–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.K.; Yoon, H.M.; Kim, Y.W.; Park, J.Y.; Ryu, K.W.; Lee, Y.J.; Jeong, O.; Yoon, K.Y.; Lee, J.H.; Lee, S.E.; et al. Laparoscopy-assisted versus Open D2 Distal Gastrectomy for Advanced Gastric Cancer: Results From a Randomized Phase II Multicenter Clinical Trial (COACT 1001). Ann. Surg. 2018, 267, 638–645. [Google Scholar] [CrossRef]
- Cai, J.; Wei, D.; Gao, C.F.; Zhang, C.S.; Zhang, H.; Zhao, T. A prospective randomized study comparing open versus laparoscopy-assisted D2 radical gastrectomy in advanced gastric cancer. Dig. Surg. 2011, 28, 331–337. [Google Scholar] [CrossRef]
- Hu, Y.; Huang, C.; Sun, Y.; Su, X.; Cao, H.; Hu, J.; Xue, Y.; Suo, J.; Tao, K.; He, X.; et al. Morbidity and Mortality of Laparoscopic Versus Open D2 Distal Gastrectomy for Advanced Gastric Cancer: A Randomized Controlled Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 1350–1357. [Google Scholar] [CrossRef]
- Shi, Y.; Xu, X.; Zhao, Y.; Qian, F.; Tang, B.; Hao, Y.; Luo, H.; Chen, J.; Yu, P. Long-term oncologic outcomes of a randomized controlled trial comparing laparoscopic versus open gastrectomy with D2 lymph node dissection for advanced gastric cancer. Surgery 2019, 165, 1211–1216. [Google Scholar] [CrossRef]
- Cui, M.; Li, Z.; Xing, J.; Yao, Z.; Liu, M.; Chen, L.; Zhang, C.; Yang, H.; Zhang, N.; Tan, F.; et al. A prospective randomized clinical trial comparing D2 dissection in laparoscopic and open gastrectomy for gastric cancer. Med. Oncol. 2015, 32, 241. [Google Scholar] [CrossRef]
- Lee, H.J.; Hyung, W.J.; Yang, H.K.; Han, S.U.; Park, Y.K.; An, J.Y.; Kim, W.; Kim, H.I.; Kim, H.H.; Ryu, S.W.; et al. Short-term Outcomes of a Multicenter Randomized Controlled Trial Comparing Laparoscopic Distal Gastrectomy With D2 Lymphadenectomy to Open Distal Gastrectomy for Locally Advanced Gastric Cancer (KLASS-02-RCT). Ann. Surg. 2019, 270, 983–991. [Google Scholar] [CrossRef]
- Li, Q.; Wang, J.; Zhang, G.; Wang, J.; Yang, B.; Zhang, Z. Feasibility and safety comparison of laparoscopy-assisted versus open gastrectomy for advanced gastric carcinoma with D2 lymphadenectomy. Jpn. J. Clin. Oncol. 2016, 46, 323–328. [Google Scholar] [CrossRef] [Green Version]
- Hao, Y.; Yu, P.; Qian, F.; Zhao, Y.; Shi, Y.; Tang, B.; Zeng, D.; Zhang, C. Comparison of laparoscopy-assisted and open radical gastrectomy for advanced gastric cancer: A retrospective study in a single minimally invasive surgery center. Medicine 2016, 95, e3936. [Google Scholar] [CrossRef]
- Li, Z.; Li, B.; Bai, B.; Yu, P.; Lian, B.; Zhao, Q. Long-term outcomes of laparoscopic versus open D2 gastrectomy for advanced gastric cancer. Surg. Oncol. 2018, 27, 441–448. [Google Scholar] [CrossRef]
- Xu, Y.; Hua, J.; Li, J.; Shi, L.; Xue, H.; Shuang, J.; Du, J. Long-term outcomes of laparoscopic versus open gastrectomy for advanced gastric cancer: A large cohort study. Am. J. Surg. 2019, 217, 750–756. [Google Scholar] [CrossRef]
- Zhao, Y.; Yu, P.; Hao, Y.; Qian, F.; Tang, B.; Shi, Y.; Luo, H.; Zhang, Y. Comparison of outcomes for laparoscopically assisted and open radical distal gastrectomy with lymphadenectomy for advanced gastric cancer. Surg. Endosc. 2011, 25, 2960–2966. [Google Scholar] [CrossRef] [PubMed]
- Desiderio, J.; Jiang, Z.W.; Nguyen, N.T.; Zhang, S.; Reim, D.; Alimoglu, O.; Azagra, J.S.; Yu, P.W.; Coburn, N.G.; Qi, F.; et al. Robotic, laparoscopic and open surgery for gastric cancer compared on surgical, clinical and oncological outcomes: A multi-institutional chart review. A study protocol of the International study group on Minimally Invasive surgery for GASTRIc Cancer-IMIGASTRIC. BMJ Open 2015, 5, e008198. [Google Scholar] [CrossRef]
- Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancerc. 2011, 14, 101–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AJCC; Brierley, J.; Gospodarowicz, M.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; Brierley, J., Gospodarowicz, M., Wittekind, C., Eds.; Wiley-Blackwell: Hoboken, NJ, USA, 2016. [Google Scholar]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Ptok, H.; Gastinger, I.; Meyer, F.; Ilsemann, A.; Lippert, H.; Bruns, C. Hospital volume effects in surgical treatment of gastric cancer: Results of a prospective multicenter observational study. Der Chir. Z. Fur Alle Geb. Der Oper. Medizen 2017, 88, 328–338. [Google Scholar] [CrossRef]
- Best, L.M.; Mughal, M.; Gurusamy, K.S. Laparoscopic versus open gastrectomy for gastric cancer. Cochrane Database Syst. Rev. 2016, 3, CD011389. [Google Scholar] [CrossRef] [Green Version]
- Chan, B.Y.O.; Yau, K.K.W.; Chan, C.K.O. Totally laparoscopic versus open gastrectomy for advanced gastric cancer: A matched retrospective cohort study. Hong Kong Med. J. Xianggang Yi Xue Za Zhi 2019, 25, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.X.; Huang, C.M.; Zheng, C.H.; Li, P.; Xie, J.W.; Wang, J.B.; Lu, J. Laparoscopy-assisted gastrectomy with D2 lymph node dissection for advanced gastric cancer without serosa invasion: A matched cohort study from South China. World J. Surg. Oncol. 2013, 11, 4. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.Y.; Huang, C.M.; Lin, J.X.; Zheng, C.H.; Li, P.; Xie, J.W.; Wang, J.B.; Lu, J. Laparoscopy-assisted versus open D2 radical gastrectomy for advanced gastric cancer without serosal invasion: A case control study. World J. Surg. Oncol. 2012, 10, 248. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Lan, Y.; Tang, B.; Hao, Y.; Shi, Y.; Yu, P. Comparative study of laparoscopy-assisted and open radical gastrectomy for stage T4a gastric cancer. Int. J. Surg. 2017, 41, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Kunisaki, C.; Makino, H.; Yamamoto, N.; Sato, T.; Oshima, T.; Nagano, Y.; Fujii, S.; Akiyama, H.; Otsuka, Y.; Ono, H.A.; et al. Learning curve for laparoscopy-assisted distal gastrectomy with regional lymph node dissection for early gastric cancer. Surg. Laparosc. Endosc. Percutaneous Tech. 2008, 18, 236–241. [Google Scholar] [CrossRef]
- Wei, Y.; Yu, D.; Li, Y.; Fan, C.; Li, G. Laparoscopic versus open gastrectomy for advanced gastric cancer: A meta-analysis based on high-quality retrospective studies and clinical randomized trials. Clin. Res. Hepatol. Gastroenterol. 2018, 42, 577–590. [Google Scholar] [CrossRef] [PubMed]
- Park, D.J.; Han, S.U.; Hyung, W.J.; Kim, M.C.; Kim, W.; Ryu, S.Y.; Ryu, S.W.; Song, K.Y.; Lee, H.J.; Cho, G.S.; et al. Long-term outcomes after laparoscopy-assisted gastrectomy for advanced gastric cancer: A large-scale multicenter retrospective study. Surg. Endosc. 2012, 26, 1548–1553. [Google Scholar] [CrossRef]
- Inokuchi, M.; Nakagawa, M.; Tanioka, T.; Okuno, K.; Gokita, K.; Kojima, K. Long- and short-term outcomes of laparoscopic gastrectomy versus open gastrectomy in patients with clinically and pathological locally advanced gastric cancer: A propensity-score matching analysis. Surg. Endosc. 2018, 32, 735–742. [Google Scholar] [CrossRef]
- Hamabe, A.; Omori, T.; Tanaka, K.; Nishida, T. Comparison of long-term results between laparoscopy-assisted gastrectomy and open gastrectomy with D2 lymph node dissection for advanced gastric cancer. Surg. Endosc. 2012, 26, 1702–1709. [Google Scholar] [CrossRef]
- Zemni, I.; Mansouri, H.; Ben Safta, I.; Ayadi, M.A.; Ben Dhiab, T.; Chargui, R.; Rahal, K. Resectable gastric signet ring cell carcinoma: Clinicopathological characteristics and survival outcomes. J. Gastric Surg. 2020, 2, 71–78. [Google Scholar] [CrossRef]
- Mansouri, H.; Zemni, I.; Ayadi, M.A.; Ben Safta, I.; Ben Dhiab, T.; Mahjoub, N.; Achouri, L.; Rahal, K. Determinants of surgical morbidity in gastric cancer: Experience of a single center and literature review. J. Gastric Surg. 2020, 2, 106–117. [Google Scholar] [CrossRef]
- Owen, R.M.; Perez, S.D.; Lytle, N.; Patel, A.; Davis, S.S.; Lin, E.; Sweeney, J.F. Impact of operative duration on postoperative pulmonary complications in laparoscopic versus open colectomy. Surg. Endosc. 2013, 27, 3555–3563. [Google Scholar] [CrossRef]
- Naffouje, S.A.; Salti, G.I. Extensive Lymph Node Dissection Improves Survival among American Patients with Gastric Adenocarcinoma Treated Surgically: Analysis of the National Cancer Database. J. Gastric Cancer 2017, 17, 319–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, Y.; Goldner, B.; Ituarte, P.; Lee, B.; Melstrom, L.; Son, T.; Noh, S.H.; Fong, Y.; Hyung, W.J. Lymphadenectomy with Optimum of 29 Lymph Nodes Retrieved Associated with Improved Survival in Advanced Gastric Cancer: A 25,000-Patient International Database Study. J. Am. Coll. Surg. 2017, 224, 546–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiki, N.; Honda, M.; Etoh, T.; Yoshida, K.; Kodera, Y.; Kakeji, Y.; Kumamaru, H.; Miyata, H.; Yamashita, Y.; Inomata, M.; et al. Higher incidence of pancreatic fistula in laparoscopic gastrectomy. Real-world evidence from a nationwide prospective cohort study. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2018, 21, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Q.; Huang, C.-M.; Chen, Q.-Y.; Lin, J.-X.; Xie, J.-W.; Li, P.; Zheng, C.-H. Current Status of Indocyanine Green Tracer-Guided Lymph Node Dissection in Minimally Invasive Surgery for Gastric Cancer. J. Gastric Surg. 2021, 3. [Google Scholar] [CrossRef]
- Coco, D.; Leanza, S. Assessment of the Completeness of Lymph Node Dissection Using Indocyanine Green in Laparoscopic and Robotic Gastrectomy for Gastric Cancer—A Review. J. Gastric Surg. 2021, 3. [Google Scholar] [CrossRef]
- Kinoshita, T.; Uyama, I.; Terashima, M.; Noshiro, H.; Nagai, E.; Obama, K.; Tamamori, Y.; Nabae, T.; Honda, M.; Abe, T.; et al. Long-term Outcomes of Laparoscopic Versus Open Surgery for Clinical Stage II/III Gastric Cancer: A Multicenter Cohort Study in Japan (LOC-A Study). Ann. Surg. 2019, 269, 887–894. [Google Scholar] [CrossRef]
- Gordon, A.C.; Kojima, K.; Inokuchi, M.; Kato, K.; Sugihara, K. Long-term comparison of laparoscopy-assisted distal gastrectomy and open distal gastrectomy in advanced gastric cancer. Surg. Endosc. 2013, 27, 462–470. [Google Scholar] [CrossRef]
- Shinohara, T.; Satoh, S.; Kanaya, S.; Ishida, Y.; Taniguchi, K.; Isogaki, J.; Inaba, K.; Yanaga, K.; Uyama, I. Laparoscopic versus open D2 gastrectomy for advanced gastric cancer: A retrospective cohort study. Surg. Endosc. 2013, 27, 286–294. [Google Scholar] [CrossRef]
- Lin, J.X.; Lin, J.P.; Desiderio, J.; Xie, J.W.; Gemini, A.; Wang, J.B.; Lu, J.; Chen, Q.Y.; Cao, L.L.; Lin, M.; et al. Difference in the short-term outcomes of laparoscopic gastrectomy for gastric carcinoma between the east and west: A retrospective study from the IMIGASTRIC trial. J. Cancer 2019, 10, 4106–4113. [Google Scholar] [CrossRef] [PubMed]
- Kong, S.H.; Lee, H.J.; Ahn, H.S.; Kim, J.W.; Kim, W.H.; Lee, K.U.; Yang, H.K. Stage migration effect on survival in gastric cancer surgery with extended lymphadenectomy: The reappraisal of positive lymph node ratio as a proper N-staging. Ann. Surg. 2012, 255, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Miyashiro, I.; Ishikawa, T.; Akazawa, K.; Fukui, K.; Katai, H.; Nunobe, S.; Oda, I.; Isobe, Y.; Tsujitani, S.; et al. Determinant Factors on Differences in Survival for Gastric Cancer Between the United States and Japan Using Nationwide Databases. J. Epidemiol. 2021, 31, 241–248. [Google Scholar] [CrossRef] [Green Version]
- Petrelli, F.; Ghidini, M.; Barni, S.; Steccanella, F.; Sgroi, G.; Passalacqua, R.; Tomasello, G. Prognostic Role of Primary Tumor Location in Non-Metastatic Gastric Cancer: A Systematic Review and Meta-Analysis of 50 Studies. Ann. Surg. Oncol. 2017, 24, 2655–2668. [Google Scholar] [CrossRef] [PubMed]
- Groth, S.S.; Habermann, E.B.; Massarweh, N.N. United States Administrative Databases and Cancer Registries for Thoracic Surgery Health Services Research. Ann. Thorac. Surg. 2020, 109, 636–644. [Google Scholar] [CrossRef] [PubMed]
- Sarrazin, M.S.; Rosenthal, G.E. Finding pure and simple truths with administrative data. JAMA 2012, 307, 1433–1435. [Google Scholar] [CrossRef]
- Fang, C.; Hua, J.; Li, J.; Zhen, J.; Wang, F.; Zhao, Q.; Shuang, J.; Du, J. Comparison of long-term results between laparoscopy-assisted gastrectomy and open gastrectomy with D2 lymphadenectomy for advanced gastric cancer. Am. J. Surg. 2014, 208, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Japanese Gastric Cancer Association. Japanese Classification of Gastric Carcinoma—2nd English Edition. Gastric Cancer 1998, 1, 10–24. [Google Scholar] [CrossRef] [Green Version]
- Wagner, A.D.; Syn, N.L.; Moehler, M.; Grothe, W.; Yong, W.P.; Tai, B.C.; Ho, J.; Unverzagt, S. Chemotherapy for advanced gastric cancer. Cochrane Database Syst. Rev. 2017, 8, CD004064. [Google Scholar] [CrossRef] [PubMed]
- Reddavid, R.; Sofia, S.; Chiaro, P.; Colli, F.; Trapani, R.; Esposito, L.; Solej, M.; Degiuli, M. Neoadjuvant chemotherapy for gastric cancer. Is it a must or a fake? World J. Gastroenterol. 2018, 24, 274–289. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Matched Cohort | |||
|---|---|---|---|
| Laparoscopic n = 624 | Open n = 624 | p-Value | |
| Age, years | 0.985 # | ||
| median (IQR) | 63 (6–72) | 64 (56–72) | |
| mean (SD) | 63.2 (11.3) | 63 (11.9) | |
| Gender, n (%) | 0.849 | ||
| Male | 466 (73.1) | 453 (72.6) | |
| Female | 168 (26.9) | 171 (27.4) | |
| Geographic area, n (%) | 0.829 | ||
| East | 504 (80.8) | 507 (81.3) | |
| West | 120 (19.2) | 117 (18.8) | |
| Year of surgery, n (%) | 1.000 | ||
| 2000–2007 | 16 (2.6) | 16 (2.6) | |
| 2008–2014 | 608 (97.4) | 608 (97.4) | |
| Body Mass Index (BMI) | 0.350 # | ||
| median (IQR) | 22 (20–24) | 22 (20–24) | |
| mean (SD) | 22.3 (3.1) | 22.1 (3.3) | |
| ASA score, n (%) | 1.000 | ||
| I | 295 (47.3) | 295 (47.3) | |
| II | 245 (39.3) | 245 (39.3) | |
| III | 84 (13.5) | 84 (13.5) | |
| Comorbidities, n (%) | 0.816 | ||
| No | 388 (62.2) | 384 (61.5) | |
| Yes | 236 (37.8) | 240 (38.5) | |
| Type of resection, n (%) | 0.955 | ||
| Distal gastrectomy | 293 (47) | 294 (47.1) | |
| Total gastrectomy | 331 (53) | 330 (52.9) | |
| Tumor location, n (%) | 0.731 | ||
| Distal third | 290 (46.5) | 284 (45.5) | |
| Middle third | 149 (23.9) | 161 (25.8) | |
| Upper third | 185 (29.6) | 179 (28.7) | |
| pTNM AJCC stage, 8th edition, n (%) | 0.860 | ||
| IA | 101 (16.2) | 91 (14.6) | |
| IB | 49 (7.9) | 43 (6.9) | |
| IIA | 67 (10.7) | 69 (11.1) | |
| IIB | 73 (11.7) | 68 (10.9) | |
| IIIA | 112 (17.9) | 117 (18.8) | |
| IIIB | 120 (19.2) | 117 (18.8) | |
| IIIC | 102 (16.3) | 119 (19.1) | |
| Histology, n (%) | 0.767 | ||
| Differentiated | 405 (64.9) | 400 (64.1) | |
| Poorly differentiated/undifferentiated | 219 (35.1) | 224 (35.9) | |
| Matched Cohort | |||
|---|---|---|---|
| LG n = 624 | OG n = 624 | p-Value | |
| Total operative time (minutes) | <0.0001 # | ||
| Median (IQR) | 180 (150–210) | 240 (180–300) | |
| Mean (SD) | 192.7 (72.6) | 243.7 (86.5) | |
| Conversion to open surgery, n (%) | 12 (1.9) | N/A | N/A |
| N. harvested lymph nodes | <0.0001 # | ||
| Median (IQR) | 32 (24–40) | 28 (22–38) | |
| Mean (SD) | 33.2 (12.6) | 31.3 (14.1) | |
| N. metastatic lymph nodes | 0.400 # | ||
| Median (IQR) | 3 (0–11) | 3 (0–11) | |
| Mean (SD) | 7 (9.1) | 7.6 (10.8) | |
| R factors | 0.021 | ||
| R0 | 604 (96.8) | 587 (94.1) | |
| R + (R1 − R2) | 20 (3.2) | 37 (5.9) | |
| Neoadjuvant chemotherapy, n (%) | 0.493 | ||
| Yes | 20 (3.2) | 15 (2.4) | |
| No | 604 (96.8) | 609 (97.6) | |
| Neoadjuvant radiotherapy, n (%) | 1.000 | ||
| Yes | 1 (0.2) | 0 (0) | |
| No | 623 (99.8) | 624 (100) | |
| Histology types in detail, n (%) | 0.767 | ||
| Differentiated (total) | 405 (64.9) | 400 (64.1) | |
| Tubular well-differentiated | 358 (57.4) | 301 (48.2) | |
| Tubular moderately differentiated | 40 (6.4) | 91 (14.6) | |
| Papillary | 7 (1.1) | 8 (1.3) | |
| Poorly differentiated/Undifferentiated (total) | 219 (35.1) | 224 (35.9) | |
| Mucinous | 69 (11.1) | 50 (8) | |
| Signet ring cell | 97 (15.5) | 96 (15.4) | |
| Poorly differentiated solid/non-solid type * | 43 (6.9) | 76 (12.2) | |
| Undifferentiated | 10 (1.6) | 2 (0.3) | |
| Postoperative hospital stay (days) | <0.0001 # | ||
| Median (IQR) | 10 (9–13) | 14.8 (10–17) | |
| Mean (SD) | 12.2 (8.2) | 13 (7.6) | |
| Patients with complications, n (%) | 94 (15.1) | 133 (21.3) | 0.004 |
| Clavien-Dindo complications, n (%) | 0.433 | ||
| I | 9 (6.4) | 16 (9.3) | |
| II | 106 (74.6) | 121 (70) | |
| IIIa | 8 (5.6) | 7 (4) | |
| IIIb | 8 (5.6) | 17 (9.8) | |
| IVa | 8 (5.6) | 10 (5.8) | |
| IVb | 2 (1.4) | 0 (0) | |
| V | 1 (0.8) | 2 (1.1) | |
| Total | 142 (100) | 173 (100) | |
| Severe in-hospital complications, n (%) | 0.689 | ||
| Clavien-Dindo ≥ 3 | 27 (19) | 36 (20.8) | |
| Reoperation, n of patients (%) | 10 (1.6) | 17 (2.7) | 0.392 |
| In-hospital mortality, n (%) | 1 (0.2) | 2 (0.3) | 0.563 |
| Matched Cohort | |||
|---|---|---|---|
| Laparoscopic n = 624 | Open n = 624 | p-Value | |
| Acute pancreatitis | 0 | 0 | 1.000 |
| Acute renal failure | 0 | 0 | 1.000 |
| Adhesive ileus | 0 | 0 | 1.000 |
| Anastomotic stenosis | 2 | 0 | 0.499 |
| Anostomosis leakage | 12 | 12 | 1.000 |
| Arrhythmias | 4 | 4 | 1.000 |
| Atelectasia | 1 | 0 | 1.000 |
| Bleeding (intra/extraluminal) | 9 | 10 | 1.000 |
| Cholecystitis | 0 | 0 | 1.000 |
| Chylous leakage | 6 | 8 | 0.789 |
| Congestive heart failure | 3 | 1 | 0.624 |
| Cerebrovascular accident | 0 | 0 | 1.000 |
| Deep vein thrombosis | 2 | 0 | 0.499 |
| Delayed gastric emptying | 8 | 7 | 1.000 |
| Delirium | 0 | 0 | 1.000 |
| Disseminated intravascular coagul. | 1 | 0 | 1.000 |
| Dizziness | 0 | 0 | 1.000 |
| Dumping syndrome | 0 | 0 | 1.000 |
| Intra-abdominal fluid collection | 14 | 9 | 0.400 |
| Incisional hernia | 1 | 2 | 1.000 |
| Liver failure | 0 | 0 | 1.000 |
| Myocardial infarction | 1 | 0 | 1.000 |
| Omental infarction | 0 | 1 | 1.000 |
| Pancreatic fistula | 2 | 6 | 0.287 |
| Pleural effusion | 3 | 2 | 1.000 |
| Pneumonia | 33 | 61 | 0.003 |
| Prolonged postoperative ileus | 1 | 1 | 1.000 |
| Pseudomembranous colitis | 2 | 2 | 1.000 |
| Pulmonary edema | 0 | 1 | 1.000 |
| Pulmonary embolism | 1 | 0 | 1.000 |
| Remnant stomach necrosis | 1 | 0 | 1.000 |
| Sepsis | 1 | 0 | 1.000 |
| Small bowel infarction | 0 | 2 | 0.499 |
| Small bowel perforation | 0 | 3 | 0.249 |
| Unexplained postoperative fever | 2 | 1 | 1.000 |
| Wound infection | 9 | 15 | 0.302 |
| Wound seroma | 0 | 1 | 1.000 |
| Other complications | 23 | 24 | 1.000 |
| Total | 142 | 173 | 0.043 |
| N of Patients | Five-Year Survival Rate | p-Value * | |||
|---|---|---|---|---|---|
| Laparoscopy | Open | Laparoscopy % | Open % | ||
| Entire cohort | |||||
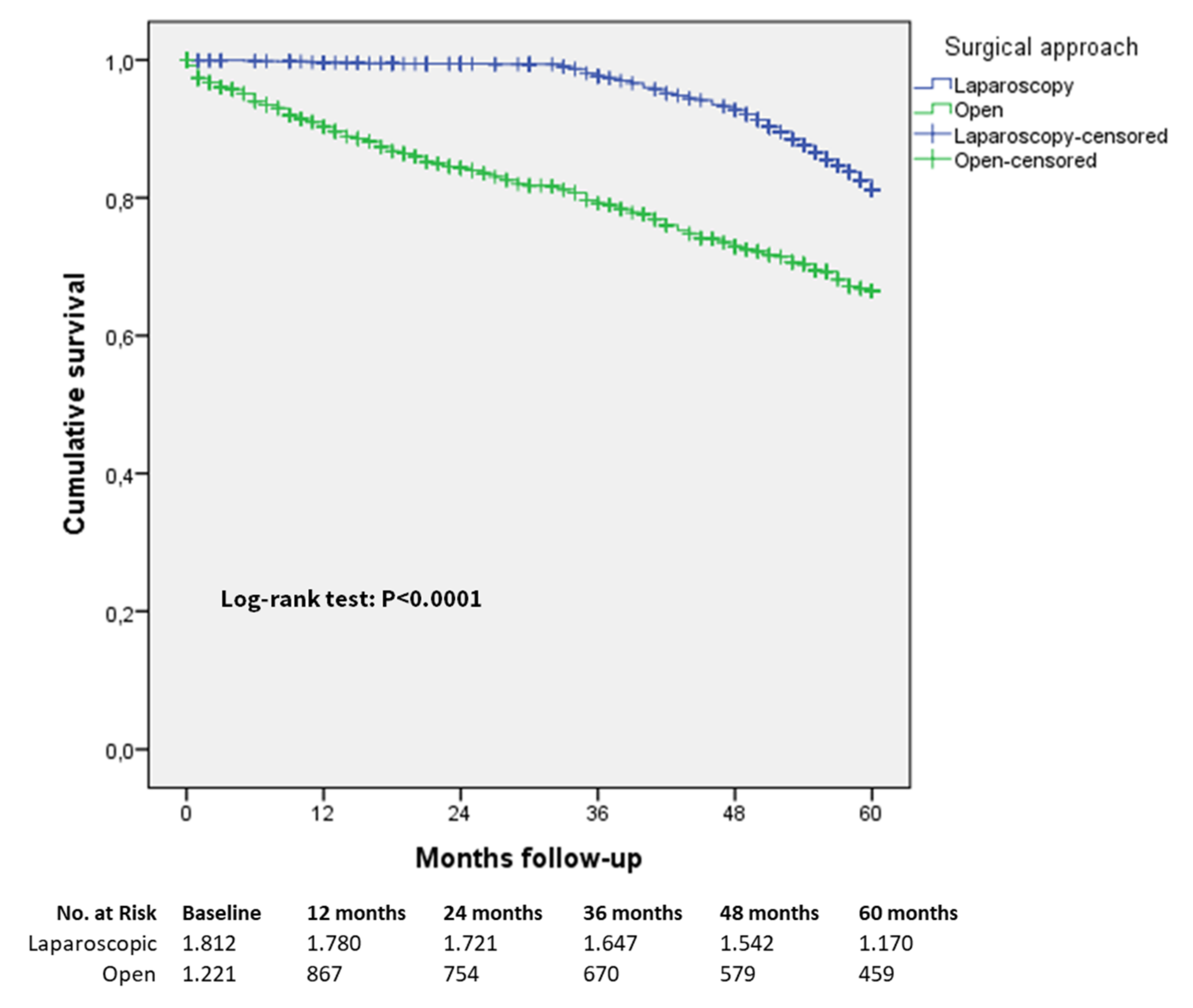
| All patients | 1812 | 1221 | 81.1 | 66.4 | <0.0001 |
| Stage IA | 358 | 199 | 97.4 | 93.5 | 0.029 |
| Stage IB | 156 | 130 | 94.2 | 75 | <0.0001 |
| Stage IIA | 191 | 161 | 90.4 | 70.3 | <0.0001 |
| Stage IIB | 213 | 144 | 88.5 | 79 | 0.002 |
| Stage IIIA | 309 | 231 | 78.5 | 56.6 | <0.0001 |
| Stage IIIB | 352 | 195 | 69 | 51 | <0.0001 |
| Stage IIIC | 233 | 161 | 60.1 | 48.5 | 0.001 |
| Matched cohort | |||||
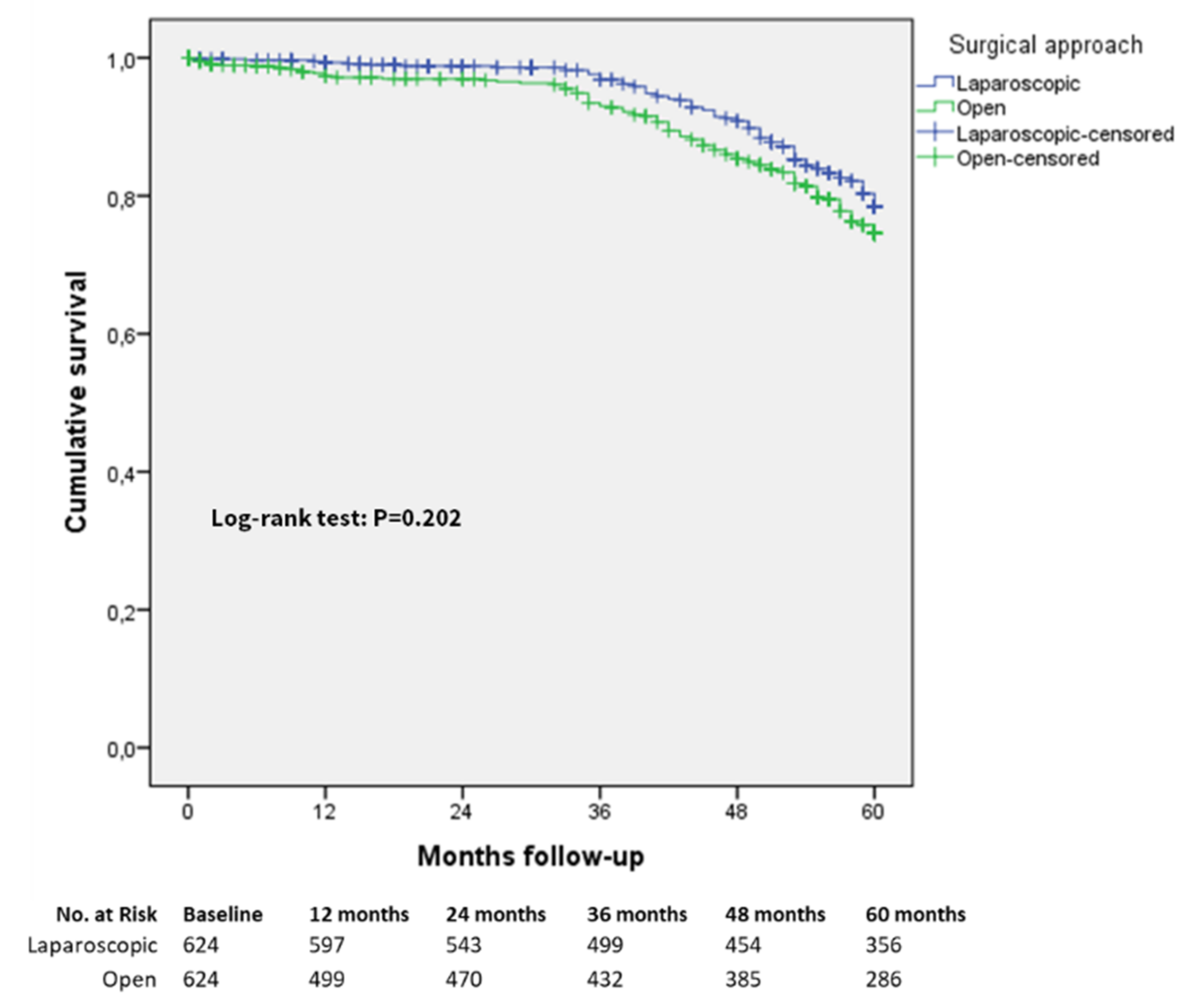
| All patients | 624 | 624 | 77.4 | 75.2 | 0.202 |
| Stage I | 150 | 134 | 96.4 | 94 | 0.432 |
| Stage IA | 101 | 91 | 95 | 98 | 0.189 |
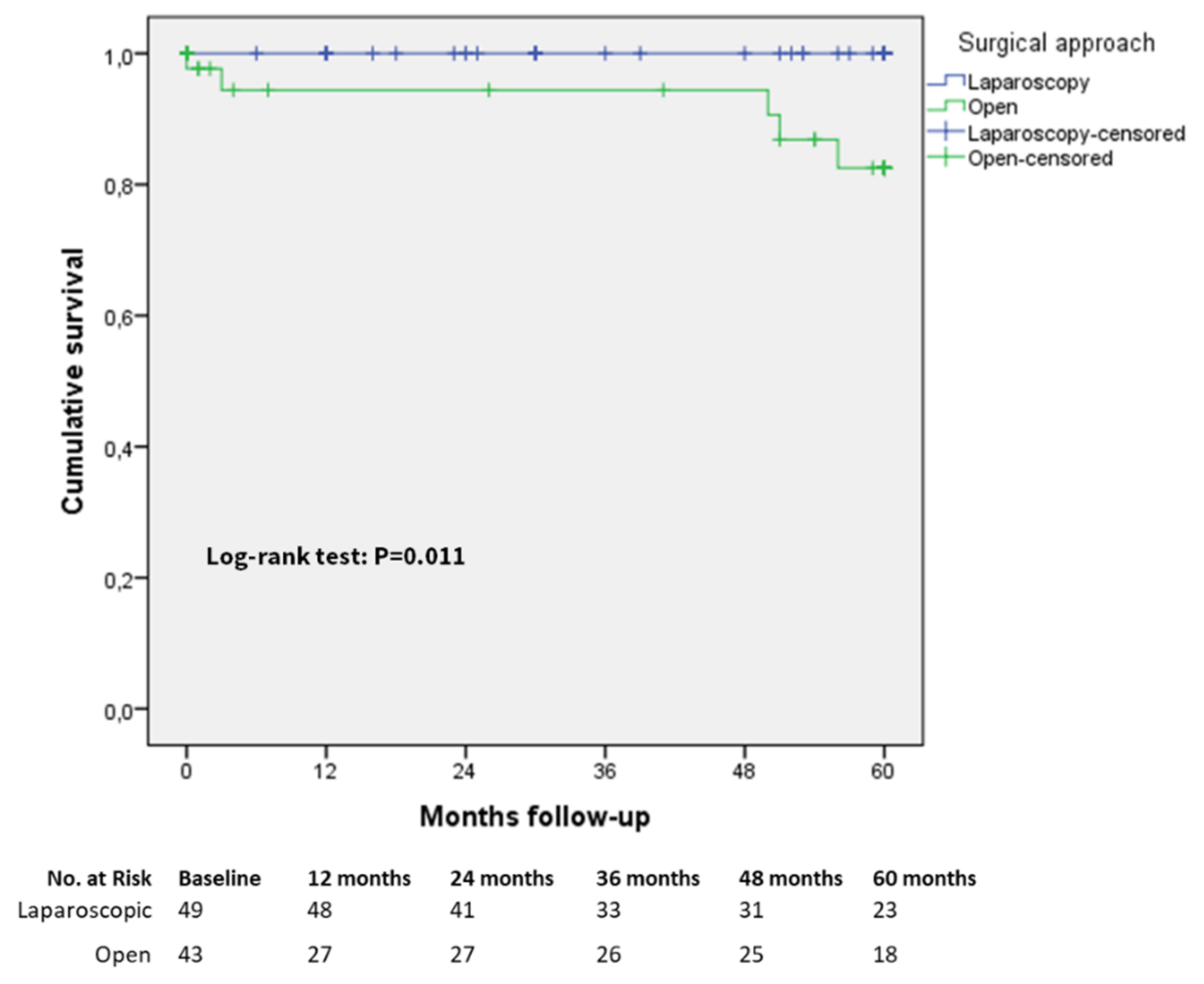
| Stage IB | 49 | 43 | 100 | 82 | 0.011 |
| Stage II | 140 | 137 | 86.7 | 83.8 | 0.469 |
| Stage IIA | 67 | 69 | 87 | 77.2 | 0.146 |
| Stage IIB | 73 | 68 | 86.6 | 91 | 0.509 |
| Stage III | 334 | 353 | 67.8 | 65 | 0.264 |
| Stage IIIA | 112 | 117 | 74.8 | 74.6 | 0.679 |
| Stage IIIB | 120 | 117 | 69 | 63.7 | 0.406 |
| Stage IIIC | 102 | 119 | 59.5 | 58.2 | 0.621 |
| Overall Cohort | Univariable Cox Regression | Multivariable Cox Regression | ||||
|---|---|---|---|---|---|---|
| N | Hazard Rate (95% CI) | p-Value | Hazard Rate (95% CI) | p-Value | ||
| Age, years | 3033 | 1.029 (1.021–1.036) | <0.0001 | 1.019 (1.011–1.027) | <0.0001 | |
| Gender | ||||||
| Male | 2165 | Reference | ||||
| Female | 868 | 1.249 (1.050–1.485) | 0.012 | |||
| Geographic area | ||||||
| East | 2187 | Reference | Reference | |||
| West | 846 | 3.718 (3.137–4.406) | <0.0001 | 6.482 (5.322–7.895) | <0.0001 | |
| Year of surgery | ||||||
| 2000–2007 | 433 | Reference | ||||
| 2008–2014 | 2600 | 0.342 (0.281–0.415) | <0.0001 | |||
| Body mass index (BMI) | 3033 | 1.027 (1.004–1.050) | 0.021 | |||
| ASA score | ||||||
| I | 1508 | Reference | Reference | |||
| II | 1211 | 1.674 (1.413–1.982) | <0.0001 | 1.273 (1.065–1.521) | 0.008 | |
| III | 314 | 2.387 (1.789–3.184) | <0.0001 | 1.338 (0.980–1.827) | 0.067 | |
| Operative time | 3033 | 1.002 (1.001–1.003) | <0.0001 | |||
| Surgical approach | ||||||
| Open | 1221 | Reference | ||||
| Laparoscopic | 1812 | 0.426 (0.363–0.500) | <0.0001 | |||
| Length of hospital stay | 3033 | 1.010 (1.001–1.018) | 0.012 | |||
| Type of resection | ||||||
| Distal gastrectomy | 1365 | Reference | ||||
| Total gastrectomy | 1668 | 2.011 (1.685–2.400) | <0.0001 | |||
| Tumor location | ||||||
| Upper third | 894 | Reference | Reference | |||
| Middle third | 819 | 0.968 (0.798–1.174) | 0.740 | 0.859 (0.707–1.045) | 0.129 | |
| Distal third | 1320 | 0.519 (0.427–0.632) | <0.0001 | 0.772 (0.633–0.941) | 0.011 | |
| N. harvested lymph nodes | 3033 | 1.009 (1.003–1.015) | 0.003 | |||
| Margin status | ||||||
| Free | 2939 | Reference | ||||
| Infiltrated | 94 | 3.072 (2.192–4.306) | <0.0001 | |||
| pTNM stage, 8th edition | ||||||
| IIIC | 394 | Reference | Reference | |||
| IIIB | 547 | 0.809 (0.651–1.006) | 0.056 | 0.810 (0.604–1.805) | 0.157 | |
| IIIA | 540 | 0.657 (0.521–0.827) | <0.0001 | 0.645 (0.454–0.916) | 0.014 | |
| IIB | 357 | 0.305 (0.217–0.429) | <0.0001 | 0.282 (0.179–0.443) | <0.0001 | |
| IIA | 352 | 0.345 (0.248–0.480) | <0.0001 | 0.261 (0.165–0.412) | <0.0001 | |
| IB | 286 | 0.258 (0.173–0.386) | <0.0001 | 0.171 (0.102–0.288) | <0.0001 | |
| IA | 557 | 0.073 (0.045–0.118) | <0.0001 | 0.057 (0.032–0.102) | 0.0004 | |
| N. of metastatic lymph nodes | 3111 | 1.040 (1.034–1.045) | 0.039 | <0.0001 | 1.018 (1.006–1.030) | 0.004 |
| Histology, n (%) | ||||||
| Tubular, Well-diff. (tub1) | 1596 | Reference | ||||
| Tubular, mod. diff. (tub2) | 368 | 3.331 (2.541–4.367) | <0.0001 | |||
| Papillary (pap) | 51 | 1.535 (0.840–2.805) | 0.163 | |||
| Mucinous (muc) | 236 | 1.422 (1.062–1.905) | 0.018 | |||
| Signet ring cell (sig) | 484 | 1.801 (1.452–2.235) | <0.0001 | |||
| Poorly diff. solid/non-solid (por1/2) * | ||||||
| Undifferentiated | 275 | 4.573 (3.481–6.008) | <0.0001 | |||
| carcinoma | 23 | 3.907 (1.933–7.897) | <0.0001 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trastulli, S.; Desiderio, J.; Lin, J.-X.; Reim, D.; Zheng, C.-H.; Borghi, F.; Cianchi, F.; Norero, E.; Nguyen, N.T.; Qi, F.; et al. Laparoscopic Compared with Open D2 Gastrectomy on Perioperative and Long-Term, Stage-Stratified Oncological Outcomes for Gastric Cancer: A Propensity Score-Matched Analysis of the IMIGASTRIC Database. Cancers 2021, 13, 4526. https://doi.org/10.3390/cancers13184526
Trastulli S, Desiderio J, Lin J-X, Reim D, Zheng C-H, Borghi F, Cianchi F, Norero E, Nguyen NT, Qi F, et al. Laparoscopic Compared with Open D2 Gastrectomy on Perioperative and Long-Term, Stage-Stratified Oncological Outcomes for Gastric Cancer: A Propensity Score-Matched Analysis of the IMIGASTRIC Database. Cancers. 2021; 13(18):4526. https://doi.org/10.3390/cancers13184526
Chicago/Turabian StyleTrastulli, Stefano, Jacopo Desiderio, Jian-Xian Lin, Daniel Reim, Chao-Hui Zheng, Felice Borghi, Fabio Cianchi, Enrique Norero, Ninh T. Nguyen, Feng Qi, and et al. 2021. "Laparoscopic Compared with Open D2 Gastrectomy on Perioperative and Long-Term, Stage-Stratified Oncological Outcomes for Gastric Cancer: A Propensity Score-Matched Analysis of the IMIGASTRIC Database" Cancers 13, no. 18: 4526. https://doi.org/10.3390/cancers13184526