 Alicia Saz-Lara1
Alicia Saz-Lara1 Iván Cavero-Redondo2*
Iván Cavero-Redondo2* Vicente Martínez-Vizcaíno1,2
Vicente Martínez-Vizcaíno1,2 Maribel Lucerón-Lucas-Torres1
Maribel Lucerón-Lucas-Torres1 Carlos Pascual-Morena1
Carlos Pascual-Morena1 Irese Sequí-Domínguez1
Irese Sequí-Domínguez1- 1Universidad de Castilla-La Mancha, Health and Social Research Center, Cuenca, Spain
- 2Universidad Autónoma de Chile, Facultad de Ciencias de la Salud, Talca, Chile
Background: Orthostatic hypotension, defined as a decrease in blood pressure on standing, is associated with an increased risk of mortality and cardiovascular events in the general population. In addition, it has recently been suggested that arterial stiffness is independently associated with orthostatic hypotension, which may be due to a loss of the buffering effect of the ascending aorta and an early return of pressure waves. However, the specific mechanisms underlying this association remain unclear. Thus, we aimed to evaluate the association between orthostatic hypotension and arterial stiffness in the adult population.
Methods: PubMed, Scopus, Web of Science, and Cochrane Library databases were searched from inception to 31 January 2022. The DerSimonian and Laird method was used to calculate pooled odds ratio (OR) estimates and their respective 95% confidence intervals (95% CI) for the association between orthostatic hypotension and arterial stiffness.
Results: Overall, 11 studies were included, with a total of 10,611 subjects. Our results showed that increased arterial stiffness raises the risk of orthostatic hypotension (OR: 1.40, 95% CI: 1.28–1.54), with a stronger association at central arterial stiffness (OR: 1.50, 95% CI: 1.34–1.68) than at peripheral arterial stiffness (OR: 1.29, 95% CI: 1.17–1.43).
Conclusion: Our findings showed that increased arterial stiffness raises the risk of orthostatic hypotension by 40% among the adult population. Considering that orthostatic hypotension, which is usually a consequence of antihypertensive treatment, has been widely associated with the risk of cardiovascular events, appropriate control of arterial stiffness could be a clinical strategy to prevent cardiovascular morbidity and mortality.
1 Introduction
Orthostatic hypotension (OH) is a condition of increasing interest in scientific research. Certain neurological diseases are associated with OH; however, OH can also occur due to non-neurological causes. OH is defined by consensus as a decrease in systolic blood pressure by at least 20 mmHg or a decrease in diastolic blood pressure by at least 10 mmHg within the first 3 min of standing upright (Freeman et al., 2011). When the upright posture is adopted, the baroreceptors located at the level of the carotid artery and the aorta are activated and a decrease in blood pressure is produced, causing inhibition of the parasympathetic nervous system and activation of the sympathetic nervous system. This activation leads to an increase in blood levels of noradrenaline, adrenaline, and plasma renin activity, thus raising peripheral arterial resistance and cardiac output to maintain blood pressure (Shibao et al., 2013).
This physiological mechanism may interfere with the presence of atheromatous plaques by sustained high blood pressure levels or by the action of various toxicants acting on the endothelium, leading to sustained arterial hypertension and, thus, favoring an abnormal blood pressure response with orthostasis. Even in subjects without baseline hypertension, OH is associated with increased arterial stiffness, (Takahashi et al., 2015), as measured by pulse wave velocity (PWv). The association is greater when PWv is higher (Mattace-Raso et al., 2006). Arterial stiffness is inversely associated with baroreceptor sensitivity; in these subjects, the mechanisms of blood pressure regulation may not be triggered by the postural change since the activity of the baroreceptor system is diminished by arterial stiffness, thus favoring the fall in blood pressure after orthostasis (Okada et al., 2012).
However, there is limited evidence supporting an association between OH and arterial stiffness, and no meta-analysis has amalgamated this evidence or synthesized this relationship. Thus, the purpose of this systematic review and meta-analysis was to provide a synthesis of the evidence regarding the relationship between OH and arterial stiffness, as measured by its reference standard, PWv.
2 Methods
This study, a systematic review and meta-analysis, was performed according to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) statement (Stroup et al., 2008) and was conducted following the recommendations of the Cochrane Collaboration Handbook (Higgins and Green, 2011). This study was registered in PROSPERO (registration number: CRD42022304329).
2.1 Search strategy
A systematic search was conducted independently by two reviewers (I.C.-R. and A.S.-L.) and was performed through four databases, namely, Scopus, PubMed, Cochrane Library, and Web of Science, from their inception to 13 March 2022. To perform the search, the following free terms combined with Boolean operators were used, following the PICO (population, intervention/exposure, comparison, and outcome) strategy: “Adults,” “Adult population,” “Adult subjects,” “Arterial stiffness,” “Pulse wave velocity,” “PWv,” “Aortic stiffness,” and “Orthostatic hypotension” (Supplementary Table S1). Furthermore, we searched previous systematic reviews or meta-analyses, and the references of the included articles.
2.2 Study selection
Studies on the association between OH and arterial stiffness were included in this systematic review and meta-analysis. The inclusion criteria were as follows: i) population: adult subjects with pathologies; ii) exposure: arterial stiffness measured by PWv; iii) comparison: subjects with OH versus subjects without OH; and iv) outcome: OH defined as a decrease in SBP of at least 20 mmHg and/or DBP of at least 10 mmHg. We excluded i) review articles, editorials, or case reports; ii) studies that did not include cross-sectional data on the association between OH and arterial stiffness; and iii) articles that were not written in English or Spanish.
2.3 Data extraction and quality assessment
Study selection, data extraction, and quality assessment of the studies were performed independently by two researchers (I.C.-R. and A.S.-L.), excluding those studies that did not meet the eligibility criteria. Disagreements were resolved by consensus or with the intervention of a third researcher (V.M.-V.).
Table 1 shows the main characteristics of the included studies and covers information on the following: (1) reference: first author and year of publication; (2) country in which the study data were collected; (3) study design (cross-sectional analysis of cohort studies or cross-sectional studies); (4) population characteristics: sample size (%female), mean age, pathologies prevalence in OH (hypertension, diabetes mellitus, heart failure, myocardial infarction, etc.); (5) exposure (arterial stiffness): PWv index (brachial to ankle PWv [ba-PWv] and carotid to femoral PWv [cf.-PWv]), device, baseline PWv levels; and (6) outcome (OH): assessment points (after standing) and OH prevalence.
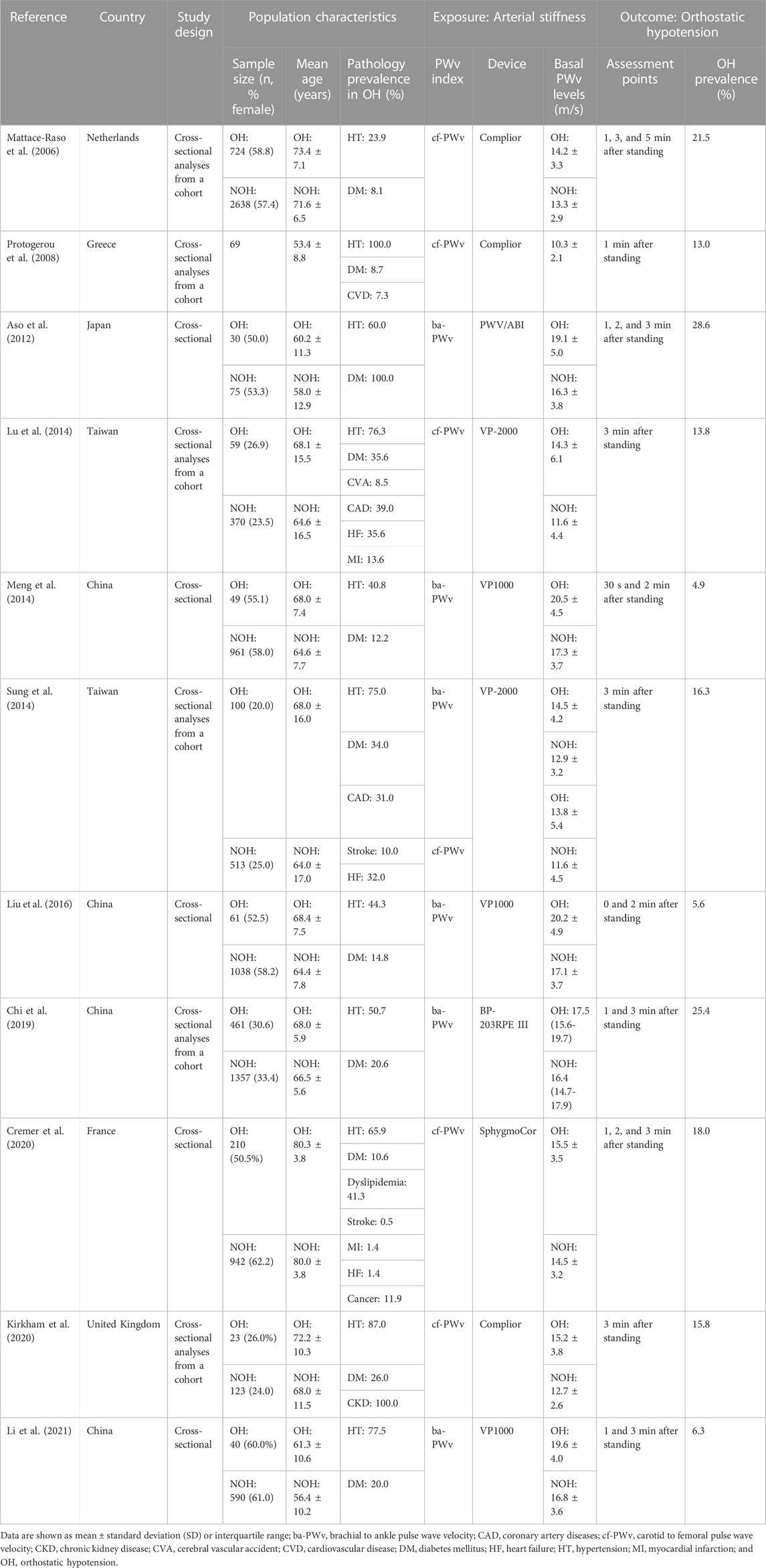
TABLE 1. Characteristics of the included studies in the systematic review and meta-analysis.
The quality assessment tool for observational cohort and cross-sectional studies from the United States National Institute of Health National Heart, Lung, and Blood Institute (National Institutes of Health, 2022) was used to assess the risk of bias according to the following domains: quality of the research question, reporting of the population definition, participation rate, recruitment, sample size, appropriateness of statistical analyses, timeframe for associations, exposure levels, ascertainment of the exposure, appropriateness of the outcome measured, outcome blinding of researchers, loss to follow-up, and confounding variables. The overall bias of each study was considered “good” if most criteria were met and there was a low risk of bias, “fair” if some criteria were met and there was a moderate risk of bias, or “poor” if few criteria were met and there was a high risk of bias.
2.4 Data synthesis and statistical analysis
The DerSimonian and Laird random-effects method (DerSimonian and Kacker, 2007) was used to compute pooled estimates of odds ratios (ORs) and their respective 95% confidence intervals (95% CIs) for the association between OH and arterial stiffness. In addition, the association between OH and central and peripheral AS was evaluated. Meta-analyses required at least five studies in each exposure group. (Jackson and Turner, 2017). Heterogeneity was examined using the I2 statistic (Higgins and Thompson, 2002), which ranges from 0% to 100%. According to I2 values, heterogeneity was considered not important (0%–30%), moderate (30%–60%), substantial (60%–75%), or considerable (75%–100%). The corresponding p-values were also considered.
Sensitivity analysis (systematic reanalysis removing studies one at a time) was conducted to assess the robustness of the summary estimates. Subgroup analyses were performed according to mean age (<65 or >65 years). Random effects meta-regression analyses addressed whether mean age, percentage of female subjects, smoking history, hypertension, and diabetes mellitus prevalence modified the association between OR and arterial stiffness. Finally, publication bias was assessed using Egger’s regression asymmetry test (Sterne et al., 2001) using a level <0.10 to determine whether publication bias might be present.
All statistical analyses were conducted with Stata SE software, version 15 (StataCorp, College Station, TX, United States).
3 Results
3.1 Baseline characteristics
In total, 11 studies (Mattace-Raso et al., 2006; Protogerou et al., 2008; Aso et al., 2012; Lu et al., 2014; Meng et al., 2014; Sung et al., 2014; Liu et al., 2016; Chi et al., 2019; Cremer et al., 2020; Kirkham et al., 2020; Li et al., 2021) were included in the systematic review and meta-analysis (Figure 1). Of the included studies, six were prospective longitudinal studies, (Mattace-Raso et al., 2006; Protogerou et al., 2008; Lu et al., 2014; Sung et al., 2014; Chi et al., 2019; Kirkham et al., 2020), and five were cross-sectional studies. (Aso et al., 2012; Meng et al., 2014; Liu et al., 2016; Cremer et al., 2020; Li et al., 2021). Studies were conducted in seven countries: four in China (Meng et al., 2014; Liu et al., 2016; Chi et al., 2019; Li et al., 2021), two in Taiwan (Lu et al., 2014; Sung et al., 2014), and one each in the Netherlands (Mattace-Raso et al., 2006), Greece (Protogerou et al., 2008), Japan (Aso et al., 2012), France (Cremer et al., 2020), and the United Kingdom. (Kirkham et al., 2020). Records were published between 2006 and 2020 and included a total of 10,611 subjects (aged 37.0–80.0 years). Regarding the type of exposure, different methods were used to measure PWv: six samples for ba-PWv (Aso et al., 2012; Meng et al., 2014; Sung et al., 2014; Liu et al., 2016; Chi et al., 2019; Li et al., 2021) and six samples for cf.-PWv. (Mattace-Raso et al., 2006; Protogerou et al., 2008; Lu et al., 2014; Sung et al., 2014; Cremer et al., 2020; Kirkham et al., 2020). Finally, the measurement of OH was performed in the range of 30 s to 5 min after standing.
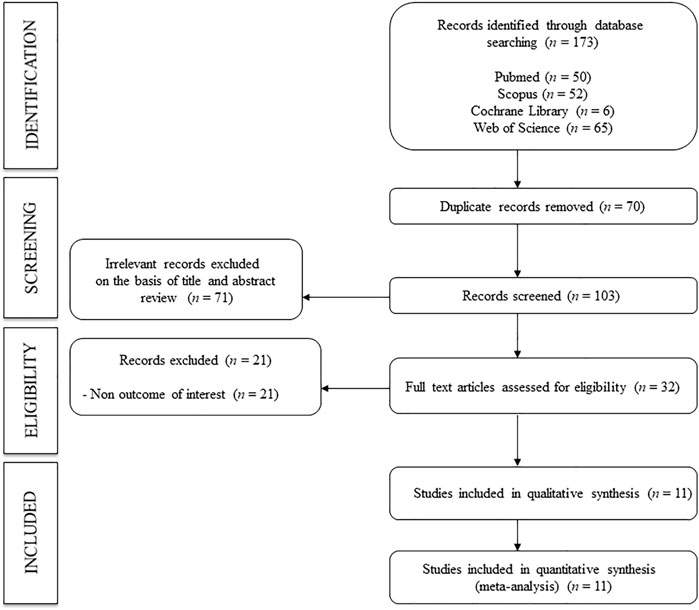
FIGURE 1. Flowchart: search strategy.
3.2 Quality assessment and potential bias
The overall risk of bias for studies examining the association between OH and arterial stiffness was fair in 45.5% of the studies and poor in 54.5% (Supplementary Table S2). For all exposures, we were able to identify three main reasons for a poor risk of bias: (i) the follow-up time was not reported or was not long enough to establish an association between the exposure and outcome; (ii) the participation rate of eligible persons was not reported; and (iii) a sample size justification was not reported. In addition, due to the cross-sectional design of the studies, none of the studies provided information on whether the researchers were blinded to the exposure status of the participants.
3.3 Association between orthostatic hypotension and arterial stiffness
Increased arterial stiffness measured by PWv was associated with an increase in the pooled OR estimate of OH (OR: 1.40; 95% CIs: 1.28–1.54). The heterogeneity of this estimate was substantial (I2 = 68.2%; p = 0.000) (Figure 2).
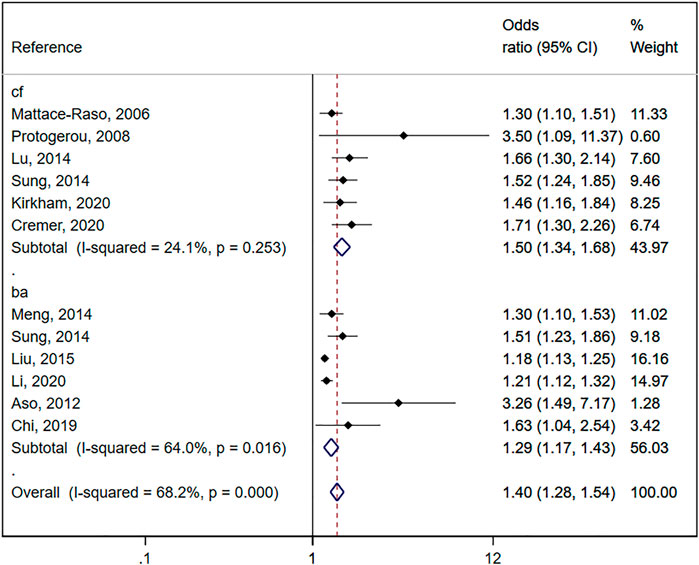
FIGURE 2. Forest plot including the association between orthostatic hypotension and arterial stiffness (central and peripheral pulse wave velocity).
3.4 Association between orthostatic hypotension and central arterial stiffness
When the association of OH and central arterial stiffness was estimated, a significant increase in subjects with OH was shown for cf.-PWv compared to subjects without OH (OR: 1.50; 95% CIs: 1.34–1.68), with no significant heterogeneity (I2 = 24.1%; p = 0.253) (Figure 2).
3.5 Association between orthostatic hypotension and peripheral arterial stiffness
When the association of OH and peripheral arterial stiffness was estimated, a significant increase in subjects with OH was shown for ba-PWv compared to subjects without OH (OR: 1.29; 95% CIs: 1.17–1.43), with substantial heterogeneity (I2 = 64.0%; p = 0.016) (Figure 2).
3.6 Sensitivity analysis
The pooled OR estimate for the association between OH and arterial stiffness was not significantly modified (in magnitude or direction) when data from individual studies were removed from the analysis one at a time.
3.7 Subgroup analysis and meta-regression models
Subgroup analyses were performed according to mean age (<65 or >65 years), and the pooled OR estimate showed significant results in subjects >65 years for increased arterial stiffness (OR: 1.38; 95% CIs: 1.24–1.53) (Supplementary Table S3). Random-effects meta-regression models showed that the percentage of female subjects could influence the pooled OR estimate for the association between OH and arterial stiffness (p = 0.028) (Supplementary Table S4).
3.8 Publication bias
Finally, evidence of publication bias was observed through Egger’s test for arterial stiffness (p = 0.000). Additionally, publication bias was found in central arterial stiffness (p = 0.050) (Supplementary Figure S1) and peripheral arterial stiffness (p = 0.003) (Supplementary Figure S2).
4 Discussion
This is a novel systematic review and meta-analysis to evaluate the association between OH and arterial stiffness in adults. Our findings provide a synthesis of the evidence supporting the observations that increased arterial stiffness measured by PWv is associated with a 40% higher risk of OH. Additionally, our findings show that the risk of OH is higher in central arterial stiffness (cf.-PWv) than in peripheral arterial stiffness (ba-PWv), at 50% and 29%, respectively.
Several studies have reported that OH is a predictor of cardiovascular disease (CVD) events (Rutan et al., 1992; Rose et al., 2000; Verwoert et al., 2008; Fedorowski et al., 2010; Fedorowski et al., 2011; Uraschek et al., 2018) based on the hypothesis that transient hypoperfusion of the heart by OH contributes to cumulative microvascular ischemia over time. However, this hypothesis remains controversial. (Juraschek et al., 2020). Furthermore, arterial stiffness measured by PWv has been shown to be associated with different CVD events. (Vlachopoulos et al., 2010; Ben-Shlomo et al., 2014; Zhong et al., 2018; Sequí-Domínguez et al., 2020). Our findings could show another possible hypothesis in which the mechanism by which OH could be a predictor of CVD events would be due to a continuous increase in arterial stiffness. Arterial stiffness is a chronic process (related to aging) that produces changes at both functional and structural levels and which seems to precede OH, which could be considered an acute and punctual process. Thus, episodes of OH could indicate a preclinical increase in arterial stiffness, although this possible hypothesis requires further research. However, given that a cause-effect association (similar to a chicken or egg first dilemma) cannot be established due to the nature of the study, another hypothesis to establish the association between OH and arterial stiffness in a young and healthy population could be the effect caused by orthostatic abnormalities in increasing vascular stiffness, which could evolve into clinical orthostatic disorders. (Wu et al., 2022).
Furthermore, our results showed a higher risk of OH associated with central arterial stiffness than with peripheral arterial stiffness. This could be explained by structural differences between central and peripheral arteries as central arteries have a greater number of smooth muscle cells and elastin. (Lacolley et al., 2017). The pathophysiology of OH points to alterations in smooth muscle cells and elastin (Singh et al., 2021) caused by damage or dysfunction of the baroreflex efferent pathway, which could be associated with this small difference in central and peripheral arterial stiffness (Mattace-Raso et al., 2007). Moreover, long-term increased arterial stiffness could generate functional changes in both central and peripheral arteries (Jordan et al., 2020), producing this possible association with subsequent CVD events associated with OH.
In addition to the main findings of this systematic review and meta-analysis, the meta-regression analysis showed that, in studies with larger numbers of women, the risk of OH associated with increased arterial stiffness decreased. This suggests that the underlying mechanisms of pressure-dependent arterial stiffness differ by sex. However, evidence supporting this idea is limited (Fonesca et al., 2018), and a better understanding of these interactions may be relevant for new approaches to the treatment of BP and arterial stiffness.
Some limitations to this study that could have compromised our results should be noted. First, the assessment of OH could have varied among the included studies (between 0 and 5 min). Second, there was evidence of significant publication bias with the Egger test, and the results of unpublished studies could have modified the results of our meta-analysis. Furthermore, the association between OH and arterial stiffness has only recently been investigated, and this may have been a source of publication bias. Third, the pooled OR for PWv and ba-PWv analysis showed a substantial risk of heterogeneity; therefore, our results should be interpreted with caution. Fourth, since PWv has been the accepted gold standard for non-invasive measurement of arterial stiffness (Van Bortel et al., 2011), only studies using PWv were included in this systematic review and meta-analysis. Fifth, given the scarcity of studies, it was not possible to perform subgroup analyses by age and by healthy or treated population, which are variables that may have influenced the association between OH and arterial stiffness. Finally, since the association reported by the included studies was cross-sectional in nature, a cause-effect relationship could not be inferred. Therefore, future follow-up studies should examine this cause-effect relationship between OH and arterial stiffness.
5 Conclusion
In summary, our data suggest that increased arterial stiffness, measured by PWv, increases the risk of OH and is higher for central arterial stiffness than peripheral arterial stiffness. Considering that OH, which is usually associated with antihypertensive, antiparkinsonian, and antidepressant treatments, has been widely associated with the risk of cardiovascular events, appropriate control of arterial stiffness could be a clinical strategy to prevent cardiovascular morbidity and mortality.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
Author contributions
Conceptualization: AS-L and IC-R; methodology: AS-L, IS-D, and IC-R; software: IC-R and IS-D; validation: CP-M and ML-L-T; formal analysis: AS-L and IS-D; investigation: AS-L and IC-R; resources: AS-L, CP-M, and ML-L-T; data curation: IC-R and VM-V; writing—original draft preparation: AS-L and IC-R; writing—review and editing: VM-V; visualization: CP-M and ML-L-T; and supervision: IC-R and VM-V. All of the authors revised and approved the final version of the article.
Funding
This study was funded by the Spanish Ministry of Science and Innovation, Instituto de Salud Carlos III and co-funded by the European Union (ERDF/ESF), grant numbers PI21/00008 and RD21/0016/0025. AS-L is supported by a grant from the University of Castilla-La Mancha (2019-PREDUCLM-10708). ML-L-T is supported by a grant from the University of Castilla-La Mancha (2022-PROD-20657). CP-M is supported by a grant from the University of Castilla-La Mancha (2018-CPUCLM-7939). IS-D is supported by a grant (FPU19/00109) from the Ministry of Science, Innovation and Universities.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2023.1164519/full#supplementary-material
References
Aso, Y., Wakabayashi, S., Terasawa, T., Naruse, R., Hara, K., Takebayashi, K., et al. (2012). Elevation of serum high molecular weight adiponectin in patients with type 2 diabetes and orthostatic hypotension: Association with arterial stiffness and hypercoagulability. Diabet. Med. 29 (1), 80–87. doi:10.1111/j.1464-5491.2011.03364.x
Ben-Shlomo, Y., Spears, M., Boustred, C., May, M., Anderson, S. G., Benjamin, E. J., et al. (2014). Aortic pulse wave velocity improves cardiovascular event prediction: An individual participant meta-analysis of prospective observational data from 17,635 subjects. J. Am. Coll. Cardiol. 63 (7), 636–646. doi:10.1016/j.jacc.2013.09.063
Chi, H. J., Feng, H. J., Chen, X. J., Zhao, X. T., Zhang, E. X., Fan, Y. F., et al. (2019). The association between orthostatic blood pressure changes and subclinical target organ damage in subjects over 60 years old. J. Geriatr. Cardiol. 16 (5), 387–394. doi:10.11909/j.issn.1671-5411.2019.05.006
Cremer, A., Boutouyrie, P., Laurent, S., Gosse, P., and Tzourio, C. (2020). Orthostatic hypotension: A marker of blood pressure variability and arterial stiffness: A cross-sectional study on an elderly population: The 3-city study. J. Hypertens. 38 (6), 1103–1109. doi:10.1097/HJH.0000000000002374
DerSimonian, R., and Kacker, R. (2007). Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 28, 105–114. doi:10.1016/j.cct.2006.04.004
Fedorowski, A., Hedblad, B., and Melander, O. (2011). Early postural blood pressure response and cause-specific mortality among middle-aged adults. Eur. J. Epidemiol. 26, 537–546. doi:10.1007/s10654-011-9578-1
Fedorowski, A., Stavenow, L., Hedblad, B., Berglund, G., Nilsson, P. M., and Melander, O. (2010). Orthostatic hypotension predicts all-cause mortality and coronary events in middle-aged individuals (The Malmo Preventive Project). Eur. Heart J. 31, 85–91. doi:10.1093/eurheartj/ehp329
Fonesca, R., Veloudi, P., Schultz, M. G., Butlin, M., Picone, D., Avolio, A., et al. (2018). “Sex differences in the association between aortic stiffness and orthostatic blood pressure changes,” in High blood pressure research council of Australia abstracts from the joint HBPRCA (AAS and AVBS Meeting).
Freeman, R., Wieling, W., Axelrod, F. B., Benditt, D. G., Benarroch, E., Biaggioni, I., et al. (2011). Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin. Auton. Res. 21, 69–72. doi:10.1007/s10286-011-0119-5
Higgins, J. P. T., and Green, S. (2011). Cochrane Handbook for systematic reviews of interventions. Version 5.1.0. (Updated March 2011). The Cochrane Collaboration. Available online at: http://crtha.iums.ac.ir/files/crtha/files/cochrane.pdf.(accessed March 25, 2022).
Higgins, J. P. T., and Thompson, S. G. (2002). Quantifying heterogeneity in a meta-analysis. Stat 21, 1539–1558. doi:10.1002/sim.1186
Jackson, D., and Turner, R. (2017). Power analysis for random-effects meta-analysis. Res. Syn. Meth 8, 290–302. doi:10.1002/jrsm.1240
Jordan, J., Ricci, F., Hoffmann, F., Hamrefors, V., and Fedorowski, A. (2020). Orthostatic hypertension: Critical appraisal of an overlooked condition. Hypertension 75 (5), 1151–1158. doi:10.1161/HYPERTENSIONAHA.120.14340
Juraschek, S. P., Taylor, A. A., Wright, J. T., Evans, G. W., Miller, E. R., Plante, T. B., et al. (2020). Orthostatic hypotension, cardiovascular outcomes, and adverse events: Results from SPRINT. Hypertension 75 (3), 660–667. doi:10.1161/HYPERTENSIONAHA.119.14309
Kirkham, F. A., Rankin, P., Parekh, N., Holt, S. G., and Rajkumar, C. (2020). Aortic stiffness and central systolic pressure are associated with ambulatory orthostatic BP fall in chronic kidney disease. J. Nephrol. 33 (2), 317–324. doi:10.1007/s40620-019-00655-6
Lacolley, P., Regnault, V., Segers, P., and Laurent, S. (2017). Vascular smooth muscle cells and arterial stiffening: Relevance in development, aging, and disease. Physiol. Rev. 27, 1555–1617. doi:10.1152/physrev.00003.2017
Li, X., Shi, R., Meng, Q., Zhang, X., and Chen, X. (2021). Does arterial stiffness affect orthostatic hypotension among high-altitude Tibetans? Postgrad. Med. 133 (2), 173–180. doi:10.1080/00325481.2020.1823683
Liu, K., Wang, S., Wan, S., Zhou, Y., Pan, P., Wen, B., et al. (2016). Arterial stiffness, central pulsatile hemodynamic load, and orthostatic hypotension. J. Clin. Hypertens. (Greenwich) 18 (7), 655–662. doi:10.1111/jch.12726
Lu, D. Y., Sung, S. H., Yu, W. C., Cheng, H. M., Chuang, S. Y., and Chen, C. H. (2014). Wave reflections, arterial stiffness, heart rate variability and orthostatic hypotension. Hypertens. Res. 37 (12), 1056–1061. doi:10.1038/hr.2014.127
Mattace-Raso, F. U., Van Den Meiracker, A. H., Bos, W. J., Van Der Cammen, T. J., Westerhof, B. E., Elias-Smale, S., et al. (2007). Arterial stiffness, cardiovagal baroreflex sensitivity and postural blood pressure changes in older adults: The rotterdam study. J. Hypertens. 25 (7), 1421–1426. doi:10.1097/HJH.0b013e32811d6a07
Mattace-Raso, F. U., Van der Cammen, T. J., Knetsch, A. M., Van den Meiracker, A. H., Schalekamp, M. A., Hofman, A., et al. (2006). Arterial stiffness as the candidate underlying mechanism for postural blood pressure changes and orthostatic hypotension in older adults: The Rotterdam Study. J. Hypertens. 24, 339–344. doi:10.1097/01.hjh.0000202816.25706.64
Meng, Q., Wang, S., Wang, Y., Wan, S., Liu, K., Zhou, X., et al. (2014). Arterial stiffness is a potential mechanism and promising indicator of orthostatic hypotension in the general population. Vasa 43 (6), 423–432. doi:10.1024/0301-1526/a000389
National Institutes of Health (2022). Quality assessment Tool for observational cohort and cross-sectional studies. National heart, Lung, and blood Institute. Available online at: www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/tools/cohort (accessed March 30, 2022).
Okada, Y., Galbreath, M. M., Shibata, S., Jarvis, S. S., VanGundy, T. B., Meier, R. L., et al. (2012). Relationship between sympathetic baroreflex sensitivity and arterial stiffness in elderly men and women. Hypertension 59 (1), 98–104. doi:10.1161/HYPERTENSIONAHA.111.176560
Protogerou, A. D., Stergiou, G. S., Lourida, P., and Achimastos, A. (2008). Arterial stiffness and orthostatic blood pressure changes in untreated and treated hypertensive subjects. J. Am. Soc. Hypertens. 2 (5), 372–377. doi:10.1016/j.jash.2008.03.011
Rose, K. M., Tyroler, H. A., Nardo, C. J., Arnett, D. K., Light, K. C., Rosamond, W., et al. (2000). Orthostatic hypotension and the incidence of coronary heart disease: The atherosclerosis risk in communities study. Am. J. Hypertens. 13, 571–578. doi:10.1016/s0895-7061(99)00257-5
Rutan, G. H., Hermanson, B., Bild, D. E., Kittner, S. J., LaBaw, F., and Tell, G. S. (1992). Orthostatic hypotension in older adults. The cardiovascular health study. CHS collaborative research group. Hypertension 19 (6), 508–519. doi:10.1161/01.hyp.19.6.508
Sequí-Domínguez, I., Cavero-Redondo, I., Álvarez-Bueno, C., Pozuelo-Carrascosa, D. P., Nunez de Arenas-Arroyo, S., and Martínez-Vizcaíno, V. (2020). Accuracy of pulse wave velocity predicting cardiovascular and all-cause mortality. A systematic review and meta-analysis. J. Clin. Med. 9 (7), 2080. doi:10.3390/jcm9072080
Shibao, C., Lipsitz, L. A., and Biaggioni, I. (2013). ASH position paper: Evaluation and treatment of orthostatic hypotension. J. Clin. Hypertens. (Greenwich) 15, 147–153. doi:10.1111/jch.12062
Singh, J. N., Nguyen, T., Kerndt, C. C., and Dhamoon, A. S. (2021). Physiology, blood pressure age related changes. Statpearls Publishing, 12. InStatPearls [Internet].
Sterne, J. A., Egger, M., and Smith, G. D. (2001). Systematic reviews in health care: Investigating and dealing with publication and other biases in meta-analysis. BMJ 323, 101–105. doi:10.1136/bmj.323.7304.101
Stroup, D. F., Berlin, J. A., Morton, S. C., Olkin, I., Williamson, G. D., Rennie, D., et al. (2008). Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-Analysis of observational studies in Epidemiology (MOOSE) group. JAMA 283, 2008–2012. doi:10.1001/jama.283.15.2008
Sung, S. H., Chen, Z. Y., Tseng, T. W., Lu, D. Y., Yu, W. C., Cheng, H. M., et al. (2014). Wave reflections, arterial stiffness, and orthostatic hypotension. Am. J. Hypertens. 27 (12), 1446–1455. doi:10.1093/ajh/hpu063
Takahashi, M., Miyai, N., Nagano, S., Utsumi, M., Oka, M., Yamamoto, M., et al. (2015). Orthostatic blood pressure changes and subclinical markers of atherosclerosis. Am. J. Hypertens. 28, 1134–1140. doi:10.1093/ajh/hpu301
Uraschek, S. P., Daya, N., Appel, L. J., Miller, E. R., McEvoy, J. W., Matsushita, K., et al. (2018). Orthostatic hypotension and risk of clinical and subclinical cardiovascular disease in middle-aged adults. J. Am. Heart Assoc. 7, e008884. doi:10.1161/JAHA.118.008884
Van Bortel, L. M., Laurent, S., Boutouyrie, P., Chowienczyk, P., Cruickshank, J. K., De Backer, T., et al. (2011). Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J. Hypertens. 30, 445–448. doi:10.1097/HJH.0b013e32834fa8b0
Verwoert, G. C., Mattace-Raso, F. U., Hofman, A., Heeringa, J., Stricker, B. H., Breteler, M. M., et al. (2008). Orthostatic hypotension and risk of cardiovascular disease in elderly people: The rotterdam study. J. Am. Geriatr. Soc. 56, 1816–1820. doi:10.1111/j.1532-5415.2008.01946.x
Vlachopoulos, C., Aznaouridis, K., and Stefanadis, C. (2010). Prediction of cardiovascular events and all-cause mortality with arterial stiffness: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 55 (13), 1318–1327. doi:10.1016/j.jacc.2009.10.061
Wu, P., Xu, G., Pan, M., Lin, L., and Cai, W. (2022). The association between orthostatic blood pressure changes and arterial stiffness. Blood Press Monit. 27 (4), 239–246. doi:10.1097/MBP.0000000000000594
Keywords: orthostatic hypotension, arterial stiffness, pulse wave velocity, adults, meta-analysis
Citation: Saz-Lara A, Cavero-Redondo I, Martínez-Vizcaíno V, Lucerón-Lucas-Torres M, Pascual-Morena C and Sequí-Domínguez I (2023) Association between arterial stiffness and orthostatic hypotension: A systematic review and meta-analysis. Front. Physiol. 14:1164519. doi: 10.3389/fphys.2023.1164519
Received: 12 February 2023; Accepted: 13 April 2023;
Published: 28 April 2023.
Edited by:
Stephen Vatner, The State University of New Jersey, United StatesReviewed by:
Luis Daniel Jiménez, Universidad Juárez Autónoma de Tabasco, MexicoViktor Nikolaevich Dorogovtsev, Federal Research and Clinical Center of Intensive Care Medicine and Rehabilitology, Russia
Copyright © 2023 Saz-Lara, Cavero-Redondo, Martínez-Vizcaíno, Lucerón-Lucas-Torres, Pascual-Morena and Sequí-Domínguez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Iván Cavero-Redondo, Ivan.Cavero@uclm.es