 Yohei Sasaki1
Yohei Sasaki1 Ryo Okubo
Ryo Okubo Kazuyoshi Takeda
Kazuyoshi Takeda Satoru Ikezawa
Satoru Ikezawa Takahiro Tabuchi
Takahiro Tabuchi- 1Department of Human Sciences, Faculty of Human Sciences, Musashino University, Koto-ku, Japan
- 2Department of Psychiatry and Neurology, National Hospital Organization Obihiro Hospital, Hokkaido, Japan
- 3Department of Clinical Data Science, Clinical Research and Education Promotion Division, National Center of Neurology and Psychiatry, Tokyo, Japan
- 4Graduate School of Arts and Sciences, The University of Tokyo, Tokyo, Japan
- 5Cancer Control Center, Osaka International Cancer Institute, Osaka, Japan
Background: Recent studies have shown an association between psychological distress and emotion malleability beliefs, meaning mindsets about whether one’s emotions are fixed or changeable. However, most studies have not examined the association between these beliefs and sociodemographic factors.
Methods: A nationwide cross-sectional Internet survey of residents of Japan aged 15–79 years was conducted using sampling weights for national estimates to investigate the association between emotion malleability beliefs and sociodemographic factors and between fixed beliefs and severe psychological distress (SPD). SPD was defined as a Kessler 6 Scale score of ≥13. Adjusted odds ratios for SPD were calculated considering potential confounders. Further analyses were stratified by sex, age and presence of any psychiatric disorder.
Results: The analysis included 23,142 participants (female, 48.64%). Fixed beliefs were associated with female sex, age < 45 years, and presence of psychiatric disorders. These beliefs were associated with SPD, and additional analysis showed stronger associations with SPD among female respondents, respondents aged 45–59 years, and those aged ≥60 years.
Conclusion: Results indicate that female sex, age < 45 years, and current mental disorders were associated with fixed emotion malleability beliefs. Associations between fixed emotion malleability beliefs and SPD were particularly strong among female respondents and people aged ≥45 years compared with the general population. Our study extends the association between emotion malleability beliefs and psychological health to the general population. Future studies should explore mechanisms underlying individual differences in emotion beliefs.
1. Introduction
Individuals’ belief systems, also known as implicit theories or mindsets (Dweck and Leggett, 1988), have been widely examined with respect to mental health. Specifically, there is growing interest in research on emotion malleability beliefs in relation to emotional problems (Kneeland et al., 2016; Burnette et al., 2020; Reffi et al., 2020; Schroder, 2021). People with more malleable beliefs about emotion show a positive correlation with positive emotions and well-being and a negative correlation with negative emotions and depressive symptoms (Tamir et al., 2007; King and dela Rosa, 2019). A recent meta-analysis demonstrated a negative association between fixed (less malleable) emotion beliefs and mental health. Moreover, previous studies suggest that individuals holding these beliefs frequently use maladaptive emotion regulation strategies (King and dela Rosa, 2019; Ortner and Pennekamp, 2020; Schell et al., 2023), which are associated with the development, persistence, and exacerbation of emotional disorders (Kneeland et al., 2016; Schroder, 2021).
Emotion dysregulation is at the core of trans-diagnostic mechanisms of emotional disorders (Gross, 2013; Sloan et al., 2017). Whether individuals believe emotions to be malleable or fixed affects their emotion regulation strategies and their experience of emotions, which is associated with psychopathologies such as depression and anxiety (for reviews, see Kneeland et al., 2016; Schroder, 2021). People who believe that emotions can be changed are more likely to engage in adaptive emotion regulation, such as cognitive reappraisal, in which they think of alternative interpretations of a situation (Tamir et al., 2007). On the other hand, people believe that emotions are fixed are more likely to be disengaged from regulation of their own emotions, and consequently to use maladaptive emotion regulation strategies such as avoidance and rumination (De Castella et al., 2018; Kneeland and Dovidio, 2020). These associations between fixed beliefs and psychological health have been observed in clinical research. In patients with social anxiety disorder, fixed beliefs independently explain variance in stress, trait anxiety, negative affect, and self-esteem, even after adjusting for the severity of social anxiety symptoms (De Castella et al., 2014). In patients with depression, fixed beliefs indirectly influence depressive symptoms via experiential avoidance (Sung et al., 2020). Thus, emotion malleability beliefs have been shown to have the potential to advance our understanding of the psychopathology of emotional disorders.
Although studies of emotion malleability beliefs should account for factors such as sex, age, and socioeconomic status, most have not. Some studies indicate that females are less likely to believe that they can regulate their own emotions (Nolen-Hoeksema and Jackson, 2001), whereas others found no gender differences (Tamir et al., 2007; De Castella et al., 2013, 2018). Such inconsistencies might be due to small sample sizes and lack of diversity among study participants. Most studies to date have included fewer than 1,000 participants, and have been conducted with young, Caucasian populations (Burnette et al., 2020). In addition, people who believe emotions are malleable tend to become stronger from early adulthood (18–25 years) to post-25 years old, although the difference was not statistically significant in comparison with adolescents aged 12–17 years (Burnette et al., 2020). Moreover, older people utilize maladaptive emotion regulation strategies less frequently than younger people (Schirda et al., 2016). These age differences in emotion regulation strategies might mean that older people have malleable beliefs about emotions than younger people. Similarly, differences in associations by race and the presence of psychiatric disorders have been examined, but no significant differences were found. Furthermore, the relationship between these beliefs and psychological health in people who have physical illnesses has not been clarified. The prevalence of depression is higher in people with physical illnesses such as hypertension, diabetes, and chronic pain compared with the general population (Gavard et al., 1993; Miller and Cano, 2009; Roy and Lloyd, 2012; Michal et al., 2013; Rayner et al., 2016). Thus, people with these illnesses may have some unique relationship between emotion malleability beliefs and psychological health. To our knowledge, no study has yet examined differences in these beliefs with respect to these factors in the general population.
Our study aimed to examine how emotion malleability beliefs vary by sex, age, health conditions and other socioeconomic factors and how these effect modifiers vary the strength of the association between these beliefs and psychological distress in a general population sample. This study is expected to provide some important findings. First, this study would reveal the relationship between emotion malleability beliefs and these factors. Empirical studies have shown that people who believe emotion is less malleable seek less support from their peers (Tamir et al., 2007) and they prefer medication to psychotherapy (Schroder et al., 2015). Thus, clarifying these associations would enable the dissemination of persuasive messages for improved mental health tailored to each group. Second, identifying a population with fixed beliefs in this study is expected to provide important data to advance the literature on emotion malleability beliefs. We expected that people with fixed beliefs would have higher rates of severe psychological distress than people with malleable beliefs. Therefore, we conducted an exploratory analysis without a specific hypothesis to examine the following research question: Do the associations between these beliefs and psychological distress differ according to the presence of various factors such as health status?
2. Methods
2.1. Study design and participants
This study was a secondary analysis of data from the second wave of the Japan “COVID-19 and Society” Internet Survey (JACSIS; Yoshioka et al., 2021). The JACSIS study complied with ethical standards of the relevant national and institutional committees on human experimentation and the 1975 Declaration of Helsinki (as revised in 2008). The protocol was approved by the Research Ethics Committee of the Osaka International Cancer Research Institute (June 19, 2020; approval number 20084), and the survey allows for secondary use of the data. The protocol for the present study was reviewed and approved by the Research Ethics Committee of the [Anonymised for review] (June 11, 2022; approval number 2021-31-02).
In September 2020, the JACSIS study conducted a nationwide baseline survey of 28,000 male and female respondents aged 15–79 years who were selected randomly from 224,389 panelists registered with a large Internet survey company (Rakuten Insight, Inc., Tokyo, Japan).1 In February 2021, a follow-up survey was conducted in which 24,059 of the 28,000 baseline survey participants took part. In addition, 1,941 participants aged 15–79 years were newly recruited, without stratification by age, sex, or prefecture of residence, giving a total of 26,000 participants. “E-points” (points used for Internet shopping or cash exchange) were offered to encourage participation. Although the survey agency declined to disclose the exact value of the e-points, one E-point is considered equivalent to approximately 100 yen (approximately US$1 at the time of the survey). The study was a cross-sectional study that used data obtained from this follow-up survey, in which participants responded to a scale to measure their beliefs about emotion malleability.
2.2. Measures
2.2.1. Emotion malleability beliefs
The Japanese version of the Personal Implicit Beliefs About Emotions scale (De Castella et al., 2013) assessed emotion malleability beliefs. This questionnaire consists of four items, two of which employ reversed items (“I can learn to control my emotions,” “If I want to, I can change the emotions that I have”). Each item is rated on a 5-point scale (1 = strongly disagree, 5 = strongly agree). A higher total score means that they strongly believe in a lack of control over their emotions.
We developed the Japanese version of this scale based on a report by a working group of the International Society for Pharmacoeconomics and Outcomes Research (Wild et al., 2005). This scale was independently translated from English to Japanese by a psychologist and a bilingual Japanese-English psychiatrist, both of whom integrated the translations through discussion. In addition, another bilingual Japanese-English psychiatrist compared the original version with the Japanese version and made corrections to the translation. The preliminary Japanese version was then back translated into English by a bilingual individual employed at a translation company who was unfamiliar with the original version. The author of the original version reviewed the back-translation and confirmed the equivalence of its semantic content with that of the original version.
De Castella et al. (2013) did not report the factor structure of the Personal Implicit Beliefs about Emotion Scale. In our analyses below, we used the total score of this scale as in previous studies (De Castella et al., 2013, 2014). In the present study, internal reliability was demonstrated based on Cronbach’s α of 0.59 and McDonald’s ω of 0.66, which were slightly lower compared with the Cronbach’s alpha of 0.73 reported previously (De Castella et al., 2018).
2.2.2. Severe psychological distress
The Japanese version of The Kessler Psychological Distress Scale, a widely used measure of psychological distress in the general population, was used to assess psychological distress (Furukawa et al., 2003). For this study, severe psychological distress (SPD) was defined as a total score of 13 or higher. A score of 13 was a cutoff to screen for severe mood disorder or any anxiety disorder (Furukawa et al., 2003; Kessler et al., 2003). The present study showed good internal consistency (α = 0.93; ω = 0.94).
2.2.3. Sociodemographic factors
The following sociodemographic factors were considered: sex, age (15–29, 30–44, 45–59, 60–79 years), income (low, <JPY2.5 million/US$25,000/£16,667; intermediate, JPY2.5–JPY4.3 million/US$25,000–US$43,000/£16,667–£28,667; high, <JPY4.3 million/<US$43,000/<£28,667; unknown/declined to answer), marital status (unmarried, married, and widowed/separated), education, working status (working, schooling, homemaker, not working), history of tobacco use, history of alcohol use, and presence of current illness (hypertension, diabetes mellitus, asthma or chronic obstructive pulmonary disease, cardiovascular disease, cerebrovascular disease, cancer, chronic pain, psychiatric disorders).
2.3. Statistical methods
First, an inverse probability weighting (IPW) method was used to correct for differences between Internet survey respondents and the general population. By logistic regression analysis, propensity scores (weights) were calculated using sex, age, and socioeconomic factors to correct for differences between respondents to the current Internet survey and respondents to the 2019 National Survey on Living Standards, which is representative of the Japanese population. Details of this calculation are described in our previous studies (Okubo et al., 2021a,b). Second, an individual’s malleable beliefs are described on a spectrum, with malleable beliefs at one pole and fixed beliefs at the other pole (Dweck and Leggett, 1988); therefore, we trichotomized participants’ beliefs as malleable (T1: total score from 4 to 10), neither (T2: total score from 11 to 12), or fixed (T3: total score from 13 to 20 scores), where high signifies a strong belief in emotion malleability. Implicit theories research explains belief effects by contrasting individuals who do believe in emotion malleability with those who do not (Dweck et al., 1995; Tamir et al., 2007). Finally, the association between emotion beliefs and SPD was clarified by calculating adjusted odds ratios (aORs) and 95% confidence intervals (CIs) for SPD by logistic regression analysis with IPW based on propensity scores. In these analyses, all variables noted above were entered into the model as independent variables. All analyses were performed using R software version 4.0.3.
3. Results
Of the 26,000 study participants, 2,858 were excluded for satisficing or straight-lining or discrepant survey responses (for example, respondents who chose inappropriate responses to the instruction “Please choose the second from the bottom of the following options.” or respondents who answered “currently have this condition and receiving treatment” or “currently have this condition but not receiving treatment” (as opposed to “never in the past” or “not now, but had in the past”) to all 16 questions regarding the following comorbidities). Thus, the analysis included data from 23,142 (89.0%) participants. The sociodemographic characteristics of the participants are shown in Table 1. Among 23,412 participants, the median total score for implicit beliefs about emotions was divided into tertiles, namely, a malleable group (T1), an neither group (T2), and a fixed group (T3) with median total scores of 16, 12, and 10, respectively. The high group had 8,123 participants (35.1%), the middle group 11,465 participants (49.5%), and the fixed group 3,554 participants (15.4%).
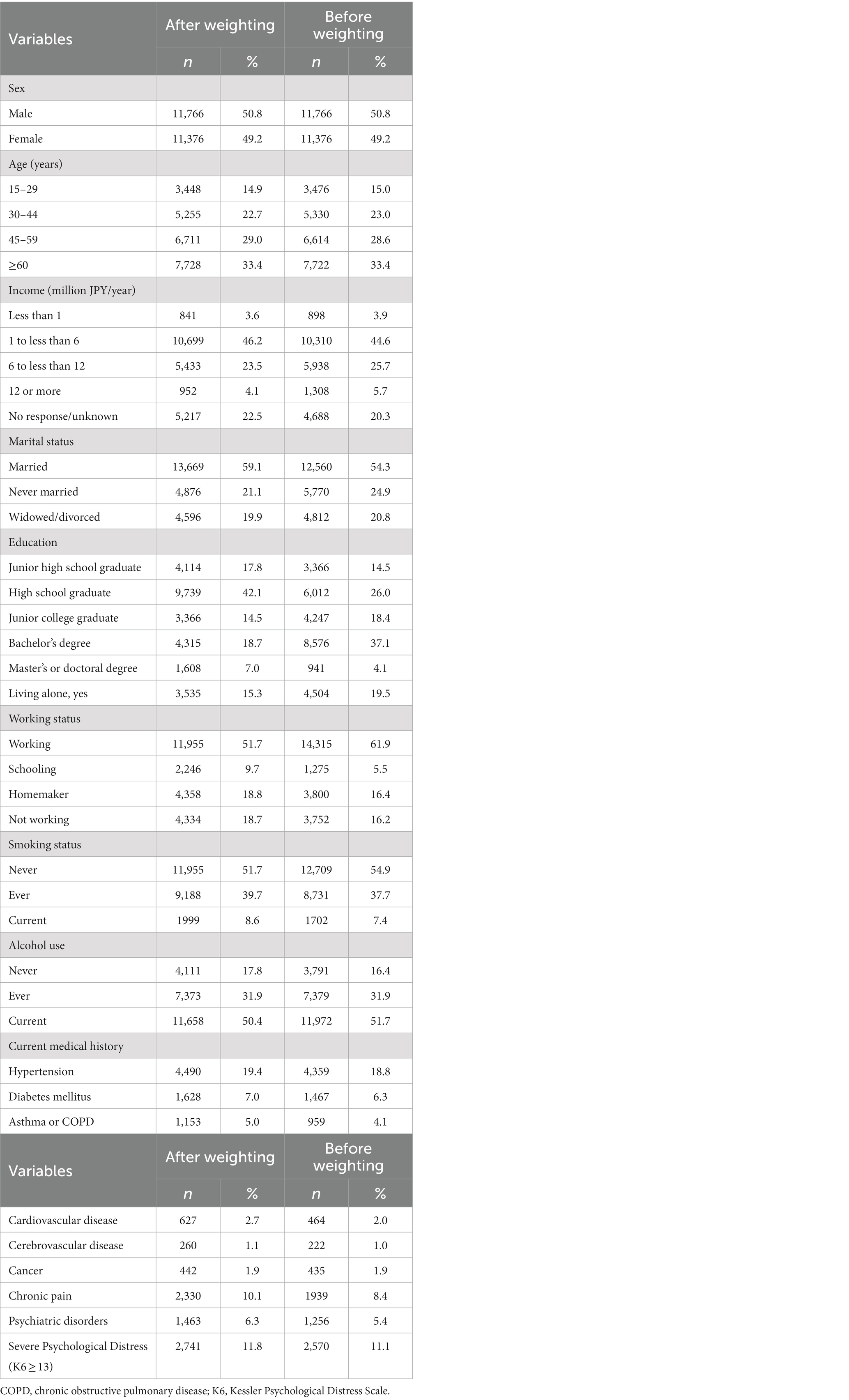
Table 1. Participant characteristics (before and after propensity score weighting).
Table 2 shows sociodemographic characteristics factors associated with emotion malleability beliefs. We found that female respondents had significantly fixed beliefs than male respondents (aOR = 1.31; 95% CI = 1.18–1.44, p < 0.001). Compared with people aged 45–59 years, those aged 29 years or younger (aOR = 1.24; 95% CI = 1.09–1.41, p < 0.001) and those aged 30–44 years (aOR = 1.16; 95% CI = 1.05–1.28, p < 0.01) had fixed beliefs, whereas those aged 60 years or older had malleable beliefs (aOR = 0.57; 95% CI = 0.51–0.65, p < 0.001). In terms of income, we found that compared with the group earning 1 million to 6 million yen, the group earning 6 million to 12 million yen had significantly fixed beliefs (aOR = 1.13; 95% CI = 1.02–1.24, p < 0.05), whereas the non-response group had significantly malleable beliefs (aOR = 0.85; 95% CI = 0.77–1.13, p < 0.01). As for marital status, never-married people had significantly fixed beliefs compared with married people (aOR = 1.13; 95% CI = 1.02–1.27, p < 0.05). Regarding educational background, compared with respondents with a bachelor’s degree, junior high school graduates (aOR = 1.20, 95% CI = 1.04–1.39, p < 0.05) and high school graduates (aOR = 1.15, 95% CI = 1.04–1.28, p < 0.01) had significantly fixed beliefs, whereas those with a master’s degree or above had significantly malleable beliefs (aOR = 0.22, 95% CI = 0.16–0.30, p < 0.001). Meanwhile, people living alone had significantly fixed beliefs than people living with others (aOR = 0.87, 95% CI = 0.77–0.98, p < 0.05). We found that emotion malleability beliefs were significantly fixed in ever-smokers (aOR = 1.20, 95% CI = 1.08–1.35, p < 0.001) and current smokers (aOR = 1.16, 95% CI = 1.04–1.30, p < 0.01) than in never-smokers. In terms of current medical history, people with hypertension (aOR = 1.19, 95% CI = 1.07–1.32, p < 0.001), diabetes (aOR = 1.21, 95% CI = 1.04–1.40, p < 0.01), chronic pain (aOR = 1.45, 95% CI = 1.29–1. 63, p < 0.001), or psychiatric disorders (aOR = 2.79, 95% CI = 2.46–3.16, p < 0.001) had significantly fixed beliefs, whereas people with cerebrovascular disease (aOR = 0.69, 95% CI = 0.48–0.98, p < 0.05) or cancer (aOR = 0.63, 95% CI = 0.44–1.82, p < 0.01) had significantly malleable beliefs.
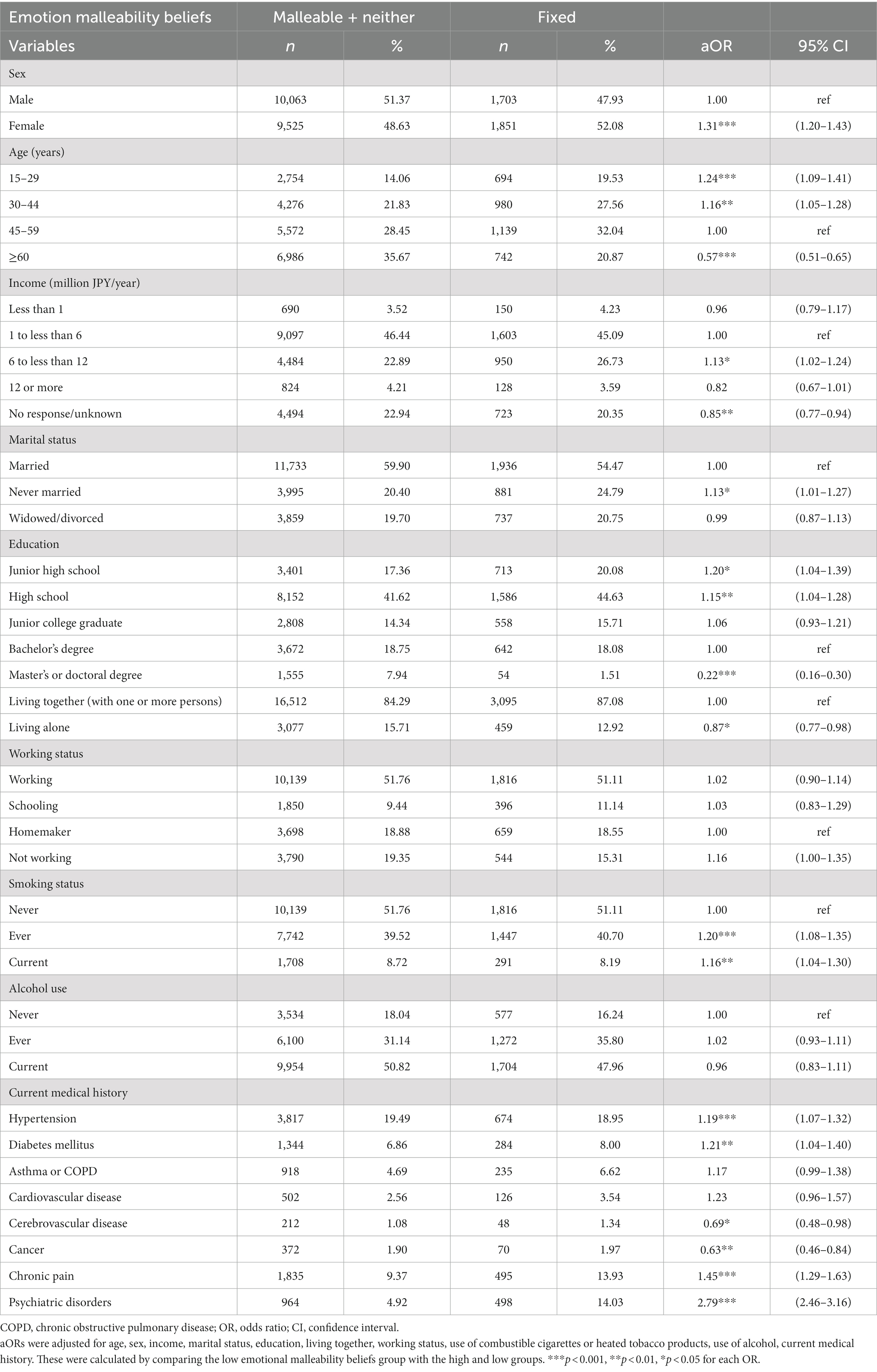
Table 2. Association between sociodemographic characteristics and total scores of binarized (malleable + neither vs. ficed) emotion malleability beliefs.
Table 3 shows the relationship between fixed malleability beliefs and risk of SPD. The aORs for the association between these beliefs and SPD were higher in the neither group (aOR = 2.48, 95% CI = 2.18–2.83, trend p < 0.001) and fixed group (aOR = 7.55, 95% CI = 6.56–8.68, trend p < 0.001) than in the malleable group. For relationships between fixed beliefs and SPD by sociodemographic characteristic factors, when compared with all participants, there was a strong association between fixed beliefs and SPD in the neither group (aOR = 3.69, 95% CI = 3.03–4.49, trend p < 0.001) and fixed group (aOR = 11.42, 95% CI = 9.27–14.08, trend p < 0.001) among females, the fixed group among those aged 45–59 years, and in the neither group (aOR = 8.81, 95% CI = 6.89–11.26, trend p < 0.001) and fixed group (aOR = 30.32, 95% CI = 14.56–64.05, trend p < 0.001) among those aged 60 years or older.
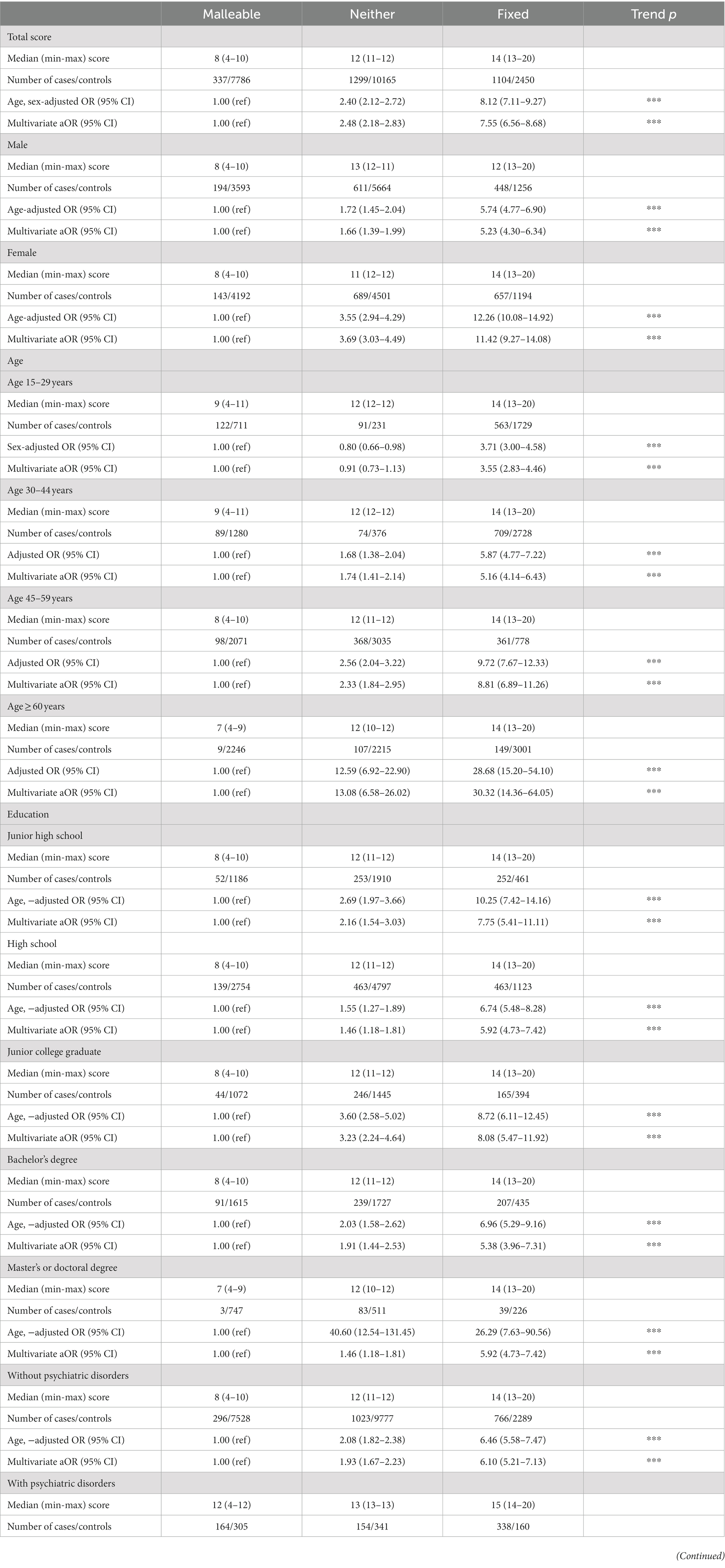
Table 3. Odds ratio and 95% confidence intervals for severe psychological distress according to the trisect of the total score on emotion malleability beliefs (lower score = lower malleability).
4. Discussion
This study aimed to examine differences in emotion malleability beliefs across sex, age, and socioeconomic factors and differences in the relative strength of the association between these beliefs and SPD across effect modifiers, such as sex and age, using a large general population sample. Logistic regression analysis revealed a significant association between fixed beliefs and female sex, younger age, lower education, unmarried status, nonemployment, smoking, and the presence of hypertension, diabetes, chronic pain, or psychiatric disorders. In addition, fixed beliefs were a risk factor for SPD, with the association stronger for female respondents and respondents aged 45 years or older than for all participants.
The proportion of respondents with high emotion malleability beliefs increased with age. This result is consistent with previous research showing that older adults exhibit more mature emotional processing and regulation strategies than younger adults (Lawton, 2001; Blanchard-Fields, 2007; Urry and Gross, 2010). Older adults are characterized by their ability to pay attention to positive aspects and to construct better evaluations when confronted with negative information (Charles and Luong, 2013). When compared with younger adults, older adults are reported to utilize more adaptive emotion regulation strategies, such as acceptance, and fewer maladaptive emotion regulation strategies during anxiety- and sadness-provoking situations (Schirda et al., 2016).
We found that female respondents had fixed beliefs than male. Although several studies have reported no sex differences in emotion malleability beliefs (Tamir et al., 2007; De Castella et al., 2013, 2018), all of these studies had small sample sizes (n = 101–437) and did not adjust for confounders such as educational background, income, and current illness. This is the first study to examine differences in the distribution of emotion malleability beliefs using a large sample (>10,000 people). Interestingly, the association between fixed beliefs and SPD was more than twice as strong in female respondents than in male respondents. This difference can be explained by sex differences in emotion regulation strategies that are strongly related to emotion malleability beliefs. Female tend to focus more attention on their emotions than do male and they engage in excessive rumination to understand their feelings and the causes of their emotions, resulting in emotion regulation failure (Nolen-Hoeksema, 2012). Meta-analyses found that female ruminate more frequently than male (Rood et al., 2009; Johnson and Whisman, 2013). Failure to regulate emotions reinforces the belief that emotions are uncontrollable. In addition, these differences in these beliefs between male and female may be partially explained by the influence of psychosocial development on sex differences. According to gender socialization theory, girls of a certain generation are expected to internalize negative emotions and display more empathy and sympathy than boys of a certain generation (Brody and Hall, 2008; Zahn-Waxler et al., 2008). Female may be affected by cultural pressures that promote the internalization of negative emotions and may develop the belief that controlling emotions is difficult.
Our finding that people with any psychiatric disorder have fixed beliefs than those without is consistent with previous studies showing fixed beliefs in patients with social anxiety disorder (De Castella et al., 2014) and depressive disorder (Sung et al., 2020) compared with healthy individuals. Our findings support the theory that people who believe that emotions are uncontrollable are less motivated to effectively regulate negative emotions and become increasingly symptomatic (Kneeland et al., 2016; Schroder, 2021). Studying individual differences in how people respond to their own emotions can help clarify the mechanisms underlying depression and anxiety disorders and elaborate psychological interventions (Campbell-Sills et al., 2007).
This study is the first to examine the association between physical illness and emotion malleability beliefs. Our results showed that people with hypertension, diabetes, and chronic pain had fixed beliefs. People with these illnesses have a high prevalence of depression. More specifically, the prevalence of depression is 21.3% in people with hypertension (Michal et al., 2013) and 30% in people with chronic pain (Miller and Cano, 2009; Rayner et al., 2016); and people with diabetes have a prevalence of depression 2–3 times that in the general adult population (Gavard et al., 1993; Roy and Lloyd, 2012). Emotion beliefs can partially explain the differences in the prevalence of depression between people with physical illness and healthy individuals. In addition, people with fixed emotion malleability beliefs tend to prefer medication over psychotherapy (Schroder et al., 2015). Psychotherapy is reported to be effective in improving comorbid depression (Li et al., 2017, 2021; Ólason et al., 2018). Therefore, clinicians might first need to motivate their patients to believe in the malleability of their emotions to enhance their motivation for treatment before providing psychological intervention.
Interestingly, our results showed that cancer patients have high emotion malleability beliefs. Some researchers have proposed that more than two-thirds of adults cancer patients do not experience clinical anxiety or mood disorders (Mitchell et al., 2011Ólason et al., 2018 Linden et al., 2015) because most people can effectively regulate their emotions throughout the disease course (Kangas and Gross, 2020). Future research should investigate changes in emotion malleability beliefs throughout the course of cancer to gain a more detailed understanding of emotion regulation processes.
The association between fixed beliefs and SPD was stronger in older adults than in younger adults. One explanation is that mediators of the association between fixed beliefs and SPD differ between younger and older adults. For example, people with fixed beliefs are less likely to receive support from new friends (Tamir et al., 2007). Fifty-five percent of older adults experience moderate or greater loneliness and social isolation, which significantly reduces their mental health (Musich et al., 2015; Erzen and Çikrikci, 2018). Future research should examine factors such as loneliness that can specifically mediate these beliefs and SPD in older adults. Development of an education or intervention program that focuses on these mediators might be needed as well.
This study has several limitations that should be considered. First, the sample was collected through an Internet survey, which does not fully reflect the demographic distribution of the general population. Although we conducted weighted sampling utilizing nationally representative data to adjust for potential bias, it is possible that only people with a high affinity for Internet use participated in the survey. Second, this cross-sectional study cannot deny the reverse causation. For example, severe depression or anxiety might cause people to believe that their emotions are fixed. Finally, recent studies have shown that beliefs about emotions are not only malleability but also include beliefs such as useful and unfriendly (Ford and Gross, 2019; Veilleux et al., 2021). The present study cannot exclude the possibility that other emotion beliefs may have a more important relationship with psychological distress.
In conclusion, we found that the beliefs that individuals hold about emotions are fixed was associated with female sex, younger age, lower educated, unmarried status, nonemployment, smoking, and hypertension, diabetes, chronic pain, and psychiatric disorders. Furthermore, the association between fixed beliefs and SPD was stronger in female respondents and the elderly. These results can be explained by differences in factors such as loneliness and emotion regulation strategies, which might mediate the association between emotion malleability beliefs and SPD. Future studies are needed to compare the strength of the association between emotion malleability beliefs and emotion regulation strategies, such as rumination, using simultaneous multi-population analyses to partially explain the 2–3 times higher risk of major depressive disorder in female compared with men (Van de Velde et al., 2010; Breslau et al., 2017). In addition, it would be beneficial to provide group education on emotion malleability beliefs and psychological distress in educational settings utilized by many young people with fixed beliefs. An intervention for middle school students was conducted with the aim of improving mental health by modifying these beliefs (Smith et al., 2018), and such intervention programs targeting emotion beliefs in young people should be further developed. Furthermore, people with fixed beliefs tend to be less motivated to engage in psychotherapy (Schroder et al., 2015), so it is important to measure emotion malleability beliefs when administering psychotherapy. Psychoeducation about the controllability of emotions prior to psychotherapy is a potentially beneficial clinical strategy for motivating patients with fixed beliefs to engage in evoke strong emotion techniques, such as exposure (Kneeland et al., 2016). Our research supports the possibility that the study of emotion malleability beliefs can contribute to the development of more tailored strategies and interventions to improve psychological health.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: all anonymized individual participant data reported in this paper are available for interested researchers who send a request for data sharing, along with a synopsis of the secondary analysis plan paper to the RO. Requests to access these datasets should be directed to RO, rokubo0425@gmail.com.
Ethics statement
The studies involving humans were approved by the Research Ethics Committee of the Osaka International Cancer Research Institute and the Research Ethics Committee of the Musashino University. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because in accordance with national legislation and institutional requirements, written informed consent was not required for this study.
Author contributions
YS and RO performed the data analysis. YS, RO, and KS drafted the manuscript. RO and TT designed the survey and collected the data. All authors contributed to the manuscript and agreed to submit it for publication.
Funding
This secondary analysis was funded by the Japan Health Research Promotion Bureau Research Fund [grant number (2020-B-09)]. This fund had no role in the study design, in the collection, analysis, or interpretation of data, in the writing of the report, or in the decision to submit the article for publication. JACSIS study was funded by the Japan Society for the Promotion of Science (JSPS) KAKENHI Grant-in-Aid for Scientific Research (Grant Nos. 18H03107, 18H03062, 20H00040, and 17H00947); Grant-in-Aid for Challenging Research (Grant No. 19K22788) and the JSPS Grant-in-Aid for Early-Career Scientists (Grant Nos. 19K2017 and 22K17844).
Acknowledgments
We would like to thank Kota Katanoda, Keisuke Kuwahara, Kanami Tsuno, Kenji Takeuchi, Hiroshi Murayama, Ai Hori, Isao Muraki, Naoki Kondo, and Takeo Fujiwara for their support related to data collection. We would like to thank all the participants in this study.
Conflict of interest
SI has received honoraria for lectures from Boehringer Ingelheim Pharmaceuticals, Inc., H. Lundbeck A/S, Otsuka Pharmaceutical Co., Ltd., Sumitomo Pharma Co., Ltd., and Takeda Pharmaceutical Company Limited, has received support for attending meetings and/or travel from Boehringer Ingelheim Pharmaceuticals, Inc., H. Lundbeck A/S, and Takeda Pharmaceutical Company Limited, and has received consulting fees from Boehringer Ingelheim Pharmaceuticals, Inc.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
Blanchard-Fields, F. (2007). Everyday problem solving and emotion: an adult developmental perspective. Curr. Dir. Psychol. Sci. 16, 26–31. doi: 10.1111/j.1467-8721.2007.00469.x
Breslau, J., Gilman, S. E., Stein, B. D., Ruder, T., Gmelin, T., and Miller, E. (2017). Sex differences in recent first-onset depression in an epidemiological sample of adolescents. Transl. Psychiatry 7, –e1139. doi: 10.1038/tp.2017.105
Brody, L. R., and Hall, J. A. (2008). “Gender and emotion in context” in Handbook of emotions. eds. M. Lewis, J. M. Haviland-Jones, and L. F. Barrett. 3rd ed (New York: The Guilford Press), 395–408.
Burnette, J. L., Knouse, L. E., Vavra, D. T., O'Boyle, E., and Brooks, M. A. (2020). Growth mindsets and psychological distress: a meta-analysis. Clin. Psychol. Rev. 77:101816. doi: 10.1016/j.cpr.2020.101816
Campbell-Sills, L., Barlow, D., and Gross, J. (2007). “Incorporating emotion regulation intoconceptualizations and treatments of anxiety and mood disorders” in Handbook of emotion regulation. ed. J. J. Gross (New York: The Guilford Press), 542–559.
Charles, S. T., and Luong, G. (2013). Emotional experience across adulthood: the theoretical model of strength and vulnerability integration. Curr. Dir. Psychol. Sci. 22, 443–448. doi: 10.1177/0963721413497013
De Castella, K., Goldin, P., Jazaieri, H., Ziv, M., Dweck, C. S., and Gross, J. J. (2013). Beliefs about emotion: links to emotion regulation, well-being, and psychological distress. Basic Appl. Soc. Psychol. 35, 497–505. doi: 10.1080/01973533.2013.840632
De Castella, K., Goldin, P., Jazaieri, H., Ziv, M., Heimberg, R. G., and Gross, J. J. (2014). Emotion beliefs in social anxiety disorder: associations with stress, anxiety, and well-being. Aust. J. Psychol. 66, 139–148. doi: 10.1111/ajpy.12053
De Castella, K., Platow, M. J., Tamir, M., and Gross, J. J. (2018). Beliefs about emotion: implications for avoidance-based emotion regulation and psychological health. Cogn. Emot. 32, 773–795. doi: 10.1080/02699931.2017.1353485
Dweck, C. S., Chiu, C.-Y., and Hong, Y.-Y. (1995). Implicit theories and their role in judgments and reactions: a word from two perspectives. Psychol. Inq. 6, 267–285. doi: 10.1207/s15327965pli0604_1
Dweck, C. S., and Leggett, E. L. (1988). A social-cognitive approach to motivation and personality. Psychol. Rev. 95, 256–273. doi: 10.1037/0033-295X.95.2.256
Erzen, E., and Çikrikci, Ö. (2018). The effect of loneliness on depression: a meta-analysis. Int. J. Soc. Psychiatry 64, 427–435. doi: 10.1177/0020764018776349
Ford, B. Q., and Gross, J. J. (2019). Why beliefs about emotion matter: An emotion-regulation perspective. Curr. Dir. in Psychol. Sci. 28, 74–81. doi: 10.1177/0963721418806697
Furukawa, T. A., Kessler, R. C., Slade, T., and Andrews, G. (2003). The performance of the K6 and K10 screening scales for psychological distress in the Australian National Survey of mental health and well-being. Psychol. Med. 33, 357–362. doi: 10.1017/s0033291702006700
Gavard, J. A., Lustman, P. J., and Clouse, R. E. (1993). Prevalence of depression in adults with diabetes: an epidemiological evaluation. Diabetes Care 16, 1167–1178. doi: 10.2337/diacare.16.8.1167
Gross, J. J. (2013). Emotion regulation: taking stock and moving forward. Emotion 13, 359–365. doi: 10.1037/a0032135
Johnson, D. P., and Whisman, M. A. (2013). Gender differences in rumination: a meta-analysis. Pers. Individ. Dif. 55, 367–374. doi: 10.1016/j.paid.2013.03.019
Kangas, M., and Gross, J. J. (2020). The affect regulation in cancer framework: understanding affective responding across the cancer trajectory. J. Health Psychol. 25, 7–25. doi: 10.1177/1359105317748468
Kessler, R. C., Barker, P. R., Colpe, L. J., Epstein, J. F., Gfroerer, J. C., Hiripi, E., et al. (2003). Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 60, 184–189. doi: 10.1001/archpsyc.60.2.184
King, R. B., and dela Rosa, E. D. (2019). Are your emotions under your control or not? Implicit theories of emotion predict well-being via cognitive reappraisal. Pers. individ. dif. 138, 177–182. doi: 10.1016/j.paid.2018.09.040
Kneeland, E. T., and Dovidio, J. F. (2020). Emotion malleability beliefs and coping with the college transition. Emotion 20 452–461. doi: 10.1037/emo0000559
Kneeland, E. T., Dovidio, J. F., Joormann, J., and Clark, M. S. (2016). Emotion malleability beliefs, emotion regulation, and psychopathology: integrating affective and clinical science. Clin. Psychol. Rev. 45, 81–88. doi: 10.1016/j.cpr.2016.03.008
Lawton, M. P. (2001). Emotion in later life. Curr. Dir. Psychol. Sci. 10, 120–123. doi: 10.1111/1467-8721.00130
Li, Y., Buys, N., Li, Z., Li, L., Song, Q., and Sun, J. (2021). The efficacy of cognitive behavioral therapy-based interventions on patients with hypertension: A systematic review and meta-analysis. Prev. Med. Rep. 23, 101477. doi: 10.1016/j.pmedr.2021.101477
Li, C., Xu, D., Hu, M., Tan, Y., Zhang, P., Li, G., et al. (2017). A systematic review and meta-analysis of randomized controlled trials of cognitive behavior therapy for patients with diabetes and depression. J. Psychosom. Res. 95, 44–54. doi: 10.1016/j.jpsychores.2017.02.006
Linden, W., MacKenzie, R., Rnic, K., Marshall, C., and Vodermaier, A. (2015). Emotional adjustment over 1 year post-diagnosis in patients with cancer: understanding and predicting adjustment trajectories. Support Care Cancer 23, 1391–1399. doi: 10.1007/s00520-014-2492-9
Michal, M., Wiltink, J., Lackner, K., Wild, P. S., Zwiener, I., Blettner, M., et al. (2013). Association of hypertension with depression in the community: results from the Gutenberg health study. J. Hypertens. 31, 893–899. doi: 10.1097/hjh.0b013e32835f5768
Miller, L. R., and Cano, A. (2009). Comorbid chronic pain and depression: who is at risk? J. Pain 10, 619–627. doi: 10.1016/j.jpain.2008.12.007
Mitchell, A. J., Chan, M., Bhatti, H., Halton, M., Grassi, L., Johansen, C., et al. (2011). Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncol. 12, 160–174. doi: 10.1016/s1470-2045(11)70002-x
Musich, S., Wang, S. S., Hawkins, K., and Yeh, C. S. (2015). The impact of loneliness on quality of life and patient satisfaction among older, sicker adults. Gerontol. Geriatr. Med. 1:2333721415582119. doi: 10.1177/2333721415582119
Nolen-Hoeksema, S. (2012). Emotion regulation and psychopathology: the role of gender. Annu. Rev. Clin. Psychol. 8, 161–187. doi: 10.1146/annurev-clinpsy-032511-143109
Nolen-Hoeksema, S., and Jackson, B. (2001). Mediators of the gender difference in rumination. Psychol. Women Q. 25, 37–47. doi: 10.1111/1471-6402.00005
Okubo, R., Yoshioka, T., Nakaya, T., Hanibuchi, T., Okano, H., Ikezawa, S., et al. (2021a). Urbanization level and neighborhood deprivation, not COVID-19 case numbers by residence area, are associated with severe psychological distress and new-onset suicidal ideation during the COVID-19 pandemic. J. Affect. Disord. 287, 89–95. doi: 10.1016/j.jad.2021.03.028
Okubo, R., Yoshioka, T., Ohfuji, S., Matsuo, T., and Tabuchi, T. (2021b). COVID-19 vaccine hesitancy and its associated factors in Japan. Vaccine 9:662. doi: 10.3390/vaccines9060662
Ólason, M., Andrason, R. H., Jónsdóttir, I. H., Kristbergsdóttir, H., and Jensen, M. P. (2018). Cognitive behavioral therapy for depression and anxiety in an interdisciplinary rehabilitation program for chronic pain: a randomized controlled trial with a 3-year follow-up. Int. J. Behav. Med. 25, 55–66. doi: 10.1007/s12529-017-9690-z
Ortner, C. N., and Pennekamp, P. (2020). Emotion malleability beliefs and event intensity and importance predict emotion regulation in daily life. Pers. Individ. Dif. 159:109887. doi: 10.1016/j.paid.2020.109887
Rayner, L., Hotopf, M., Petkova, H., Matcham, F., Simpson, A., and McCracken, L. M. (2016). Depression in patients with chronic pain attending a specialised pain treatment centre: prevalence and impact on health care costs. Pain 157, 1472–1479. doi: 10.1097/j.pain.0000000000000542
Reffi, A. N., Darnell, B. C., Himmerich, S. J., and White, K. J. (2020). Implicit beliefs of emotion and anxiety in psychotherapy. Motiv. Emot. 44, 453–463. doi: 10.1007/s11031-019-09794-6
Rood, L., Roelofs, J., Bögels, S. M., Nolen-Hoeksema, S., and Schouten, E. (2009). The influence of emotion-focused rumination and distraction on depressive symptoms in non-clinical youth: a meta-analytic review. Clin. Psychol. Rev. 29, 607–616. doi: 10.1016/j.cpr.2009.07.001
Roy, T., and Lloyd, C. E. (2012). Epidemiology of depression and diabetes: a systematic review. J. Affect. Disord. 142, S8–S21. doi: 10.1016/s0165-0327(12)70004-6
Schell, V., De France, K., Lin, L., and Hollenstein, T. (2023). The role of avoidance in understanding emotional dysfunction associated with a fixed emotion mindset. Pers. Individ. Dif. 201:111945. doi: 10.1016/j.paid.2022.111945
Schirda, B., Valentine, T. R., Aldao, A., and Prakash, R. S. (2016). Age-related differences in emotion regulation strategies: examining the role of contextual factors. Dev. Psychol. 52, 1370–1380. doi: 10.1037/dev0000194
Schroder, H. S. (2021). Mindsets in the clinic: applying mindset theory to clinical psychology. Clin. Psychol. Rev. 83:101957. doi: 10.1016/j.cpr.2020.101957
Schroder, H. S., Dawood, S., Yalch, M. M., Donnellan, M. B., and Moser, J. S. (2015). The role of implicit theories in mental health symptoms, emotion regulation, and hypothetical treatment choices in college students. Cogn. Ther. Res. 39, 120–139. doi: 10.1007/s10608-014-9652-6
Sloan, E., Hall, K., Moulding, R., Bryce, S., Mildred, H., and Staiger, P. K. (2017). Emotion regulation as a transdiagnostic treatment construct across anxiety, depression, substance, eating and borderline personality disorders: a systematic review. Clin. Psychol. Rev. 57, 141–163. doi: 10.1016/j.cpr.2017.09.002
Smith, E. N., Romero, C., Donovan, B., Herter, R., Paunesku, D., Cohen, G. L., et al. (2018). Emotion theories and adolescent well-being: results of an online intervention. Emotion 18, 781–788. doi: 10.1037/emo0000379
Sung, G., Park, Y., Choi, T. K., and Park, S. W. (2020). Implicit theories and depression in clinical and non-clinical samples: the mediating role of experiential avoidance. Curr. Psychol. 39, 68–73. doi: 10.1007/s12144-017-9736-z
Tamir, M., John, O. P., Srivastava, S., and Gross, J. J. (2007). Implicit theories of emotion: affective and social outcomes across a major life transition. J. Pers. Soc. Psychol. 92, 731–744. doi: 10.1037/0022-3514.92.4.731
Urry, H. L., and Gross, J. J. (2010). Emotion regulation in older age. Curr. Dir. Psychol. Sci. 19, 352–357. doi: 10.1177/0963721410388395
Van de Velde, S., Bracke, P., and Levecque, K. (2010). Gender differences in depression in 23 European countries. Cross-national variation in the gender gap in depression. Soc. Sci. Med. 71, 305–313. doi: 10.1016/j.socscimed.2010.03.035
Veilleux, J. C., Chamberlain, K. D., Baker, D. E., and Warner, E. A. (2021). Disentangling beliefs about emotions from emotion schemas. J. Clin.Psychol. 77, 1068–1089. doi: 10.1002/jclp.23098
Wild, D., Grove, A., Martin, M., Eremenco, S., McElroy, S., Verjee-Lorenz, A., et al. (2005). Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health 8, 94–104. doi: 10.1111/j.1524-4733.2005.04054.x
Yoshioka, T., Okubo, R., Tabuchi, T., Odani, S., Shinozaki, T., and Tsugawa, Y. (2021). Factors associated with serious psychological distress during the COVID-19 pandemic in Japan: a nationwide cross-sectional internet-based study. BMJ Open 11:e051115. doi: 10.1136/bmjopen-2021-051115
Keywords: emotion regulation, emotion malleability beliefs, mindset, psychological distress, emotion belief
Citation: Sasaki Y, Okubo R, Takeda K, Ikezawa S, Tabuchi T and Shirotsuki K (2023) The association between emotion malleability beliefs and severe psychological distress stratified by sex, age, and presence of any psychiatric disorders. Front. Psychol. 14:1251945. doi: 10.3389/fpsyg.2023.1251945
Edited by:
Gabriele Nibbio, University of Brescia, ItalyReviewed by:
Irene Calzavara-Pinton, University of Brescia, ItalyCeren Gökdağ, Manisa Celal Bayar University, Türkiye
Copyright © 2023 Sasaki, Okubo, Takeda, Ikezawa, Tabuchi and Shirotsuki. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ryo Okubo, rokubo0425@gmail.com