Case Report: Endovascular Treatment of Chronic Atherosclerotic Renal Artery Total Occlusions with Failed Medical Therapy
 Pengyu Li
Pengyu Li Guochen Niu
Guochen Niu Ziguang Yan
Ziguang Yan Bihui Zhang
Bihui Zhang Min Yang
Min Yang- Department of Interventional Radiology and Vascular Surgery, Peking University First Hospital, Beijing, China
Background: Current guidelines generally no longer support revascularization for chronic renal artery occlusive diseases because results from randomized controlled trials favor medical therapy over angioplasty. However, increasing reports indicate that patients with renal artery occlusion (RAO) can benefit from revascularization under certain circumstances.
Case summary: Here, we present a patient with renal artery stenosis (RAS) who does not have refractory hypertension or fit any clinical trial inclusion criteria by far. Medical therapy failed to prevent the progression of RAS in this patient, leading to total occlusion of his right renal artery. This patient had progressive renal insufficiency but recovered renal function after endovascular treatment.
Conclusion: This case demonstrates that angioplasty can be beneficial in selected RAO patients, especially those with residual renal function and collateral perfusion.
Introduction
Renal artery stenosis (RAS) is a leading cause of refractory hypertension and ischemic nephropathy with a progressive decline in renal function (1). A principal cause of the occlusive renovascular disease is atherosclerosis, which accounts for nearly 90% of RAS cases (2). Renal artery occlusion (RAO) is defined as occlusion without an anterograde flow of the renal artery, and if a RAO patient presents with hypertension or renal insufficiency for more than 3 months, the occlusion is considered chronic (3). Treatment for RAO lacks guidelines on account of low incidence. The effect of revascularization in RAS aiming at preventing the progression of chronic kidney disease and lowering blood pressure (BP) is controversial compared with medical therapy alone. Herein, we report a case of a 61-year-old patient in whom medications failed to prevent total occlusion of his right renal artery, resulting in progressive renal insufficiency. His renal function recovered after endovascular revascularization and remained stable during a long-term follow-up of 4 years.
Case Presentation
A 61-year-old male patient came to our hospital for kidney dysfunction. Elevated serum creatinine (142 µmol/L) was found during a routine annual physical examination 3 months before admission. He had been diagnosed with hypertension 20 years earlier and maintained with an angiotensin-converting enzyme inhibitor and calcium channel blocker with good BP control. This patient also had a stroke 4 years earlier with no sequela left. After the stroke, he was treated with daily aspirin 100 mg and atorvastatin 20 mg.
Upon admission to our institution, his BP was 122/74 mmHg with the administration of irbesartan 150 mg and nifedipine controlled-release tablets 30 mg per day. Urinalysis showed no abnormality, and low-density lipoprotein-cholesterol was 1.64 mmol/L. His serum creatinine (Scr) was 133 µmol/L, and the estimated glomerular filtration rate (eGFR) calculated by the modification of diet in renal disease (MDRD) formula corrected for Chinese (4) was 50.65 mL/min/1.73 m2. Doppler ultrasound demonstrated severe stenosis in the right renal artery (>70%, RI = 0.47), while the contralateral renal artery was widely patent. The overall length of the right kidney had decreased to 9.6 cm, while the contralateral kidney was 11.3 cm. Split kidney function [split GFR (sGFR)] was then assessed by 99mTc-DTPA (diethylene-triamine-pentaacetate) renal dynamic scintigraphy, and the sGFR of the ischemic kidney was significantly lower than the contralateral kidney (14 mL/min vs. 41 mL/min, respectively).
Angiography showed total occlusion of the right renal artery at the ostial level with collateral perfusion to the right kidney (Figure 1A,B). Sequential dilation by balloons up to 4 × 40 mm was performed followed by deployment of balloon-expandable stents and successfully revascularized the ischemic kidney (Figure 1C).
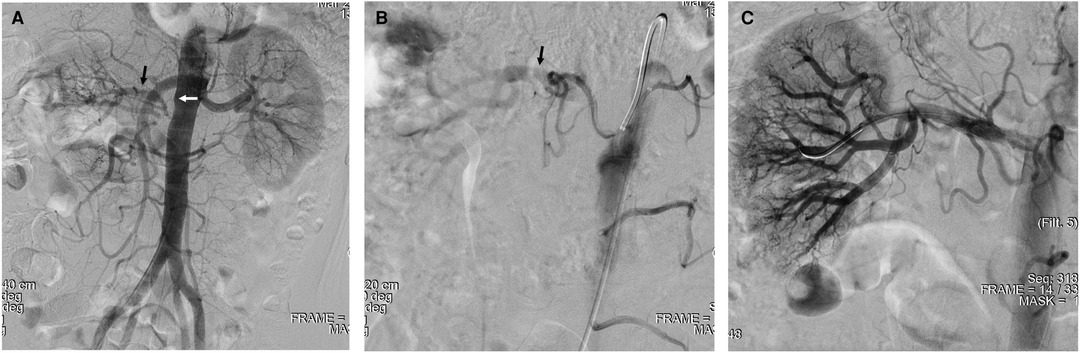
Figure 1. Stenting for occlusive right renal artery. (A,B) Angiography demonstrated complete occlusion of the right renal artery with collateral perfusion. (C) Ischemic kidney was revascularized after deployment of balloon-expandable stents. The black arrow indicates collateral flow, and the white arrow indicates the occlusive right renal artery.
This patient continued the same anti-hypertensive therapy and other medications after endovascular treatment. During a 4-year follow-up, his BP has been kept in good control with an average of 130/80 mmHg. Doppler ultrasound observed no sign of restenosis and that the size of the ischemic kidney remained unchanged at the latest follow-up. Scr did not decrease but seemed slightly rebound 1 month after intervention (Figure 2A). While during the long-term follow-up, his Scr fell down to the normal range along with a mild recovery of eGFR (Figure 2A). The function of the ischemic kidney remained stable, and a rise in the right-to-left sGFR ratio was presented (Figure 2B,C).

Figure 2. Recovery of renal function after stenting. (A) Change of serum creatinine and estimated glomerular filtration rate (GFR). (B) Change of GFR in the split kidney. (C) Split GFR ratio of the right-to-left kidney. 3m-pre indicates 3 months before treatment, pre indicates pretreatment, the post indicates post-treatment.
Discussion
Revascularization for RAS is controversial. Recent randomized controlled trials (RCTs) have failed to prove any advantages of angioplasty over optimal medical therapy (OMT) alone in RAS patients with respect to either BP control or renal protection (1, 5, 6). Although these trials have been plagued by serious methodological flaws in study design, including inclusion and exclusion criteria and endpoints (2, 7), the latest european society of cardiology/european society for vascular surgery (ESC/ESVC) guidelines (2017) still indicated that routine revascularization is not recommended in RAS secondary to atherosclerosis based on results from these RCTs (8). Indications of revascularization in chronic RAO are more strictly controlled. SCAI Appropriate Use Criteria (AUC) for renal artery stenting (2014) pointed out that it would rarely be appropriate for a treatment to be performed on an occlusive renal artery (2). However, SCAI statement (2017) regarding renal intervention in RAS stuck to the most current american heart association/american college of cardiology (ACC/AHA) guidelines, suggesting the AUC including resistant hypertension, ischemic nephropathy, and cardiac disturbances (9, 10). How to identify proper RAO patients who might benefit from revascularization has been a major concern for vascular specialists. The sudden onset of hypertension or deterioration of BP seemed to be the most common complaint of RAO patients in few published studies, and some patients had refractory hypertension (11, 12). Nonetheless, this patient’s BP had been kept in good control by two kinds of drugs. Some studies suggested that in patients with chronic kidney disease and severe RAS, angioplasty is most beneficial in those with a more rapid decline of renal function (13). However, serum creatinine elevation in this patient was not so sharp compared with previous cases and had been seemingly stable during the past 3 months before hospitalization. We have to admit that it is a patient who does not fit any clinical trial inclusion criteria by far. However, for this patient, comprehensive medications failed to prevent the progression of RAS, resulting in total occlusion; thus, renal artery stenting was performed. Considering that the average progressive GFR decline in RAO patients was 4.1 mL/min per year (14), the validity of revascularization in this patient was reasonable. Patients with symptomatic RAS are reasonable candidates for revascularization when optimal medical therapy fails (15). This case also challenged the efficiency of medical therapy in preventing the progression of RAS.
Most studies just assessed global renal function and do not evaluate split renal function in the ischemic and the contralateral kidney. However, as the reduction in sGFR in the ischemic kidney due to hemodynamically significant RAS may be compensated by hyperfiltration in the contralateral kidney that is exposed to hypertension, total eGFR poorly reflects the progression of the disease and the effects of revascularization (16, 17). Thus, we evaluated split renal function by renal dynamic scintigraphy. Previous studies reported that renal angioplasty would likely increase GFR in stenotic kidneys while decreasing filtration in contralateral kidneys (17, 18). Paradoxically, analysis of split renal function in this patient showed no improvement of sGFR in the ischemic kidney but a slight reduction of sGFR in the contralateral kidney. Although we believe that the result of preservation of the ischemic kidney function without further deterioration is acceptable, it is contradictory to the long-term follow-up outcome that presents a reduction in serum creatinine and an increase in overall eGFR. Renal dynamic scintigraphy is viewed as an effective tool in assessing the change in sGFR in the ischemic kidney (16, 17). However, measurement bias of renal dynamic imaging at different time points by different nuclear medicine physicians should be taken into consideration. We recommend the use of the right-to-left sGFR ratio as a potential solution. Although GFR of the ischemic kidney in this patient remained stable after stenting, its proportion in total renal function increased. This result probably reflected the recovery of the ischemic kidney, on the other hand. However, the efficiency of this index needs to be tested in larger trials.
So, how do we recognize patients for whom renal function can be salvaged? Preserved blood flow and kidney structure might be associated with renal outcomes after recanalization. ACC/AHA guidelines suggested that patients with an atrophic kidney size of pole-to-pole length <7 cm are unlikely to benefit from revascularization (9). However, recent studies demonstrated that patients might benefit from recanalization when collateral flow preserves even if the atrophic kidney is smaller than the indicated size in the guidelines (11, 12). Organ viability could be preserved with complete arterial occlusion in the presence of collateral arterial supply (19). Metabolic needs of the kidney only require 10% of the oxygen supplied from arterial blood (20). Collateral circulation is capable of protecting the ischemic kidney from infarction when the main renal artery is occlusive (12). There is mounting evidence indicating that for RAO patients, angioplasty may be clinically feasible in the kidney with a preserved subsegmental collateral perfusion.
Being considered as a noninvasive, side-effect-free, and cost-effective method, Doppler ultrasound has become routine and the first-line clinical examination in the diagnosis of RAS. Evaluation by ultrasound is mostly based on direct hemodynamic parameters including peak systolic velocity and renal aortic ratio and indirect parameters such as resistance index and acceleration time (21, 22). These criteria are affected by lesions in the kidney and other systemic factors of patients (22). Although the reported sensitivity and specificity of Doppler ultrasound can both reach more than 95% by the hands of experienced sonographer (23), assessments are not made on the basis of changes in vascular luminal diameter. The above-mentioned limitations of Doppler ultrasound can partly explain the inconsistency of results between ultrasound and angiography in this patient.
In summary, this case demonstrated that revascularization is feasible in RAO patients who have preserved collateral flows after optimal medical therapy fails. Even if RAO patients do not have refractory hypertension or fit any clinical trial inclusion criteria by far. Moreover, we found that the results of sGFR measured by renal dynamic scintigraphy might not be in agreement with the total eGFR calculated by the MDRD formula. The right-to-left sGFR ratio could be considered a new index when evaluating the efficacy of angioplasty in RAS patients.
Data availability statement
The original contributions presented in the study are included in the article/supplementary materials; further inquiries can be directed to the corresponding author.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
PL and MY drafted the manuscript. BZ and ZY helped with the acquisition, analysis, and interpretation of data. GN and MY revised the final draft. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Cooper CJ, Murphy TP, Cutlip DE, Jamerson K, Henrich W, Reid DM, et al. Stenting and medical therapy for atherosclerotic renal-artery stenosis. N Engl J Med. (2014) 370(1):13–22. doi: 10.1056/NEJMoa1310753
2. Parikh SA, Shishehbor MH, Gray BH, White CJ, Jaff MR. SCAI expert consensus statement for renal artery stenting appropriate use. Catheter Cardiovasc Interv. (2014) 84(7):1163–71. doi: 10.1002/ccd.25559
3. Yang M, Lin L, Niu G, Yan Z, Zhang B, Tong X, et al. Successful endovascular treatment of chronic renal artery occlusion: a preliminary retrospective case series including 15 patients. Int Urol Nephrol. (2019) 51(2):285–91. doi: 10.1007/s11255-018-02067-0
4. Ma YC, Zuo L, Chen JH, Luo Q, Yu XQ, Li Y, et al. Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease. J Am Soc Nephrol. (2006) 17(10):2937–44. doi: 10.1681/ASN.2006040368
5. Wheatley K, Ives N, Gray R, Gray R, Kalra PA, Moss JG, et al. Revascularization versus medical therapy for renal-artery stenosis. N Engl J Med. (2009) 361(20):1953–62. doi: 10.1056/NEJMoa0905368
6. Mann SJ, Sos TA. Stent placement in patients with atherosclerotic renal artery stenosis and impaired renal function. Ann Intern Med. (2010) 152(3):197; author reply 198. doi: 10.7326/0003-4819-152-3-201002020-00021
7. George JC, White CJ. Renal artery stenting: lessons from ASTRAL (angioplasty and stenting for renal artery lesions). JACC Cardiovasc Interv. (2010) 3(7):786–7. doi: 10.1016/j.jcin.2010.06.003
8. Aboyans V, Ricco JB, Bartelink MEL, Bjorck M, Brodmann M, Cohnert T, et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries. Endorsed by: the European Stroke Organization (ESO) the Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J. (2018) 39(9):763–816. doi: 10.1093/eurheartj/ehx095
9. Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients with Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. (2006) 113(11):e463–e654. doi: 10.1161/CIRCULATIONAHA.106.174526
10. Klein AJ, Jaff MR, Gray BH, Aronow HD, Bersin RM, Diaz-Sandoval LJ, et al. SCAI appropriate use criteria for peripheral arterial interventions: an update. Catheter Cardiovasc Interv. (2017) 90(4):E90–E110. doi: 10.1002/ccd.27141
11. Petrov I, Tasheva I, Garvanski I, Marzyanov M, Adam G. Recanalization and stenting of total occlusions of the renal arteries for blood pressure control in resistant to treatment hypertension. Cardiovasc Revasc Med. (2018) S1553-8389(18):30275–6. doi: 10.1016/j.carrev.2018.06.026
12. Sasaki Y, Mishima E, Kikuchi K, Toyohara T, Suzuki T, Ota H, et al. Treatment of refractory hypertension with timely angioplasty in total renal artery occlusion with atrophic kidney. Intern Med. (2021) 60(2):287–92. doi: 10.2169/internalmedicine.5290-20
13. Muray S, Martín M, Amoedo ML, García C, Jornet AR, Vera M, et al. Rapid decline in renal function reflects reversibility and predicts the outcome after angioplasty in renal artery stenosis. Am J Kidney Dis. (2002) 39(1):60–6. doi: 10.1053/ajkd.2002.29881
14. Cheung CM, Wright JR, Shurrab AE, Mamtora H, Foley RN, O'Donoghue DJ, et al. Epidemiology of renal dysfunction and patient outcome in atherosclerotic renal artery occlusion. J Am Soc Nephrol: JASN. (2002) 13(1):149–57. doi: 10.1681/ASN.V131149
15. Prince M, Tafur JD, White CJ. When and how should we revascularize patients with atherosclerotic renal artery stenosis? JACC Cardiovasc Interv. (2019) 12(6):505–17. doi: 10.1016/j.jcin.2018.10.023
16. Rossi GP, Seccia TM, Miotto D, Zucchetta P, Cecchin D, Calò L, et al. The medical and endovascular treatment of atherosclerotic renal artery stenosis (METRAS) study: rationale and study design. J Hum Hypertens. (2012) 26(8):507–16. doi: 10.1038/jhh.2011.62
17. Saeed A, Fortuna EN, Jensen G. Split renal function in patients with unilateral atherosclerotic renal artery stenosis-effect of renal angioplasty. Clin Kidney J. (2017) 10(4):496–502. doi: 10.1093/ckj/sfx052
18. Garovic VD, Textor SC. Renovascular hypertension and ischemic nephropathy. Circulation. (2005) 112(9):1362–74. doi: 10.1161/CIRCULATIONAHA.104.492348
19. Werner GS. The role of coronary collaterals in chronic total occlusions. Curr Cardiol Rev. (2014) 10(1):57–64. doi: 10.2174/1573403X10666140311123814
20. Manohar S, Hamadah A, Herrmann SM, Textor SC. Total renal artery occlusion: recovery of function after revascularization. Am J Kidney Dis. (2018) 71(5):748–53. doi: 10.1053/j.ajkd.2017.11.014
21. Schäberle W, Leyerer L, Schierling W, Pfister K. Ultrasound diagnostics of renal artery stenosis: stenosis criteria, CEUS and recurrent in-stent stenosis. Gefasschirurgie. (2016) 21:4–13. doi: 10.1007/s00772-015-0060-3
22. Wang Y, Li Y, Wang S, Ma N, Ren J. Role of contrast-enhanced ultrasound in the evaluation of patients with suspected renal arterial stenosis. Front Cardiovasc Med. (2022) 9:721201. doi: 10.3389/fcvm.2022.721201
Keywords: renal artery occlusion (RAO), endovascular treatment, medical therapy, split renal function, blood pressure
Citation: Li P, Niu G, Yan Z, Zhang B and Yang M (2022) Case Report: Endovascular Treatment of Chronic Atherosclerotic Renal Artery Total Occlusions with Failed Medical Therapy. Front. Surg. 9:843568. doi: 10.3389/fsurg.2022.843568
Received: 5 January 2022; Accepted: 7 April 2022;
Published: 18 October 2022.
Edited by:
Piergiorgio Settembrini, University of Milan, ItalyReviewed by:
Felipe Nasser, Hospital Israelita Albert Einstein, BrazilJun Zhang, The First Affiliated Hospital of Shandong First Medical University, China
Copyright © 2022 Li, Niu, Yan, Zhang and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Min Yang dryangmin@gmail.com
Speciality section: This article was submitted to Vascular Surgery, a section of the journal Frontiers in Surgery