
Whole-Body Vibration Associated with Strength Training on the Lower-Limb Blood Flow and Mobility in Older Adults with Type 2 Diabetes: A Study Protocol for a Randomized Controlled Trial

 , , , , , , ,
, , , , , , ,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
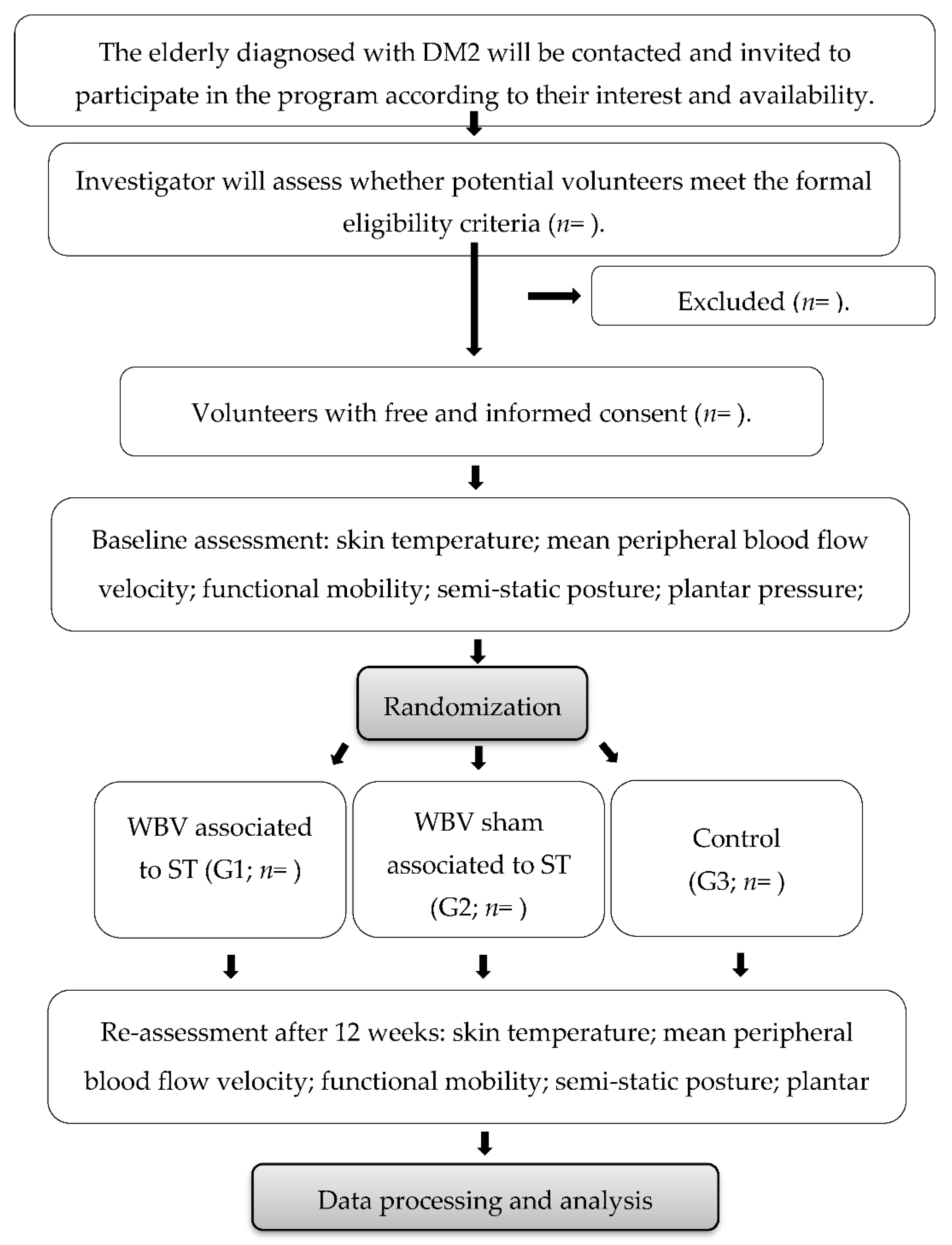
2.1. Experimental Design and Location
2.2. Sampling and Enrollment Strategies
2.3. Eligibility Criteria
2.4. Sample Size
2.5. Randomization and Blinding
2.6. Intervention
2.7. Outcome Measurements
2.7.1. Primary Outcomes
- Skin temperature
- Mean peripheral arterial blood flow velocity
- Mobility
2.7.2. Secondary Outcomes
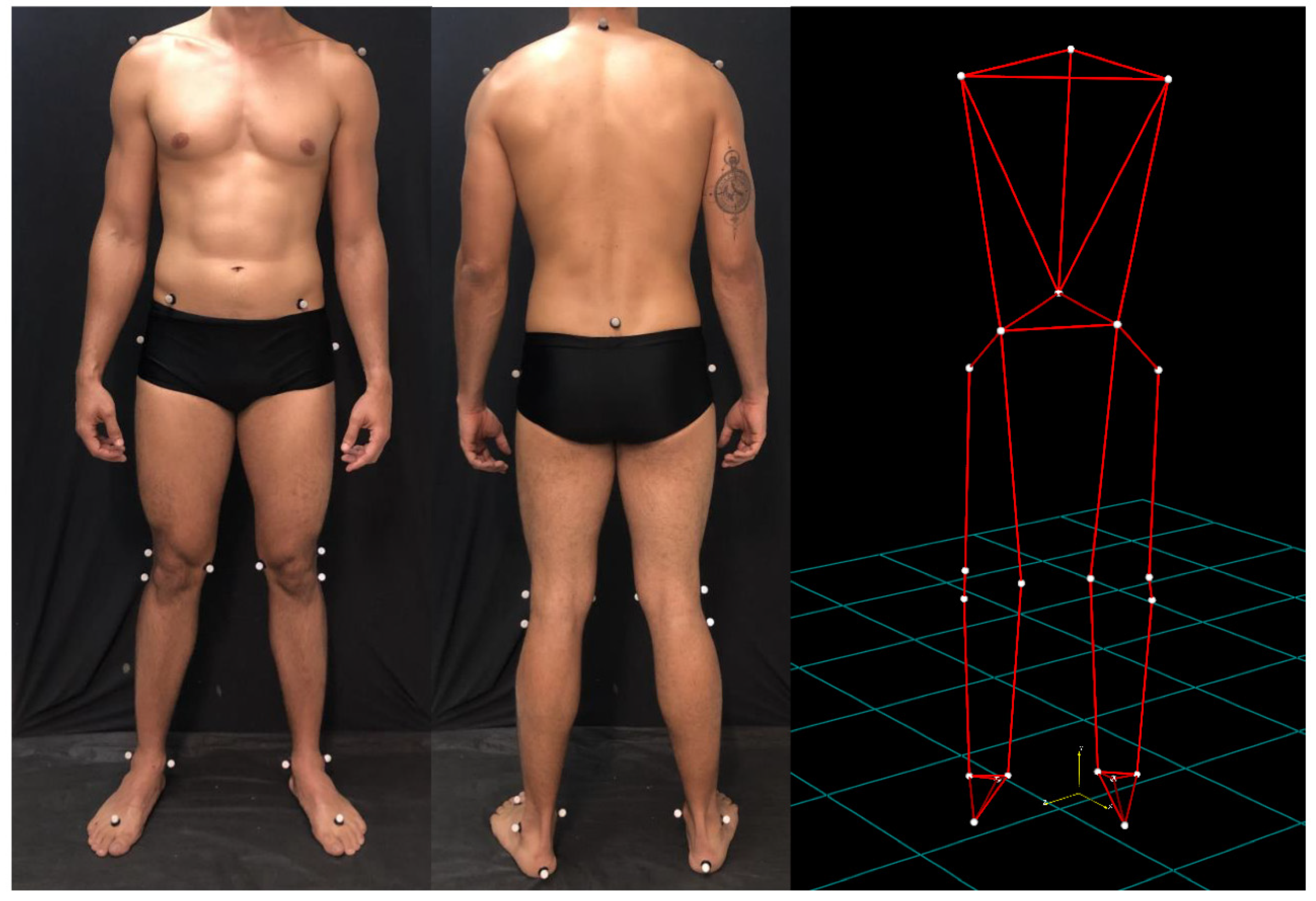
- Quasi-static posture
- Plantar pressure and body balance
2.8. Monitoring Measurements
- Vital signs and capillary glycemia
- Other biochemical markers
2.9. Data Processing and Analysis
3. Discussion
4. Strengths and Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Siddiqui, M.I. Health of the Elderly. In Book: Community Medicine & Public Health, 8th ed.; Time Publisher: New York, NY, USA, 2016; pp. 595–600. [Google Scholar]
- Giovannini, S.; Onder, G.; Lattanzio, F.; Bustacchini, S.; Di Stefano, G.; Moresi, R.; Russo, A.; Bernabei, R.; Landi, F. Selenium concentrations and mortality among community-dwelling older adults: Results from IlSIRENTE study. J. Nutr. Health Aging 2018, 22, 608–612. [Google Scholar] [CrossRef] [PubMed]
- Giovannini, S.; Onder, G.; Leeuwenburgh, C.; Carter, C.; Marzetti, E.; Russo, A.; Capoluongo, E.; Pahor, M.; Bernabei, R.; Landi, F. Myeloperoxidase levels and mortality in frail community-living elderly individuals. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2010, 65, 369–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Onder, G.; Giovannini, S.; Sganga, F.; Manes-Gravina, E.; Topinkova, E.; Finne-Soveri, H.; Garms-Homolová, V.; Declercq, A.; van der Roest, H.G.; Jónsson, P.V.; et al. Interactions between drugs and geriatric syndromes in nursing home and home care: Results from Shelter and IBenC projects. Aging Clin. Exp. Res. 2018, 30, 1015–1021. [Google Scholar] [CrossRef] [PubMed]
- Alves, K.F.; Ferreira, A.P.; Parente, L.C.; Rodrigues, F.T.; Marques, T.V.; Antonino, G.B.; Melo, L.C.; Villela, D.W.; Guerino, M.R.; Leite, W.S.; et al. Immediate Effect of Whole-Body Vibration on Skin Temperature and Lower-Limb Blood Flow in Older Adults with Type 2 Diabetes: Pilot Study. Appl. Sci. 2020, 10, 690. [Google Scholar] [CrossRef] [Green Version]
- Cho, N.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Sociedade Brasileira de Diabetes. Diretrizes da Sociedade Brasileira de Diabetes (2019–2020); Sociedade Brasileira de Diabetes: Brasília, Brazil, 2019. [Google Scholar]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014, 37 (Suppl. 1), S81–S90. [Google Scholar] [CrossRef] [Green Version]
- Nordström, A.; Hadrévi, J.; Olsson, T.; Franks, P.W.; Nordström, P. Higher prevalence of type 2 diabetes in men than in women is associated with differences in visceral fat mass. J. Clin. Endocrinol. Metab. 2016, 101, 3740–3746. [Google Scholar] [CrossRef] [Green Version]
- Clough, G.F.; Kuliga, K.Z.; Chipperfield, A.J. Flow motion dynamics of microvascular blood flow and oxygenation: Evidence of adaptive changes in obesity and type 2 diabetes mellitus/insulin resistance. Microcirculation 2017, 24, e12331. [Google Scholar] [CrossRef]
- McClatchey, P.M.; Bauer, T.A.; Regensteiner, J.G.; Reusch, J.E. Exercise, blood flow, and the skeletal muscle microcirculation in diabetes mellitus. In Diabetes and Exercise 2018; Humana Press: Cham, Switzerland, 2018; pp. 165–172. [Google Scholar]
- Jannu, C.; Babu, P.S.; Puchchakayala, G.; Chandupatla, V.D. Efficacy of interferential therapy versus transcutaneous electrical nerve stimulation to reduce pain in patients with diabetic neuropathy. Indian J. Public Health Res. Dev. 2018, 9, 121–124. [Google Scholar] [CrossRef]
- Mustapa, A.; Justine, M.; Mohd Mustafah, N.; Jamil, N.; Manaf, H. Postural control and gait performance in the diabetic peripheral neuropathy: A systematic review. BioMed Res. Int. 2016, 2016, 9305025. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.Y.; Tsai, Y.J.; Liao, Y.T.; Yang, Y.C.; Lu, F.H.; Lin, S.I. Reactive balance control in older adults with diabetes. Gait Posture 2018, 61, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Kalyani, R.R.; Tian, J.; Xue, Q.L.; Walston, J.; Cappola, A.R.; Fried, L.P.; Brancati, F.L.; Blaum, C.S. Hyperglycemia and incidence of frailty and lower extremity mobility limitations in older women. J. Am. Geriatr. Soc. 2012, 60, 1701–1707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, S.; Cai, X.; Yin, H.; Sun, Z.; Zügel, M.; Steinacker, J.M.; Schumann, U. Exercise training and endothelial function in patients with type 2 diabetes: A meta-analysis. Cardiovasc. Diabetol. 2018, 17, 64. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos Araujo, J.E.; Macedo, F.N.; Barreto, A.S.; dos Santos, M.R.; Antoniolli, A.R.; Quintans-Junior, L.J. Effects of Resistance and Combined training on Vascular Function in Type 2 Diabetes: A Systematic Review of Randomized Controlled Trials. Rev. Diabet. Stud. 2019, 15, 16–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Pozo-Cruz, B.; Alfonso-Rosa, R.M.; del Pozo-Cruz, J.; Sañudo, B.; Rogers, M.E. Effects of a 12-wk whole-body vibration based intervention to improve type 2 diabetes. Maturitas 2014, 77, 52–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramos, L.A.; Rodrigues, F.T.; Shirahige, L.; Barros, M.D.; de Carvalho, A.G.; Guerino, M.R.; de Lima Ferreira, A.P.; Guerra, R.O.; de Araújo, M.D. A single whole body vibration session influences quadriceps muscle strength, functional mobility and balance of elderly with osteopenia and/or osteoporosis? Pragmatic clinical trial. J. Diabetes Metab. Disord. 2019, 18, 73–80. [Google Scholar] [CrossRef]
- Piotrowska, A.; Czerwińska-Ledwig, O.; Stefańska, M.; Pałka, T.; Maciejczyk, M.; Bujas, P.; Bawelski, M.; Ridan, T.; Żychowska, M.; Sadowska-Krępa, E.; et al. Changes in Skin Microcirculation Resulting from Vibration Therapy in Women with Cellulite. Int. J. Environ. Res. Public Health 2022, 19, 3385. [Google Scholar] [CrossRef]
- Maciejczyk, M.; Bawelski, M.; Więcek, M.; Szygula, Z.; Michailov, M.L.; Vadašová, B.; Kačúr, P.; Pałka, T. Acute Effects of Whole-Body Vibration on Resting Metabolic Rate and Substrate Utilisation in Healthy Women. Biology 2022, 11, 655. [Google Scholar] [CrossRef]
- Johnson, P.K.; Feland, J.B.; Johnson, A.W.; Mack, G.W.; Mitchell, U.H. Effect of whole body vibration on skin blood flow and nitric oxide production. J. Diabetes Sci. Technol. 2014, 8, 889–894. [Google Scholar] [CrossRef] [Green Version]
- Sañudo, B.; Alfonso-Rosa, R.; del Pozo-Cruz, B.; del Pozo-Cruz, J.; Galiano, D.; Figueroa, A. Whole body vibration training improves leg blood flow and adiposity in patients with type 2 diabetes mellitus. Eur. J. Appl. Physiol. 2013, 113, 2245–2252. [Google Scholar] [CrossRef] [Green Version]
- Robinson, C.C.; Barreto, R.P.; Sbruzzi, G.; Plentz, R.D. The effects of whole body vibration in patients with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Braz. J. Phys. Ther. 2016, 20, 4–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomes-Neto, M.; de Sá-Caputo, D.D.; Paineiras-Domingos, L.L.; Brandão, A.A.; Neves, M.F.; Marin, P.J.; Sañudo, B.; Bernardo-Filho, M. Effects of Whole-Body Vibration in Older Adult Patients with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Can. J. Diabetes 2019, 43, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Bemben, D.A.; Palmer, I.J.; Bemben, M.G.; Knehans, A.W. Effects of combined whole-body vibration and resistance training on muscular strength and bone metabolism in postmenopausal women. Bone 2010, 47, 650–656. [Google Scholar] [CrossRef]
- Marín, P.J.; Rhea, M.R. Effects of vibration training on muscle power: A meta-analysis. J. Strength Cond. Res. 2010, 24, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Osawa, Y.; Oguma, Y. Effects of resistance training with whole-body vibration on muscle fitness in untrained adults. Scand. J. Med. Sci. Sports 2013, 23, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.; Tetzlaff, J.M.; Gøtzsche, P.C.; Altman, D.G.; Mann, H.; Berlin, J.A.; Dickersin, K.; Hróbjartsson, A.; Schulz, K.F.; Parulekar, W.R.; et al. SPIRIT 2013 explanation and elaboration: Guidance for protocols of clinical trials. BMJ 2013, 346, e7586. [Google Scholar] [CrossRef] [Green Version]
- Schultz, K.F. CONSORT statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18–27. [Google Scholar] [CrossRef] [Green Version]
- Ioannidis, J.P.; Evans, S.J.; Gøtzsche, P.C.; O’neill, R.T.; Altman, D.G.; Schulz, K.; Moher, D. Better reporting of harms in randomized trials: An extension of the CONSORT statement. Ann. Intern. Med. 2004, 141, 781–788. [Google Scholar] [CrossRef]
- World Health Organization (WHO). BMI Classification. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-ealthy-lifestyle/body-mass-index-bmi (accessed on 22 July 2019).
- Lourenço, R.A.; Veras, R.P. Mini-Exame do Estado Mental: Características psicométricas em idosos ambulatoriais. Rev. Saúde Pública 2006, 40, 712–719. [Google Scholar] [CrossRef]
- Sardinha, A.; Levitan, M.N.; Lopes, F.L.; Perna, G.; Esquivel, G.; Griez, E.J.; Nardi, A.E. Tradução e adaptação transcultural do Questionário de Atividade Física Habitual. Arch. Clin. Psychiatry 2010, 37, 16–22. [Google Scholar] [CrossRef]
- Selfe, J.; Whitaker, J.; Hardaker, N. A narrative literature review identifying the minimum clinically important difference for skin temperature asymmetry at the knee. Thermol. Int. 2008, 18, 41–44. [Google Scholar]
- Wang, H.; Chow, S.C. Sample size calculation for comparing proportions. Encycl. Stat. Sci. 2004, 10, 9781118445112. [Google Scholar]
- Larose, J.; Sigal, R.J.; Boule, N.G.; Wells, G.A.; Prud’homme, D.; Fortier, M.S.; Reid, R.D.; Tulloch, H.; Coyle, D.; Phillips, P.; et al. Effect of exercise training on physical fitness in type II diabetes mellitus. Med. Sci. Sports Exerc. 2010, 42, 1439–1447. [Google Scholar] [CrossRef] [PubMed]
- Evans, N.A. Anatomia da Musculação: Guia Ilustrado para o Aumento de Massa e Definição do Corpo (Portuguese Brazilian), 2nd ed.; Manole: Barueri, SP, Brazil, 2017. [Google Scholar]
- American College of Sports Medicine. American College of Sports Medicine Position Stand. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 1998, 30, 992–2008. [Google Scholar]
- Phillips, W.T.; Batterham, A.M.; Valenzuela, J.E.; Burkett, L.N. Reliability of maximal strength testing in older adults. Arch. Phys. Med. Rehabil. 2004, 85, 329–334. [Google Scholar] [CrossRef]
- Sá-Caputo, D.; Paineiras-Domingos, L.L.; Francisca-Santos, A.; dos Anjos, E.M.; Reis, A.S.; Neves, M.F.; Oigman, W.; Oliveira, R.; Brandão, A.; Machado, C.B.; et al. Whole-body vibration improves the functional parameters of individuals with metabolic syndrome: An exploratory study. BMC Endocr. Disord. 2019, 19, 6. [Google Scholar] [CrossRef] [Green Version]
- Rosenberger, A.; Beijer, Å.; Schoenau, E.; Mester, J.; Rittweger, J.; Zange, J. Changes in motor unit activity and respiratory oxygen uptake during 6 weeks of progressive whole-body vibration combined with progressive, high intensity resistance training. J. Musculoskelet. Neuronal Interact. 2019, 19, 159. [Google Scholar]
- Kang, J.; Porfido, T.; Ismaili, C.; Selamie, S.; Kuper, J.; Bush, J.A.; Ratamess, N.A.; Faigenbaum, A.D. Metabolic responses to whole-body vibration: Effect of frequency and amplitude. Eur. J. Appl. Physiol. 2016, 116, 1829–1839. [Google Scholar] [CrossRef]
- Rittweger, J. Metabolic Responses to Whole-Body Vibration Exercise. In Manual of Vibration Exercise and Vibration Therapy; Springer: Cham, Switzerland, 2020; pp. 143–153. [Google Scholar]
- Pessoa, M.F.; Brandão, D.C.; Sá, R.B.; Barcelar, J.D.; Rocha, T.D.; Souza, H.C.; Dornelas de Andrade, A. Vibrating platform training improves respiratory muscle strength, quality of life, and inspiratory capacity in the elderly adults: A randomized controlled trial. J. Gerontol. Ser. A: Biomed. Sci. Med. Sci. 2017, 72, 683–688. [Google Scholar] [CrossRef] [Green Version]
- ISO 2631-1; Mechanical Vibration and Shock—Evaluation of Human Exposure to Whole Body Vibration. Part 1 General Requirements; International Standards Organization: Geneva, Switzerland, 1997.
- Quesada, J.I. (Ed.) Application of Infrared Thermography in Sports Science; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Ammer, K. The Glamorgan Protocol for recording and evaluation of thermal images of the human body. Thermol. Int. 2008, 18, 125–144. [Google Scholar]
- de Oliveira Guirro, E.C.; de Jesus Guirro, R.R.; Dibai-Filho, A.V.; Pascote, S.C.; Rodrigues-Bigaton, D. Immediate effects of electrical stimulation, diathermy, and physical exercise on lower limb arterial blood flow in diabetic women with peripheral arterial disease: A randomized crossover trial. J. Manip. Physiol. Ther. 2015, 38, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [PubMed]
- Guia do Usuário do BTS Smart Capture; BTS Bioengineering: Milão, Italy, 2006.
- Davis, R.B.; Ounpuu, S.; Tyburski, D.; Gage, J.R. A gait analysis data collection and reduction technique. Hum. Mov. Sci. 1991, 10, 575–587. [Google Scholar] [CrossRef]
- Neto, H.P.; Grecco, L.A.; Ferreira, L.A.; Christovão, T.C.; Duarte, N.D.; Oliveira, C.S. Clinical analysis and baropodometric evaluation in diagnosis of abnormal foot posture: A clinical trial. J. Bodyw. Mov. Ther. 2015, 19, 429–433. [Google Scholar] [CrossRef]
- Malachias, M.V.; Souza, W.K.; Plavnik, F.L.; Rodrigues, C.I.; Brandão, A.A.; Neves, M.F. Brazilian Society of Cardiology. VII Brazilian Guidelines on Hypertension. Arq. Bras. Cardiol. 2016, 107 (Suppl. 3), 1–83. [Google Scholar]
- Lough, M.E. Hemodynamic Monitoring-E-Book: Evolving Technologies and Clinical Practice; Elsevier Health Sciences: Amsterdam, The Netherlands, 2015. [Google Scholar]
- ISO 15197:2003; In Vitro Diagnostic Test Systems–Requirements for Blood-Glucose Monitoring Systems for Self-Testing in Managing Diabetes Mellitus; International Organization for Standardization: Geneva, Switzerland, 2013.
- Wei, N.; Ng, S.S.; Ng, G.Y.; Lee, R.S.; Lau, M.C.; Pang, M.Y. Whole-body vibration training improves muscle and physical performance in community dwelling with sarcopenia: A randomized controlled trial. Int. J. Phys. Ther. Rehabil. 2016, 2016, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Zhao, G.; Ford, E.S.; Li, C.; Balluz, L.S. Physical activity in US older adults with diabetes mellitus: Prevalence and correlates of meeting physical activity recommendations. J. Am. Geriatr. Soc. 2011, 59, 132–137. [Google Scholar] [CrossRef]
- Sharma-Ghimire, P.; Chen, Z.; Sherk, V.; Bemben, M.; Bemben, D. Sclerostin and parathyroid hormone responses to acute whole-body vibration and resistance exercise in young women. J. Bone Miner. Metab. 2019, 37, 358–367. [Google Scholar] [CrossRef]
- Astasio-Picado, A.; Martínez, E.E.; Nova, A.M.; Rodríguez, R.S.; Gómez–Martín, B. Thermal map of the diabetic foot using infrared thermography. Infrared Phys. Technol. 2018, 93, 59–62. [Google Scholar] [CrossRef]
- Bonnin, P.; Fressonnet, R. Notions d’hémodynamique et techniques ultrasonores pour l’exploration des artères. J. Radiol. 2005, 86, 615–627. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Set A | Set B |
|---|---|
 Prone Plank Muscles Worked: Abdominal rectum, external oblique, serratus anterior, pectoralis major, tensor fascia lata, quadriceps. |  Prone Plank Muscles Worked: Abdominal rectum, external oblique, serratus anterior, pectoralis major, tensor fascia lata, quadriceps. |
 Seated Low Row Muscles Worked: Trapezius, latissimus dorsi, rhomboids, posterior deltoid. |  Dumbbell Shoulder Press Muscles Worked: Anterior deltoid, lateral deltoid, triceps, trapezius, upper chest. |
 Lat Pulldown Machines Muscles Worked: Latissimus dorsum, posterior deltoid, lower trapezius, rhomboids. |  Chest Fly Machine Muscles Worked: Pectoralis major, anterior deltoid. |
 Upright Cable Row Muscles Worked: Lateral deltoid, trapezius, anterior deltoid, supraspinatus, infraspinatus, minor round. |  Triceps Pushdown Muscles Worked: Triceps, deltoid, forearm. |
 Standing Bicep Curl (Cable) Muscles Worked: Biceps, brachialis, brachioradialis, anterior deltoid, forearm. |  Cable Hip Abduction Muscles Worked: Gluteus maximus, gluteus minimus, tensor fascia lata. |
 Standing Leg Curl Muscles Worked: Isquiotibiales, gluteos, sural triceps. |  Cable Hip Adduction Muscles Worked: Long adductor, short adductor, magnum, gracilis, pectinous. |
 Leg Extension Muscles Worked: Quadriceps, anterior tibialis. |  Standing Calf Raise Muscles Worked: Sural Triceps. |
| Weeks | Time per Exercise (s)/Number of WBV Exercise | Frequency (Hz) | Rest Period (s) | WBV Total Time (s) |
|---|---|---|---|---|
| 1–2 | 30/8 | 16 | 30 | 480 |
| 3–4 | 30/8 | 18 | 30 | 480 |
| 5–6 | 45/8 | 20 | 30 | 720 |
| 7–8 | 45/8 | 22 | 30 | 720 |
| 9–10 | 60/8 | 24 | 30 | 960 |
| 11–12 | 60/8 | 26 | 30 | 960 |
 | ROI: Anterior thigh region.
|
 | ROI: Posterior thigh region.
|
 | ROI: Anterior leg region.
|
 | ROI: Posterior leg region.
|
 | ROI: Dorsal foot region.
|
 | ROI: Plantar foot region.
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, F.T.M.; Ferreira, A.P.d.L.; Alves, K.F.P.; Marques, T.V.; de Lima, D.F.; de Lucena, L.C.; Campos, S.L.; Leite, W.S.; Guerra, R.O.; Rapin, A.; et al. Whole-Body Vibration Associated with Strength Training on the Lower-Limb Blood Flow and Mobility in Older Adults with Type 2 Diabetes: A Study Protocol for a Randomized Controlled Trial. Diagnostics 2022, 12, 1550. https://doi.org/10.3390/diagnostics12071550
Rodrigues FTM, Ferreira APdL, Alves KFP, Marques TV, de Lima DF, de Lucena LC, Campos SL, Leite WS, Guerra RO, Rapin A, et al. Whole-Body Vibration Associated with Strength Training on the Lower-Limb Blood Flow and Mobility in Older Adults with Type 2 Diabetes: A Study Protocol for a Randomized Controlled Trial. Diagnostics. 2022; 12(7):1550. https://doi.org/10.3390/diagnostics12071550
Chicago/Turabian StyleRodrigues, François Talles Medeiros, Ana Paula de Lima Ferreira, Kennedy Freitas Pereira Alves, Thais Vitorino Marques, Daniel Florentino de Lima, Larissa Coutinho de Lucena, Shirley Lima Campos, Wagner Souza Leite, Ricardo Oliveira Guerra, Amandine Rapin, and et al. 2022. "Whole-Body Vibration Associated with Strength Training on the Lower-Limb Blood Flow and Mobility in Older Adults with Type 2 Diabetes: A Study Protocol for a Randomized Controlled Trial" Diagnostics 12, no. 7: 1550. https://doi.org/10.3390/diagnostics12071550