 Ting Yuan
Ting Yuan Xiang Dong Li2†
Xiang Dong Li2† Ming Zhang
Ming Zhang- 1Department of Gynecology and Obstetrics Nursing, School of Nursing, Wannan Medical College, Wuhu, China
- 2Department of Gerontology, Yijishan Hospital, The First Affiliated Hospital of Wannan Medical College, Wuhu, China
- 3School of Innovation and Entrepreneurship, Wannan Medical College, Wuhu, China
- 4Department of Nursing, Yijishan Hospital, The First Affiliated Hospital of Wannan Medical College, Wuhu, China
- 5Department of Blood Purification Centre, Yijishan Hospital, The First Affiliated Hospital of Wannan Medical College, Wuhu, China
Objective: The pandemic of COVID-19 continues to challenge people's health worldwide. In the second year of the pandemic, adherence to COVID-19 preventive behavior is key to continuing efforts to overcome the epidemic. This study aims to assess the COVID-19-related knowledge, attitude, and prevention behavior (KAP) and electronic health literacy (eHealth literacy) among Anhui residents in China.
Methods: From January 30 to March 27, 2021, the cross-sectional study was performed among Anhui residents in China, including 16 cities. An online survey was adopted to assess KAP regarding COVID-19, and eHealth, involving a total of 2,122 citizens. Following informed consent, residents were recruited by convenience sampling. Frequencies and proportions were calculated. Additionally, Mann–Whitney U tests were used to analyze the variables. Independent predictors of preventive behavior of COVID-19 were ascertained using a multivariable logistic regression model.
Result: Residents demonstrated good knowledge, positive attitudes, acceptable practices, and good eHealth literacy. Online news and WeChat are the main health information resources. Citizens who had good knowledge, a positive attitude, good eHealth, and did not participate in the online lectures or training COVID-19 were more likely to take preventive measures. Those with poor health, who were male, did not have family members working in health care facilities, and did not work in a face-to-face environment were less likely to take precautions. Compared with a master's degree and above, participants with middle school education level and below took preventive behavior sometimes. Residents who browse the COVID-19 webpage <15 min weekly seldom took preventive actions.
Conclusion: The study showed that in the second year of the COVID-19 pandemic, Chinese residents had adequate knowledge of COVID-19, positive attitudes, appropriate preventive practices, and basic eHealth literacy. To prevent the rebound of the COVID-19 epidemic, the government and health agencies should inform citizens concerning which information channels or websites to use and assist the underprivileged population who lacks basic infrastructure. In addition, increasing the level of knowledge and attitude, enhancing eHealth literacy and the Health Belief Model (HBM), and implementing the Health Code were seen as ways to reinforce adherence to preventive behavior. Targeting men, implementing public awareness campaigns, community engagement strategies, and health education programs are recommended.
Introduction
The coronavirus disease 2019 (COVID-19) was first reported by officials in Wuhan, Hubei Province, China, in December 2019 (1). Deeply concerned by both the speed and severity of transmission, on March 11, 2020, the World Health Organization (WHO) declared COVID-19 as a pandemic (2). As of February 2, 2021, there were more than 102 million confirmed cases and 2.2 million deaths worldwide (3). The COVID-19 pandemic remains out of control globally (4).
The COVID-19 pandemic has led to the most serious health crisis of the 21st century (5).
People around the world experience higher rates of depression, anxiety, stress, and trauma due to the pandemic (6–8). In addition, public concern and fear may be raised after the loss of more than 2 million lives (9, 10).
To control COVID-19 transmissions, high-quality preventive measures and aggressive actions have been implemented by the government, including lockdowns, mask-wearing, handwashing, infected and contact case tracing, detection, and isolation. As a result of these, the global economy has deeply plunged into recession (11). Countless livelihoods were destroyed, millions of people forcibly displaced, the health system disrupted, and people pushed into poverty (12). Also, the lack of social contact and changes in lifestyle have led to an increase in smartphone addiction, internet addiction, alcohol and cannabis use (6, 13–15). Thus, the plight of vulnerable people has been exacerbated (16).
With the vaccine roll-out, public health advocated vaccination as a preferred method of protection. However, SARS-CoV-2 antibodies haven't been shown to confer durable immunity against reinfections up to now (17, 18). SARS-CoV-2 is an RNA virus. SARS-CoV-2 mutations occurred when RNA viruses encoded genes for surface glycoproteins, resulting in lessening the efficacy of vaccines (19). While a number of previous studies have found that vaccinations reduce participants' compliance with public health measures (20–22). Additionally, Italian studies showed that the behavior or attitudes toward the adoption of most protective behaviors on COVID-19 decreased over time (23, 24). Hence, maintaining compliance with preventive measures remains essential for pandemic control.
People infected with COVID-19 can present as either symptomatic or asymptomatic. Growing evidence suggests that asymptomatic carriers of the SARS-CoV-2 can also transmit the virus (25, 26). It is a challenge to control the disease's spread as asymptomatic individuals are more likely to be out rather than be isolated in their homes, which can pose a significant public health risk (27). Therefore, continual precautions should also be taken to prevent viral transmission.
During the global pandemic, it is reported that many individuals rely on the internet as their major source of health-related information (28). On the other hand, misinformation or conspiracy theories on the internet may interfere with or undermine adherence to prevention guidelines, potentially reducing public protective behaviors against the pandemic (29–32).
In response to the global COVID-19 pandemic, eHealth literacy is critical in disease control strategies, which help the public access health information quickly and accurately and avoid the spread of misinformation and conspiracy theories (33). Prior surveys found that higher scores of eHealth literacy were positively associated with physical exercise, a healthy diet, adherence to infection prevention and control measures, and protective behavioral practices (33–37).
Before herd immunity has been built up by vaccination, we will still coexist with SARS-CoV-2. Public health measures should also be carried out. However, the public precautions against COVID-19 in Nigeria, Ethiopia, Egypt, and China were unsatisfactory based on previous studies (4, 38–40). Understanding the predictors of practice against COVID-19 may aid in the resolution of COVID-19 future pandemics. Therefore, to address existing knowledge gaps, further analysis and research on the correlation between public adherence to preventive measures and knowledge, attitudes, and eHealth literacy during pandemic control is needed. Thus, this study aimed to: (1) evaluate the knowledge, attitude, and preventive practices toward COVID-19 of the Chinese population to date; (2) assess the eHealth literacy and their associations with preventive behaviors, (3) and identify the associated factors of individuals' prevention behaviors.
Methods and materials
A descriptive cross-sectional survey was performed among the general population of Anhui, China, from January 30 to March 27, 2021. The online self-report questionnaire was used to collect data to investigate knowledge, prevention behaviors, attitudes, and electronic health literacy (eHealth literacy) 1 year after the 2019 novel coronavirus outbreak. The access link was shared between acquaintances, friends, family members, and colleagues via WeChat. Participants were chosen through convenience sampling.
Ethical consideration
This research was approved by the Ethics Committee of the School of Nursing of Wannan Medical College (no. 20200012.10).
Participants
The study recruited 2,946 residents of Anhui, China. After eliminating the participants with missing or incomplete data, and those who met the exclusion criteria, a total of 2,122 samples were used in the surveys. The subjects consented to participate in this survey by volunteering to complete and submit the questionnaire. The participants could withdraw from the survey at any time.
The inclusion criteria for the participants were: (1) ≥18 years old; (2) community-dwelling Chinese residents; (3) willing to participate in the study; and (4) all the questionnaire response time≥180s. The exclusion criteria for the participants were: (1) diagnosed with a mental disorder; and (2) unable to understand the questions completely. The demographics of the study participants are presented in Table 1.
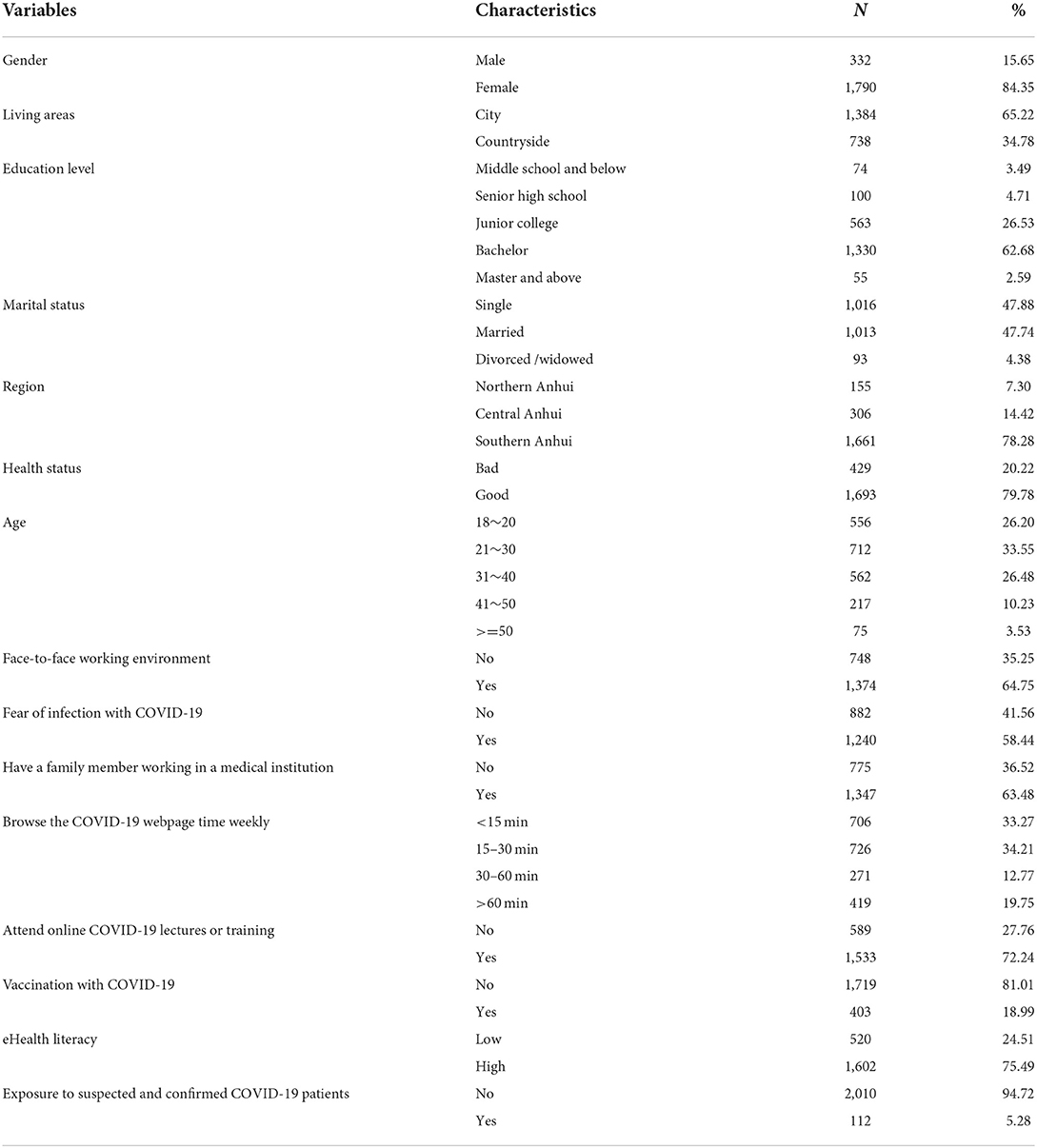
Table 1. Sample characteristics (N = 2,122).
Anhui Province is situated in the eastern part of China. The total area of the province is over 139,000 square kilometers, with a population of about 60 million. It is bounded by the provinces of Hubei, Jiangsu, Zhejiang, Jiangxi, Henan and Shandong. Sixteen cities in Anhui Province are defined by administrative divisions. Northern Anhui refers to the area north of the Huai River in Anhui, including the six cities of Suizhou, Huabei, Bengbu, Fuyang, Huainan, and Bozhou. Anhui central refers to the area north of the Yangtze River in Anhui Province, south of the Huai River, including the four cities of Hefei, Lu'an, Chuzhou, and Anqing. Southern Anhui refers to the area south of the Yangtze River in Anhui Province, including the six cities of Huangshan, Wuhu, Maanshan, Tongling, Xuancheng, and Chizhou.
Questionnaire development
The online survey is based on the eighth edition of the guidelines from the National Health Commission of China and some previous surveys (41–44).
Two public health researchers formed a panel to develop the questionnaire. The questionnaire was tested among 30 Chinese residents to assess clarity, readability, and length. In the pilot study, all the residents shown that the questions were easy to understand, and the length was appropriate and acceptable. These 30 Chinese residents did not participate in the actual survey.
Questionnaire
The present design of the self-administered structured questionnaire contains 48 questions and consists of five sections.
Section A recorded the participant's demographic data, including sex, living areas, education level, marital status, region, current health status, age, working directly with people face-to-face, fear of infection with COVID-19, family members who work in health care facilities, browsing the COVID-19 webpage time weekly, online COVID-19 lectures or training, vaccination with COVID-19, eHealth literacy, and exposure to suspected and confirmed COVID-19 patients.
Section B gathered information on participants' knowledge of COVID-19 by using 14 items. This section includes facts about COVID-19 (2 items), symptoms (3 items), transmission (4 items), and treatment and prevention (5 items). Participants were given three options: Yes, Not sure, and No (1 = correct answer; 0 = wrong answer or not sure).
The Cronbach 's alpha value for the knowledge section was 0.637.
Section C assessed the respondents' attitude to COVID-19 using 8 questions, and each question used a 5 point Likert scale ranging from 1 = Strongly disagree to 5 = Strongly Agree. The total scores range from 0 to 40, with higher scores indicating a better attitude.
The Cronbach 's alpha value for the attitude section was 0.835.
Section D consists of 12 questions to evaluate respondents' preventive behavior. A 5 point Likert scale (1 = never; 2 = seldom; 3 = sometimes; 4 = often; 5 = always) was used to assess each item. All the scores were summed up and ranged from 12 to 60. A higher score indicated the participant practices better prevention behavior.
The Cronbach's alpha value for the preventive behavior section was 0.886.
Section E is the eHealth Literacy Scale (eHeaLS) (45) mainly to discern the participants' eHealth literacy level. This scale included 8 items with a 5-point Likert scale ranging from 1 = Strongly disagree to 5 = Strongly Agree. The total score ranged from 8 to 40 points (cut-off score ≥ 32). A higher score indicated a better literacy level.
The Cronbach's alpha value for the eHealth literacy section was 0.947.
Statistical analysis
All analyses were carried out using IBM SPSS, version 21.0 (Chicago, IL, USA).
Frequencies and percentages are used to describe the distribution of categorical variables. Kolmogorov–Smirnov tests were used to verify that the data had a normal distribution. The Mann–Whitney U and Kruskal–Wallis tests were used to assess contributors to differences in knowledge, attitudes, and practices related to COVID-19. The correlations between variables were analyzed by Spearman's rank correlation test. Multinomial logistic regression was performed, to identify associated factors related to preventive behavior. A P-value < 0.05 was considered statistically significant.
Results
Sample characteristics
The sample characteristics of Anhui citizens and their eHealth literacy scores on COVID-19 were shown in Table 1. A total of 2,122 citizens (332 male and 1,790 female) in three regions of Anhui in China (155, 7.30% from the northern region, 306, 14.42% from the central region, and 1,661, 78.28% from the southern region) agreed to participate in the survey and complete the questionnaires assessing their knowledge, attitude, prevention behavior, and eHealth literacy regarding COVID-19 outbreaks. The response rate was 72.03%. The mean age of participants was 29.10 (SD 10.01) years, of which 26.20% were in aged 18–20 years old, 33.55% were aged 21–30 years old, 26.48% were aged 31–40 years old, and 10.23% were aged 41~50 years old. Of the sample, 65.22% were living in the city, 47.88% were single, 47.74% were married, and 4.38% were divorced or widowed. The education level of the sample comprised 3.49% middle school and below, 4.71% senior high school, 26.53% junior college, and 62.68% bachelor's. The majority (79.78%) of the participants were in good health; 64.75% were in a face-to-face working environment; 58.44% were afraid of infection with COVID-19; and 63.48% had family members who work in health care facilities. Every week, 33.27% of participants browsed the COVID-19 webpage <15 min, 34.21% for 15–30 min, and 19.75% for more than an hour.72.24% of participants reported having online COVID-19 lectures or training, 18.99% had injected the COVID-19 vaccine, 75.49% were at a high eHealth literacy level, and 5.28% had been exposed to suspected or confirmed COVID-19 patients (Table 1).
Anhui citizens are more likely to seek information about COVID-19 through online news, WeChat, friends or colleagues, TikTok, television, and information published by the government or health board (Figure 1). The mean (SD) scores of knowledge, preventive behavior, attitude, and eHealth literacy were 10.78 (1.89), 52.25 (8.27), 34.09 (4.24), and 34.23 (5.61), respectively.
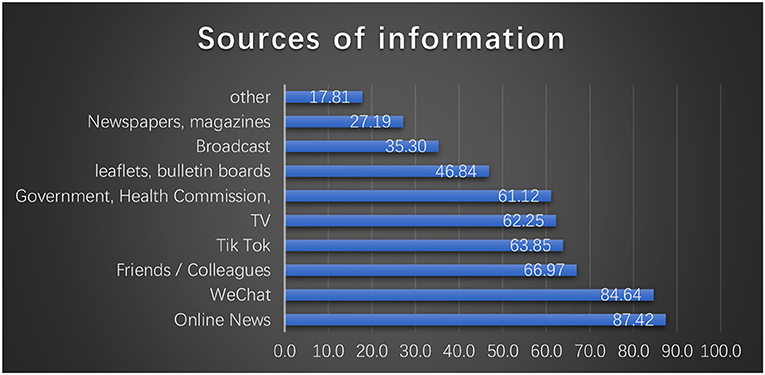
Figure 1. Source of COVID-19 information reported by citizens.
Knowledge of citizens about COVID-19
Most citizens were aware of the knowledge, including facts, symptoms, transmission, treatment, and prevention of COVID-19, as shown in Table 2. However, 35.06% of participants were not aware of the coronavirus that belongs to the β genus of coronaviruses. About 43.26% of participants held the misconception that people infected with COVID-19 were less likely to experience nasal congestion, runny nose, and sneezing with symptoms different from those of the common cold. Of the samples, 65.22% incorrectly believed that only people who are older or have underlying medical conditions will develop severe cases. 28.28% of citizens incorrectly responded that not all people are susceptible to COVID-19. Over 70% of citizens incorrectly believed that residents could wear general masks to prevent COVID-19 infection.
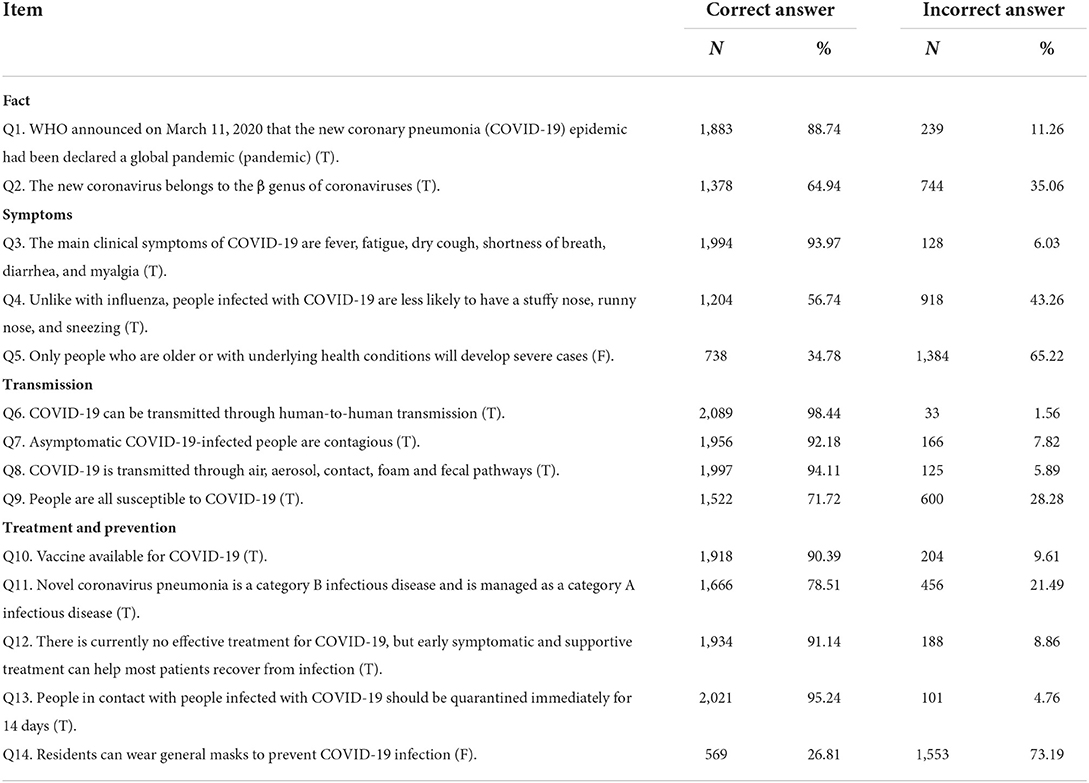
Table 2. Level of knowledge of COVID-19 (N = 2,122).
The results of the knowledge score were significantly different in gender (Zmwu= −7.77, P < 0.001), living areas (Zmwu= −10.51, P < 0.001), family members who work in health care facilities (Zmwu= −10.89, P < 0.001), online COVID-19 lectures or training (Zmwu= −12.94, P < 0.001), vaccination with COVID-19 (Zmwu = −8.75, P < 0.001), eHealth literacy (Zmwu = −10.21, P < 0.001), working directly with people face-to-face (Zmwu = −15.16, P < 0.001), exposure to suspected and confirmed COVID-19 patients (Zmwu = −4.34, P < 0.001), age ( = 189.79, P < 0.001), education level ( = 50.11, P < 0.001), marital status ( = 123.61, P < 0.001), browsing the COVID-19 webpage time weekly ( = 53.40, P < 0.001), and region of Anhui ( = 101.33, P < 0.001) (Table 3).
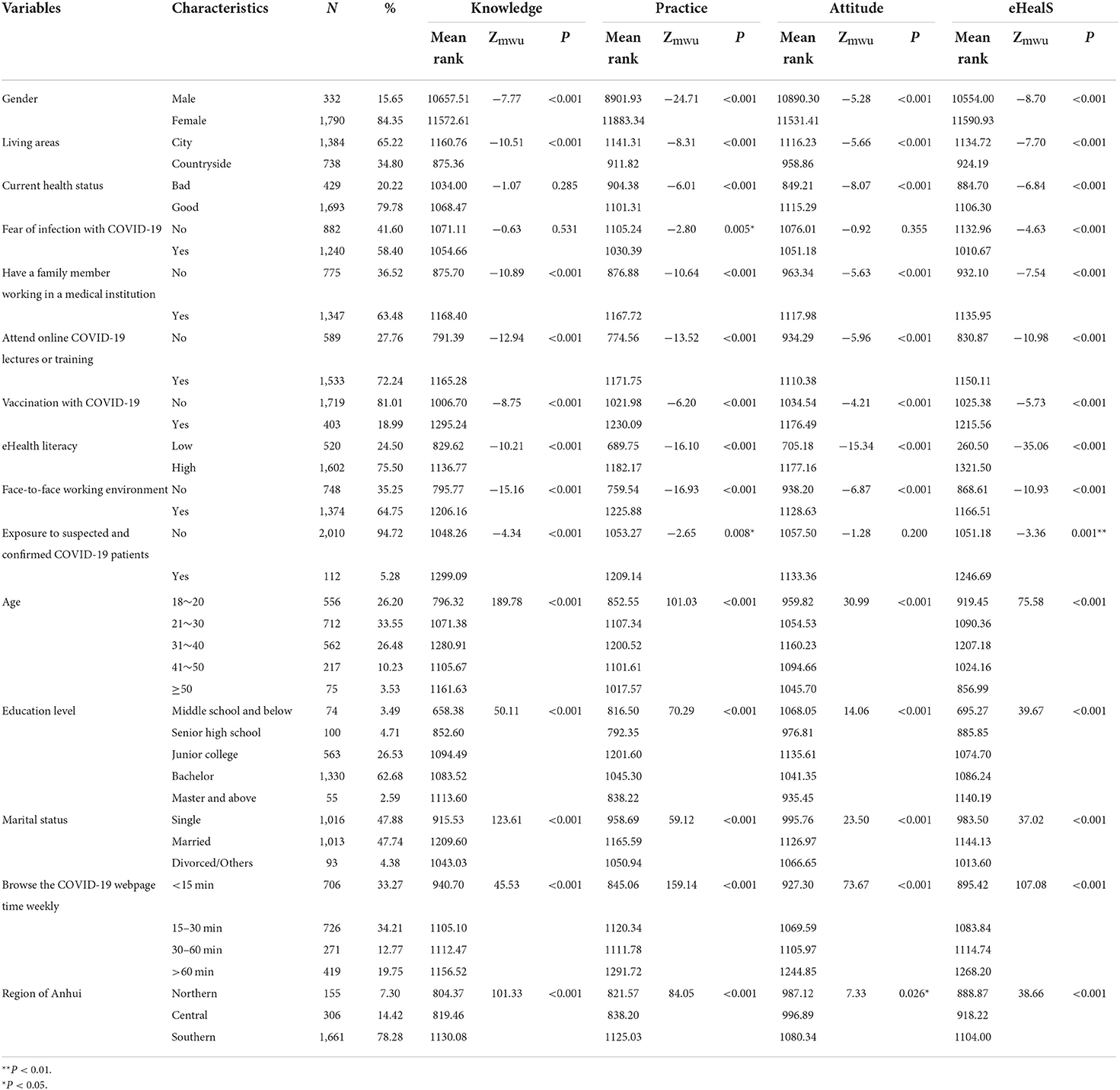
Table 3. Level of knowledge, attitude, and prevention behavior according to demographic characteristics (N = 2,122).
The attitude of citizens toward COVID-19
Nearly 80–90% of the participants agreed that injecting the COVID-19 vaccines, staying at home during the Spring Festival, and not returning to their hometown without necessity, strengthening self-protection, and health education would drive down transmission. Only 52.16% of the population agreed that the targets for terminating the coronavirus pandemic would be achieved this year. Active cooperation with the government's epidemic prevention and control work has been supported by almost all citizens (96.52%), although the epidemic prevention and control measures would affect their work and daily life. The majority of participants had an acceptable attitude (94.07%) that SARS-CoV-2 nucleic acid testing should be performed for those who had visited a high-risk county (district) in COVID-19 within 14 days (Table 4).
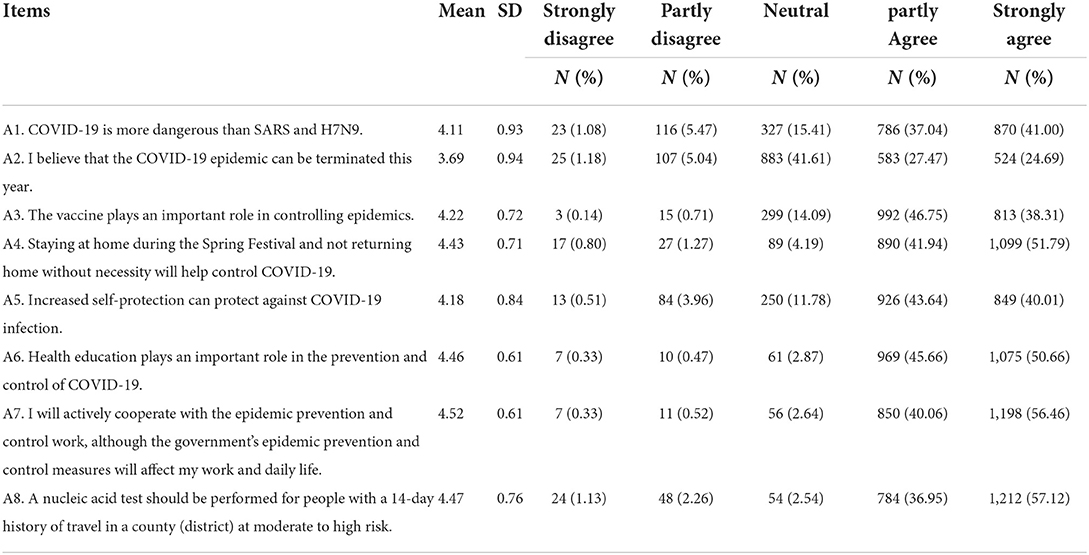
Table 4. Attitude toward COVID-19 (N = 2,122).
There was a significant difference in attitude based on gender (Zmwu= −5.28, P < 0.001), living areas (Zmwu = −5.66, P < 0.001), health status (Zmwu = 8.07, P < 0.001), family members who work in health care facilities (Zmwu = −5.63, P < 0.001), online COVID-19 lectures or training (Zmwu = −5.96, P < 0.001), vaccination with COVID-19 (Zmwu = −4.21, P < 0.001), eHealth literacy (Zmwu = −15.34, P < 0.001), working directly with people face-to-face (Zmwu = −6.87, P < 0.001), age ( = 30.99, P < 0.001), education level ( = 14.06, P < 0.001), marital status ( = 23.50, P < 0.001), browsing the COVID-19 webpage time weekly ( = 73.67, P < 0.001), and region of Anhui ( = 7.33, P < 0.05) (Table 3).
eHealth literacy of Anhui citizens
Approximately 75.50 % of participants had a high level of eHealth literacy. There was a significant difference in eHealth literacy according to gender (Zmwu = −8.70, P < 0.001), living areas (Zmwu = −7.70, P < 0.001), health status (Zmwu = −6.84, P < 0.001), fear of infection with COVID-19 (Zmwu = −4.63, P < 0.001), family members who work in health care facilities (Zmwu = −7.54, P < 0.001), online COVID-19 lectures or training (Zmwu = −10.98, P < 0.001), vaccination with COVID-19 (Zmwu = −5.73, P < 0.001), eHealth literacy (Zmwu = −35.06, P < 0.001), work with people face-to-face directly (Zmwu = −10.93, P < 0.001), exposure to suspected and confirmed COVID-19 patients (Zmwu = −3.36, P < 0.01), age ( = 75.58, P < 0.001), education level ( = 39.67, P < 0.001), marital status ( = 37.02, P < 0.001), browse the COVID-19 webpage time weekly ( = 107.08, P < 0.001), and region of Anhui ( = 38.66, P < 0.001) (Table 3).
Prevention behavior of citizens about COVID-19
The table shows that the majority of citizens were able to implement preventive behaviors. The responses to the preventive behavior questions reported that 14.56, 13.86, 13.43, 12.54, 11.97, and 11.97% of the citizens had never or rarely performed the items 1, 3, 4, 6, 11, and 12, respectively (Table 5).
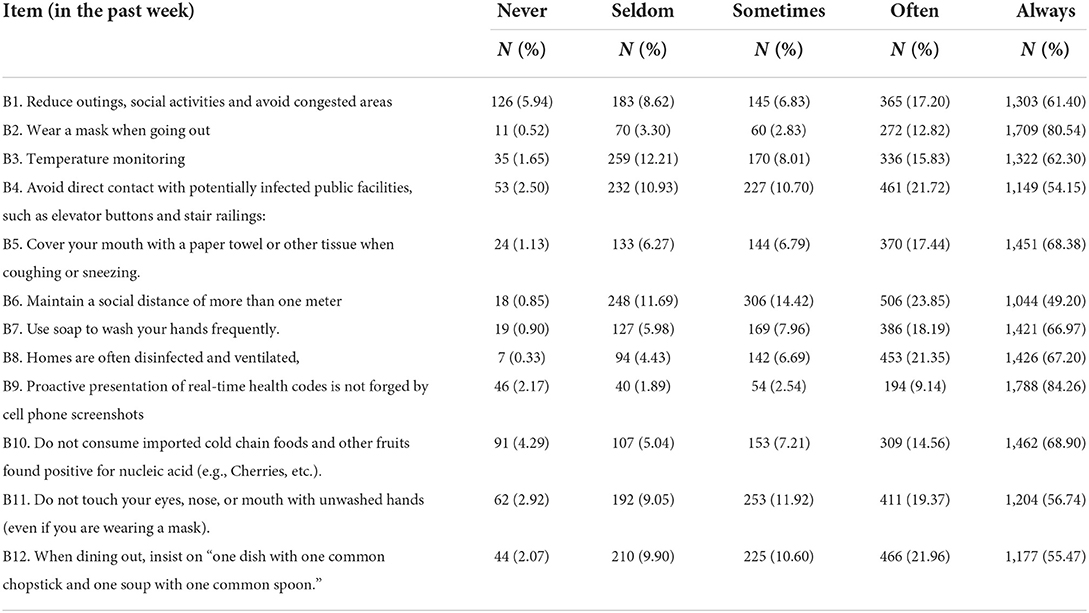
Table 5. Level of preventive behavior for COVID-19 (N = 2,122).
The results of the prevention behavior score differed significantly by gender (Zmwu = −24.71, P < 0.001), living areas (Zmwu = −8.31, P < 0.001), health status (Zmwu = −6.01, P < 0.001), fear of infection with COVID-19 (Zmwu = −2.80, P < 0.001), family members who work in health care facilities (Zmwu = −10.64, P < 0.001), attending online COVID-19 lectures or training (Zmwu = −13.52, P < 0.001), vaccination with COVID-19 (Zmwu = −6.20, P < 0.001), eHealth literacy (Zmwu = −16.10, P < 0.001), working with people face-to-face directly (Zmwu = −16.93, P < 0.001), exposure to suspected and confirmed COVID-19 patients (Zmwu = −2.65, P < 0.01), age ( = 101.03, P < 0.001), education level ( = 70.29, P < 0.001), marital status ( = 59.12, P < 0.001), browsing the COVID-19 webpage time weekly ( = 159.14, P < 0.001), and region of Anhui ( = 84.05, P < 0.001) (Table 3).
Influencing factors on preventive behavior for COVID-19
The category classification of preventive behaviors was used as the dependent variable, and a multivariate logistic regression analysis was conducted with the significant factors in the univariate analysis as independent variables.
In the multiple logistic regression analysis, the scores of preventive behaviors were divided into 3 categories, namely rarely group (score < 60), sometimes group (60 ≤ score < 80), and always group (score ≥ 80). The third group (always) was used as the reference group.
Compared with the group of citizens that always exhibit preventive behaviors, citizens who had a poor attitude (OR = 0.782, P < 0.001), had low eHealth literacy (OR = 0.875, P < 0.001), male (OR = 3.170, P < 0.001), have a worse health status (OR = 2.417, P < 0.05), do not have family members working in health care facilities (OR = 1.882, P < 0.05), and do not work in a face-to-face environment (OR = 2.598, P < 0.05) rarely exhibit preventive behaviors. Meanwhile, those who sometimes took preventive behaviors were more likely to be lacking in knowledge on COVID-19 (OR = 0.892, P < 0.05), to have a negative attitude toward COVID-19 (OR = 0.872, P < 0.001), to have a low eHealth literacy (OR = 0.916, P < 0.001), to be male (OR = 1.490, P < 0.05), to have a poor health status (OR = 1.393, P < 0.05), to have not participated in COVID-19 lectures or training (OR = 0.710, P < 0.05), to not work in a face-to-face environment (OR = 2.598, P < 0.001), to have a junior high school education level or less (OR = 0.382, P < 0.05), and to browse the COVID-19 webpage time < 15 min weekly (OR = 1.511, P < 0.05), than those were in the always group (Table 6).
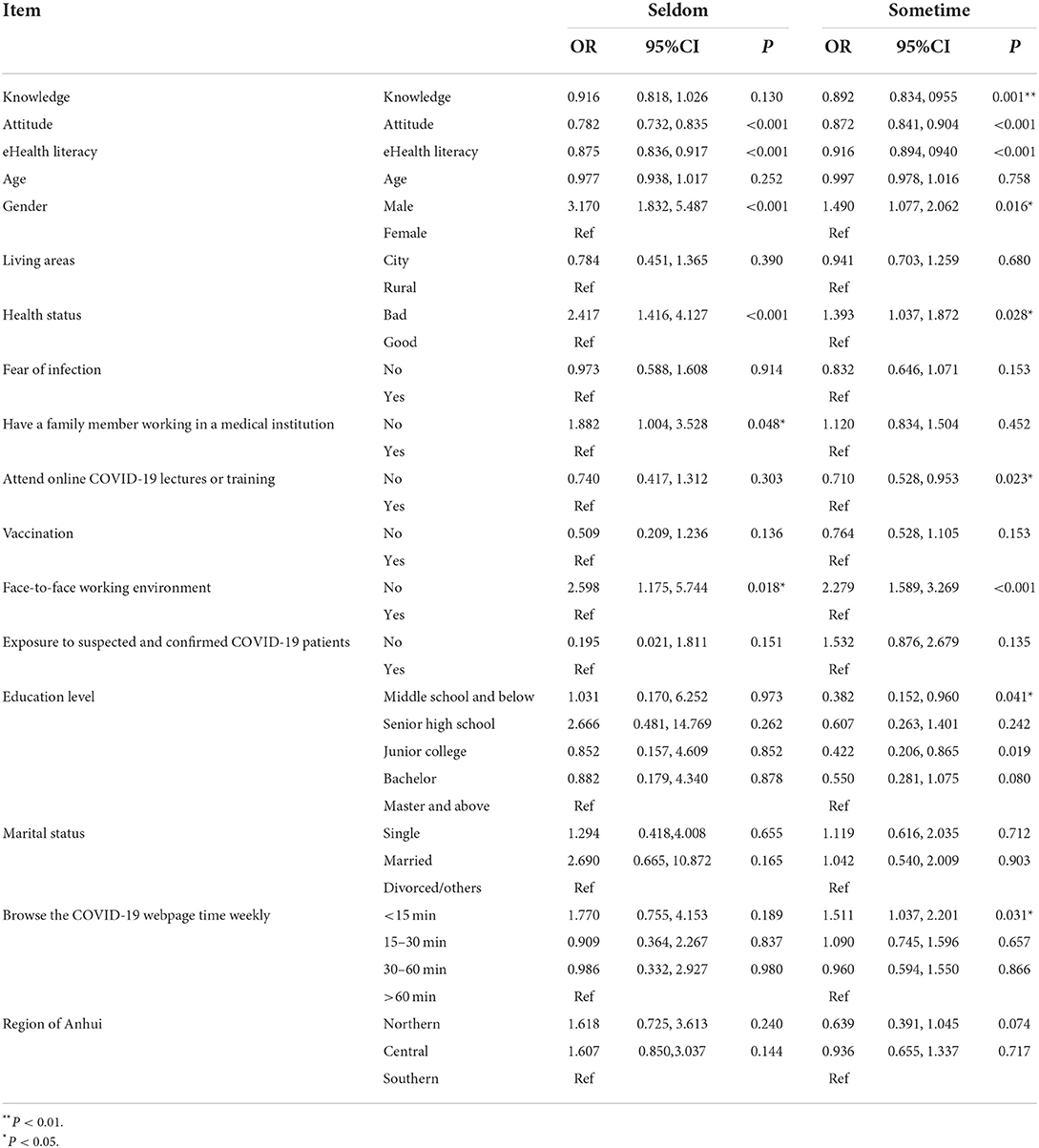
Table 6. Multinomial logistic regression analysis of the factors affecting preventive behavior level toward COVID-19 among the nursing students (N = 2,122).
Discussion
Although COVID-19 has shifted from a pandemic response model to coexistence with the virus, ongoing public health measures are essential. This is because some countries and regions still face localized spikes or localized recurrences of large numbers of confirmed and fatal cases. Moreover, in the second year of a COVID-19 pandemic, following prevention guidelines and directions may be difficult due to pandemic fatigue. Therefore, it remains important to understand citizens' preventive behaviors for COVID-19.
In China, online news (87.4%) and WeChat (84.6%) are today's important health information resources. In North-Central Nigeria, the internet, social media (55.7%), and television (27.5%) were the main information resources. According to the Office for National Statistics, in the UK, 59% of females and 50% of males have accessed health-related information online within 3 months (46). The Internet and social media are broadly recognized as a health communication and education instrument for transforming medical care and public health in Italy (47–49). Internet-based health information and knowledge may be a valuable resource for health-behavior interventions and programs (50, 51). Following such research, the means of information dissemination should be utilized to improve COVID-19 epidemic stewardship. A wide range of interventions could be designed to help individuals access COVID-19 information by developing public eHealth literacy, training health information professionals to provide sustained conversation services online, and disseminating quality health information to the general population (48, 52). The government and health agencies should make an effort to inform citizens about which information channels or websites to use and to provide them with specific assistance (53). This will prevent citizens from being misled by misinformation. Additionally, another study conducted in Ethiopia showed that public information is primarily obtained through television and radio (72.6%) (54). During such tough times, it is still necessary to assist the underprivileged population who lack access to information on official online platforms due to the lack of basic infrastructure.
In this study, participants demonstrated a high level of knowledge about SARS-CoV-2 infection, positive attitudes, acceptable practices, and a good level of eHealth literacy.
Through the combined efforts of government authorities and healthcare workers, 1 year since the COVID-19 pandemic, the knowledge and awareness of controlling the spread of infection has improved. Our results show that the participants had sufficient knowledge regarding symptoms, transmission, and treatment of COVID-19. However, lack of knowledge about virus types (35.06%), virus management classifications (21.49%), susceptible populations (28.28%), populations developing severe cases (65.22%), similarities and differences between influenza and COVID-19 (43.26%), and the choice of type of mask to wear (73.19%), may still be widespread.
Concerning attitudes, the results of the study showed that most of the participants had positive attitudes and were actively cooperating with the government in COVID-19 prevention. However, nearly half of the participants lack confidence in epidemic control and termination. This finding was contrary to the study conducted among the community health workers in Nepal (55). A total of ~85.06% of respondents stated that COVID-19 vaccines can protect recipients from infection by building up immunity. Thus, perceived COVID-19 severity and vaccine benefits help the government to deal with vaccine hesitancy and achieve high vaccination coverage rates, which was supported by a study in Hong Kong (56).
Factors influencing the residents' practice of COVID-19 were assessed. Adequate knowledge and positive attitudes are the driving forces for more feasible and effective behavior, which are supported by the principle of the KAP model (57–59). The eHealth literacy score showed a positive independent association with adherence to protective behaviors. Similar findings have been demonstrated in previous studies that participants with lower eHealth literacy scores were less likely to seek health information (60, 61). Some studies have reported the relationship between eHealth literacy scores and health outcomes. Minh H. Nguyen et al. noted that the fear of COVID-19 can be mitigated and health-related quality of life can be improved as a result of eHealth literacy (34). The Australian survey showed that respondents who received higher eHealth literacy scores would perform “critically appraisal” information on the Internet (62).
A study by Lawrence An, USA, found that people with higher CoV-eHealth literacy scores had a greater rejection of conspiracy theories (37). Strengthening eHealth literacy is seen as a way to curb the spread of the pandemic and improve the behavior of the general population.
It was observed that male respondents adopted fewer safety practices than females. The studies from Iran, and Saudi Arabia also exhibit a similar result (34, 63). Much of the research showed that females had a higher rate of compliance with preventive behaviors (37, 62). Also, published literatures show that women are more prone to having varied fears related to COVID-19, such as health, economic, and political crises caused by pandemics, and have higher COVID-19 stress exposure (64–69). Individuals who perceived the severity of COVID-19 were more likely to comply with COVID-19 prevention measures (53). Moreover, previous studies found that men are more likely to engage in risk-taking behavior (59, 70). Therefore, targeting men, implementing public awareness campaigns, community engagement strategies, and health education programs are recommended (59, 71).
The study found that healthier residents were more likely to take preventive precautions than those in poorer health. Evidence to support the conclusion has been drawn from research on health belief models (HBM) and preventive health behavior (72, 73). HBM is a theoretical model used to guide health promotion, explain and predict health behaviors, and disease prevention. Based on the Health Belief Model (HBM), in order to prevent infection with COVID-19, the intention to carry out preventive activities will increase by the healthier person. This could imply that increased awareness of COVID-19 information may predispose people to take effective precautionary measures.
As for family members of health care workers (HCWs), the practice score of the participants was reported to be higher. This was supported by previous studies that showed good infection control practices were observed among HCWs in relation to COVID-19 (74). HCWs may have a direct effect on the practices of family members, and, consequently, the citizens adopt more proactive preventive measures.
The current survey found that despite not having been trained or lectured on COVID-19, participants had a higher level of practice than expected. The study also showed that citizens with a middle school education or less took more protective measures than those with a master's degree or higher. The main reason for this was that these adults with lower secondary education and no training or lectures might maintain social lives through manual labor. Also, the prevalence of COVID-19 infections in China and worldwide has been reported daily in the media, making people feel more threatened about being infected. Under these circumstances, they may fear being quarantined and isolated due to infection, which could result in a loss of income and productivity. In addition, as the government encourages companies and social organizations to undertake health management, the growing health concern has created a more favorable environment for conducting preventive behavior. Individuals with a green health code are free in public spaces, whereas those with a yellow or red code are barred from public places, public transportation stations, and residential areas by security guards and gatekeepers (43, 44). The implementation of the Health Code has created an efficient way to respond to the COVID-19 pandemic (75).
This study's finding showed that participants in face-to-face work environments exhibit better practice. According to previous research, people who work face-to-face experience more financial threats, especially those with caregiving responsibilities (76). And for social-health personnel (such as doctors and nurses), professional face-to-face activity had to be continued, because it was deemed essential. For occupational reasons, employees who work in a face-to-face modality may be potentially exposed to COVID-19. Despite the high risks faced by individuals, they may place great emphasis on transmission risk mitigation, so the level of adherence to COVID-19 effective preventive measures was high. Another study showed that Latino and black frontline workers in high-risk occupations were less likely to take adequate COVID-19 protection (77). These differences may be related to sociodemographic conditions, countries' response patterns, and cultural differences.
Based on the findings of this study, a lower practice score was observed in people who spent time on the COVID-19-related media for <15 min, compared with people who consumed more than 1 h. It may be because the fact that COVID-19 information may cause intense concern about infection, which would increase protective behavior (78). However, another study (79) in the US noted that increased exposure to social media to learn about COVID-19 increased mental distress, and reduced the likelihood of compliance with health guidance measures as a result. This discrepancy might be due to higher information overload in Western populations (80). Multiple studies have shown that misinformation and conspiracy theories could reduce health behaviors. Therefore, evidence-based information should be disseminated by the public health authorities, such as the governments, the Centers for Disease Control, and the World Health Organization. It is also important to increase individuals' eHealth literacy, which helps them to examine information credibility.
Strengthen and limitations of the study
To our knowledge, this was one of the first studies on empirical evidence on the COVID-19 related knowledge, attitudes, and practices (KAP) and eHealth literacy in the second year of the pandemic of residents in China.
This study had some limitations. First, the online study was self-reported, which could exist the recall bias and social desirability bias. Thus, face-to-face interviews among vulnerable populations (e.g., older adults) who lack basic infrastructure also deserve special study. Second, due to the cross-sectional survey conducted in one province in China, the generalizability might be compromised, and causal relationships cannot be established. Third, the participants were overwhelmingly composed of females. Therefore, this result may be limited to a lack of sufficient male cases.
Conclusions
In this study, the residents in China acquired good knowledge, formed positive attitudes, performed the appropriate preventive behavior toward COVID-19 and had basic eHealth literacy. It is vital for the government and health agencies to inform citizens concerning which information channels or websites to use and assist the underprivileged population who lack basic infrastructure. In particular, the information on the type of mask to wear and populations developing severe cases still needs to be reinforced by the Chinese National Health Council and the governments.
Our findings suggest that good knowledge, positive attitudes, and enhanced eHealth literacy were seen as a way to improve the behavior of the population. Implementing public awareness campaigns, community engagement strategies, and health education programs that target the male gender may improve men's preventive behavior. Based on HBM, people in good health, family members with HCW, being in a face-to-face work environment, and viewing COVID-19-related information for a long time may predispose people to take effective precautionary measures. The implementation of the Health Code may facilitate more protective measures for those with a middle school education or less, and those who have not received COVID-19 training or lectures.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
TY, HL, and XDL conceived the study and performed the statistical analysis. MZ, XBT, and SJX carried out the literature searches. XBT, SJX, and HL distributed the online questionnaire and extracted the data. XBT assessed the study quality. TY and XDL wrote the manuscript. TY, HL, MZ, XDL, XBT, and SJX revised the manuscript. All authors contributed to the concept of this study. All authors read the published version of the manuscript and gave their consent.
Funding
This work was supported by Anhui Provincial Department of Education College Outstanding Talent Cultivation Funding Project, No. gxgwfx2019032; the Teaching Quality and Teaching Reform Project of Anhui Provincial Department of Education, No. 2020jyxm2090; and Humanities and Social Sciences Research Project of Colleges and Universities in Anhui Province (SK2018A0199).
Acknowledgments
We appreciate all the participants for their cooperation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
PHEIC, public health emergency; HCWs, health care workers; eHeals, the eHealth Literacy Scale; KAP, knowledge, attitudes and practices.
References
1. Alsoufi A, Alsuyihili A, Msherghi A, Elhadi A, Atiyah H, Ashini A, et al., Impact of the COVID-19 pandemic on medical education: medical students' knowledge, attitudes, and practices regarding electronic learning. PLoS ONE. (2020) 15:e0242905. doi: 10.1371/journal.pone.0242905
2. World Health Orgnization. Timeline: WHO's COVID-19 Response. (2020). Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/interactive-timeline#event-72 (accessed March 11, 2020).
3. World Health Orgnization. COVID-19 Weekly Epidemiological Update. (2021). Available online at: https://www.who.int/publications/m/item/weekly-epidemiological-update-$-$2-february-2021 (accessed February 2, 2021).
4. Yuan J, Cao B, Zhang C, Chan PS, Xin M, Fang Y, et al., Changes in compliance with personal preventive measures and mental health status among chinese factory workers during the COVID-19 pandemic: an observational prospective cohort study. Front Public Health. (2022) 10:831456. doi: 10.3389/fpubh.2022.831456
5. Pollard CA, Morran MP, Nestor-Kalinoski AL. The COVID-19 pandemic: a global health crisis. Physiol Genomics. (2020) 52:549–57. doi: 10.1152/physiolgenomics.00089.2020
6. Jones EAK, Mitra AK, Bhuiyan AR. Impact of COVID-19 on mental health in adolescents: a systematic review. Int J Environ Res Public Health. (2021) 18:2470. doi: 10.3390/ijerph18052470
7. Riedel B, Horen SR, Reynolds A, Hamidian Jahromi A. Mental health disorders in nurses during the COVID-19 pandemic: implications and coping strategies. Front Public Health. (2021) 9:707358. doi: 10.3389/fpubh.2021.707358
8. Alshammari MA, Alshammari TK. COVID-19: a new challenge for mental health and policymaking recommendations. J Infect Public Health. (2021) 14:1065–8. doi: 10.1016/j.jiph.2021.05.020
9. Fellendorf FT, Reininghaus EZ, Ratzenhofer M, Lenger M, Maget A, Platzer M, et al. COVID-19-related fears and information frequency predict sleep behavior in bipolar disorder. Brain Behav. (2021) 11:e02182. doi: 10.1002/brb3.2182
10. French MT, Mortensen K, Timming AR. Psychological distress and coronavirus fears during the initial phase of the COVID-19 pandemic in the United States. J Ment Health Policy Econ. (2020) 23:93–100.
11. Açikgöz Ö, Günay A. Short-term impact of the Covid-19 pandemic on the global and Turkish economy. Turk J Med Sci. (2021) 51:3182–93. doi: 10.3906/sag-2106-271
12. Onyeaka H, Anumudu CK, Al-Sharify ZT, Egele-Godswill E, Mbaegbu P. COVID-19 pandemic: a review of the global lockdown and its far-reaching effects. Sci Prog. (2021) 104:368504211019854. doi: 10.1177/00368504211019854
13. Simon FAJ, Schenk M, Palm D, Faltraco F, Thome J. The collateral damage of the COVID-19 outbreak on mental health and psychiatry. Int J Environ Res Public Health. (2021) 18:4440. doi: 10.3390/ijerph18094440
14. Li YY, Sun Y, Meng SQ, Bao YP, Cheng JL, Chang XW, et al. Internet addiction increases in the general population during COVID-19: evidence from China. Am J Addict. (2021) 30:389–97. doi: 10.1111/ajad.13156
15. Caponnetto P, Inguscio L, Valeri S, Maglia M, Polosa R, Lai C, et al. Smartphone addiction across the lifetime during Italian lockdown for COVID-19. J Addict Dis. (2021) 39:441–9. doi: 10.1080/10550887.2021.1889751
16. Wei X, Li L, Zhang F. The impact of the COVID-19 pandemic on socio-economic and sustainability. Environ Sci Pollut Res Int. (2021) 28:68251–60. doi: 10.1007/s11356-021-14986-0
17. Hansen CH, Michlmayr D, Gubbels SM, Mølbak K, Ethelberg S. Assessment of protection against reinfection with SARS-CoV-2 among 4 million PCR-tested individuals in Denmark in 2020: a population-level observational study. Lancet. (2021) 397:1204–12. doi: 10.1016/S0140-6736(21)00575-4
18. Yahav D, Yelin D, Eckerle I, Eberhardt CS, Wang J, Cao B, et al. Definitions for coronavirus disease 2019 reinfection, relapse and PCR re-positivity. Clin Microbiol Infect. (2021) 27:315–8. doi: 10.1016/j.cmi.2020.11.028
19. Francis AI, Ghany S, Gilkes T, Umakanthan S. Review of COVID-19 vaccine subtypes, efficacy and geographical distributions. Postgrad Med J. (2022) 98:389–94. doi: 10.1136/postgradmedj-2021-140654
20. Hossain ME, Islam MS, Rana MJ, Amin MR, Rokonuzzaman M, Chakrobortty S, et al. Scaling the changes in lifestyle, attitude, and behavioral patterns among COVID-19 vaccinated people: insights from Bangladesh. Hum Vaccin Immunother,. (2022) 18:2022920. doi: 10.1080/21645515.2021.2022920
21. Si R, Yao Y, Zhang X, Lu Q, Aziz N. Investigating the Links Between Vaccination Against COVID-19 and public attitudes toward protective countermeasures: implications for public health. Front Public Health. (2021) 9:702699. doi: 10.3389/fpubh.2021.702699
22. Zhang N, Liu X, Jin T, Zhao P, Miao D, Lei H, et al. Weakening personal protective behavior by Chinese university students after COVID-19 vaccination. Build Environ. (2021) 206:108367. doi: 10.1016/j.buildenv.2021.108367
23. Grano C, Singh Solorzano C, Di Pucchio A. Predictors of protective behaviours during the Italian Covid-19 pandemic: an application of protection motivation theory. Psychol Health. (2022) 1–21. doi: 10.3390/ijerph191610153. [Epub ahead of print].
24. Grano C, Singh Solorzano C, Di Pucchio A. Changes in behaviors and attitudes in response to COVID-19 pandemic and vaccination in healthcare workers and university students in Italy. Vaccines. (2021) 9:1276. doi: 10.3390/vaccines9111276
25. Nogrady, B., What the data say about asymptomatic COVID infections. Nature. (2020) 587:534–5. doi: 10.1038/d41586-020-03141-3
26. Johansson MA, Quandelacy TM, Kada S, Prasad PV, Steele M, Brooks JT, et al. SARS-CoV-2 transmission from people without COVID-19 symptoms. JAMA Netw Open. (2021) 4:e2035057. doi: 10.1001/jamanetworkopen.2020.35057
27. Bi Q, Lessler J, Eckerle I, Lauer SA, Kaiser L, Vuilleumier N, et al. Insights into household transmission of SARS-CoV-2 from a population-based serological survey. Nat Commun. (2021) 12:3643. doi: 10.1101/2020.11.04.20225573
28. Davidsson P, Thoresson A. Survey on Swedes' Internet Habits. (2021). Available online at: https://internetstiftelsen.se/docs/Svenskarna_och_internet_2017.pdf (accessed August 25, 2021).
29. Cinelli M, Quattrociocchi W, Galeazzi A, Valensise CM, Brugnoli E, Schmidt AL, et al. The COVID-19 social media infodemic. Sci Rep. (2020) 10:16598. doi: 10.1038/s41598-020-73510-5
30. Freeman D, Waite F, Rosebrock L, Petit A, Causier C, East A, et al. Coronavirus conspiracy beliefs, mistrust, and compliance with government guidelines in England. Psychol Med. (2022) 52:251–63. doi: 10.1017/S0033291720001890
31. Tangcharoensathien V, Calleja N, Nguyen T, Purnat T, D'Agostino M, Garcia-Saiso S, et al. Framework for managing the COVID-19 infodemic: methods and results of an online, crowdsourced WHO technical consultation. J Med Internet Res. (2020) 22:e19659. doi: 10.2196/19659
32. Tasnim S, Hossain MM, Mazumder H. Impact of rumors and misinformation on COVID-19 in social media. J Prev Med Public Health. (2020) 53:171–4. doi: 10.3961/jpmph.20.094
33. Guo Z, Zhao SZ, Guo N, Wu Y, Weng X, Wong JY, et al. Socioeconomic disparities in ehealth literacy and preventive behaviors during the COVID-19 pandemic in Hong Kong: cross-sectional study. J Med Internet Res. (2021) 23:e24577. doi: 10.2196/24577
34. Nguyen MH, Pham TTM, Nguyen KT, Nguyen YH, Tran TV, Do BN, et al. Negative impact of fear of COVID-19 on health-related quality of life was modified by health literacy, eHealth literacy, and digital healthy diet literacy: a multi-hospital survey. Int J Environ Res Public Health. (2021) 18:4929. doi: 10.3390/ijerph18094929
35. Britt RK, Collins WB, Wilson K, Linnemeier G, Englebert AM. eHealth literacy and health behaviors affecting modern college students: a pilot study of issues identified by the american college health association. J Med Internet Res. (2017) 19:e392. doi: 10.2196/jmir.3100
36. Do BN, Tran TV, Phan DT, Nguyen HC, Nguyen TTP, Nguyen HC, et al. Health literacy, ehealth literacy, adherence to infection prevention and control procedures, lifestyle changes, and suspected COVID-19 symptoms among health care workers during lockdown: online survey. J Med Internet Res. (2020) 22:e22894. doi: 10.2196/22894
37. An L, Bacon E, Hawley S, Yang P, Russell D, Huffman S, et al. Relationship between coronavirus-related ehealth literacy and COVID-19 knowledge, attitudes, and practices among US adults: web-based survey study. J Med Internet Res. (2021) 23:e25042. doi: 10.2196/25042
38. Alemayehu A, Demissie A, Yusuf M, Feleke D, Minsamo K, Abdullahi Y, et al. Covid-19 prevention: level and determinants of knowledge, attitude and practice toward WHO recommended Covid-19 prevention measures after second wave of Covid 19 among harar population, Eastern Ethiopia: a community-based cross-sectional study. J Multidiscip Healthc. (2021). doi: 10.31124/advance.16803607. [Epub ahead of print].
39. Reuben RC, Danladi MMA, Saleh DA, Ejembi PE. Knowledge, attitudes and practices towards COVID-19: an epidemiological survey in North-Central Nigeria. J Community Health. (2021) 46:457–70. doi: 10.1007/s10900-020-00881-1
40. Kasemy ZA, Bahbah WA, Zewain SK, Haggag MG, Alkalash SH, Zahran E, et al. Knowledge, attitude and practice toward COVID-19 among Egyptians. J Epidemiol Glob Health. (2020) 10:378–85. doi: 10.2991/jegh.k.200909.001
41. National Health Commission of the People's Republic of China. Guidelines for the diagnosis and treatment of novel coronavirus pneumonia (trial version eighth). (2020). Available online at: http://www.nhc.gov.cn/xcs/zhengcwj/202008/0a7bdf12bd4b46e5bd28ca7f9a7f5e5a.shtml (accessed August 8, 2020).
42. The Official Website of the People's Government of Anhui Province. East China city detects coronavirus on imported food packaging. (2020). Available online at: http://english.ah.gov.cn/Government/GovernmentBulletin/553936871.html (accessed December 23, 2020).
43. Liu C. Seeing like a state, enacting like an algorithm: (re)assembling contact tracing and risk assessment during the COVID-19 pandemic. Sci Technol Hum Values. (2021) 47:698–725. doi: 10.1177/01622439211021916
44. Liang F. COVID-19 and health code: how digital platforms tackle the pandemic in China. Soc Media Soc. (2020) 6:2056305120947657. doi: 10.1177/2056305120947657
45. Norman CD, Skinner HA. eHealth literacy: essential skills for consumer health in a networked world. J Med Internet Res. (2006) 8:e9. doi: 10.2196/jmir.8.2.e9
46. Office for National Statistics. Internet access–households and individuals, Great Britain: 2018. (2018). Available online at: https://www.ons.gov.uk/peoplepopulationandcommunity/householdcharacteristics/homeinternetandsocialmediausage/bulletins/internetaccesshouseholdsandindividuals/2018 (accessed August 25, 2018).
47. Aghdam ZN, Rahmani AM, Hosseinzadeh M. The role of the internet of things in healthcare: future trends and challenges. Comput Methods Programs Biomed. (2021) 199:105903. doi: 10.1016/j.cmpb.2020.105903
48. Zucco R, Lavano F, Anfosso R, Bianco A, Pileggi C, Pavia M. Internet and social media use for antibiotic-related information seeking: findings from a survey among adult population in Italy. Int J Med Inform. (2018) 111:131–9. doi: 10.1016/j.ijmedinf.2017.12.005
49. Licata F, Angelillo S, Nobile CGA, Di Gennaro G, Bianco A. Understanding individual barriers to HIV testing among undergraduate university students: results from a cross-sectional study in Italy. Front Med. (2022) 9:882125. doi: 10.3389/fmed.2022.882125
50. Licata F, Angelillo S, Oliverio A, Bianco A. The internet: friend or foe of antibiotic resistance? Results of a cross-sectional study among Italian university students. Antibiotics. (2021) 10:1091. doi: 10.3390/antibiotics10091091
51. Bianco A, Zucco R, Nobile CG, Pileggi C, Pavia M. Parents seeking health-related information on the Internet: cross-sectional study. J Med Internet Res. (2013) 15:e204. doi: 10.2196/jmir.2752
52. Anderson A. Online health information and public knowledge, attitudes, and behaviours regarding antibiotics in the UK: multiple regression analysis of Wellcome Monitor and Eurobarometer Data. PLoS ONE. (2018) 13:e0204878. doi: 10.1371/journal.pone.0204878
53. Corea F, Folcarelli L, Napoli A, Del Giudice GM, Angelillo IF. The impact of COVID-19 Vaccination in changing the adherence to preventive measures: evidence from Italy. Vaccines. (2022) 10:777. doi: 10.3390/vaccines10050777
54. Adugna B, Merera O, Negash W, Abdulkadir O, Mohammed Y. Knowledge, Attitude and Practice (KAP) assessment on lifestyle, public health measures practiced by society and their impact to contain COVID-19 transmission among afar community in selected parts of afar region, Ethiopia. Infect Drug Resist. (2022) 15:1277–87. doi: 10.2147/IDR.S349019
55. Shrestha A, Thapa TB, Giri M, Kumar S, Dhobi S, Thapa H, et al. Knowledge and attitude on prevention of COVID-19 among community health workers in Nepal-a cross-sectional study. BMC Public Health. (2021) 21:1424. doi: 10.1186/s12889-021-11400-9
56. Wong MCS, Wong ELY, Huang J, Cheung AWL, Law K, Chong MKC, et al. Acceptance of the COVID-19 vaccine based on the health belief model: a population-based survey in Hong Kong. Vaccine. (2021) 39:1148–56. doi: 10.1016/j.vaccine.2020.12.083
57. Tachfouti N, Slama K, Berraho M, Nejjari C. The impact of knowledge and attitudes on adherence to tuberculosis treatment: a case-control study in a Moroccan region. Pan Afr Med J. (2012) 12:52.
58. Brown Wilson J, Deckert A, Shah R, Kyei N, Copeland Dahn L, Doe-Rogers R, et al. COVID-19-related knowledge, attitudes and practices: a mixed-mode cross-sectional survey in Liberia. BMJ Open. (2021) 11:e049494. doi: 10.1136/bmjopen-2021-049494
59. Zhong BL, Luo W, Li HM, Zhang QQ, Liu XG, Li WT, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. (2020) 16:1745–52. doi: 10.7150/ijbs.45221
60. Rice RE. Influences, usage, and outcomes of Internet health information searching: multivariate results from the Pew surveys. Int J Med Inform. (2006) 75:8–28. doi: 10.1016/j.ijmedinf.2005.07.032
61. Sherman LD, Patterson MS, Tomar A, Wigfall LT. Use of digital health information for health information seeking among men living with chronic disease: data from the health information national trends survey. Am J Mens Health. (2020) 14:1557988320901377. doi: 10.1177/1557988320901377
62. Richtering SS, Hyun K, Neubeck L, Coorey G, Chalmers J, Usherwood T, et al. eHealth literacy: predictors in a population with moderate-to-high cardiovascular risk. JMIR Hum Factors. (2017) 4:e4. doi: 10.2196/humanfactors.6217
63. Al-Hanawi MK, Angawi K, Alshareef N, Qattan AMN, Helmy HZ, Abudawood Y, et al. Knowledge, attitude and practice toward COVID-19 among the public in the kingdom of saudi arabia: a cross-sectional study. Front Public Health. (2020) 8:217. doi: 10.3389/fpubh.2020.00217
64. Park CL, Russell BS, Fendrich M, Finkelstein-Fox L, Hutchison M, Becker J, et al. Americans' COVID-19 stress, coping, and adherence to CDC guidelines. J Gen Intern Med. (2020) 35:2296–303. doi: 10.1007/s11606-020-05898-9
65. Nowak BM, Miedziarek C, Pełczyński S, Rzymski P. Misinformation, fears and adherence to preventive measures during the early phase of COVID-19 pandemic: a cross-sectional study in Poland. Int J Environ Res Public Health. (2021) 18:12266. doi: 10.3390/ijerph182212266
66. Faria de Moura Villela E, López RVM, Sato APS, de Oliveira FM, Waldman EA, Van den Bergh R, et al. COVID-19 outbreak in Brazil: adherence to national preventive measures and impact on people's lives, an online survey. BMC Public Health. (2021) 21:152. doi: 10.1186/s12889-021-10222-z
67. Luk TT, Zhao S, Wu Y, Wong JY, Wang MP, Lam TH. Prevalence and determinants of SARS-CoV-2 vaccine hesitancy in Hong Kong: a population-based survey. Vaccine. (2021) 39:3602–7. doi: 10.1016/j.vaccine.2021.05.036
68. Galasso V, Pons V, Profeta P, Becher M, Brouard S, Foucault M. Gender differences in COVID-19 attitudes and behavior: panel evidence from eight countries. Proc Natl Acad Sci USA. (2020) 117:27285–91. doi: 10.1073/pnas.2012520117
69. Kassim MAM, Pang NTP, Mohamed NH, Kamu A, Ho CM, Ayu F, et al. Relationship between fear of COVID-19, psychopathology and sociodemographic variables in Malaysian population. Int J Ment Health Addict. (2022) 20:1303–10. doi: 10.1007/s11469-020-00444-4
70. Pawlowski B, Atwal R., Dunbar RIM. Sex differences in everyday risk-taking behavior in humans. Evol Psychol. (2008) 6:29–42. doi: 10.1177/147470490800600104
71. Bazaid AS, Aldarhami A, Binsaleh NK, Sherwani S, Althomali OW. Knowledge and practice of personal protective measures during the COVID-19 pandemic: a cross-sectional study in Saudi Arabia. PLoS ONE. (2020) 15:e0243695. doi: 10.1371/journal.pone.0243695
72. Irwin M. Rosenstock. The health belief model and preventive health behavior. Health Educ Monogr. (1974) 2:354–86. doi: 10.1177/109019817400200405
73. Irwin M. Rosenstock. Historical origins of the health belief model. Health Educ Monogr. (1974) 2:328–35. doi: 10.1177/109019817400200403
74. Hesaraki M, Akbarizadeh M, Ahmadidarrehsima S, Moghadam MP, Izadpanah F. Knowledge, attitude, practice and clinical recommendations of health care workers towards COVID-19: a systematic review. Rev Environ Health. (2021) 36:345–57. doi: 10.1515/reveh-2020-0099
75. Wang J, Wagner AL, Chen Y, Jaime E, Hu X, Wu S, et al. Would COVID-19 vaccination willingness increase if mobile technologies prohibit unvaccinated individuals from public spaces? A nationwide discrete choice experiment from China. Vaccine. (2021). doi: 10.1016/j.vaccine.2021.10.020. [Epub ahead of print].
76. Soubelet-Fagoaga I, Arnoso-Martinez M, Elgorriaga-Astondoa E, Martínez-Moreno E. Telework and face-to-face work during COVID-19 confinement: the predictive factors of work-related stress from a holistic point of view. Int J Environ Res Public Health. (2022) 19:3837. doi: 10.3390/ijerph19073837
77. Goldman N, Pebley AR, Lee K, Andrasfay T, Pratt B. Racial and ethnic differentials in COVID-19-related job exposures by occupational standing in the US. PLoS ONE. (2021) 16:e0256085. doi: 10.1371/journal.pone.0256085
78. Trent M, Seale H, Chughtai AA, Salmon D, MacIntyre CR. Trust in government, intention to vaccinate and COVID-19 vaccine hesitancy: a comparative survey of five large cities in the United States, United Kingdom, and Australia. Vaccine. (2022) 40:2498–505. doi: 10.1016/j.vaccine.2021.06.048
79. Riehm KE, Holingue C, Kalb LG, Bennett D, Kapteyn A, Jiang Q, et al. Associations between media exposure and mental distress among U.S. adults at the beginning of the COVID-19 pandemic. Am J Prev Med. (2020) 59:630–8. doi: 10.1016/j.amepre.2020.06.008
Keywords: knowledge, attitude, preventive behavior, COVID-19, eHealth literacy, residents, China
Citation: Yuan T, Li XD, Zhang M, Tao XB, Xu SJ and Liu H (2022) Impact of the eHealth literacy, knowledge and attitudes on COVID-19 prevention behavior among residents in the second year of the COVID-19 pandemic: A cross-sectional study in Anhui Province, China. Front. Public Health 10:1015803. doi: 10.3389/fpubh.2022.1015803
Received: 10 August 2022; Accepted: 07 October 2022;
Published: 02 November 2022.
Edited by:
Italo F. Angelillo, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Francesca Licata, University Magna Graecia of Catanzaro, ItalyZixin Wang, The Chinese University of Hong Kong, China
Copyright © 2022 Yuan, Li, Zhang, Tao, Xu and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huan Liu, wnyxyliuhuan@foxmail.com
†These authors have contributed equally to this work and share first authorship