 Hamid Ravaghi
Hamid Ravaghi Mahnaz Afshari
Mahnaz Afshari Parvaneh Isfahani
Parvaneh Isfahani Alireza Mahboub-Ahari5
Alireza Mahboub-Ahari5- 1WHO Regional Office for the Eastern Mediterranean, Cairo, Egypt
- 2School of Nursing and Midwifery, Saveh University of Medical Sciences, Saveh, Iran
- 3Student Research Committee, Saveh University of Medical Sciences, Saveh, Iran
- 4School of Public Health, Zabol University of Medical Sciences, Zabol, Iran
- 5Department of Health Economics, Iranian Evidence Based Medicine Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
Background: Recent rising costs and shortages of healthcare resources make it necessary to address the issue of hospital efficiency. Increasing the efficiency of hospitals can result in the better and more sustainable achievement of their organizational goals.
Objective: The purpose of this research is to examine hospital efficiency in the Eastern Mediterranean Region (EMR) using data envelopment analysis (DEA).
Methods: This study is a systematic review and meta-analysis of all articles published on hospital efficiency in Eastern Mediterranean countries between January 1999 and September 2020, identified by searching PubMed through MEDLINE, Web of Science, Scopus, Science Direct, and Google Scholar. The reference lists of these articles were checked for additional relevant studies. Finally, 37 articles were selected, and data were analyzed through Comprehensive Meta-Analysis Software (v.2.2.064).
Results: Using the random-effects model, the mean hospital efficiency in Eastern Mediterranean hospitals was 0.882 ± 0.01 at 95% CI. Technical efficiency (TE) was higher in some countries such as Iraq (0.976 ± 0.035), Oman (0.926 ± 0.032), and Iran (0.921 ±0.012). A significant statistical correlation was observed between the hospital efficiency and the year of publication and sample size (p < 0.05).
Conclusion: Efficiency plays a significant role in hospital growth and development. Therefore, it is important for healthcare managers and policymakers in the EMR to identify the causes of inefficiency, improve TE, and develop cost-effective strategies.
Background
Countries across the Eastern Mediterranean Region (EMR) spent more than US$ 92 billion on their health in 2008. Being exposed to enormous substantial challenges such as increasing complexity and specialization, rapidly growing demand for new medical technologies, and social claims for high-quality services, the health system in EMR allocates 60–80% of its total budget to public hospitals (1, 2). Policymakers need to be ascertained that such an overwhelming investment is in line with society's real needs and preferences. Public hospitals are often viewed in terms of the efficient use of public resources, where the final objective of these prominent non-market sectors goes beyond that of the free market such as income or benefit margin. According to the World Health Organization (WHO), hospital performance in the EMR is often poor due to several reasons such as mismanagement, low bed occupancy rate, long average lengths of stay, and high rate of hospital-associated infections (3). In its 2009 report, the WHO highlighted that hospital resources are inefficiently utilized in low- and middle-income countries compared to their developed counterparts (3). Given the complex nature of functions undertaken by public hospitals and the absence of usual market indicators, there is a clear necessity for appropriate performance measurement tools to seek out best practices and identify gaps for improvement (4, 5).
A wide variety of analytic methods has been utilized by researchers to measure hospital efficiency in terms of costs and production frontiers and the associated inefficiency of individual organizations (6–8). These techniques can be divided into two main categories: parametric and non-parametric methods. Parametric methods use econometric techniques to estimate the parameters of a specific cost of production functions, and non-parametric methods use observed real-world data to draw the shape of the frontier (5). The premier of parametric methods in use is called stochastic frontier analysis (SFA) which uses multivariate regression analysis to estimate a cost or production function, where the decomposed unexplained error term represents inefficiency (which, in the case of a cost function, will always be greater than zero) (5).
Most non-parametric methods take the form of data envelopment analysis (DEA) and its many variants. DEA uses linear programming methods to infer a piecewise linear production possibility frontier in effect seeking out those efficient observations that dominate (or envelop) the others. In contrast to parametric methods, DEA can handle multiple inputs and outputs without difficulty. DEA determines a best practice frontier of various decision-making units (DMUs) that envelops all inefficient DMUs. The estimation of the technical efficiency score is the major concern of almost all DEA models, indicating that the proper allocation of resources is not part of the calculations. Compared to parametric methods that need to initially specify production function before measurement, DEA is not subject to production function specification (9, 10).
In recent years, a vast amount of studies has been conducted in high-income countries benefiting from cutting-edge methodologies (8, 11), so some of them incorporated preferences into the analysis (7, 12, 13), as well as in the EMR, aiming at measuring hospital efficiency through both parametric and non-parametric approaches (14–16). A context-specific overview and analysis of existing articles are helpful for everyone interested in the field of efficiency measurement in healthcare with a focus on hospitals. According to our preliminary search, two systematic reviews have been conducted to address the issue in the hospital setting (17, 18). The study by Ravaghi et al. explored the potential sources of inefficiency in EMR hospitals which had been reported by 56 eligible studies and summarized the possible solutions by using qualitative synthesis (18). The second review has included 22 eligible studies from the Gulf region and estimated the technical efficiency (TE) through pooled estimation. Despite this study having systematically reviewed the existing literature and addressed one important aspect of hospital economic performance, the focus of the study was only on Gulf region countries which might limit the generalizability of the study findings to other similar settings (17). This systematic review aimed to deeply scrutinize the published literature on hospital efficiency in EMR hospitals and estimate technical efficiency which has been reported by previous studies through meta-analysis.
Methods
The present study is a systematic review and meta-analysis to examine hospital efficiency in the EMR using DEA.
Eligibility criteria
Studies were included in this systematic review if they (1) measured efficiency using a statistical method, (2) used the hospital as the analysis unit, (3) measured hospital efficiency using data envelopment analysis, (4) reported data necessary to calculate it, (5) were written in English, (6) performed a study in EMR, (7) contained data required for analysis (by access to the full text or by request from the author), and (8) included mean and SD (VRS TE or CRS TE).
Studies were excluded if they (1) used methods other than DEA (for example SFA and Pabon Lasso Model), (2) are performed at private hospitals or settings other than a hospital, and (3) were a thesis, case series, randomized controlled trials, case-control, commentaries, letters to the editor, book chapters, books, editorials, expert opinions, brief reports, and reviews.
Search sources and search strategies
PubMed through MEDLINE, Web of Science, Scopus, Science Direct, and Google Scholar were searched from January 1999 to September 2020. All of the keywords were in English, and the search strategy was restricted to English-language publications. The electronic search was complemented by hand-searching of the related articles as well as the reference lists of the final studies (Table 1).
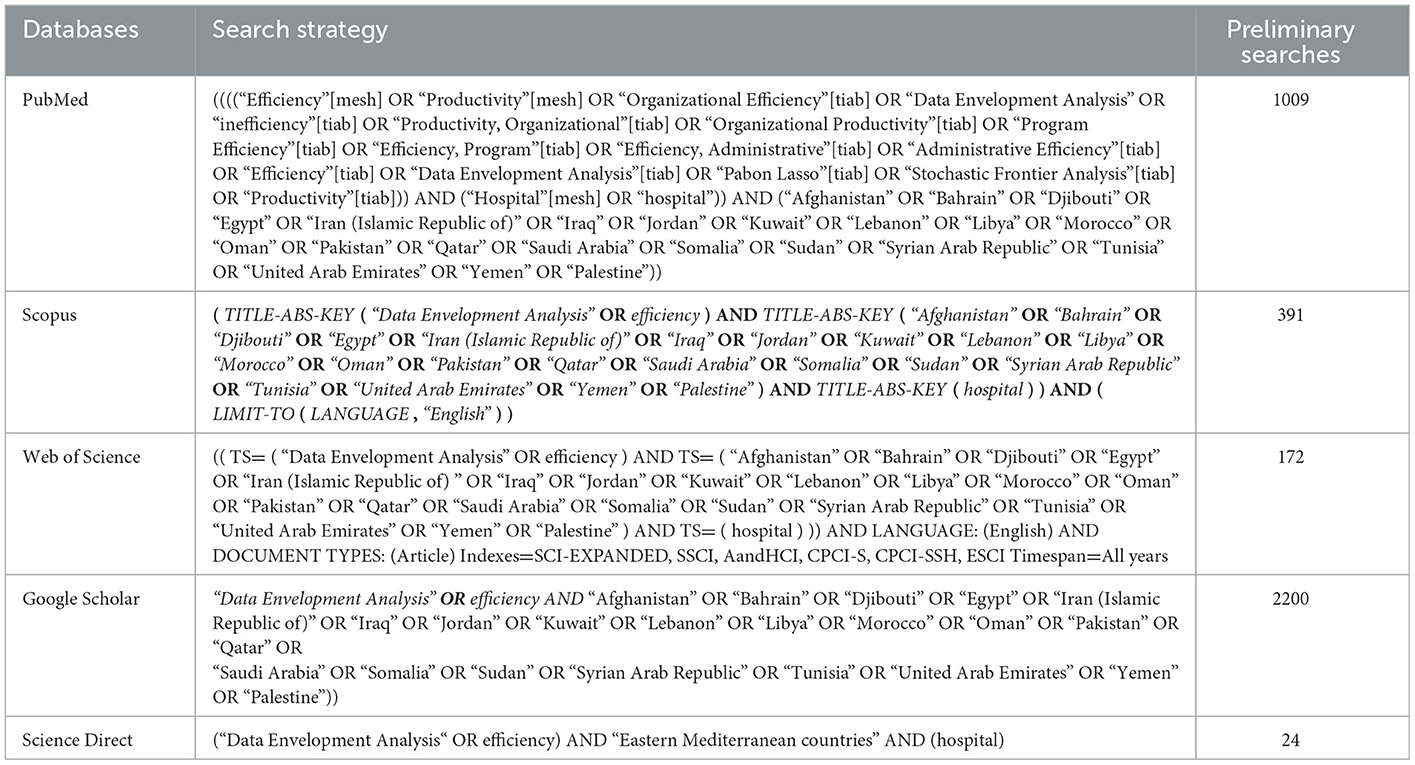
Table 1. Search strategy specific to the international electronic databases.
Screening and study selection
Search results were imported and managed via EndNote X8 (Thomson Reuters, New York, USA). Duplicates were first removed electronically and then manually. Subsequently, the title and abstract of the included studies were independently screened by two reviewers (AM and MA), and disagreements were finally resolved by helping a third reviewer (HR). The full text of potential studies was retrieved and reviewed by the two reviewers. Email or ResearchGate contact was used to obtain full-text or English versions of the inaccessible studies.
Data extraction
Two reviewers (MA and AM) extracted data for the country where the study was conducted, year of publication, research purpose, sample size, data collection method, number of hospitals examined, and mean and standard deviation (SD) of TE.
Quality assessment
The methodological quality of the eligible studies was assessed using the five-question instrument which was introduced and applied by Mitton et al. (19) (see the Appendix). Each question was given a score of 0 (not present or reported), 1 (present but low quality), 2 (present and mid-range quality), or 3 (present and high quality). Criteria for assessment of quality included a literature review and identifying research gaps; research questions, hypotheses, and design; population and sampling; data collection process and instruments; and analysis and reporting of results. The assessment was conducted by both AM and MA, and discrepancies were then resolved either by discussion or by the third reviewer (HR).
Data analysis
Since the mean and standard deviation of TE had not been reported by most of the included studies, we dealt with this missing information by contacting the authors of these studies or calculating the values using available data. Meta-analysis was conducted to synthesize the mean technical efficiency (TE) using the random-effects model by the sample size weighting (20). The results were presented with 95% confidence intervals (95% CIs) (20). Statistical heterogeneity among the studies was assessed by Cochran's Q statistic and I2 index (21, 22). As the analytical results revealed a high heterogeneity (96.07%), the random-effects model was employed and covariates between variables were examined using the meta-regression function. All these statistical analyses were conducted using the Comprehensive Meta-Analysis Software (v.2.2.064).
Results
The initial search resulted in 3,796 articles. After excluding duplicates and irrelevant articles, 2,725 studies were selected for abstract examination, whereas 2,674 articles were removed after reviewing abstracts. We also scrutinized 51 full-text articles for eligibility and excluded 14 because they did not satisfy our inclusion/exclusion criteria [Four were review articles (17, 18, 23, 24), five used different estimation methods (14, 16, 25–29), one article was conducted in a single hospital ward (30), and two articles did not report mean and SD (neither VRS TE nor CRS TE) (31, 32)]. Finally, 37 articles were found eligible for inclusion in this systematic review and meta-analysis. The reference lists of these 37 articles were manually searched, but no additional studies were included (Figure 1). The PRISMA flow diagram (33) was followed in this study.

Figure 1. PRISMA flow diagram (33) illustrating the study selection process.
Characteristics of the included studies
Over half of the studies had been published after 2010, with most having been conducted in 2017 and 2014 (Figure 2). Studies were only conducted in 11 of the 22 EMR countries. The overwhelming majority of these are located in Iran (N = 20) and Saudi Arabia (N = 4). The sample size varied from three (34) to 270 (35) hospitals. Health reports, interviews, hospital records, or annual statistical records were reported as the sources of data.
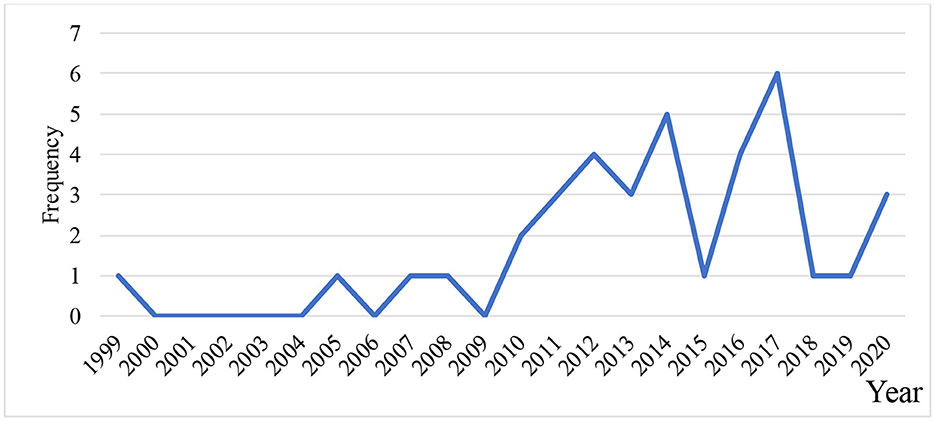
Figure 2. Distribution of hospital efficiency studies by publication year.
Efficiency had been assessed in light of various concepts including technical, scale, and pure efficiency with a primary focus on TE in the reviewed studies. The reviewed studies varied in the models used to estimate the TE of public hospitals. Twelve studies used both constant and variable return to the efficiency scale (CRS and VRS), whereas 19 applied variable return to scale (VRS) and 6 used constant return to scale (CRS). The inputs used in the included studies are presented in Table 2, with a range of 2–5. Predominant inputs were the labor (including full-time and part-time physicians, full-time and part-time nurses, midwives, non-medical staff, and dentists) and capital (number of beds) variables. Two studies (36, 37) used capital expenses in the inputs. Numerous output dimensions were used in the efficiency models (range: 1–9 variables). Output variables focused on the number of outpatient visits and inpatient admissions. Twelve studies used bed turnover (BTR) and occupancy (BOR) rates, and 10 studies used an average length of stay (ALS), while one study (38) used mortality rate in hospitals as an output variable (Table 2).
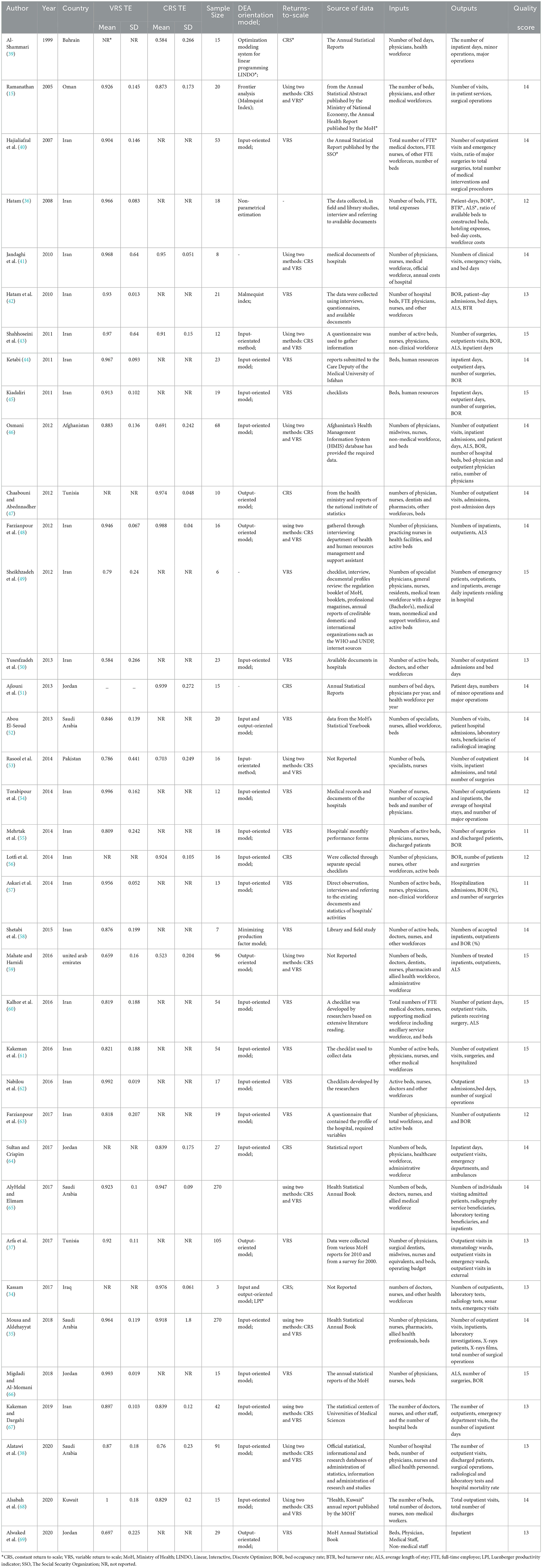
Table 2. Characteristics of included studies reported technical efficiency in hospitals located in EMR.
The methodological quality of included studies
No articles were excluded based on the quality appraisal. All the included studies acquired more than 70% of the overall score. So that 95% (N = 35) of the studies were in the third quarter Q3 (≥75% of overall score). More than 65% (N = 13) of the studies have developed a good research question, and most of them adopted an appropriate sample size (92%, n = 34). With respect to the data collection method, 100% of the studies followed the standard guideline in collecting data and acquired the full score in this item. The analysis and results of the reporting item were the one item that most of the studies could not get a full score; therefore, only 33% (N = 12) of the studies got a full score here. The quality assessment scores are presented in Table 2.
To examine the consistency of efficiency assessments, we conducted a meta-analysis of the estimated TE scores reported in the reviewed studies. The mean and standard deviation of TE with the CRS model in Eastern Mediterranean hospitals are 0.826 ± 0.03 at the 95% significance level. According to the random-effects model, TE was higher in Iran (0.988 ± 0.010) in 2012 (Figure 3).
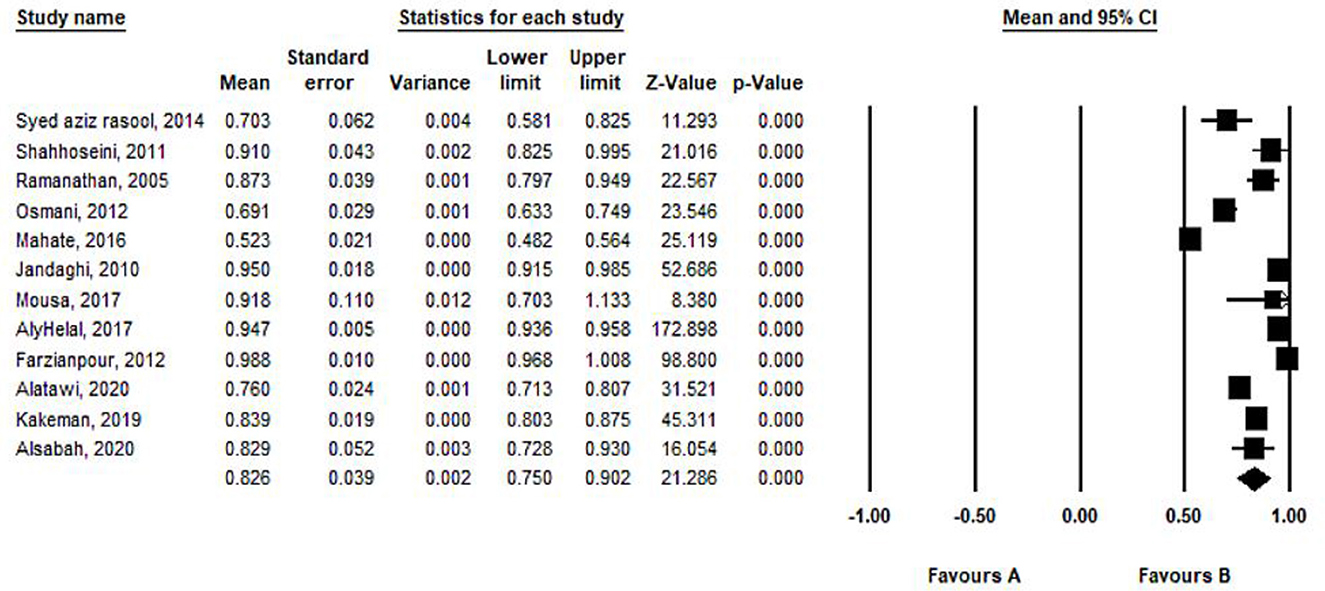
Figure 3. Mean and standard deviation of TE with CRS model in included studies based on the random-effects model.
The mean and standard deviation of TE with the VRS model in Eastern Mediterranean hospitals are 0.892 ± 0.012 at a 95% significance level. According to the random-effects model, TE was high in Kuwait (1.00 ± 0.046) (Figure 4).
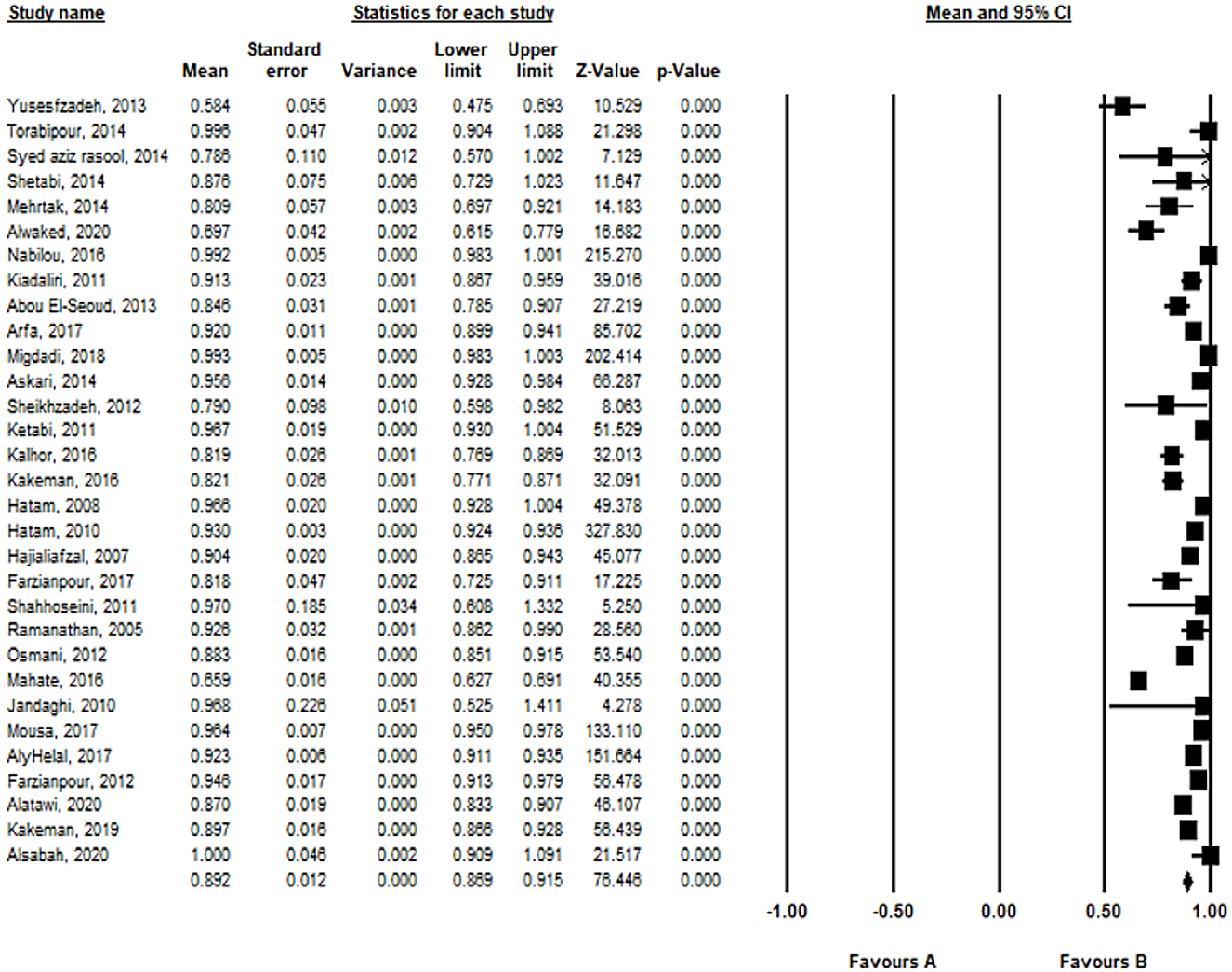
Figure 4. Mean and standard deviation of TE with the VRS model in included studies based on the random-effects model.
Studies examining fewer hospitals for estimations reported higher efficiency scores compared to studies using more hospitals. Studies published in lower-middle-income countries reported TE to score higher compared to others (Table 3).
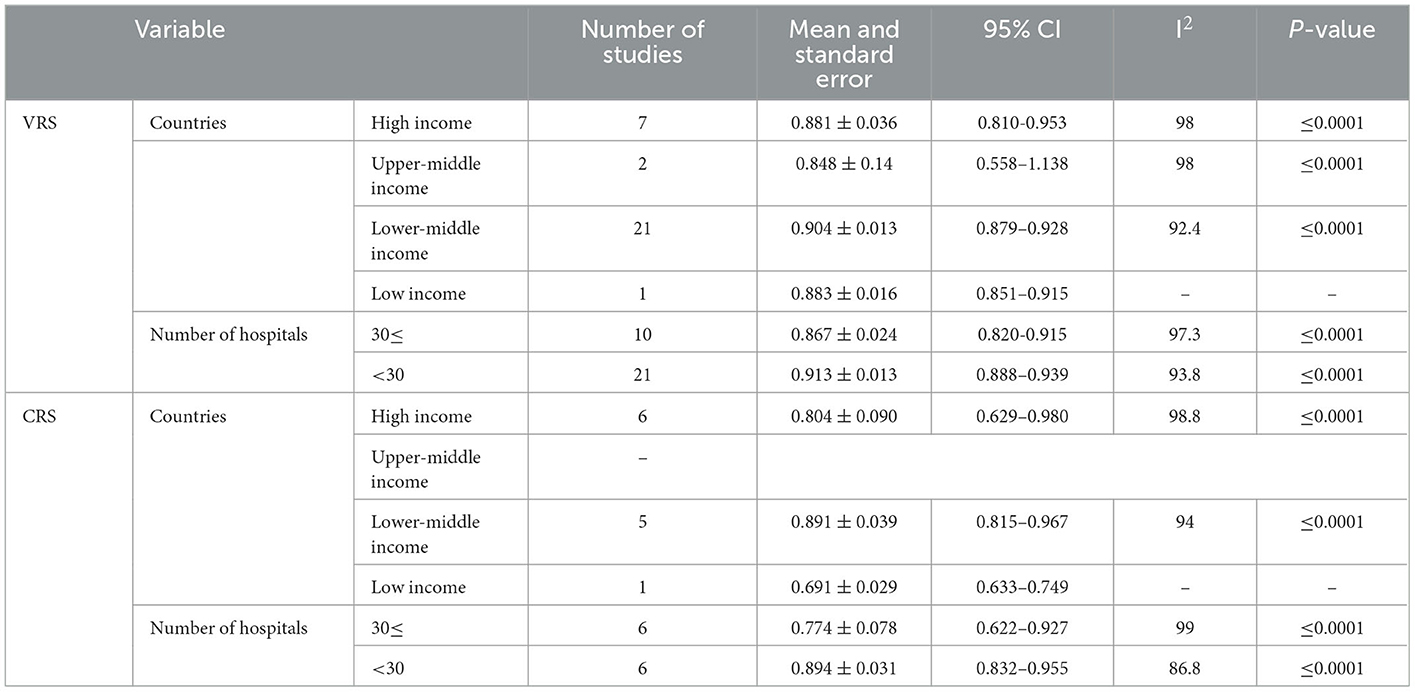
Table 3. Subgroup analysis of efficiency scores by country and method of analysis.
The results of the heterogeneity test indicated a high level of heterogeneity between the studies (I2 = 96.07%, P = 0.0001). Therefore, potential sources of heterogeneity were examined using the meta-regression function. The results are displayed in Table 4, indicating that the year of publication and sample size of articles have caused heterogeneity between the reviewed studies (p < 0.05). The results of meta-regression with VRS, based on the year of study, demonstrated that an increase of one unit per year of study causes a higher incidence of hospital efficiency by 0.003 units. Moreover, the efficiency of the hospital decreases by 0.00008 as the sample size of articles increases. On the other hand, the results of meta-regression with CRS, based on the year of study, demonstrated that an increase of one unit per year of study causes a lower incidence of hospital efficiency by 0.006 units. Moreover, the efficiency of the hospital decreases by 0.006 as the sample size of articles increases.

Table 4. Results of the heterogeneity test (meta-regression model).
Discussion
Several systematic reviews have been conducted on hospital efficiency worldwide (18, 70, 71). For example, a 2018 study reviewed 57 articles using DEA (18), and a 2014 study reviewed 23 articles using DEA, SFA, and balanced scorecard (71). To our knowledge, this is the first attempt to measure hospital efficiency using meta-analysis in the Eastern Mediterranean region. There was a growing trend in recent years to measure the efficiency of hospitals using different methods. In this study, we reviewed studies that measured the TE of hospitals in EMR countries. A total of 37 articles which calculated hospital efficiency using DEA were eligible for inclusion in the meta-analysis.
It must be noted that the vast majority of studies on hospital efficiency were conducted in Iran. This may partly be due to the Iranian Ministry of Health and Medical Education's attempt at reducing hospital costs. In addition, efficiency and strategies for improving it have become a key priority for the Iranian government.
A mean TE of 0.882 ± 0.01 was estimated for Eastern Mediterranean countries. This finding is consistent with the results of previous studies in other countries (24, 72, 73). Pereira et al. (4) examined the convergence in productivity and indicated that in the EMR, the performance spread among countries is decreasing and the gap between the best and worst practice frontier is increasing. Also, they showed that innovator EMR countries are Egypt, Jordan, Kuwait, Qatar, Tunisia, and the United Arab Emirates, and the lagging EMR WHO Member State is Somalia. In the study conducted by Du (73) on Chinese hospitals economic performance, the mean hospital efficiency was estimated at 0.74, 0.902, and 0.805 in the Central, Eastern, and Western regions of the country, respectively (73). Blatnik et al. (72) examined hospital efficiency in Slovenia and reported a mean TE of 0.936 (72). These extensive empirical works indicate that hospital efficiency can significantly vary across different countries and regions (4, 11).
According to our findings, the mean hospital efficiency varied in high-income countries such as Saudi Arabia, Oman, the United Arab Emirates, and Bahrain. For example, Oman had the highest mean TE, and Bahrain had the lowest mean TE. According to the 2017 WHO's report on “Eastern Mediterranean Region Framework for health information systems and core indicators for monitoring the health situation and health system performance,” Bahrain and Oman had the highest general government expenditure on health as a percentage of general government expenditure (10.5 and 6.8%, respectively) among the four countries (74). On the other hand, mean hospital efficiency also varied in low- and middle-income countries such as Pakistan, Afghanistan, Iran, Jordan, Tunisia, Palestine, and Iraq. For instance, among these countries, Iraq and Iran stood at the top of the list, whereas Pakistan had the lowest mean TE among other counterparts. WHO's world health report 2017 highlighted that among these seven countries, Iran had the highest and Pakistan had the lowest general government expenditure on health as a percentage of general government expenditure (17.5 and 4.7%, respectively) (74). Therefore, hospital managers and policymakers must focus on improving efficiency and reducing healthcare costs in regions that have lower rates of hospital efficiency. Furthermore, a study using the ‘Sustainable Public Health Index' showed that Bahrain, Egypt, Iran (the Islamic Republic of), Jordan, Kuwait, Libya, Morocco, Oman, Pakistan, Qatar, Saudi Arabia, the Syrian Arab Republic, and the United Arab Emirates were the efficient EMR countries between WHO Member States (75).
Hospital internal structure (11), regional differences (4, 11), and decision-maker participation in the assessment (13) of the environmental, social, and economic sustainability of the hospital (7) have a significant impact on the efficiency of hospitals. The development of outpatient care (23), reducing supplier-induced demand (76), the strengthening of hospital management and quality management (70, 77), the strengthening of governance and regulation (78), and enhanced crisis resilience such as COVID-19 crisis (8) are recommended as effective strategies to increase hospital efficiency. In addition, hospitals can serve as productive business entities through health system structure reform at the macro level, proper implementation of healthcare stratification, and responsiveness of insurance companies (23, 79). This allows hospitals to increase patient satisfaction and provide safe, high-quality care.
The measurement of hospital efficiency is done through a set of input and output variables (80, 81). The present findings show that the most commonly used input variables in studies on hospital efficiency in the EMR are the number of employees and the number of beds, while the most commonly used output variables are the number of outpatient visits, the number of inpatient admission, and the number of operations. For example, in a study on hospital efficiency in Oman, Ramanathan (2005) used outpatient visits, inpatient services, and surgical operations as outputs, and the number of beds and manpower as inputs (15). In addition, some studies have used other inputs such as work hours, non-labor costs (i.e., equipment, food, and drugs), the area of the hospital in cubic meters (82, 83), and outputs such as mortality rate, number of nursing students, number of medical students, number of nursing and medical training weeks, and number of scientific publications (84, 85). Pereira proposed a framework to make a “sustainable public health index” and assessed the performance of the WHO Member States by using the 13 indicators of the UN's SDG 3 targets as input and output (75). They found that the EMR was in fourth place among six WHO regions (75). Researchers must use more input and output variables when measuring hospital efficiency to increase the accuracy of their findings.
In some countries, mean efficiency has increased significantly in recent years. For example, Helal et al. (65) showed a significant improvement in the average efficiency of Saudi hospitals in 2014 compared to 2006, with hospital efficiency reaching 92.3% in 2014 (65).
The present systematic review showed that, on average, small-scale (47) and public hospitals (61) have a lower level of efficiency. For example, Chaabouni and Abednnadher (2016), who examined Tunisian public hospitals, reported a positive association between cost-effectiveness and hospital size. They found that the mean cost-effectiveness was 0.995 in large hospitals compared to 0.875 in small hospitals (47). In a study on Iranian hospitals, Ketabi (2011) showed that CCUs in 83.3% of teaching hospitals and 60% of private hospitals perform inefficiently (44). This was attributed to the excess of medical equipment as well as personnel and technological capabilities. Teaching hospitals were less efficient because of bureaucratic processes, and private hospitals had lower BORs. There is a larger demand for care in public hospitals than in private hospitals, and thus, public hospital managers in particular must make optimal use of their resources.
The present review showed that hospital efficiency decreases by 0.00008 as the sample size of articles increases. On the other hand, hospital efficiency increases by 0.003% as the publication date increases by 1 year. In other words, the time sequence of studies on hospital efficiency indicates lower levels of efficiency in recent years compared to previous years.
Conclusion
The results of this systematic review and meta-analysis of hospital efficiency in Eastern Mediterranean countries highlighted that the reviewed studies varied in the model used to estimate the technical efficiency in public hospitals (CRS and VRS). The EMR studies have based their analysis on hospital inputs. Also, a significant statistical correlation was observed between the hospital efficiency and the year of publication and sample size.
The results of this article should, however, be cautiously interpreted. Although the pooled estimation of hospital efficiency reflects only the performance of a limited number of Eastern Mediterranean countries, this gap in the literature indicates that the reviewed studies are not comprehensive in terms of coverage and methodology. Other variables, such as ownership or type of hospital, can impact the results of efficiency analysis, but a small sample size restricts control of this variable.
In recent years, the number of studies on efficiency has significantly increased, likely due to the increase in interest in the subject due to resource scarcity. To enable effective and efficient hospital management and improvement in hospital efficiency, health managers and policymakers must identify the causes of hospital inefficiency. An effective way of increasing hospital efficiency is by using evidence-based interventions. Therefore, health policymakers in Eastern Mediterranean countries must first identify the causes of hospital inefficiency and take necessary remedial actions to facilitate the optimal use of scarce resources.
Author contributions
MA and HR designed the research. MA, AM-A, and PI conducted it. MA and PI extracted the data. MA, HR, VB, AM-A, and PI wrote the study. MA had primary responsibility for the final content. All authors read and approved the final manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1085459/full#supplementary-material
Abbreviations
EMR, Eastern Mediterranean Region; BOR, bed occupancy rate; BTR, bed turnover rate; ALS, the average length of stay; HICs, high-income countries; DEA, data envelopment analysis; SFA, stochastic frontier analysis; WHO, World Health Organization; LMICs, low- and middle-income; MoH, Ministry of Health; FTE, full-time employee.
References
1. Organization WH. High Level Expert Meeting on Health Priorities in the Eastern Mediterranean Region, 1-2 March 2012: Health Systems in the Eastern Mediterranean Region: Situation, Challenges and Gaps, Priorities and WHO Contribution. (2012). Geneva: WHO.
2. EMRO Countries and Health Costs. Available online at: https://www.emro.who.int/entity/health-economics/index.html (accessed October 07, 2022).
3. Organization WH. Improving hospital performance in the Eastern Mediterranean Region. Geneva: WHO (2009).
4. Pereira MA, Camanho AS, Marques RC, Figueira JR. The convergence of the world health organization member states regarding the united nations' sustainable development goal ‘good health and well-being'. Omega. (2021) 104:102495. doi: 10.1016/j.omega.2021.102495
5. Jacobs R, Smith PC, Street A. Measuring Efficiency in Health Care: Analytic Techniques and Health Policy. Cambridge: Cambridge University Press (2006).
6. Gannon B. Testing for variation in technical efficiency of hospitals in Ireland. Econom Soc Rev. (2005) 36:273–94.
7. Pederneiras YM, Pereira MA, Figueira JR. Are the Portuguese public hospitals sustainable? A triple bottom line hybrid data envelopment analysis approach. Int Trans Operational Res. (2021). 30:453–75. doi: 10.1111/itor.12966
8. Pereira MA, Dinis DC, Ferreira DC, Figueira JR, Marques RC. A network data envelopment analysis to estimate nations' efficiency in the fight against SARS-CoV-2. Expert Syst Appl. (2022) 210:118362. doi: 10.1016/j.eswa.2022.118362
9. Cooper W, Seiford L, Tone K, Zhu J. Some models and measures for evaluating performances with DEA: past accomplishments and future prospects. J Prod Anal. (2007) 28:151–63. doi: 10.1007/s11123-007-0056-4
10. Kohl S, Schoenfelder J, Fügener A, Brunner JO. The use of data envelopment analysis (DEA) in healthcare with a focus on hospitals. Health Care Manag Sci. (2019) 22:245–86. doi: 10.1007/s10729-018-9436-8
11. Pereira MA, Ferreira DC, Figueira JR, Marques RC. Measuring the efficiency of the Portuguese public hospitals: a value modelled network data envelopment analysis with simulation. Expert Syst Appl. (2021) 181:115169. doi: 10.1016/j.eswa.2021.115169
12. Pereira MA, Camanho AS, Figueira JR, Marques RC. Incorporating preference information in a range directional composite indicator: the case of Portuguese public hospitals. Eur J Oper Res. (2021) 294:633–50. doi: 10.1016/j.ejor.2021.01.045
13. Pereira MA, Figueira JR, Marques RC. Using a Choquet integral-based approach for incorporating decision-maker's preference judgments in a data envelopment analysis model. Eur J Oper Res. (2020) 284:1016–30. doi: 10.1016/j.ejor.2020.01.037
14. Hamidi S. Measuring efficiency of governmental hospitals in Palestine using stochastic frontier analysis. Cost Effect Res Allocat. (2016) 14:1–12. doi: 10.1186/s12962-016-0052-5
15. Ramanathan R. Operations assessment of hospitals in the Sultanate of Oman. Int J Operat Prod Manage. (2005) 25:39–54. doi: 10.1108/01443570510572231
16. Younsi M. Performance of Tunisian public hospitals: A comparative assessment using the Pabón Lasso Model. Int J Hos Res. (2014) 3:159–66.
17. Alatawi A, Ahmed S, Niessen L, Khan J. Systematic review and meta-analysis of public hospital efficiency studies in Gulf region and selected countries in similar settings. Cost Effect Res Allocation. (2019) 17:1–12. doi: 10.1186/s12962-019-0185-4
18. Ravaghi H Afshari M Isfahani P Bélorgeot Bélorgeot VD A systematic review on hospital inefficiency in the Eastern Mediterranean Region: sources and solutions. BMC Health Serv Res. (2019) 19:1–20. doi: 10.1186/s12913-019-4701-1
19. Mitton C, Adair CE, McKenzie E, Patten SB, Perry BW. Knowledge transfer and exchange: review and synthesis of the literature. Milbank Q. (2007) 85:729–68. doi: 10.1111/j.1468-0009.2007.00506.x
20. Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration. Available online at: https://www.cochrane-handbook.org (2011) (accessed October 10, 2022).
21. Denison HJ, Dodds RM, Ntani G, Cooper R, Cooper C, Sayer AA, et al. How to get started with a systematic review in epidemiology: an introductory guide for early career researchers. Arch Pub Health. (2013) 71:1–8. doi: 10.1186/0778-7367-71-21
22. Fiest K, Pringsheim T, Patten S, Svenson L, Jette N. The role of systematic reviews and meta-analyses of incidence and prevalence studies in neuroepidemiology. Neuroepidemiology. (2014) 42:16–24. doi: 10.1159/000355533
23. Mosadeghrad AM, Esfahani P, Afshari M. Strategies to improve hospital efficiency in Iran: a scoping review. Payesh. (2019) 18:7–21.
24. Mosadeghrad AM, Esfahani P, Nikafshar M. Hospitals' efficiency in Iran: a systematic review and meta-analysis of two decades of research. J Payavard Salamat. (2017) 11:318–31.
25. Bastani P, Vatankhah S, Salehi M. Performance ratio analysis: a national study on Iranian hospitals affiliated to ministry of health and medical education. Iran J Public Health. (2013) 42:876.
26. Chaabouni S, Abednnadher C. Cost efficiency of Tunisian public hospitals: a Bayesian comparison of random and fixed frontier models. J Knowl Econ. (2016) 7:771–81. doi: 10.1007/s13132-015-0245-8
27. Hassanain M, Zamakhshary M, Farhat G, Al-Badr A. Use of Lean methodology to improve operating room efficiency in hospitals across the Kingdom of Saudi Arabia. Int J Health Plann Manage. (2017) 32:133–46. doi: 10.1002/hpm.2334
28. Masoompour SM, Petramfar P, Farhadi P, Mahdaviazad H. Five-year trend analysis of capacity utilization measures in a teaching hospital 2008-2012. Shiraz E-Med J. (2015) 16:e211. doi: 10.17795/semj21176
29. Sajadi HS, Sajadi ZS, Sajadi FA, Hadi M, Zahmatkesh M. The comparison of hospitals' performance indicators before and after the Iran's hospital care transformations plan. J Educ Health Prom. (2017) 6:16. doi: 10.4103/jehp.jehp_134_16
30. Al-Shayea AM. Measuring hospital's units efficiency: A data envelopment analysis approach. Int J Eng Technol. (2011) 11:7–19.
31. Marnani AB, Sadeghifar J, Pourmohammadi K, Mostafaie D, Abolhalaj M, Bastani P. Performance assessment indicators: how DEA and Pabon Lasso describe Iranian hospitals' performance. HealthMED. (2012) 13:791–6.
32. Safdar KA, Emrouznejad A, Dey PK. Assessing the queuing process using data envelopment analysis: an application in health centres. J Med Syst. (2016) 40:1–13. doi: 10.1007/s10916-015-0393-1
33. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. (2021) 10:1–11. doi: 10.1186/s13643-021-01626-4
34. Kassam A. Efficiency analysis of healthcare sector. Eng Technol J. (2017) 35:509–15. doi: 10.30684/etj.35.5A.10
35. Mousa W, Aldehayyat JS. Regional efficiency of healthcare services in Saudi Arabia. Middle East Dev J. (2018) 10:152–74. doi: 10.1080/17938120.2018.1443607
36. Hatam N. The role of Data Envelopment Analysis (DEA) pattern in the efficiency of social security hospitals in Iran. Iranian Red Cresc Med J. (2008) 10:211–7.
37. Arfa C, Leleu H, Goaïed M, Van Mosseveld C. Measuring the capacity utilization of public district hospitals in tunisia: using dual data envelopment analysis approach. Int J Health Policy Manage. (2017) 6:9. doi: 10.15171/ijhpm.2016.66
38. Alatawi AD, Niessen LW, Khan JA. Efficiency evaluation of public hospitals in Saudi Arabia: an application of data envelopment analysis. BMJ Open. (2020) 10:e031924. doi: 10.1136/bmjopen-2019-031924
39. Al-Shammari M. A multi-criteria data envelopment analysis model for measuring the productive efficiency of hospitals. Int J Operat Prod Manag. (1999) 19:879–91. doi: 10.1108/01443579910280205
40. Hajialiafzali H, Moss J, Mahmood M. Efficiency measurement for hospitals owned by the Iranian social security organisation. J Med Syst. (2007) 31:166–72. doi: 10.1007/s10916-007-9051-6
41. Jandaghi G, Matin HZ, Doremami M, Aghaziyarati M. Efficiency evaluation of Qom public and private hospitals using data envelopment analysis. Eur J Econ Financ Admin Sci. (2010) 22:83–91.
42. Hatam N, Sh M, Askarian M, Shokrpour N. The efficiency of general public hospitals in Fars Province, Southern Iran. Iranian Red Cresc Med J. (2010) 12:138–44.
43. Shahhoseini R, Tofighi S, Jaafaripooyan E, Safiaryan R. Efficiency measurement in developing countries: application of data envelopment analysis for Iranian hospitals. Health Serv Manage Res. (2011) 24:75–80. doi: 10.1258/hsmr.2010.010017
44. Ketabi S. Efficiency measurement of cardiac care units of Isfahan hospitals in Iran. J Med Syst. (2011) 35:143–50. doi: 10.1007/s10916-009-9351-0
45. Kiadaliri AA. Measuring efficiency of general hospitals in the South of Iran. World Appl Sci J. (2011) 13:1310–6.
46. Osmani AR. Technical efficiency of district hospitals in afghanistan: a data envelopment analysis approach. PSAKU Int J Int Res. (2012) 1:82–107. doi: 10.12778/235108618X15452373185048
47. Chaabouni S, Abednnadher C. Efficiency of public hospitals in Tunisia: a DEA with bootstrap application. Int J Behav Healthcare Res. (2012) 3:198–211. doi: 10.1504/IJBHR.2012.051380
48. Farzianpour F, Hosseini S, Amali T, Hosseini S, Hosseini SS. The evaluation of relative efficiency of teaching hospitals. Am J Appl Sci. (2012) 9:392. doi: 10.3844/ajassp.2012.392.398
49. Sheikhzadeh Y, Roudsari AV, Vahidi RG, Emrouznejad A, Dastgiri S. Public and private hospital services reform using data envelopment analysis to measure technical, scale, allocative, and cost efficiencies. Health Prom Persp. (2012) 2:28–41. doi: 10.5681/hpp.2012.004
50. Yusefzadeh H, Ghaderi H, Bagherzade R, Barouni M. The efficiency and budgeting of public hospitals: case study of Iran. Iran Red Crescent Med J. (2013) 15:393. doi: 10.5812/ircmj.4742
51. Ajlouni MM, Zyoud A, Jaber B, Shaheen H, Al-Natour M, Anshasi RJ. The relative efficiency of Jordanian public hospitals using data envelopment analysis and Pabon Lasso diagram. Global J Bus Res. (2013) 7:59–72.
52. Abou El-Seoud M. Measuring efficiency of reformed public hospitals in Saudi Arabia: an application of data envelopment analysis. Int J Econ Manag Sci. (2013) 2:44–53.
53. Rasool SA, Saboor A, Raashid M. Measuring efficiency of hospitals by DEA: an empirical evidence from Pakistan. Int J Publ Health Sci. (2014) 3:129–36. doi: 10.11591/.v3i2.4684
54. Torabipour A, Najarzadeh M, Mohammad A, Farzianpour F, Ghasemzadeh R. Hospitals productivity measurement using data envelopment analysis technique. Iran J Public Health. (2014) 43:1576.
55. Mehrtak M, Yusefzadeh H, Jaafaripooyan E. Pabon Lasso and Data Envelopment Analysis: a complementary approach to hospital performance measurement. Glob J Health Sci. (2014) 6:107. doi: 10.5539/gjhs.v6n4p107
56. Lotfi F, Kalhor R, Bastani P, Zadeh NS, Eslamian M, Dehghani MR, et al. Various indicators for the assessment of hospitals' performance status: differences and similarities. Iranian Red Crescent Med J. (2014) 16:12950. doi: 10.5812/ircmj.12950
57. Askari R, Farzianpour F, Goudarzi R, Shafii M, Sojaei S. Efficiency evaluation of hospitals affiliated with Yazd University of medical sciences using quantitative approach of data envelopment analysis in the year 2001 to 2011. Pensee J. (2014) 76:416–25.
58. Shetabi H, Mirbahari SQ, Nasiripour AA, Safi-keykaleh M, Mohammadi H, Esfandnia A, et al. Evaluating technical efficiency of Kermanshah city universities by means of data envelopment analysis model. Res J Med Sci. (2015) 9:53–7. doi: 10.36478/rjmsci.2015.53.57
59. Mahate A, Hamidi S. Frontier efficiency of hospitals in United Arab Emirates: an application of data envelopment analysis. J Hosp Admin. (2016) 5:7–16. doi: 10.5430/jha.v5n1p7
60. Kalhor R, Amini S, Sokhanvar M, Lotfi F, Sharifi M, Kakemam E. Factors affecting the technical efficiency of general hospitals in Iran: data envelopment analysis. J Egypt Publ Health Assoc. (2016) 91:20–5. doi: 10.1097/01.EPX.0000480717.13696.3c
61. Kakeman E, Forushani AR, Dargahi H. Technical efficiency of hospitals in Tehran, Iran. Iran J Public Health. (2016) 45:494.
62. Nabilou B, Yusefzadeh H, Rezapour A, Azar FEF, Safi PS, Asiabar AS, et al. The productivity and its barriers in public hospitals: case study of Iran. Med J Islam Repub Iran. (2016) 30:316.
63. Farzianpour F, Emami AH, Foroushani AR, Ghiasi A. Determining the technical efficiency of hospitals in tabriz city using data envelopment analysis for 2013-2014. Glob J Health Sci. (2016) 9:42. doi: 10.5539/gjhs.v9n5p42
64. Sultan WI, Crispim J. Evaluating the productive efficiency of Jordanian public hospitals. Int J Bus Manag. (2016) 12:68–83. doi: 10.5539/ijbm.v12n1p68
65. Helal SMA, Elimam HA. Measuring the efficiency of health services areas in Kingdom of Saudi Arabia using data envelopment analysis (DEA): a comparative study between the years 2014 and 2006. Int J Econ Finance. (2017) 9:172–84. doi: 10.5539/ijef.v9n4p172
66. Migdadi YKA-A, Al-Momani HSM. The operational determinants of hospitals inpatients departments efficiency in Jordan. Int J Operat Res. (2018) 32:1–23. doi: 10.1504/IJOR.2018.10012181
67. Kakemam E, Dargahi H. The health sector evolution plan and the technical efficiency of public hospitals in Iran. Iran J Public Health. (2019) 48:1681.
68. Alsabah A, Haghparast-Bidgoli H, Skordis J. Measuring the efficiency of public hospitals in Kuwait: a two-stage data envelopment analysis and a qualitative survey study. J Health Sci. (2020) 12:3. doi: 10.5539/gjhs.v12n3p121
69. Alwaked AA, Al-qalawi UR, Azaizeh SY. Efficiency of Jordanian public hospitals (2006–2015). J Pub Affairs. (2020) 22:e2383. doi: 10.1002/pa.2383
70. Cantor VJM, Poh KL. Integrated analysis of healthcare efficiency: a systematic review. J Med Syst. (2018) 42:1–23. doi: 10.1007/s10916-017-0848-7
71. Rahimi H. Khammar-nia M, Kavosi Z, Eslahi M. Indicators of hospital performance evaluation: a systematic review. Int J Hos Res. (2014) 3:199–208.
72. Blatnik P, Bojnec Š, Tušak M. Measuring efficiency of secondary healthcare providers in Slovenia. Open Med. (2017) 12:214–25. doi: 10.1515/med-2017-0031
73. Du T. Performance measurement of healthcare service and association discussion between quality and efficiency: Evidence from 31 provinces of mainland China. Sustainability. (2017) 10:74. doi: 10.3390/su10010074
74. World Health Organization. Eastern Mediterranean Region: Framework for Health Information Systems and Core Indicators for Monitoring Health Situation and Health System Performance. Geneva: World Health Organization (2016). Available online at: http://applications.emro.who.int/dsaf/EMROPUB_2016_EN_19169.pdf?ua=1&ua=1 (accessed October 21, 2022).
75. Pereira MA, Marques RC. The ‘Sustainable Public Health Index': What if public health and sustainable development are compatible? World Dev. (2022) 149:105708. doi: 10.1016/j.worlddev.2021.105708
76. Seyedin H, Afshari M, Isfahani P, Hasanzadeh E, Radinmanesh M, Bahador RC. The main factors of supplier-induced demand in health care: a qualitative study. J Educ Health Prom. (2021) 10:49. doi: 10.4103/jehp.jehp_68_20
77. Mosadeghrad AM, Afshari M. Quality management effects on operating theater's productivity: a participatory action research. TQM J. (2020) 33:882–95. doi: 10.1108/TQM-04-2020-0083
78. Pereira MA, Marques RC. Is sunshine regulation the new prescription to brighten up public hospitals in Portugal? Socioecon Plann Sci. (2022) 84:101219. doi: 10.1016/j.seps.2021.101219
79. Mosadeghrad AM, Afshari M. The impact of quality management on income of operating theatre in a hospital: brief report. Tehran Univ Med J. (2018) 75:768–72.
80. Goudarzi R, Pourreza A, Shokoohi M, Askari R, Mahdavi M, Moghri J. Technical efficiency of teaching hospitals in Iran: the use of stochastic frontier analysis, 1999–2011. Int J Health Policy Manage. (2014) 3:91. doi: 10.15171/ijhpm.2014.66
81. Kiadaliri AA, Jafari M, Gerdtham U-G. Frontier-based techniques in measuring hospital efficiency in Iran: a systematic review and meta-regression analysis. BMC Health Serv Res. (2013) 13:1–11. doi: 10.1186/1472-6963-13-312
82. Carey K. Hospital cost efficiency and system membership. J Health Care Org Prov Financ. (2003) 40:25–38. doi: 10.5034/inquiryjrnl_40.1.25
83. Dewar D, Lambrinos J. Does managed care more efficiently allocate resources to older patients in critical care settings? Cost Q. (2000) 6:18–37.
84. Morey RC, Ozcan YA, Retzlaff-Roberts DL, Fine DJ. Estimating the hospital-wide cost differentials warranted for teaching hospitals: an alternative to regression approaches. Med Care. (1995) 1:531–52. doi: 10.1097/00005650-199505000-00007
Keywords: efficiency, meta-analysis, hospital, eastern mediterranean countries, technical efficiency (TE)
Citation: Ravaghi H, Afshari M, Isfahani P, Mahboub-Ahari A and Bélorgeot VD (2023) Hospital efficiency in the eastern mediterranean region: A systematic review and meta-analysis. Front. Public Health 11:1085459. doi: 10.3389/fpubh.2023.1085459
Received: 31 October 2022; Accepted: 09 January 2023;
Published: 02 February 2023.
Edited by:
Diogo Ferreira, University of Lisbon, PortugalReviewed by:
Alexandre Nunes, University of Lisbon, PortugalMiguel Pereira, University of Porto, Portugal
Copyright © 2023 Ravaghi, Afshari, Isfahani, Mahboub-Ahari and Bélorgeot. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mahnaz Afshari,  mahnazafshar89@gmail.com
mahnazafshar89@gmail.com