Peripheral Biomarkers in DSM-5 Anxiety Disorders: An Updated Overview

 , , , and
, , , and
Abstract
:1. Introduction
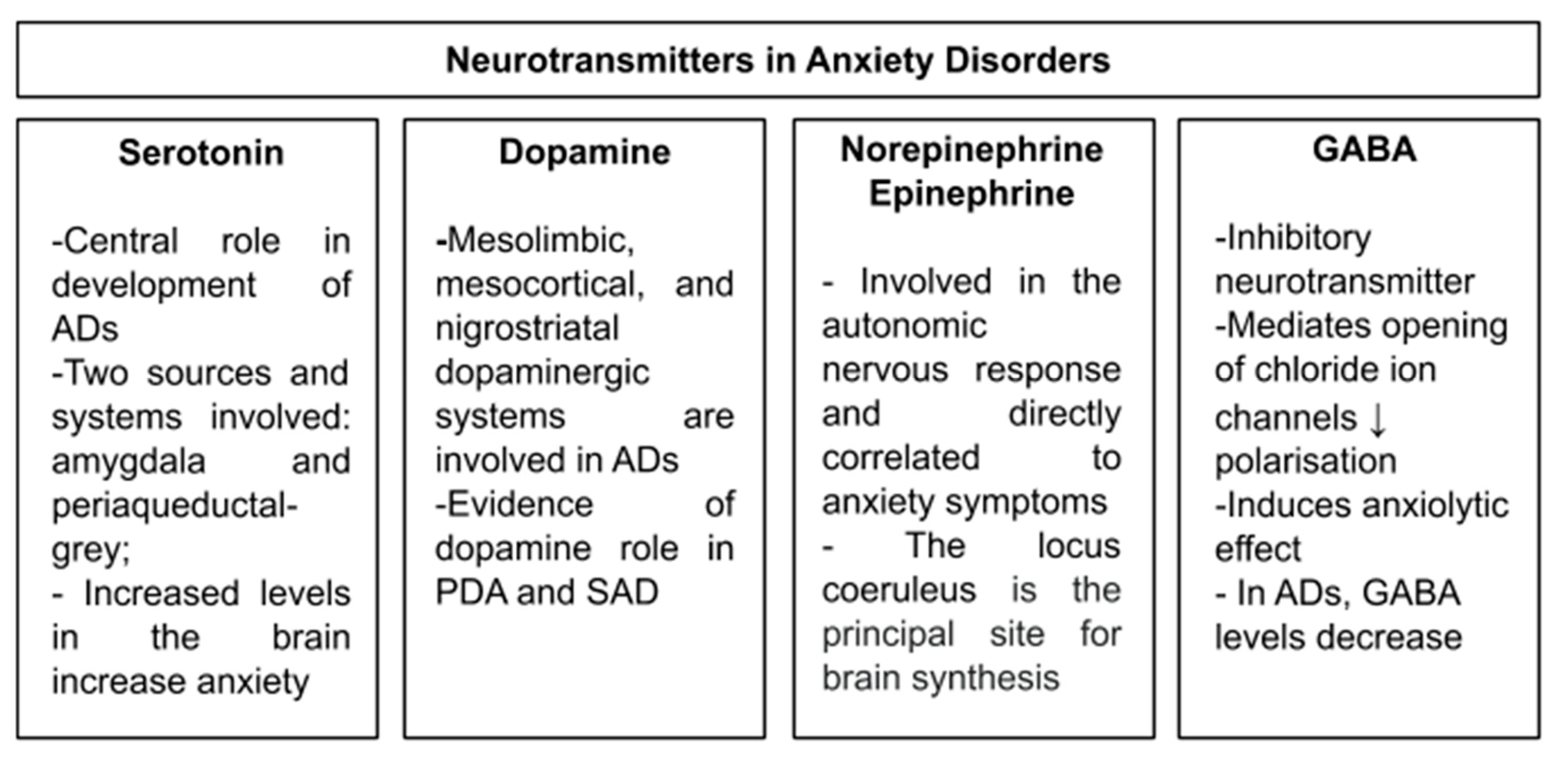
2. Neurotransmitters
2.1. General Anxiety Disorders
2.2. Panic Disorders with or without Agoraphobia
2.3. Social Anxiety Disorder
3. Neuropeptides
3.1. General Anxiety Disorders
3.2. Panic Disorders with or without Agoraphobia
3.3. Social Anxiety Disorder
4. Hypothalamic–Pituitary–Adrenal Axis
4.1. General Anxiety Disorders
4.2. Panic Disorders with or without Agoraphobia
4.3. Social Anxiety Disorder
5. Neurotrophic Factors
5.1. General Anxiety Disorders
5.2. Panic Disorders with or without Agoraphobia
5.3. Social Anxiety Disorder
6. Inflammation and immune system
6.1. General Anxiety Disorders
6.2. Panic Disorders with or without Agoraphobia
6.3. Social Anxiety Disorder
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baxter, A.J.; Scott, K.M.; Vos, T.; Whiteford, H.A. Global prevalence of anxiety disorders: A systematic review and meta-regression. Psychol. Med. 2013, 43, 897–910. [Google Scholar] [CrossRef] [PubMed]
- Bandelow, B.; Baldwin, D.; Abelli, M.; Bolea-Alamanac, B.; Bourin, M.; Chamberlain, S.R.; Cinosi, E.; Davies, S.J.; Domschke, K.; Fineberg, N.; et al. Biological markers for anxiety disorders, OCD and PTSD: A consensus statement. Part II: Neurochemistry, neurophysiology and neurocognition. World J. Biol. Psychiatry 2017, 18, 162–214. [Google Scholar] [CrossRef] [PubMed]
- Serretti, A.; Chiesa, A.; Calati, R.; Perna, G.; Bellodi, L.; Ronchi, D.D. Common genetic, clinical, demographic and psychosocial predictors of response to pharmacotherapy in mood and anxiety disorders. Int. Clin. Psychopharmacol. 2009, 24, 1–18. [Google Scholar] [CrossRef]
- Maron, E.; Nutt, D. Biological predictors of pharmacological therapy in anxiety disorders. Dialog. Clin. Neurosci. 2015, 17, 305–317. [Google Scholar]
- Dell’Osso, B.; Mundo, E.; Marazziti, D.; Altamura, A.C. Switching from serotonin reuptake inhibitors to duloxetine in patients with resistant obsessive compulsive disorder: A case series. J. Psychopharmacol. 2008, 22, 210–213. [Google Scholar] [CrossRef]
- Dell’Osso, B.; Buoli, M.; Baldwin, D.S.; Altamura, A.C. Serotonin norepinephrine reuptake inhibitors (SNRIs) in anxiety disorders: A comprehensive review of their clinical efficacy. Hum. Psychopharmacol. Clin. Exp. 2010, 25, 17–29. [Google Scholar] [CrossRef]
- Niculescu, A.B.; Levey, D.F.; Le-Niculescu, H.; Niculescu, E.; Kurian, S.M.; Salomon, D. Psychiatric blood biomarkers: Avoiding jumping to premature negative or positive conclusions. Mol. Psychiatry 2015, 20, 286–288. [Google Scholar] [CrossRef] [Green Version]
- Quevedo, J.; Yatham, L.N. Biomarkers in mood disorders: Are we there yet? J. Affect. Disord. 2018, 233, 1–2. [Google Scholar] [CrossRef]
- Massaro, A.R.; Scivoletto, G.; Tonali, P. Cerebrospinal fluid markers in neurological disorders. Ital. J. Neurol. Sci. 1990, 11, 537–547. [Google Scholar] [CrossRef]
- Orlovska-Waast, S.; Köhler-Forsberg, O.; Brix, S.W.; Nordentoft, M.; Kondziella, D.; Krogh, J.; Benros, M.E. Correction: Cerebrospinal fluid markers of inflammation and infections in schizophrenia and affective disorders: A systematic review and meta-analysis. Mol. Psychiatry 2019, 24, 929–934. [Google Scholar] [CrossRef] [Green Version]
- Faravelli, C.; Sauro, C.L.; Godini, L.; Lelli, L.; Benni, L.; Pietrini, F.; Lazzeretti, L.; Talamba, G.A.; Fioravanti, G.; Ricca, V. Childhood stressful events, HPA axis and anxiety disorders. World J. Psychiatry 2012, 2, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Stein, M.; Keller, S.E.; Schleifer, S.J. Immune system. Relationship to anxiety disorders. Psychiatr. Clin. N. Am. 1988, 11, 349–360. [Google Scholar] [CrossRef]
- Heninger, G.R.; Charney, D.S. Monoamine Receptor Systems and Anxiety Disorders. Psychiatr. Clin. N. Am. 1988, 11, 309–326. [Google Scholar] [CrossRef]
- Dell’Osso, B.; Palazzo, M.; Oldani, L.; Altamura, A.C. The Noradrenergic Action in Antidepressant Treatments: Pharmacological and Clinical Aspects. CNS Neurosci. Ther. 2010, 17, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Gray, J.; McNaughton, N. The Neuropsychology of Anxiety: An Enquiry into the Functions of Septo-Hippocampal System; Oxford University Press: Oxford, UK, 2000. [Google Scholar]
- McNaughton, N.; Corr, P.J. A two-dimensional neuropsychology of defense: Fear/anxiety and defensive distance. Neurosci. Biobehav. Rev. 2004, 28, 285–305. [Google Scholar] [CrossRef]
- Pletscher, A.; Affolter, H. The 5-hydroxytryptamine receptor of blood platelets. J. Neural Transm. 1983, 57, 233–242. [Google Scholar] [CrossRef]
- Domschke, K.; Zwanzger, P. GABAergic and Endocannabinoid Dysfunction in Anxiety—Future Therapeutic Targets? Curr. Pharm. Des. 2008, 14, 3508–3517. [Google Scholar] [CrossRef] [PubMed]
- Olson, R. GABA. In Neuropsychopharmacology The Fifth Generation of Progress: An Official Publication of the American College of Neuropsychopharmacology; Davis, D.K.L., Charney, J.T., Coyle, C.N., Eds.; Lippincott, Williams and Wilkins: Philadelphia, PA, USA, 2002; pp. 150–168. [Google Scholar]
- Papadopoulos, V.; Baraldi, M.; Guilarte, T.R.; Knudsen, T.B.; Lacapere, J.-J.; Lindemann, P.; Norenberg, M.D.; Nutt, D.J.; Weizman, A.; Zhang, M.-R.; et al. Translocator protein (18 kDa): New nomenclature for the peripheral-type benzodiazepine receptor based on its structure and molecular function. Trends Pharmacol. Sci. 2006, 27, 402–409. [Google Scholar] [CrossRef]
- Farb, D.H.; Ratner, M.H. Targeting the Modulation of Neural Circuitry for the Treatment of Anxiety Disorders. Pharmacol. Rev. 2014, 66, 1002–1032. [Google Scholar] [CrossRef] [Green Version]
- Iny, L.J.; Pecknold, J.; Suranyi-Cadotte, B.E.; Bernier, B.; Luthe, L.; Nair, N.P.V.; Meaney, M.J. Studies of a neurochemical link between depression, anxiety, and stress from [3H]imipramine and [3H]paroxetine binding on human platelets. Biol. Psychiatry 1994, 36, 251–291. [Google Scholar] [CrossRef]
- Schneider, L.S.; Munjack, D.; Severson, J.A.; Palmer, R. Platelet [3H]Imipramine binding in generalized anxiety disorder, panic disorder, and agoraphobia with panic attacks. Biol. Psychiatry 1987, 22, 59–66. [Google Scholar] [CrossRef]
- Hernández, E.; Lastra, S.; Urbina, M.; Carreira, I.; Lima, L. Serotonin, 5-hydroxyindoleacetic acid and serotonin transporter in blood peripheral lymphocytes of patients with generalized anxiety disorder. Int. Immunopharmacol. 2002, 2, 893–900. [Google Scholar] [CrossRef]
- Sevy, S.; Papadimitriou, G.N.; Surmont, D.W.; Goldman, S.; Mendiewicz, J. Noradrenergic function in generalized anxiety disorder, major depressive disorder, and healthy subjects. Biol. Psychiatry 1989, 25, 141–152. [Google Scholar] [CrossRef]
- Cameron, O.G.; Smith, C.B.; Lee, M.A.; Hollingsworth, P.J.; Hill, E.M.; Curtis, G.C. Adrenergic status in anxiety disorders: Platelet alpha2-adrenergic receptor binding, blood pressure, pulse, and plasma catecholamines in panic and generalized anxiety disorders patients and in normal subjects. Biol. Psychiatry 1990, 28, 3–20. [Google Scholar] [CrossRef] [Green Version]
- Weizman, R.; Tanne, Z.; Granek, M.; Karp, L.; Golomb, M.; Tyano, S.; Gavish, M. Peripheral benzodiazepine binding sites on platelet membranes are increased during diazepam treatment of anxious patients. Eur. J. Pharmacol. 1987, 138, 289–292. [Google Scholar] [CrossRef]
- Ferrarese, C.; Appollonio, I.; Frigo, M.; Perego, M.; Piolti, R.; Trabucchi, M.; Frattola, L. Decreased density of benzodiazepine receptors in lymphocytes of anxious patients: Reversal after chronic diazepam treatment. Acta Psychiatr. Scand. 1990, 82, 169–173. [Google Scholar] [CrossRef]
- Rocca, P.; Beoni, A.M.; Eva, C.; Ferrero, P.; Zanalda, E.; Ravizza, L. Peripheral benzodiazepine receptor messenger RNA is decreased in lymphocytes of generalized anxiety disorder patients. Biol. Psychiatry 1998, 43, 767–773. [Google Scholar] [CrossRef]
- Evans, L.; Schneider, P.; Ross-Lee, L.; Wiltshire, B.; Eadie, M.; Kenardy, J.; Hoey, H. Plasma serotonin levels in agoraphobia. Am. J. Psychiatry 1985, 142, 267. [Google Scholar] [CrossRef] [PubMed]
- Shutov, A.A.; Bystrova, O.V. Serum-blood Serotonin Level as a Marker of Panic Attacks Severity and Effectiveness of Their Treatment. Zh Nevrol Psikhiatr Im S S Korsakova 2008, 108, 49–54. [Google Scholar]
- Balon, R.; Pohl, R.; Yeragani, V.; Rainey, J.; Oxenkrug, G.F. Platelet serotonin levels in panic disorder. Acta Psychiatr. Scand. 1987, 75, 315–317. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, I.M.; Judd, F.K.; Burrows, G.D.; Norman, T.R. Serotonin in Panic Disorder: Platelet uptake and concentration. Int. Clin. Psychopharmacol. 1989, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Butler, J.; O’Halloran, A.; Leonard, B.E. The galway study of panic disorder II: Changes in some peripheral markers of noradrenergic and serotonergic function in DSM III-R panic disorder. J. Affect. Disord. 1992, 26, 89–99. [Google Scholar] [CrossRef]
- Lewis, D.A.; Noyes, R.; Coryell, W.; Clancy, J. Tritiated imipramine binding to platelets is decreased in patients with agoraphobia. Psychiatry Res. 1985, 16, 1–9. [Google Scholar] [CrossRef]
- Pecknold, J.C.; Suranyi-Cadotte, B.; Chang, H.; Nair, N.P.V. Serotonin uptake in panic disorder and agoraphobia. Neuropsychopharmacology 1988, 1, 173–176. [Google Scholar] [CrossRef]
- Innis, R.B.; Charney, D.S.; Heninger, G.R. Differential 3H-imipramine platelet binding in patients with panic disorder and depression. Psychiatry Res. 1987, 21, 33–41. [Google Scholar] [CrossRef]
- Nutt, D.J.; Fraser, S. Platelet binding studies in panic disorder. J. Affect. Disord. 1987, 12, 7–11. [Google Scholar] [CrossRef]
- Pecknold, J.C.; Chang, H.; Fleury, D.; Koszychi, D.; Quirion, R.; Nair, N.P.V.; Suranyi-Cadotte, B.E. Platelet imipramine binding in patients with panic disorder and major familial depression. J. Psychiatr. Res. 1987, 21, 319–326. [Google Scholar] [CrossRef]
- Uhde, T.W.; Berrettini, W.H.; Roy-Byrne, P.P.; Boulenger, J.-P.; Post, R.M. Platelet [3H]imipramine binding in patients with panic disorder. Biol. Psychiatry 1987, 22, 52–58. [Google Scholar] [CrossRef]
- Norman, T.R.; Sartor, D.M.; Judd, F.K.; Burrows, G.D.; Gregory, M.S.; McIntyre, I.M. Platelet serotonin uptake and 3H-imipramine binding in panic disorder. J. Affect. Disord. 1989, 17, 77–81. [Google Scholar] [CrossRef]
- Norman, T.R.; Judd, F.K.; Burrows, G.D.; McIntyre, I.M. Platelet serotonin uptake in panic disorder patients: A replication study. Psychiatry Res. 1989, 30, 63–68. [Google Scholar] [CrossRef]
- Norman, T.R.; Judd, F.K.; Gregory, M.; James, R.H.; Kimber, N.M.; McIntyre, I.M.; Burrows, G.D. Platelet serotonin uptake in panic disorder. J. Affect. Disord. 1986, 11, 69–72. [Google Scholar] [CrossRef]
- Eriksson, E.; Westberg, P.; Alling, C.; Thuresson, K.; Modigh, K. Cerebrospinal fluid levels of monoamine metabolites in panic disorder. Psychiatry Res. 1991, 36, 243–251. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Oquendo, M.A.; Huang, Y.-Y.; Mann, J.J. Elevated cerebrospinal fluid 5-hydroxyindoleacetic acid levels in women with comorbid depression and panic disorder. Int. J. Neuropsychopharmacol. 2006, 9, 547–556. [Google Scholar] [CrossRef] [Green Version]
- Esler, M.; Alvarenga, M.; Lambert, G.; Kaye, D.; Hastings, J.; Jennings, G.L.; Morris, M.J.; Schwarz, R.; Richards, J. Cardiac sympathetic nerve biology and brain monoamine turnover in panic disorder. Ann. N. Y. Acad. Sci. 2004, 1018, 505–514. [Google Scholar] [CrossRef]
- Coplan, J.D.; Tamir, H.; Calaprice, D.; Dejesus, M.; Nuez, M.D.L.; Pine, D.; Papp, L.A.; Klein, D.F.; Gorman, J.M. Plasma anti-serotonin and serotonin anti-idiotypic antibodies are elevated in panic disorder. Neuropsychopharmacology 1999, 20, 386–391. [Google Scholar] [CrossRef] [Green Version]
- Oh, J.Y.; Yu, B.H.; Heo, J.Y.; Yoo, I.; Song, H.; Jeon, H.J. Plasma catecholamine levels before and after paroxetine treatment in patients with panic disorder. Psychiatry Res. 2015, 225, 471–475. [Google Scholar] [CrossRef]
- Pitchot, W.; Ansseau, M.; Moreno, A.G.; Hansenne, M.; Frenckell, v.R. Dopaminergic function in panic disorder: Comparison with major and minor depression. Biol. Psychiatry 1992, 32, 1004–1011. [Google Scholar] [CrossRef]
- Cameron, O.G.; Smith, C.B.; Nesse, R.M.; Hill, E.M.; Hollingsworth, P.J.; Abelson, J.A.; Hariharan, M.; Curtis, G.C. Platelet alpha2-adrenoreceptors, catecholamines, hemodynamic variables, and anxiety in panic patients and their asymptomatic relatives. Psychosom. Med. 1996, 58, 289–301. [Google Scholar] [CrossRef] [Green Version]
- Gurguis, G.N.M.; Blakeley, J.E.; Antai-Otong, D.; Vo, S.P.; Orsulak, P.J.; Petty, F.; Rush, A.J. Adrenergic receptor function in panic disorder II. Neutrophil β2 receptors: Gs protein coupling, effects of imipramine treatment and relationship to treatment outcome. J. Psychiatr. Res. 1999, 33, 309–321. [Google Scholar] [CrossRef]
- George, D.T.; Adinoff, B.; Ravitz, B.; Nutt, D.J.; Jong, J.D.; Berrettini, W.; Mefford, I.N.; Costa, E.; Linnoila, M. A cerebrospinal fluid study of the pathophysiology of panic disorder associated with alcoholism. Acta Psychiatr. Scand. 1990, 82, 1–7. [Google Scholar] [CrossRef]
- Nutt, D.J.; Glue, P.; Lawson, C.; Wilson, S. Flumazenil Provocation of Panic Attacks: Evidence for Altered Benzodiazepine Receptor Sensitivity in Panic Disorder. Arch. Gen. Psychiatry 1990, 47, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Ströhle, A.; Romeo, E.; Michele, F.D.; Pasini, A.; Yassouridis, A.; Holsboer, F.; Rupprecht, R. GABAA receptor-modulating neuroactive steroid composition in patients with panic disorder before and during paroxetine treatment. Am. J. Psychiatry 2002, 159, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Ströhle, A.; Romeo, E.; Michele, F.D.; Pasini, A.; Hermann, B.; Gajewsky, G.; Holsboer, F.; Rupprecht, R. Induced panic attacks shift γ-aminobutyric acid type A receptor modulatory neuroactive steroid composition in patients with panic disorder: Preliminary results. Arch. Gen. Psychiatry 2003, 60, 161–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marazziti, D.; Rotondo, A.; Martini, C.; Giannaccini, G.; Lucacchini, A.; Pancioli-Guadagnucci, M.L.; Diamond, B.I.; Borison, R.; Cassano, G.B. Changes in peripheral benzodiazepine receptors in patients with panic disorder and obsessive-compulsive disorder. Neuropsychobiology 1994, 29, 8–11. [Google Scholar] [CrossRef]
- Chatterjee, S.; Sunitha, T.A.; Velayudhan, A.; Khanna, S. An investigation into the psychobiology of social phobia: Personality domains and serotonergic function. Acta Psychiatr. Scand. 1997, 95, 544–550. [Google Scholar] [CrossRef]
- Hollander, E.; Kwon, J.; Weiller, F.; Cohen, L.; Stein, D.J.; DeCaria, C.; Liebowitz, M.; Simeon, D. Serotonergic function in social phobia: Comparison to normal control and obsessive-compulsive disorder subjects. Psychiatry Res. 1998, 79, 213–217. [Google Scholar] [CrossRef]
- Tancer, M.E.; Mailman, R.B.; Stein, M.B.; Mason, G.A.; Carson, S.W.; Golden, R.N. Neuroendocrine Responsivity to Monoaminergic System Probes in Generalized Social Phobia. Anxiety 1994, 1, 216–223. [Google Scholar]
- Hood, S.D.; Potokar, J.P.; Davies, S.J.C.; Hince, D.A.; Morris, K.; Seddon, K.M.; Nutt, D.J.; Argyropoulos, S.V.; Hood, S. Dopaminergic challenges in social anxiety disorder: Evidence for dopamine D3 desensitisation following successful treatment with serotonergic antidepressants. J. Psychopharmacol. 2010, 24, 709–716. [Google Scholar] [CrossRef]
- Corchs, F.; Nutt, D.J.; Hince, D.A.; Davies, S.J.C.; Bernik, M.; Hood, S.D. Evidence for serotonin function as a neurochemical difference between fear and anxiety disorders in humans? J. Psychopharmacol. 2015, 29, 1061–1069. [Google Scholar] [CrossRef]
- Boulenger, J.P.; Uhde, T.W. Biological peripheral correlates of anxiety. L’Encéphale 1982, 8, 119–130. [Google Scholar] [PubMed]
- Anthony, J.C.; Tien, A.Y.; Petronis, K.R. Epidemiologic evidence on cocaine use and panic attacks. Am. J. Epidemiol. 1989, 129, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.S.; Kim, K.J.; Kang, E.H.; Yu, B.H. β-adrenoceptor affinity as a biological predictor of treatment response to paroxetine in patients with acute panic disorder. J. Affect. Disord. 2008, 110, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Charney, D.S.; Heninger, G.R.; Redmond, D.E. Yohimbine induced anxiety and increased noradrenergic function in humans: Effects of diazepam and clonidine. Life Sci. 1983, 33, 19–29. [Google Scholar] [CrossRef]
- Nutt, D.J.; Glue, P. Imipramine in panic disorder. 1. Clinical response and pharmacological changes. J. Psychopharmacol. 1991, 5, 56–64. [Google Scholar] [CrossRef]
- Figari, W.J.A.; Herrmann, S.; Akogyeram, C.; Qian, Q. New onset hypertension following abrupt discontinuation of citalopram. Clin. Nephrol. 2014, 82, 202–204. [Google Scholar] [CrossRef]
- Ströhle, A.; Kellner, M.; Holsboer, F.; Wiedemann, K. Behavioral, neuroendocrine, and cardiovascular response to flumazenil: No evidence for an altered benzodiazepine receptor sensitivity in panic disorder. Biol. Psychiatry 1999, 45, 321–326. [Google Scholar] [CrossRef]
- Rupprecht, R. Neuroactive steroids: Mechanisms of action and neuropsychopharmacological properties. Psychoneuroendocrinology 2003, 28, 139–168. [Google Scholar] [CrossRef]
- Rupprecht, R.; Holsboer, F. Neuroactive steroids: Mechanisms of action and neuropsychopharmacological perspectives. Trends Neurosci. 1999, 22, 410–416. [Google Scholar] [CrossRef]
- Rupprecht, R.; Rammes, G.P.; Eser, D.; Baghai, T.C.; Schüle, C.; Nothdurfter, C.; Troxler, T.; Gentsch, C.; Kalkman, H.O.; Chaperon, F.; et al. Translocator Protein (18 kD) as Target for Anxiolytics Without Benzodiazepine-Like Side Effects. Science 2009, 325, 490–493. [Google Scholar] [CrossRef] [Green Version]
- Surget, A.; Leman, S.; Griebel, G.; Belzung, C.; Yalcin, I. Neuropeptides in Psychiatric Diseases: An Overview with a Particular Focus on Depression and Anxiety Disorders. CNS Neurol. Disord. Drug Targets 2008, 5, 135–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burbach, J.P.H. What are neuropeptides? Methods Mol. Biol. 2011, 789, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Megen, v.H.J.G.M.; Boer, d.J.A.; Westenberg, H.G.M. Neuropeptiden en angststoornissen. Acta Neuropsychiatr. 1992, 4, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.E.-J. Neuropeptides as Therapeutic Targets in Anxiety Disorders. Curr. Pharm. Des. 2012, 18, 5709–5727. [Google Scholar] [CrossRef]
- Lydiard, R. Neuropeptides and Anxiety: Focus on Cholecystokinin. Clin. Chem. 1994, 40, 315–318. [Google Scholar] [CrossRef]
- Bradwejn, J.; Tertre, d.A.C.; Palmour, R.; Ervin, F.; Bourin, M. The cholecystokinin hypothesis of panic and anxiety disorders: A review. J. Psychopharmacol. 1992, 6, 345–351. [Google Scholar] [CrossRef]
- Li, H.; Ohta, H.; Izumi, H.; Matsuda, Y.; Seki, M.; Toda, T.; Akiyama, M.; Matsushima, Y.; Goto, Y.I.; Kaga, M.; et al. Behavioral and cortical EEG evaluations confirm the roles of both CCKA and CCKB receptors in mouse CCK-induced anxiety. Behav. Brain Res. 2013, 237, 325–332. [Google Scholar] [CrossRef]
- Gottschalk, M.G.; Domschke, K. Oxytocin and Anxiety Disorders. In Current Topics in Behavioral Neurosciences; Springer: Singapore, 2018; Volume 35, pp. 467–498. [Google Scholar]
- Neumann, I.D.; Slattery, D.A. Oxytocin in General Anxiety and Social Fear: A Translational Approach. Biol. Psychiatry 2016, 79, 213–221. [Google Scholar] [CrossRef] [Green Version]
- Carson, D.S.; Berquist, S.W.; Trujillo, T.H.; Garner, J.P.; Hannah, S.L.; Hyde, S.A.; Sumiyoshi, R.D.; Jackson, L.P.; Moss, J.K.; Strehlow, M.C.; et al. Cerebrospinal fluid and plasma oxytocin concentrations are positively correlated and negatively predict anxiety in children. Mol. Psychiatry 2015, 20, 1085–1090. [Google Scholar] [CrossRef] [Green Version]
- Weisman, O.; Zagoory-Sharon, O.; Schneiderman, I.; Gordon, I.; Feldman, R. Plasma oxytocin distributions in a large cohort of women and men and their gender-specific associations with anxiety. Psychoneuroendocrinology 2013, 38, 694–701. [Google Scholar] [CrossRef]
- Iftikhar, K.; Siddiq, A.; Baig, S.G.; Zehra, S. Substance P: A neuropeptide involved in the psychopathology of anxiety disorders. Neuropeptides 2020, 79, 101993. [Google Scholar] [CrossRef] [PubMed]
- Ressler, K.J.; Mercer, K.B.; Bradley, B.; Jovanovic, T.; Mahan, A.; Kerley, K.; Norrholm, S.D.; Kilaru, V.; Smith, A.K.; Myers, A.J.; et al. Post-traumatic stress disorder is associated with PACAP and the PAC1 receptor. Nature 2011, 470, 492–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, R.A.; Hoeppner, S.S.; Hellberg, S.N.; O’Day, E.B.; Rosencrans, P.L.; Ressler, K.J.; May, V.; Simon, N.M. Circulating PACAP peptide and PAC1R genotype as possible transdiagnostic biomarkers for anxiety disorders in women: A preliminary study. Neuropsychopharmacology 2020, 45, 1125–1133. [Google Scholar] [CrossRef] [PubMed]
- Chuang, J.-C.; Zigman, J.M. Ghrelin’s Roles in Stress, Mood, and Anxiety Regulation. Int. J. Pept. 2010, 2010, 460549. [Google Scholar]
- Oomura, Y.; Hori, N.; Shiraishi, T.; Fukunaga, K.; Takeda, H.; Tsuji, M.; Matsumiya, T.; Ishibashi, M.; Aou, S.; Li, X.L.; et al. Leptin facilitates learning and memory performance and enhances hippocampal CA1 long-term potentiation and CaMK II phosphorylation in rats. Peptides 2006, 27, 2738–2749. [Google Scholar] [CrossRef]
- Jetty, P.V.; Charney, D.S.; Goddard, A.W. Neurobiology of Generalized Anxiety Disorder. Psychiatr. Clin. N. Am. 2001, 24, 75–97. [Google Scholar] [CrossRef]
- Boccia, M.L.; Petrusz, P.; Suzuki, K.; Marson, L.; Pedersen, C.A. Immunohistochemical localization of oxytocin receptors in human brain. Neuroscience 2013, 253, 155–164. [Google Scholar] [CrossRef]
- Viero, C.; Shibuya, I.; Kitamura, N.; Verkhratsky, A.; Fujihara, H.; Katoh, A.; Ueta, Y.; Zingg, H.H.; Chvatal, A.; Syková, E.; et al. Oxytocin: Crossing the Bridge between Basic Science and Pharmacotherapy. CNS Neurosci. Ther. 2010, 16, e138–e156. [Google Scholar] [CrossRef] [Green Version]
- Yoon, S.; Kim, Y.-K. The Role of the Oxytocin System in Anxiety Disorders. In Advances in Experimental Medicine and Biology; Springer: Singapore, 2020; Volume 1191, pp. 103–120. [Google Scholar]
- Myers, A.J.; Williams, L.; Gatt, J.M.; McAuley-Clark, E.Z.; Dobson-Stone, C.; Schofield, P.R.; Nemeroff, C.B. Variation in the oxytocin receptor gene is associated with increased risk for anxiety, stress and depression in individuals with a history of exposure to early life stress. J. Psychiatr. Res. 2014, 59, 93–100. [Google Scholar] [CrossRef] [Green Version]
- Feifel, D.; MacDonald, K.; McKinney, R.; Heisserer, N.; Serrano, V. A randomized, placebo-controlled investigation of intranasal oxytocin in patients with anxiety | Request PDF. Neuropsychopharmacology 2011, 36, S324–S449. [Google Scholar]
- Currie, P.J.; Khelemsky, R.; Rigsbee, E.M.; Dono, L.M.; Coiro, C.D.; Chapman, C.D.; Hinchcliff, K. Ghrelin is an orexigenic peptide and elicits anxiety-like behaviors following administration into discrete regions of the hypothalamus. Behav. Brain Res. 2012, 226, 96–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spencer, S.J.; Xu, L.; Clarke, M.A.; Lemus, M.; Reichenbach, A.; Geenen, B.; Kozicz, T.; Andrews, Z.B. Ghrelin Regulates the Hypothalamic-Pituitary-Adrenal Axis and Restricts Anxiety After Acute Stress. Biol. Psychiatry 2012, 72, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Brawman-Mintzer, O.; Lydiard, R.B.; Bradwejn, J.; Villarreal, G.; Knapp, R.; Emmanuel, N.; Ware, M.R.; He, Q.; Ballenger, J.C. Effects of the cholecystokinin agonist pentagastrin in patients with generalized anxiety disorder. Am. J. Psychiatry 1997, 154, 700–702. [Google Scholar] [CrossRef] [PubMed]
- Ozmen, S.; Şeker, A.; Demirci, E. Ghrelin and leptin levels in children with anxiety disorders. J. Pediatr. Endocrinol. Metab. 2019, 32, 1043–1047. [Google Scholar] [CrossRef] [PubMed]
- Lydiard, R.B.; Ballenger, J.C.; Laraia, M.T.; Fossey, M.D.; Beinfeld, M.C. CSF cholecystokinin concentrations in patients with panic disorder and in normal comparison subjects. Am. J. Psychiatry 1992, 149, 691–693. [Google Scholar] [CrossRef]
- Brambilla, F.; Bellodi, L.; Perna, G.; Garberi, A.; Panerai, A.; Sacerdote, P. Lymphocyte cholecystokinin concentrations in panic disorder. Am. J. Psychiatry 1993, 150, 1111–1113. [Google Scholar] [CrossRef]
- Kim, K.; Jang, E.H.; Kim, A.Y.; Fava, M.; Mischoulon, D.; Papakostas, G.I.; Kim, H.; Na, E.J.; Yu, H.Y.; Jeon, H.J. Pre-treatment peripheral biomarkers associated with treatment response in panic symptoms in patients with major depressive disorder and panic disorder: A 12-week follow-up study. Compr. Psychiatry 2019, 95, 152140. [Google Scholar] [CrossRef]
- Masdrakis, V.G.; Papageorgiou, C.; Markianos, M. Associations of plasma leptin to clinical manifestations in reproductive aged female patients with panic disorder. Psychiatry Res. 2017, 255, 161–166. [Google Scholar] [CrossRef]
- Kellner, M.; Jahn, H.; Wiedemann, K. Natriuretic peptides and panic disorder: Therapeutic prospects. Expert Rev. Neurother. 2003, 3, 381–386. [Google Scholar] [CrossRef]
- Kellner, M.; Herzog, L.; Yassouridis, A.; Holsboer, F.; Wiedemann, K. Possible role of atrial natriuretic hormone in pituitary-adrenocortical unresponsiveness in lactate-induced panic. Am. J. Psychiatry 1995, 152, 1365–1367. [Google Scholar] [CrossRef]
- Unsal, C.; Hariri, A.G.; Yanartas, O.; Sevinc, E.; Atmaca, M.; Bilici, M. Low plasma adiponectin levels in panic disorder. J. Affect. Disord. 2012, 139, 302–305. [Google Scholar] [CrossRef] [PubMed]
- Hoge, E.A.; Lawson, E.A.; Metcalf, C.A.; Keshaviah, A.; Zak, P.J.; Pollack, M.H.; Simon, N.M. Plasma oxytocin immunoreactive products and response to trust in patients with social anxiety disorder. Depress. Anxiety 2012, 29, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Oh, K.S.; Kim, E.J.; Ha, J.W.; Woo, H.Y.; Kwon, M.J.; Shin, N.W.; Shin, Y.C.; Lim, S.W. The Relationship between Plasma Oxytocin Levels and Social Anxiety Symptoms. Psychiatry Investig. 2018, 15, 1079–1086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, L.; Field, M.J.; Hughes, J.; Menzies, R.; Oles, R.J.; Vass, C.A.; Woodruff, G.N. The behavioural properties of CI-988, a selective cholecystokininB receptor antagonist. Br. J. Pharmacol. 1991, 104, 239–245. [Google Scholar] [CrossRef] [Green Version]
- Dooley, D.J.; Klamt, I. Differential profile of the CCKB receptor antagonist CI-988 and diazepam in the four-plate test. Psychopharmacology 1993, 112, 452–454. [Google Scholar] [CrossRef]
- Josselyn, S.A.; Frankland, P.W.; Petrisano, S.; Bush, D.E.A.; Yeomans, J.S.; Vaccarino, F.J. The CCKB antagonist, L-365,260, attenuates fear-potentiated startle. Peptides 1995, 16, 1313–1315. [Google Scholar] [CrossRef]
- Bradwejn, J.; Koszycki, D.; Tertre, A.C.; Megen, v.H.; Boer, d.J.; Westenberg, H.; Annable, L. The Panicogenic Effects of Cholecystokinin-Tetrapeptide Are Antagonized by L-365, 260, a Central Cholecystokinin Receptor Antagonist, in Patients with Panic Disorder. Arch. Gen. Psychiatry 1994, 51, 486–493. [Google Scholar] [CrossRef]
- Belzung, C.; Pineau, N.; Beuzen, A.; Misslin, R. PD135158, a CCK-B antagonist, reduces “state,” but not “trait” anxiety in mice. Pharmacol. Biochem. Behav. 1994, 49, 433–436. [Google Scholar] [CrossRef]
- Goddard, A.W.; Woods, S.W.; Money, R.; Pande, A.C.; Charney, D.S.; Goodman, W.K.; Heninger, G.R.; Price, L.H. Effects of the CCKB antagonist CI-988 on responses to mCPP in generalized anxiety disorder. Psychiatry Res. 1999, 85, 225–240. [Google Scholar] [CrossRef]
- Adams, J.B.; Pyke, R.E.; Costa, J.; Cutler, N.R.; Schweizer, E.; Wilcox, C.S.; Wisselink, P.G.; Greiner, M.; Pierce, M.W.; Pande, A.C. A Double-Blind, Placebo-Controlled Study of a CCK-B Receptor Antagonist, CI-988, in Patients With Generalized Anxiety Disorder. J. Clin. Psychopharmacol. 1995, 15, 428–434. [Google Scholar] [CrossRef]
- Hughes, J.; Woodruff, G. Neuropeptides. Function and Clinical Applications. Arzneimittelforschung 1992, 42, 250–255. [Google Scholar] [PubMed]
- Vécsei, L.; Tuka, B.; Tajti, J. Role of PACAP in Migraine Headaches. Brain 2014, 137, 650–651. [Google Scholar] [CrossRef] [PubMed]
- Kinhult, J.; Andersson, J.A.; Uddman, R.; Stjärne, P.; Cardell, L.O. Pituitary adenylate cyclase-activating peptide 38 a potent endogenously produced dilator of human airways. Eur. Respir. J. 2000, 15, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, R.; Yatsuya, H.; Tamakoshi, K.; Matsushita, K.; Wada, K.; Toyoshima, H. Perceived Psychological Stress and Serum Leptin Concentrations in Japanese Men. Obesity 2006, 14, 1832–1838. [Google Scholar] [CrossRef]
- Bailey, J.E.; Kendrick, A.; Diaper, A.; Potokar, J.P.; Nutt, D.J. A validation of the 7.5% CO2 model of GAD using paroxetine and lorazepam in healthy volunteers. J. Psychopharmacol. 2007, 21, 42–49. [Google Scholar] [CrossRef]
- Oliveira, D.D.C.G.; Chagas, M.H.N.; Garcia, L.V.; Crippa, J.A.S.; Zuardi, A.W. Oxytocin interference in the effects induced by inhalation of 7.5% CO2 in healthy volunteers. Hum. Psychopharmacol. Clin. Exp. 2012, 27, 378–385. [Google Scholar] [CrossRef]
- Bradwejn, J. Neurobiological Investigations Into the Role of Cholecystokinin in Panic Disorder. J. Psychiatry Neurosci. 1993, 18, 178–188. [Google Scholar]
- Bradwejn, J.; Koszycki, D.; Shriqui, C. Enhanced Sensitivity to Cholecystokinin Tetrapeptide in Panic Disorder: Clinical and Behavioral Findings. Arch. Gen. Psychiatry 1991, 48, 603–610. [Google Scholar] [CrossRef]
- Bradwejn, J.; Koszycki, D.; Bourin, M. Dose Ranging Study of the Effects of Cholecystokinin in Healthy Volunteers. J. Psychiatry Neurosci. 1991, 16, 91–95. [Google Scholar]
- Zwanzger, P.; Baghai, T.C.; Schuele, C.; Ströhle, A.; Padberg, F.; Kathmann, N.; Schwarz, M.; Möller, H.-J.; Rupprecht, R. Vigabatrin Decreases Cholecystokinin-Tetrapeptide (CCK-4) Induced Panic in Healthy Volunteers. Neuropsychopharmacology 2001, 25, 699–703. [Google Scholar] [CrossRef]
- Zwanzger, P.; Eser, D.; Aicher, S.; Schüle, C.; Baghai, T.C.; Padberg, F.; Ella, R.; Möller, H.-J.; Rupprecht, R. Effects of Alprazolam on Cholecystokinin-Tetrapeptide-Induced Panic and Hypothalamic–Pituitary–Adrenal-Axis Activity: A Placebo-Controlled Study. Neuropsychopharmacology 2003, 28, 979–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Megen, V.H.J.G.M.; Westenberg, H.G.M.; Boer, J.A.D.; Slaap, B.; Scheepmakers, A. Effect of the selective serotonin reuptake inhibitor fluvoxamine on CCK-4 induced panic attacks. Psychopharmacology 1997, 129, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Tõru, I.; Maron, E.; Raag, M.; Vasar, V.; Nutt, D.J.; Shlik, J. The effect of 6-week treatment with escitalopram on CCK-4 challenge: A placebo-controlled study in CCK-4-sensitive healthy volunteers. Eur. Neuropsychopharmacol. 2013, 23, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Kellner, M.; Wiedemann, K.; Holsboer, F. Atrial natriuretic factor inhibits the CRH-stimulated secretion of ACTH and cortisol in man. Life Sci. 1992, 50, 1835–1842. [Google Scholar] [CrossRef]
- Ströhle, A.; Kellner, M.; Holsboer, F.; Wiedemann, K. Atrial natriuretic hormone decreases endocrine response to a combined dexamethasone-corticotropin-releasing hormone test. Biol. Psychiatry 1998, 43, 371–375. [Google Scholar] [CrossRef]
- Wiedemann, K.; Jahn, H.; Kellner, M. Effects of natriuretic peptides upon hypothalamo-pituitary-adrenocortical system activity and anxiety behaviour. Exp. Clin. Endocrinol. Diabetes 2000, 108, 5–13. [Google Scholar] [CrossRef]
- Ströhle, A.; Kellner, M.; Holsboer, F.; Wiedemann, K. Anxiolytic Activity of Atrial Natriuretic Peptide in Patients With Panic Disorder. Am. J. Psychiatry 2001, 158, 1514–1516. [Google Scholar] [CrossRef]
- Guastella, A.J.; Howard, A.L.; Dadds, M.R.; Mitchell, P.B.; Carson, D.S. A randomized controlled trial of intranasal oxytocin as an adjunct to exposure therapy for social anxiety disorder. Psychoneuroendocrinology 2009, 34, 917–923. [Google Scholar] [CrossRef]
- Considine, R.V.; Sinha, M.K.; Heiman, M.L.; Kriauciunas, A.; Stephens, T.W.; Nyce, M.R.; Ohannesian, J.P.; Marco, C.C.; McKee, L.J.; Bauer, T.L.; et al. Serum Immunoreactive-Leptin Concentrations in Normal-Weight and Obese Humans. N. Engl. J. Med. 1996, 334, 292–295. [Google Scholar] [CrossRef]
- Gautron, L.; Elmquist, J.K. Sixteen years and counting: An update on leptin in energy balance. J. Clin. Investig. 2011, 121, 2087–2093. [Google Scholar] [CrossRef] [Green Version]
- Haleem, D.J. Investigations into the involvement of leptin in responses to stress. Behav. Pharmacol. 2014, 25, 384–397. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chua, S.C. Leptin Function and Regulation. Compr. Physiol. 2018, 8, 351–369. [Google Scholar] [CrossRef]
- Graeff, F.G.; Junior, H.Z.; Paulo, S.; Hélio, B.; Junior, Z. The hypothalamic-pituitary-adrenal axis in anxiety and panic. Psychol. Neurosci. 2010, 3, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Moreno-Peral, P.; Conejo-Cerón, S.; Motrico, E.; Rodriguez-Morejón, A.; Fernández, A.; García-Campayo, J.; Roca, M.; Serrano-Blanco, A.; Rubio-Valera, M.; Bellón, J.Á. Risk factors for the onset of panic and generalised anxiety disorders in the general adult population: A systematic review of cohort studies. J. Affect. Disord. 2014, 168, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Zorn, J.V.; Schür, R.R.; Boks, M.P.; Kahn, R.S.; Joëls, M.; Vinkers, C.H. Cortisol stress reactivity across psychiatric disorders: A systematic review and meta-analysis. Psychoneuroendocrinology 2017, 77, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Gerra, G.; Zaimovic, A.; Zambelli, U.; Timpano, M.; Reali, N.; Bernasconi, S.; Brambilla, F. Neuroendocrine responses to psychological stress in adolescents with anxiety disorder. Neuropsychobiology 2000, 42, 82–92. [Google Scholar] [CrossRef]
- Phillips, A.C.; Batty, G.D.; Gale, C.R.; Lord, J.M.; Arlt, W.; Carroll, D. Major depressive disorder, generalised anxiety disorder, and their comorbidity: Associations with cortisol in the Vietnam Experience Study. Psychoneuroendocrinology 2011, 36, 682–690. [Google Scholar] [CrossRef] [Green Version]
- Okasha, A.; Bishry, Z.; Khalil, A.H.; Darwish, T.A.; El Dawla, A.S.; Shohdy, A. Panic Disorder: An overlapping or independent entity? Br. J. Psychiatry 1994, 164, 818–825. [Google Scholar] [CrossRef]
- Chaudieu, I.; Beluche, I.; Norton, J.; Boulenger, J.P.; Ritchie, K.; Ancelin, M.L. Abnormal reactions to environmental stress in elderly persons with anxiety disorders: Evidence from a population study of diurnal cortisol changes. J. Affect. Disord. 2008, 106, 307–313. [Google Scholar] [CrossRef] [Green Version]
- Mantella, R.C.; Butters, M.A.; Amico, J.A.; Mazumdar, S.; Rollman, B.L.; Begley, A.E.; Reynolds, C.F.; Lenze, E.J. Salivary cortisol is associated with diagnosis and severity of late-life generalized anxiety disorder. Psychoneuroendocrinology 2008, 33, 773–781. [Google Scholar] [CrossRef] [Green Version]
- Staufenbiel, S.M.; Penninx, B.W.J.H.; Spijker, A.T.; Elzinga, B.M.; Rossum, V.E.F.C. Hair cortisol, stress exposure, and mental health in humans: A systematic review. Psychoneuroendocrinology 2013, 38, 1220–1235. [Google Scholar] [CrossRef] [PubMed]
- Steudte, S.; Stalder, T.; Dettenborn, L.; Klumbies, E.; Foley, P.; Beesdo-Baum, K.; Kirschbaum, C. Decreased hair cortisol concentrations in generalised anxiety disorder. Psychiatry Res. 2011, 186, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Reeves, J.W.; Fisher, A.J.; Newman, M.G.; Granger, D.A. Sympathetic and hypothalamic-pituitary-adrenal asymmetry in generalized anxiety disorder. Psychophysiology 2016, 53, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Vreeburg, S.A.; Zitman, F.G.; Pelt, V.J.; DeRijk, R.H.; Verhagen, J.C.M.; Dyck, V.R.; Hoogendijk, W.J.G.; Smit, J.H.; Penninx, B.W.J.H. Salivary Cortisol Levels in Persons With and Without Different Anxiety Disorders. Psychosom. Med. 2010, 72, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Hek, K.; Direk, N.; Newson, R.S.; Hofman, A.; Hoogendijk, W.J.G.; Mulder, C.L.; Tiemeier, H. Anxiety disorders and salivary cortisol levels in older adults: A population-based study. Psychoneuroendocrinology 2013, 38, 300–305. [Google Scholar] [CrossRef] [Green Version]
- Tafet, G.E.; Feder, D.J.; Abulafia, D.P.; Roffman, S.S. Regulation of hypothalamic-pituitary-adrenal activity in response to cognitive therapy in patients with generalized anxiety disorder. Cogn. Affect. Behav. Neurosci. 2005, 5, 37–40. [Google Scholar] [CrossRef]
- Lenze, E.J.; Mantella, R.C.; Shi, P.; Goate, A.M.; Nowotny, P.; Butters, M.A.; Andreescu, C.; Thompson, P.A.; Rollman, B.L. Elevated Cortisol in Older Adults With Generalized Anxiety Disorder Is Reduced by Treatment: A Placebo-Controlled Evaluation of Escitalopram. Am. J. Geriatr. Psychiatry 2011, 19, 482–490. [Google Scholar] [CrossRef] [Green Version]
- Rosnick, C.B.; Rawson, K.S.; Butters, M.A.; Lenze, E.J. Association of cortisol with neuropsychological assessment in older adults with generalized anxiety disorder. Aging Ment. Health 2013, 17, 432–440. [Google Scholar] [CrossRef] [Green Version]
- Cohn, J.B.; Wilcox, C.S.; Meltzer, H.Y. Neuroendocrine effects of buspirone in patients with generalized anxiety disorder. Am. J. Med. 1986, 80, 36–40. [Google Scholar] [CrossRef]
- Klein, E.; Zinder, O.; Colin, V.; Zilberman, I.; Levy, N.; Greenberg, A.; Lenox, R.H. Clinical similarity and biological diversity in the response to alprazolam in patients with panic disorder and generalized anxiety disorder. Acta Psychiatr. Scand. 1995, 92, 399–408. [Google Scholar] [CrossRef]
- Roy-Byrne, P.P.; Cowley, D.S.; Hommer, D.; Ritchie, J.; Greenblatt, D.; Nemeroff, C. Neuroendocrine effects of diazepam in panic and generalized anxiety disorders. Biol. Psychiatry 1991, 30, 73–80. [Google Scholar] [CrossRef]
- Pomara, N.; Willoughby, L.M.; Sidtis, J.J.; Cooper, T.B.; Greenblatt, D.J. Cortisol response to diazepam: Its relationship to age, dose, duration of treatment, and presence of generalized anxiety disorder. Psychopharmacology 2005, 178, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Avery, D.H.; Osgood, T.B.; Ishiki, D.M.; Wilson, L.G.; Kenny, M.; Dunner, D.L. The DST in psychiatric outpatients with generalized anxiety disorder, panic disorder, or primary affective disorder. Am. J. Psychiatry 1985, 142, 844–848. [Google Scholar] [CrossRef] [PubMed]
- Schweizer, E.E.; Swenson, C.M.; Winokur, A.; Rickels, K.; Maislin, G. The Dexamethasone Suppression Test in Generalised Anxiety Disorder. Br. J. Psychiatry 1986, 149, 320–322. [Google Scholar] [CrossRef] [PubMed]
- Tiller, J.W.G.; Biddle, N.; Maguire, K.P.; Davies, B.M. The dexamethasone suppression test and plasma dexamethasone in generalized anxiety disorder. Biol. Psychiatry 1988, 23, 261–270. [Google Scholar] [CrossRef]
- Schittecatte, M.; Garcia-Valentin, J.; Charles, G.; Machowski, R.; Pena-Othaitz, M.-J.; Mendlewicz, J.; Wilmotte, J. Efficacy of the ‘clonidine REM suppression test (CREST)’ to separate patients with major depression from controls; a comparison with three currently proposed biological markers of depression. J. Affect. Disord. 1995, 33, 151–157. [Google Scholar] [CrossRef]
- Goetz, R.R.; Gorman, J.M.; Dillon, D.J.; Papp, L.A.; Hollander, E.; Fyer, A.J.; Liebowitz, M.R.; Klein, D.F. Do panic disorder patients indiscriminately endorse somatic complaints? Psychiatry Res. 1989, 29, 207–213. [Google Scholar] [CrossRef]
- Roy-Byrne, P.P.; Uhde, T.W.; Post, R.M.; Gallucci, W.; Chrousos, G.P.; Gold, P.W. The corticotropin-releasing hormone stimulation test in patients with panic disorder. Am. J. Psychiatry 1986, 143, 896–899. [Google Scholar] [CrossRef]
- Nesse, R.M.; Cameron, O.G.; Curtis, G.C.; McCann, D.S.; Huber-Smith, M.J. Adrenergic Function in Patients With Panic Anxiety. Arch. Gen. Psychiatry 1984, 41, 771–776. [Google Scholar] [CrossRef]
- Abelson, J.L.; Curtis, G.C.; Cameron, O.G. Hypothalamic-pituitary-adrenal axis activity in panic disorder: Effects of alprazolam on 24 h secretion of adrenocorticotropin and cortisol. J. Psychiatr. Res. 1996, 30, 79–93. [Google Scholar] [CrossRef]
- Stein, M.B.; Uhde, T.W. Cortisol response to clonidine in panic disorder: Comparison with depressed patients and normal controls. Biol. Psychiatry 1988, 24, 322–330. [Google Scholar] [CrossRef]
- Brambilla, F.; Bellodi, L.; Ferna, G.; Battaglia, M.; Sciuto, G.; Diaferia, G.; Petraglia, F.; Panerai, A.; Sacerdote, P. Psychoimmunoendocrine Aspects of Panic Disorder. Neuropsychobiology 1992, 26, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Uhde, T.W.; Joffe, R.T.; Jimerson, D.C.; Post, R.M. Normal urinary free cortisol and plasma MHPG in panic disorder: Clinical and theoretical implications. Biol. Psychiatry 1988, 23, 575–585. [Google Scholar] [CrossRef]
- Bandelow, B.; Sengos, G.; Wedekind, D.; Huether, G.; Pilz, J.; Broocks, A.; Hajak, G.; Rüther, E. Urinary Excretion of Cortisol, Norepinephrine, Testosterone, and Melatonin in Panic Disorder. Pharmacopsychiatry 1997, 30, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.L.; Kathol, R.G.; Noyes, R. Reduction in urinary free cortisol during benzodiazepine treatment of panic disorder. Psychoneuroendocrinology 1990, 15, 23–28. [Google Scholar] [CrossRef]
- Wedekind, D.; Sprute, A.; Broocks, A.; Huther, G.; Engel, K.; Falkai, P.; Bandelow, B. Nocturnal urinary cortisol excretion over a randomized controlled trial with paroxetine vs. placebo combined with relaxation training or aerobic exercise in panic disorder. Curr. Pharm. Des. 2008, 14, 3518–3524. [Google Scholar] [CrossRef]
- Holsboer, F.; Bardeleben, v.U.; Buller, R.; Heuser, I.; Steiger, A. Stimulation response to corticotropin-releasing hormone (CRH) in patients with depression, alcoholism and panic disorder. Horm. Metab. Res. Suppl. Ser. 1987, 16, 80–88. [Google Scholar]
- Rapaport, M.H.; Risch, S.C.; Golshan, S.; Gillin, J.C. Neuroendocrine effects of ovine corticotropin-releasing hormone in panic disorder patients. Biol. Psychiatry 1989, 26, 344–348. [Google Scholar] [CrossRef]
- Cameron, O.G.; Lee, M.A.; Curtis, G.C.; McCann, D.S. Endocrine and physiological changes during “spontaneous” panic attacks. Psychoneuroendocrinology 1987, 12, 321–331. [Google Scholar] [CrossRef] [Green Version]
- Siegmund, A.; Köster, L.; Meves, A.M.; Plag, J.; Stoy, M.; Ströhle, A. Stress hormones during flooding therapy and their relationship to therapy outcome in patients with panic disorder and agoraphobia. J. Psychiatr. Res. 2011, 45, 339–346. [Google Scholar] [CrossRef]
- Carr, D.B.; Sheehan, D.V.; Surman, O.S.; Coleman, J.H.; Greenblatt, D.J.; Heninger, G.R.; Jones, K.J.; Levine, P.H.; Watkins, W.D. Neuroendocrine correlates of lactate-induced anxiety and their response to chronic alprazolam therapy. Am. J. Psychiatry 1986, 143, 483–494. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.P.; Doran, A.R.; Liebowitz, M.R.; Fyer, A.J.; Gorman, J.M.; Klein, D.F.; Paul, S.M. Pituitary adrenocortical unresponsiveness in lactate-induced panic. Psychiatry Res. 1987, 21, 23–32. [Google Scholar] [CrossRef]
- Boer, J.A.D.; Westenberg, H.G.M.; Klompmakers, A.; Lint, v.L.E.M. Behavioral biochemical and neuroendocrine concomitants of lactate-induced panic anxiety. Biol. Psychiatry 1989, 26, 612–622. [Google Scholar] [CrossRef]
- Gorman, J.M.; Battista, D.; Goetz, R.R.; Dillon, D.J.; Liebowitz, M.R.; Fyer, A.J.; Kahn, J.; Sandberg, D.; Klein, D.F. A Comparison of Sodium Bicarbonate and Sodium Lactate Infusion in the Induction of Panic Attacks. Arch. Gen. Psychiatry 1989, 46, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Targum, S.D. Cortisol response during different anxiogenic challenges in panic disorder patients. Psychoneuroendocrinology 1992, 17, 453–458. [Google Scholar] [CrossRef]
- Ströhle, A.; Kellner, M.; Yassouridis, A.; Holsboer, F.; Wiedemann, K. Effect of Flumazenil in Lactate-Sensitive Patients With Panic Disorder. Am. J. Psychiatry 1998, 155, 610–612. [Google Scholar] [CrossRef]
- Liebowitz, M.R.; Gorman, J.M.; Fyer, A.J.; Levitt, M.; Dillon, D.; Levy, G.; Appleby, I.L.; Anderson, S.; Palij, M.; Davies, S.O.; et al. Lactate Provocation of Panic Attacks: II. Biochemical and Physiological Findings. Arch. Gen. Psychiatry 1985, 42, 709–719. [Google Scholar] [CrossRef]
- Charney, D.S.; Woods, S.W.; Goodman, W.K.; Heninger, G.R. Neurobiological mechanisms of panic anxiety: Biochemical and behavioral correlates of yohimbine-induced panic attacks. Am. J. Psychiatry 1987, 144, 1030–1036. [Google Scholar] [CrossRef]
- Charney, D.S.; Heninger, G.R.; Jatlow, P.I. Increased Anxiogenic Effects of Caffeine in Panic Disorders. Arch. Gen. Psychiatry 1985, 42, 233. [Google Scholar] [CrossRef]
- Klein, E.; Zohar, J.; Geraci, M.F.; Murphy, D.L.; Uhde, T.W. Anxiogenic effects of m-CPP in patients with panic disorder: Comparison to caffeine’s anxiogenic effects. Biol. Psychiatry 1991, 30, 973–984. [Google Scholar] [CrossRef] [Green Version]
- Bandelow, B.; Wedekind, D.; Pauls, J.; Broocks, A.; Hajak, G.; Rüther, E. Salivary Cortisol in Panic Attacks. Am. J. Psychiatry 2000, 157, 454–456. [Google Scholar] [CrossRef] [PubMed]
- Potts, N.L.; Davidson, J.R.; Krishnan, K.R.; Doraiswamy, P.M.; Ritchie, J.C. Levels of urinary free cortisol in social phobia. J. Clin. Psychiatry 1991, 52, 41–42. [Google Scholar] [PubMed]
- Uhde, T.W.; Tancer, M.E.; Gelernter, C.S.; Vittone, B.J. Normal urinary free cortisol and postdexamethasone cortisol in social phobia: Comparison to normal volunteers. J. Affect. Disord. 1994, 30, 155–161. [Google Scholar] [CrossRef]
- Klumbies, E.; Braeuer, D.; Hoyer, J.; Kirschbaum, C. The Reaction to Social Stress in Social Phobia: Discordance between Physiological and Subjective Parameters. PLoS ONE 2014, 9, e105670. [Google Scholar] [CrossRef] [Green Version]
- Veen, v.J.F.; Vliet, v.I.M.; DeRijk, R.H.; Pelt, v.J.; Mertens, B.; Zitman, F.G. Elevated alpha-amylase but not cortisol in generalized social anxiety disorder. Psychoneuroendocrinology 2008, 33, 1313–1321. [Google Scholar] [CrossRef]
- Tamura, A.; Maruyama, Y.; Ishitobi, Y.; Kawano, A.; Ando, T.; Ikeda, R.; Inoue, A.; Imanaga, J.; Okamoto, S.; Kanehisa, M.; et al. Salivary alpha-Amylase and Cortisol Responsiveness Following Electrical Stimulation Stress in Patients with the Generalized Type of Social Anxiety Disorder. Pharmacopsychiatry 2013, 46, 225–260. [Google Scholar] [CrossRef]
- Martel, F.; Hayward, C.; Lyons, D.M.; Sanborn, K.; Varady, S.; Schatzberg, A. Salivary cortisol levels in socially phobic adolescent girls. Depress. Anxiety 1999, 10, 25–27. [Google Scholar] [CrossRef]
- Essex, M.J.; Klein, M.H.; Slattery, M.J.; Goldsmith, H.H.; Kalin, N.H. Early Risk Factors and Developmental Pathways to Chronic High Inhibition and Social Anxiety Disorder in Adolescence. Am. J. Psychiatry 2010, 167, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Adam, E.K.; Vrshek-Schallhorn, S.; Kendall, A.D.; Mineka, S.; Zinbarg, R.E.; Craske, M.G. Prospective associations between the cortisol awakening response and first onsets of anxiety disorders over a six-year follow-up--2013 Curt Richter Award Winner. Psychoneuroendocrinology 2014, 44, 47–59. [Google Scholar] [CrossRef] [Green Version]
- Shlik, J.; Maron, E.; Aluoja, A.; Vasar, V.; Toru, I. Citalopram challenge in social anxiety disorder. Eur. Neuropsychopharmacol. 2002, 12, 339–340. [Google Scholar] [CrossRef]
- Katzman, M.A.; Koszycki, D.; Bradwejn, J. Effects of CCK-tetrapeptide in patients with social phobia and obsessive-compulsive disorder. Depress. Anxiety 2004, 20, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Veen, V.J.F.; Wee, V.d.N.J.A.; Fiselier, J.; Vliet, V.I.M.; Westenberg, H.G.M. Behavioural effects of rapid intravenous administration of meta-chlorophenylpiperazine (m-CPP) in patients with generalized social anxiety disorder, panic disorder and healthy controls. Eur. Neuropsychopharmacol. 2007, 17, 637–642. [Google Scholar] [CrossRef]
- Furlan, P.M.; DeMartinis, N.; Schweizer, E.; Rickels, K.; Lucki, I. Abnormal salivary cortisol levels in social phobic patients in response to acute psychological but not physical stress. Biol. Psychiatry 2001, 50, 254–259. [Google Scholar] [CrossRef]
- Condren, R.M.; O’Neill, A.; Ryan, M.C.M.; Barrett, P.; Thakore, J.H. HPA axis response to a psychological stressor in generalised social phobia. Psychoneuroendocrinology 2002, 27, 693–703. [Google Scholar] [CrossRef]
- West, v.D.; Claes, S.; Sulon, J.; Deboutte, D. Hypothalamic-pituitary-adrenal reactivity in prepubertal children with social phobia. J. Affect. Disord. 2008, 111, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Young, E.A.; Abelson, J.L.; Cameron, O.G. Effect of comorbid anxiety disorders on the Hypothalamic-Pituitary-Adrenal axis response to a social stressor in major depression. Biol. Psychiatry 2004, 56, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Veen, v.J.F.; Vliet, v.I.M.; DeRijk, R.H.; Pelt, v.J.; Mertens, B.; Fekkes, D.; Zitman, F.G. Tryptophan depletion affects the autonomic stress response in generalized social anxiety disorder. Psychoneuroendocrinology 2009, 34, 1590–1594. [Google Scholar] [CrossRef] [PubMed]
- Alfano, C.A.; Reynolds, K.; Scott, N.; Dahl, R.E.; Mellman, T.A. Polysomnographic sleep patterns of non-depressed, non-medicated children with generalized anxiety disorder. J. Affect. Disord. 2013, 147, 379–384. [Google Scholar] [CrossRef] [Green Version]
- Hood, S.D.; Melichar, J.K.; Taylor, L.G.; Kalk, N.; Edwards, T.R.; Hince, D.A.; Lenox-Smith, A.; Lingford-Hughes, A.R.; Nutt, D. Noradrenergic function in generalized anxiety disorder: Impact of treatment with venlafaxine on the physiological and psychological responses to clonidine challenge. J. Psychopharmacol. 2011, 25, 78–86. [Google Scholar] [CrossRef]
- Ising, M.; Höhne, N.; Siebertz, A.; Parchmann, A.-M.; Erhardt, A.; Keck, M. Stress response regulation in panic disorder. Curr. Pharm. Des. 2012, 18, 5675–5684. [Google Scholar] [CrossRef]
- Plag, J.; Gaudlitz, K.; Schumacher, S.; DiMeo, F.; Bobbert, T.; Kirschbaum, C.; Ströhle, A. Effect of combined cognitive-behavioural therapy and endurance training on cortisol and salivary alpha-amylase in panic disorder. J. Psychiatr. Res. 2014, 58, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Tancer, M.E.; Stein, M.B.; Uhde, T.W. Lactic acid response to caffeine in panic disorder: Comparison with social phobics and normal controls. Anxiety 1994, 1, 138–140. [Google Scholar] [CrossRef]
- Dieleman, G.C.; Huizink, A.C.; Tulen, J.H.M.; Utens, E.M.W.J.; Creemers, H.E.; Ende, v.d.J.; Verhulst, F.C. Alterations in HPA-axis and autonomic nervous system functioning in childhood anxiety disorders point to a chronic stress hypothesis. Psychoneuroendocrinology 2015, 51, 135–150. [Google Scholar] [CrossRef] [PubMed]
- Krämer, M.; Seefeldt, W.L.; Heinrichs, N.; Tuschen-Caffier, B.; Schmitz, J.; Wolf, O.T.; Blechert, J. Subjective, Autonomic, and Endocrine Reactivity during Social Stress in Children with Social Phobia. J. Abnorm. Child Psychol. 2012, 40, 95–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.Y.; Jing, D.; Bath, K.G.; Ieraci, A.; Khan, T.; Siao, C.J.; Herrera, D.G.; Toth, M.; Yang, C.; McEwen, B.S.; et al. Genetic Variant BDNF (Val66Met) Polymorphism Alters Anxiety-Related Behavior. Science 2006, 314, 140–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Zhang, H.; Li, Y.; Wang, Z.; Fan, Q.; Yu, S.; Lin, Z.; Xiao, Z. BDNF Val66Met polymorphism and plasma levels in Chinese Han population with obsessive-compulsive disorder and generalized anxiety disorder. J. Affect. Disord. 2015, 186, 7–12. [Google Scholar] [CrossRef]
- Gioiosa, L.; Iannitelli, A.; Aloe, L. Stress, anxiety schizophrenia and neurotrophic factors: The pioneer studies with nerve growth factor. Riv. di Psichiatr. 2009, 44, 88–94. [Google Scholar]
- Diniz, B.S.; Teixeira, A.L.; Machado-Vieira, R.; Talib, L.L.; Gattaz, W.F.; Forlenza, O.V. Reduced Serum Nerve Growth Factor in Patients With Late-Life Depression. Am. J. Geriatr. Psychiatry 2013, 21, 493–496. [Google Scholar] [CrossRef]
- Moreira, F.P.; Wiener, C.D.; Jansen, K.; Portela, L.V.; Lara, D.R.; Souza, L.D.d.M.; Silva, d.R.A.; Oses, J.P. Serum GDNF levels and anxiety disorders in a population-based study of young adults. Clin. Chim. Acta 2018, 485, 21–25. [Google Scholar] [CrossRef]
- Levi-Montalcini, R.; Toso, R.D.; Valle, d.F.; Skaper, S.D.; Leon, A. Update of the NGF saga. J. Neurol. Sci. 1995, 130, 119–127. [Google Scholar] [CrossRef]
- Lang, U.E.; Hellweg, R.; Bajbouj, M.; Gaus, V.; Sander, T.; Gallinat, J. Gender-dependent Association of a Functional NGF Polymorphism with Anxiety-related Personality Traits. Pharmacopsychiatry 2008, 41, 196–199. [Google Scholar] [CrossRef] [PubMed]
- Aloe, L.; Bracci-Laudiero, L.; Alleva, E.; Lambiase, A.; Micera, A.; Tirassa, P. Emotional stress induced by parachute jumping enhances blood nerve growth factor levels and the distribution of nerve growth factor receptors in lymphocytes. Proc. Natl. Acad. Sci. USA 1994, 91, 10440–10444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiener, C.D.; Ferreira, S.D.M.; Moreira, F.P.; Bittencourt, G.; Oliveira, D.J.F.; Molina, M.L.; Jansen, K.; Souza, L.D.D.M.; Lara, D.R.; Portela, L.V.; et al. Serum levels of nerve growth factor (NGF) in patients with major depression disorder and suicide risk. J. Affect. Disord. 2015, 184, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Suliman, S.; Hemmings, S.M.J.; Seedat, S. Brain-Derived Neurotrophic Factor (BDNF) protein levels in anxiety disorders: Systematic review and meta-regression analysis. Front. Integr. Neurosci. 2013, 7. [Google Scholar] [CrossRef] [Green Version]
- Graham, B.M.; Zagic, D.; Richardson, R. Low Endogenous Fibroblast Growth Factor 2 Levels Are Associated With Heightened Conditioned Fear Expression in Rats and Humans. Biol. Psychiatry 2017, 82, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Carlino, D.; Francavilla, R.; Baj, G.; Kulak, K.; D’Adamo, P.; Ulivi, S.; Cappellani, S.; Gasparini, P.; Tongiorgi, E. Brain-derived neurotrophic factor serum levels in genetically isolated populations: Gender-specific association with anxiety disorder subtypes but not with anxiety levels or Val66Met polymorphism. PeerJ 2015, 3, e1252. [Google Scholar] [CrossRef]
- Molendijk, M.L.; Bus, B.A.A.; Spinhoven, P.; Penninx, B.W.J.H.; Prickaerts, J.; Voshaar, R.C.O.; Elzinga, B.M. Gender specific associations of serum levels of brain-derived neurotrophic factor in anxiety. World J. Biol. Psychiatry 2011, 13, 535–543. [Google Scholar] [CrossRef]
- Ball, S.; Marangell, L.B.; Lipsius, S.; Russell, J.M. Brain-derived neurotrophic factor in generalized anxiety disorder: Results from a duloxetine clinical trial. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2013, 43, 217–221. [Google Scholar] [CrossRef]
- Salles, F.H.M.; Soares, P.S.M.; Wiener, C.D.; Mondin, T.C.; Silva, d.P.M.; Jansen, K.; Souza, L.D.d.M.; Silva, d.R.A.; Oses, J.P. Mental disorders, functional impairment, and nerve growth factor. Psychol. Res. Behav. Manag. 2017, 10, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Shen, Z.; Zhu, J.; Yuan, Y.; Ren, L.; Qian, M.; Lin, M.; Cai, M.; Zhang, Z.; Shen, X.; Qian, M. The roles of brain-derived neurotrophic factor (BDNF) and glial cell line-derived neurotrophic factor (GDNF) in predicting treatment remission in a Chinese Han population with generalized anxiety disorder. Psychiatry Res. 2019, 271, 319–324. [Google Scholar] [CrossRef]
- Shen, X.H.; Qian, M.C.; Niu, F.R.; Sun, S.T.; Zhu, Y.P.; Yang, J.H.; Lin, M.; Yu, B.R.; Li, L.; Shen, Z.X. Dynamic level observation of brain-derived neurotrophic factor in patients with first-episode generalized anxiety disorder. Zhonghua Yi Xue Za Zhi 2011, 91, 2939–2941. [Google Scholar] [PubMed]
- Uguz, F.; Sonmez, E.Ö.; Sahingoz, M.; Gökmen, Z.; Basaran, M.; Gezginc, K.; Sonmez, G.; Kaya, N.; Erdem, S.S.; Cicekler, H.; et al. Maternal generalized anxiety disorder during pregnancy and fetal brain development: A comparative study on cord blood brain-derived neurotrophic factor levels. J. Psychosom. Res. 2013, 75, 346–350. [Google Scholar] [CrossRef]
- Jockers-Scherübl, M.C.; Zubraegel, D.; Baer, T.; Linden, M.; Danker-Hopfe, H.; Schulte-Herbrüggen, O.; Neu, P.; Hellweg, R. Nerve growth factor serum concentrations rise after successful cognitive–behavioural therapy of generalized anxiety disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2007, 31, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.Y.; Tseng, P.T. Decreased glial cell line-derived neurotrophic factor levels in patients with depression: A meta-analytic study. J. Psychiatr. Res. 2015, 63, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, K.; Shimizu, E.; Hashimoto, K.; Mitsumori, M.; Koike, K.; Okamura, N.; Koizumi, H.; Ohgake, S.; Matsuzawa, D.; Zhang, L.; et al. Serum brain-derived neurotrophic factor (BDNF) levels in patients with panic disorder: As a biological predictor of response to group cognitive behavioral therapy. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2005, 29, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Pallanti, S.; Tofani, T.; Zanardelli, M.; Mannelli, L.D.C.; Ghelardini, C. BDNF and ARTEMIN are increased in drug-naïve non-depressed GAD patients: Preliminary data. Int. J. Psychiatry Clin. Pract. 2014, 18, 255–260. [Google Scholar] [CrossRef]
- Molendijk, M.L.; Bus, B.A.A.; Spinhoven, P.; Penninx, B.W.J.H.; Kenis, G.; Prickaerts, J.; Voshaar, R.O.; Elzinga, B.M. Serum levels of brain-derived neurotrophic factor in major depressive disorder: State–trait issues, clinical features and pharmacological treatment. Mol. Psychiatry 2011, 16, 1088–1095. [Google Scholar] [CrossRef] [Green Version]
- Ströhle, A.; Stoy, M.; Graetz, B.; Scheel, M.; Wittmann, A.; Gallinat, J.; Lang, U.E.; DiMeo, F.; Hellweg, R. Acute exercise ameliorates reduced brain-derived neurotrophic factor in patients with panic disorder. Psychoneuroendocrinology 2010, 35, 364–368. [Google Scholar] [CrossRef]
- Han, E.J.; Kim, Y.K.; Hwang, J.A.; Kim, S.H.; Lee, H.J.; Yoon, H.K.; Na, K.S. Evidence for Association between the Brain-Derived Neurotrophic Factor Gene and Panic Disorder: A Novel Haplotype Analysis. Psychiatry Investig. 2015, 12, 112–117. [Google Scholar] [CrossRef]
- Lam, P.; Cheng, C.Y.; Hong, C.J.; Tsai, S.J. Association Study of a Brain-Derived Neurotrophic Factor (Val66Met) Genetic Polymorphism and Panic Disorder. Neuropsychobiology 2004, 49, 178–181. [Google Scholar] [CrossRef]
- Santacana, M.; Arias, B.; Mitjans, M.; Bonillo, A.; Montoro, M.; Rosado, S.; Guillamat, R.; Vallès, V.; Pérez, V.; Forero, C.G.; et al. Predicting Response Trajectories during Cognitive-Behavioural Therapy for Panic Disorder: No Association with the BDNF Gene or Childhood Maltreatment. PLoS ONE 2016, 11, e0158224. [Google Scholar] [CrossRef]
- Vogelzangs, N.; Beekman, A.T.F.; Jonge, D.P.; Penninx, B.W.J.H. Anxiety disorders and inflammation in a large adult cohort. Transl. Psychiatry 2013, 3, e249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michopoulos, V.; Powers, A.; Gillespie, C.F.; Ressler, K.J.; Jovanovic, T. Inflammation in Fear- and Anxiety-Based Disorders: PTSD, GAD, and Beyond. Neuropsychopharmacology 2017, 42, 254–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weik, U.; Herforth, A.; Kolb-Bachofen, V.; Deinzer, R. Acute Stress Induces Proinflammatory Signaling at Chronic Inflammation Sites. Psychosom. Med. 2008, 70, 906–912. [Google Scholar] [CrossRef] [PubMed]
- Carroll, D.; Phillips, A.C.; Thomas, G.N.; Gale, C.R.; Deary, I.; Batty, G.D. Generalized Anxiety Disorder Is Associated with Metabolic Syndrome in the Vietnam Experience Study. Biol. Psychiatry 2009, 66, 91–93. [Google Scholar] [CrossRef] [Green Version]
- Roest, A.M.; Martens, E.J.; Jonge, d.P.; Denollet, J. Anxiety and Risk of Incident Coronary Heart Disease. J. Am. Coll. Cardiol. 2010, 56, 38–46. [Google Scholar] [CrossRef] [Green Version]
- Duivis, H.E.; Vogelzangs, N.; Kupper, N.; Jong, D.P.; Penninx, B.W.J.H. Differential association of somatic and cognitive symptoms of depression and anxiety with inflammation: Findings from the Netherlands Study of Depression and Anxiety (NESDA). Psychoneuroendocrinology 2013, 38, 1573–1585. [Google Scholar] [CrossRef] [Green Version]
- Haskó, G.; Szabo, C. Regulation of cytokine and chemokine production by transmitters and co-transmitters of the autonomic nervous system. Biochem. Pharmacol. 1998, 56, 1079–1087. [Google Scholar] [CrossRef]
- Fedoce, A.d.G.; Ferreira, F.; Bota, R.G.; Bonet-Costa, V.; Sun, P.Y.; Davies, K.W. The role of oxidative stress in anxiety disorder: Cause or consequence? Free Radic. Res. 2018, 52, 737–750. [Google Scholar] [CrossRef]
- Dowlati, Y.; Herrmann, N.; Swardfager, W.; Liu, H.; Sham, L.; Reim, E.K.; Lanctôt, K.L. A Meta-Analysis of Cytokines in Major Depression. Biol. Psychiatry 2010, 67, 446–457. [Google Scholar] [CrossRef]
- Costello, H.; Gould, R.L.; Abrol, E.; Howard, R. Systematic review and meta-analysis of the association between peripheral inflammatory cytokines and generalised anxiety disorder. BMJ Open 2019, 9, e027925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emhan, A.; Selek, S.; Bayazıt, H.; Karababa, I.F.; Kati, M.; Aksoy, N.; Katı, M.; Bayazit, H. Evaluation of oxidative and antioxidative parameters in generalized anxiety disorder. Psychiatry Res. 2015, 230, 806–810. [Google Scholar] [CrossRef] [PubMed]
- Ercan, A.C.; Bahceci, B.; Polat, S.; Cenker, O.C.; Bahceci, I.; Koroglu, A.; Sahin, K.; Hocaoglu, C. Oxidative status and prolidase activities in generalized anxiety disorder. Asian J. Psychiatry 2017, 25, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Bonifacio, K.L.; Morelli, N.R.; Vargas, H.O.; Moreira, E.G.; Stoyanov, D.S.; Barbosa, D.S.; Carvalho, A.F.; Nunes, S.O.V. Generalized Anxiety Disorder (GAD) and Comorbid Major Depression with GAD Are Characterized by Enhanced Nitro-oxidative Stress, Increased Lipid Peroxidation, and Lowered Lipid-Associated Antioxidant Defenses. Neurotox. Res. 2018, 34, 489–510. [Google Scholar] [CrossRef] [PubMed]
- Fındıklı, E.; Camkurt, M.A.; Izci, F.; Karaaslan, M.F.; Fındıklı, H.A.; Sümer, P.; Kurutas, E.B. The Diagnostic Value of Malondialdehyde, Superoxide Dismutase and Catalase Activity in Drug Naïve, First Episode, Non-Smoker Generalized Anxiety Disorder Patients. Clin. Psychopharmacol. Neurosci. 2018, 16, 88–94. [Google Scholar] [CrossRef]
- Kaya, M.C.; Bez, Y.; Karababa, I.F.; Emhan, A.; Aksoy, N.; Bulut, M.; Günes, M.; Atli, A.; Selek, S. Decreased Serum Sulphydryl Levels as a Sign of Increased Oxidative Stress in Generalized Anxiety Disorder. Psychiatry Investig. 2013, 10, 281–285. [Google Scholar] [CrossRef] [Green Version]
- Bulut, M.; Selek, S.; Bez, Y.; Karababa, I.F.; Kaya, M.C.; Günes, M.; Emhan, A.; Aksoy, N.; Sir, A. Reduced PON1 enzymatic activity and increased lipid hydroperoxide levels that point out oxidative stress in generalized anxiety disorder. J. Affect. Disord. 2013, 150, 829–833. [Google Scholar] [CrossRef]
- Yarpuz, A.Y.; Yılmaz, A.; Soykan, A.; Elgün, S.; Kumbasar, H. Levels of adenosine deaminase and dipeptidyl peptidase IV in patients with panic disorder. Turk. J. Psychiatry 2008, 19, 149–156. [Google Scholar]
- Quagliato, L.A.; Nardi, A.E. Cytokine alterations in panic disorder: A systematic review. J. Affect. Disord. 2018, 228, 91–96. [Google Scholar] [CrossRef]
- Petrowski, K.; Wichmann, S.; Kirschbaum, C. Stress-induced pro- and anti-inflammatory cytokine concentrations in panic disorder patients. Psychoneuroendocrinology 2018, 94, 31–37. [Google Scholar] [CrossRef]
- Quagliato, L.A.; Freire, R.C.; Nardi, A.E. Elevated peripheral kynurenine/tryptophan ratio predicts poor short-term auditory memory in panic disorder patients. J. Psychiatr. Res. 2019, 113, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Jabłoński, M.; Kucharska-Mazur, J.; Tarnowski, M.; Dołegowska, B.; Pędziwiatr, D.; Kubiś, E.; Budkowska, M.; Sałata, D.; Pełka-Wysiecka, J.; Kazimierczak, A.; et al. Mobilization of Peripheral Blood Stem Cells and Changes in the Concentration of Plasma Factors Influencing their Movement in Patients with Panic Disorder. Stem Cell Rev. Rep. 2017, 13, 217–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foldager, L.; Köhler-Forsberg, O.; Steffensen, R.; Thiel, S.; Kristensen, A.S.; Jensenius, J.C.; Mors, O. Bipolar and panic disorders may be associated with hereditary defects in the innate immune system. J. Affect. Disord. 2014, 164, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.R.; Park, Q.; Yu, B.H. Changes in lymphocyte subsets after short-term pharmacotherapy in patients with panic disorder. Psychiatry Res. 2004, 128, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Schleifer, S.J.; Keller, S.E.; Bartlett, J.A. Panic disorder and immunity: Few effects on circulating lymphocytes, mitogen response, and NK cell activity. Brain Behav. Immun. 2002, 16, 698–705. [Google Scholar] [CrossRef]
- Marazziti, D.; Ambrogi, F.; Vanacore, R.; Mignani, V.; Savino, M.; Palego, L.; Cassano, G.B.; Akiskal, H.S. Immune Cell Imbalance in Major Depressive and Panic Disorders. Neuropsychobiology 1992, 26, 23–26. [Google Scholar] [CrossRef]
- Martens, E.J.; Jonge, D.P.; Na, B.; Cohen, B.E.; Lett, H.; Whooley, M.A. Scared to Death? Generalized Anxiety Disorder and Cardiovascular Events in Patients With Stable Coronary Heart Disease: The heart and soul study. Arch. Gen. Psychiatry 2010, 67, 750–758. [Google Scholar] [CrossRef] [Green Version]
- Ng, F.; Berk, M.; Dean, O.; Bush, A.I. Oxidative stress in psychiatric disorders: Evidence base and therapeutic implications. Int. J. Neuropsychopharmacol. 2008, 11, 851–876. [Google Scholar] [CrossRef] [Green Version]
- Rapaport, M.H. Circulating lymphocyte phenotypic surface markers in anxiety disorder patients and normal volunteers. Biol. Psychiatry 1998, 43, 458–463. [Google Scholar] [CrossRef]
- Manfro, G.; Pollack, M.; Otto, M.; Worthington, J.; Rosenbaum, J.; Scott, E. Cell-surface Expression of L-selectin (CD62L) by Blood Lymphocytes: Correlates With Affective Parameters and Severity of Panic Disorder. Depress. Anxiety 2000, 11, 31–37. [Google Scholar] [CrossRef]
- Koh, K.B.; Lee, Y.J. Reduced Anxiety Level by Therapeutic Interventions and Cell-Mediated Immunity in Panic Disorder Patients. Psychother. Psychosom. 2004, 73, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Bandelow, B.; Baldwin, D.; Abelli, M.; Altamura, C.; Dell’Osso, B.; Domschke, K.; Fineberg, N.A.; Grünblatt, E.; Jarema, M.; Maron, E.; et al. Biological markers for anxiety disorders, OCD and PTSD—A consensus statement. Part I: Neuroimaging and genetics. World J. Biol. Psychiatry 2016, 17, 321–365. [Google Scholar] [CrossRef] [PubMed]
- D’Addario, C.; Bellia, F.; Benatti, B.; Grancini, B.; Vismara, M.; Pucci, M.; Carlo, D.V.; Viganò, C.; Galimberti, D.; Fenoglio, C.; et al. Exploring the role of BDNF DNA methylation and hydroxymethylation in patients with obsessive compulsive disorder. J. Psychiatr. Res. 2019, 114, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, A.A.; Singh, R.; Hunter, R.G. Anxiety and Epigenetics. In Advances in Experimental Medicine and Biology; Springer LLC: New York, NY, USA, 2017; Volume 978, pp. 145–166. [Google Scholar]
- Lee, B.H.; Kim, Y.K. The Roles of BDNF in the Pathophysiology of Major Depression and in Antidepressant Treatment. Psychiatry Investig. 2010, 7, 231–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feifel, D. Oxytocin as a Potential Therapeutic Target for Schizophrenia and Other Neuropsychiatric Conditions. Neuropsychopharmacology 2012, 37, 304–305. [Google Scholar] [CrossRef]
- Katahira, K.; Yamashita, Y. A Theoretical Framework for Evaluating Psychiatric Research Strategies. Comput. Psychiatry 2017, 1, 184–207. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Carroll, B.J. Biomarkers in DSM-5: Lost in translation. Aust. N. Z. J. Psychiatry 2013, 47, 676–678. [Google Scholar] [CrossRef]
- Hayashi-Takagi, A.; Vawter, M.P.; Iwamoto, K. Peripheral Biomarkers Revisited: Integrative Profiling of Peripheral Samples for Psychiatric Research. Biol. Psychiatry 2014, 75, 920–928. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Z.; Wu, T.C.; Wang, B.; Wang, H.; Tu, X.M.; Feng, C. Machine learning methods in psychiatry: A brief introduction. Gen. Psychiatry 2020, 33, e100171. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Biomarker | Finding | |
|---|---|---|
| General anxiety disorder | ||
| Serotoninergic system | Platelet 5-HT reuptake binding density | ↓ vs. HCs [23] =vs. GAD, PDA, and HCs [24] |
| Lymphocytes 5-HT reuptake binding density | =vs. HCs [25] | |
| 5-HT and 5-HIAA concentration in platelet-rich and -poor plasma and in lymphocytes | =vs. HCs [25] | |
| Noradrenergic system | Platelet alpha-2 adrenergic peripheral receptor binding density | ↓ vs. HCs [26,27] |
| GABAergic system | Platelet peripheral BDZ binding sites number | ↓ vs. HCs [28] |
| Lymphocytes peripheral BDZ binding sites number | ↓ vs. HCs [29,30] | |
| BDZ peripheral binding sites number after treatment with BDZ | ↑ vs. HCs [28,30] | |
| Panic disorders with or without agoraphobia | ||
| Serotoninergic system | 5-HT plasma levels | ↓ vs. HCs [24,31,32] |
| Platelet 5-HT concentration | =vs. HCs [33,34] | |
| Platelet aggregation in response to 5-HT | ↓ vs. HCs [35] | |
| Platelet 5-HT uptake | ↓ vs. HCs [23,35,36,37] =vs. HCs [24,38,39,40,41,42,43] ↑ vs. HCs [42,44] | |
| 5-HIAA CSF levels | =vs. HCs [45] ↓ in patients with positive response to TCAs [45] ↑ in MDD females with comorbid PDA vs. patients without comorbid PDA and vs. HCs [46] | |
| 5-HIAA jugular venous overflow | ↑ vs. HCs [47] | |
| Plasma anti-5-HT and 5-HT anti-idiotypic antibodies | ↑ vs. HCs [48] | |
| Dopaminergic system | D plasma level | ↑ vs. HCs [49] |
| GH levels in response to apomorphine | ↑ vs. MDD [50] | |
| HVA CSF concentration | =vs. HCs [45] | |
| Noradrenergic system | E plasma levels | ↑ vs. HCs [49] |
| Platelet aggregation in response to NE, platelet α-2-receptor density, and lymphocyte β-receptor density before and after TCAs treatment | ↑ vs. HCs [35] | |
| Tritiated clonidine binding (to measure platelet α-2-adrenoceptors) | ↓ vs. HCs [51] | |
| Standing plasma NE | ↑ vs. HCs [51] | |
| Beta-2-adrenoceptor density in both lying and standing position | ↑ vs. HCs [52] | |
| Plasma MHPG in alcoholics with PDA | ↑ vs. alcoholics without PDA [53] | |
| GABAergic system | BDZ receptor sensitivity (measured by the severity of panic attacks after flumazenil intravenous injection) | ↑ vs. HCs [54] |
| GABA agonistic 3α-reduced neurosteroids | ↑vs. HCs [55] ↓ vs. HCs [56] | |
| GABA antagonistic 3α-reduced isomer | ↑ vs. HCs [56] | |
| Platelets peripheral BDZ receptors | ↓ vs. HCs and vs. OCD [57] | |
| Social anxiety disorder | ||
| Serotoninergic system | Platelet 5-HT2 receptor density | =vs. HCs [58] |
| Prolactin response to mCPP | =vs. HCs [59] | |
| Cortisol response to acute fenfluramine administration | ↑ vs. HCs [60] | |
| Dopaminergic system | D3 receptor desensitization after SSRIs treatment (measured by pramipexole impact) | ↑ vs. HCs [61] |
| Biomarker | Finding | |
|---|---|---|
| General anxiety disorder | ||
| CCK | Pentagastrin induced panic attacks rate | ↑ vs. HCs [97] |
| PACAP | PACAP concentrations in females | ↓ vs. HCs [86] |
| Ghrelin | Ghrelin plasma levels in children | ↑ vs. HCs [98] |
| Leptin | Leptin circulating levels | =vs. GAD, SAD, and HCs [98] |
| Panic disorders with or without agoraphobia | ||
| CCK | CCK-4 induced panic attacks rate | ↑ vs. HCs [78] |
| CCK-8 levels in CSF | ↓ vs. HCs [99] | |
| CCK-8 levels in peripheral lymphocytes | ↓ vs. HCs [100] | |
| Leptin | Leptin plasma levels | =vs. PDA and HCs [101] |
| Leptin serum levels | correlated with disease severity in female patients [102] | |
| ANP | ANP baseline plasma levels | ↓ vs. HCs [103] |
| ANP plasma levels after lactate induced panic attacks | ↑ vs. HCs [104] | |
| Adiponectin | Adiponectin plasma levels | ↓ vs. HCs [105] |
| =vs. PDA and HCs [101] | ||
| Social anxiety disorder | ||
| OXT | OXT plasma levels | =vs. SAD and HCs [106] |
| correlated with disease severity [107] | ||
| Biomarker | Finding | |
|---|---|---|
| General anxiety disorder | ||
| Basal levels | Plasma ACTH concentration | ↑ vs. HCs [140] |
| Plasma cortisol level | =vs. HCs [140,141] | |
| ↑ vs. HCs [142] | ||
| Salivary cortisol levels | =vs. HCs [107,143] | |
| ↑ vs. HCs and positively correlated with symptoms [144] | ||
| Hair cortisol levels | ↓ vs. HCs [145,146] | |
| sAA/cortisol ratio | ↑ vs. HCs [147] | |
| Salivary cortisol awakening response | ↑ in GAD with comorbid MDD vs. HCs [148] | |
| ↓ vs. HCs in adults (>65 years) with long-lasting ADs [149] | ||
| Plasma DHEAS levels | =vs. HCs [141] | |
| Cortisol/ DHEAS ratio | =vs. HCs [141] | |
| After stress-tests/treatments | Plasma cortisol levels (after stress-test) | =vs. HCs [140] |
| Plasma ACTH concentration (after stress-test) | =vs. HCs [140] | |
| Salivary cortisol levels (after a common stressful situation) | In males, ↓ decline rate of post-stress cortisol increases vs. HCs [143] | |
| In females, ↑ post-stress cortisol secretion and ↓ recuperation capacity correlated with clinical severity [143] | ||
| Plasma cortisol levels (following CBT, escitalopram, and treatments refocusing patients’ attention) | ↓ vs. HCs [150,151,152] | |
| Plasma cortisol levels (after treatment with buspirone, alprazolam, or diazepam) | =pre vs. post treatment [153,154,155,156] | |
| sAA/cortisol ratio (after mental arithmetic challenge) | ↓ vs. HCs [147] | |
| HPA axis modifications (after dexamethasone suppression test) | =vs. MDD [142,157,158,159,160] | |
| Panic disorders with or without agoraphobia | ||
| Basal levels | Cortisol plasma levels | ↑ vs. HCs [161,162,163,164] |
| =vs. HCs [165,166] | ||
| Urinary free cortisol levels | =vs. HCs [167] | |
| ↑ vs. HCs [168] | ||
| ↑ in complicated PDA vs. HCs [169] | ||
| =in active (paroxetine) vs. placebo treatment [170] | ||
| Plasma ACTH concentration | ↑ vs. HCs [166] | |
| After stress-tests/treatments | Plasma ACTH concentration (response to CRH) | ↓ vs. HCs [162,166,171] |
| = vs. HCs [172] | ||
| Plasma cortisol levels (response to CRH) | ↓ vs. HCs [162,166] | |
| =vs. HCs [171,172] | ||
| Plasma cortisol levels (after spontaneous panic attacks) | =vs. HCs [173] | |
| Plasma cortisol levels (after feared situations) | =vs. HCs [174] | |
| Plasma cortisol levels (during panic attacks induced by lactate infusion) | =vs. HCs [175,176,177,178,179,180] | |
| ↑ vs. HCs [181] | ||
| ↓ vs. HCs [59] | ||
| Plasma cortisol levels (after yohimbine-induced panic attacks) | ↑ vs. HCs [182] | |
| Plasma cortisol levels (after caffeine or mCPP administration) | =vs. HCs [183,184] | |
| Salivary cortisol levels (during spontaneous panic attacks) | ↑ vs. after [185] | |
| Plasma ACTH concentrations (after feared situations) | =vs. HCs [174] | |
| Plasma ACTH concentrations (during panic attacks induced by lactate infusion) | =vs. HCs [175,176,177,178,179,180] | |
| Social anxiety disorder | ||
| Basal levels | Urinary free cortisol levels | =vs. HCs [186,187] |
| Salivary cortisol levels | =vs. HCs [188,189,190] | |
| =in female adolescents vs. HCs [191] | ||
| risk factor for SAD onset [192] | ||
| Salivary cortisol awakening response | ↑ in SAD patients with comorbid MDD [148] | |
| ↑ in children vs. HCs and significantly predicted SAD onset [193] | ||
| Plasma cortisol levels | =vs. HCs [188] | |
| sAA/cortisol ratio | ↑ vs. HCs [189,190] | |
| After stress-tests/treatments | Salivary cortisol levels (after TSST) | =vs. HCs [188] |
| Salivary cortisol levels (after dexamethasone) | =vs. HCs [187] | |
| Salivary cortisol levels (after intravenous citalopram, CCK-4 or mCPP) | =vs. HCs [194,195,196] | |
| Salivary cortisol levels (after administration of fenfluramine or mCPP) | ↑ vs. HCs [59,197] | |
| Salivary cortisol levels (after stress test) | ↑ vs. HCs [198,199] | |
| Plasma cortisol levels (after TSST) | =vs. HCs [188,200] | |
| ↑ in SAD patients with comorbid MDD vs. HCs [200] | ||
| sAA/cortisol ratio (after TSST) | =vs. HCs [188] | |
| sAA/cortisol ratio (after electrical stimulation) | ↑ vs. HCs [190] | |
| sAA/cortisol ratio (after dexamethasone) | ↑ vs. HCs [189] | |
| sAA/cortisol ratio (after public speaking task) | ↑ vs. HCs [201] | |
| Hair cortisol concentration (after TSST) | =vs. HCs [188] | |
| Plasma ACTH concentration (after TSST) | ↑ in SAD patients with MDD vs. HCs [200] | |
| =vs. HCs [200] | ||
| Biomarker | Finding | |
|---|---|---|
| General anxiety disorder | ||
| BDNF | Plasma levels | =vs. HCs, ↓ in females [220,221] |
| No association with disorder severity [222] | ||
| ↓ vs. HCs [210,223,224] | ||
| ↑ vs. HCs, with normalization after remission [225] | ||
| BDNF levels in the newborn’s cord blood of women with GAD | ↑ vs. HCs [226] | |
| NGF | Serum levels | =vs. HCs at baseline, ↑ after remission [227] |
| GDNF | Serum BDNF/GDNF levels | ↓ vs. HCs [228] |
| Panic disorders with or without agoraphobia | ||
| BDNF | Plasma levels | =vs. HCs [101] |
| =vs. HCs, ↓ in females [221] | ||
| ↓ in patients with a greater risk to develop panic symptoms [218] | ||
| ↓ in patients with inadequate treatment response to CBT [229] | ||
| NGF | Serum levels | =vs. HCs [223] |
| GDNF | Serum levels | ↑ vs. HCs [213] |
| Social anxiety disorder | ||
| BDNF | Plasma levels | =vs. HCs, ↓ in females [221] |
| GDNF | Serum levels | ↑ vs. HCs [213] |
| Biomarker | Finding | |
|---|---|---|
| General anxiety disorder | ||
| Cytokines | Peripheral levels of CRP, INF-γ, TNF-α, IL-1, IL-1α, IL-2, IL-6, IL-8, IL-10, IL-12p70, MCP-1, SDF-1, CM-CSF | ↑ vs. HCs [245] |
| Oxidative system | Total oxidant status and oxidative stress index | ↑ vs. HCs [246,247] |
| Nitro-oxidative stress | ↑ vs. HCs [248] | |
| Peripheral superoxide dismutase and catalase concentration | ↑ vs. HCs [248] | |
| ↓ vs. HCs [249] | ||
| Paraoxonase-1 serum levels | ↓ vs. HCs [250] | |
| ↑ vs. HCs [248,251] | ||
| Free sulfhydryl groups levels | ↓ vs. HCs [250] | |
| Lipid hydroperoxides levels | ↑ vs. HCs [248,251] | |
| Lipid-associated antioxidant defenses levels and HDL-cholesterol levels | ↓vs. HCs [248] | |
| Malondialdehyde levels | ↑ vs. HCs [249] | |
| Uric acid levels | ↑ vs. HCs [248] | |
| Panic disorders with or without agoraphobia | ||
| Cytokines | Lymphocyte proliferative response to phytohemagglutinin and IL-2 production | ↓ vs. HCs [252] |
| =vs. HCs after treatment [252] | ||
| Serum IL-6, IL-1β and IL-5 levels | ↑ vs. HCs [253] | |
| IL-6 peak reaction after a psychosocial stress test | correlated with disease severity [254] | |
| Serum IL-10 levels | ↑ vs. HCs [254] | |
| Elevated KYN/tryptophan ratio | correlated with poor short-term verbal memory [255] | |
| C3a, C5a, and C5b levels before and after pharmacological treatment | ↓ vs. HCs [256] | |
| MBL and MBL-associated serine protease-2 levels | ↓ vs. HCs [257] | |
| Peripheral lymphocyte subsets | =vs. HCs [258] | |
| CD3+, CD4+, and CD8+ T lymphocyte proportion after SSRIs treatment | ↑ vs. HCs [258] | |
| B lymphocyte proportion after SSRIs treatment | ↓ vs. HCs [258] | |
| CD19+ B lymphocytes number | ↓ vs. HCs [259] | |
| CD4+ cells number | ↓ vs. HCs [260] | |
| ADA and DPPIV serum levels | ↑ vs. HCs [252] | |
| Social anxiety disorder | ||
| Cytokines | CRP and IL-6 plasma levels | ↓ in females vs. HCs [236] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vismara, M.; Girone, N.; Cirnigliaro, G.; Fasciana, F.; Vanzetto, S.; Ferrara, L.; Priori, A.; D’Addario, C.; Viganò, C.; Dell’Osso, B. Peripheral Biomarkers in DSM-5 Anxiety Disorders: An Updated Overview. Brain Sci. 2020, 10, 564. https://doi.org/10.3390/brainsci10080564
Vismara M, Girone N, Cirnigliaro G, Fasciana F, Vanzetto S, Ferrara L, Priori A, D’Addario C, Viganò C, Dell’Osso B. Peripheral Biomarkers in DSM-5 Anxiety Disorders: An Updated Overview. Brain Sciences. 2020; 10(8):564. https://doi.org/10.3390/brainsci10080564
Chicago/Turabian StyleVismara, Matteo, Nicolaja Girone, Giovanna Cirnigliaro, Federica Fasciana, Simone Vanzetto, Luca Ferrara, Alberto Priori, Claudio D’Addario, Caterina Viganò, and Bernardo Dell’Osso. 2020. "Peripheral Biomarkers in DSM-5 Anxiety Disorders: An Updated Overview" Brain Sciences 10, no. 8: 564. https://doi.org/10.3390/brainsci10080564