 Rachel Prevost1†
Rachel Prevost1† Basile Chretien1†Elise-Marie Minoc1,2
Basile Chretien1†Elise-Marie Minoc1,2 Charles Dolladille1,3Angélique Da-Silva1†
Charles Dolladille1,3Angélique Da-Silva1† Ahmad Nehme4†
Ahmad Nehme4† Florence Joly3,5†Véronique Lelong-Boulouard1,2†
Florence Joly3,5†Véronique Lelong-Boulouard1,2† Etienne Bastien1,5*†
Etienne Bastien1,5*†- 1Department of Pharmacology, University Teaching Hospital of Caen-Normandie, Caen, France
- 2Normandie University, UNICAEN, INSERM COMETE, U1075, Caen, France
- 3Normandie University, UNICAEN, INSERM U1086 “Interdisciplinary Research Unit for Cancers Prevention and Treatment” (ANTICIPE), Caen, France
- 4Department of Neurology, University Teaching Hospital of Caen-Normandie, Caen, France
- 5Comprehensive Cancer Center Baclesse, Unicancer, Caen, France
Importance: Endocrine therapies (ETs) and inhibitors of cyclin-dependent kinases-4/6 (iCDK4/6s) are a standard treatment in breast cancer. However, data on potential neurocognitive impacts remain inconsistent for ET and are scarce for iCDK4/6s.
Objective: To evaluate whether ET and iCDK4/6s are associated with neurocognitive impairment (NCI).
Methods: We used observational, real-world cases of NCI from the World Health Organization’s database VigiBase® to perform disproportionality analysis. Cases were defined as any symptom of NCI in females treated with ETs or iCDK4/6s. The study period was from the date of the first adverse event reported in VigiBase® with iCDK4/6s (1 January 2014) until the date of data extraction (16 March 2022). In our primary analysis, we calculated the reporting odds ratio (ROR) adjusted for age to identify a potential association between NCI and individual ETs in isolation or in combination with iCDK4/6s. We also performed subgroup analyses by the NCI class.
Results: We identified 2.582 and 1.943 reports of NCI associated with ETs and iCDK4/6s, respectively. NCI was significantly associated with each ET [anastrozole: n = 405, aROR = 1.52 (95% CI: 1.37–1.67); letrozole: n = 741, aROR = 1.37 (95% CI: 1.27–1.47); exemestane: n = 316, aROR = 1.37 (95% CI: 1.22–1.53); tamoxifen: n = 311, aROR = 1.25 (95% CI: 1.12–1.40); and fulvestrant: n = 319, aROR = 1.19 (95% CI: 1.06–1.33)] and only with palbociclib for iCDK4/6s [n = 1,542, aROR = 1.41 (95% CI: 1.34–1.48)].
Conclusion: These findings suggest that in females treated for breast cancer, all ETs may be associated with NCI. However, amongst iCDK4/6s, NCI may be specific to palbociclib. NCI most frequently involved learning and memory as well as language. Neurocognitive impact of treatments requires better consideration and management.
1 Introduction
Endocrine therapies (ETs) have contributed to a significant increase in survival for females with breast cancer. Aromatase inhibitors (AIs) (anastrozole, letrozole, and exemestane), selective estrogen-receptor modulators and degraders (SERMs and SERDs) (tamoxifen, toremifene, and fulvestrant), and gonadotrophin-releasing hormone (GnRH) analogs (leuprorelin, goserelin, and triptorelin) are used in early or metastatic ER-positive breast cancer (Cardoso et al., 2019).
Inhibitors of cyclin-dependent kinases-4/6 (iCDK4/6s) have recently revolutionized the adjuvant and first line treatment of high-risk and metastatic ER-positive breast cancer. They are used in combination to improve the efficacy of ET by acting on the cell cycle checkpoint (Roskoski, 2016). The U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) have currently approved three iCDK4/6s: abemaciclib, palbociclib, and ribociclib (Ibrance, 2018; Kisqali, 2018; Verzenios, 2018; FDA, 2019a; FDA, 2022; FDA, 2023).
By means of all these therapeutic advances, patients survive longer and are treated for more extended periods of time. Therefore, they are potentially at risk for long-term adverse events (AEs). This raises questions regarding the impact of ET on quality of life and related outcomes (Franzoi et al., 2021; Haggstrom et al., 2022; Siegel et al., 2022). Numerous studies report neurocognitive impairment (NCI) with ET (Hugo and Ganguli, 2014; Haggstrom et al., 2022). However, the literature remains scarce and conclusions inconsistent (Lange et al., 2019; Haggstrom et al., 2022). Limited data are available regarding the impact of iCDK4/6s on cognition. Nevertheless, a recent review suggests that iCDK4/6s may negatively impact cognition (Kjoe et al., 2022).
Using neurocognitive symptoms reported in the World Health Organization’s (WHO) pharmacovigilance database VigiBase®, we performed a disproportionality analysis to evaluate the association between NCI and ETs in isolation or in combination with iCDK4/6s. In secondary analyses, we described the clinical features of NCI cases reported with ETs and iCDK4/6s.
2 Methods
2.1 Pharmacovigilance study procedure
We performed a pharmacovigilance study within VigiBase®, the largest pharmacovigilance database with more than 30 million reports received from more than 160 member countries. Vigibase® has been developed to detect potential associations between drugs (including cancer treatments) and AEs (Guerrero et al., 2019; Briggs et al., 2022). AEs can be reported by healthcare or non-healthcare professionals, such as patients or manufacturers. Drugs are coded with the anatomical therapeutic chemical and AEs with the Medical Dictionary for Regulatory Activities (MedDRA). Cases were included when the imputability of NCI symptoms to ET and iCDK4/6s was defined as suspect/interacting/concomitant, using the WHODrug Global dictionary. Serious AE is defined as results in death, life threatening, require inpatient hospitalization or prolongation of existing hospitalization, results in persistent or significant disability, or at the judgment of the reporter.
As previously published, our query used the standardized MedDRA query and high-level group terms related to NCI: “dementia,” “mental impairment disorders,” “cognitive and attention disorders and disturbances,” “deliria,” “dementia and amnestic condition,” and “disturbances in thinking and perception” (Briggs et al., 2022; Gouverneur et al., 2023). In the absence of specific terms that describe drug-induced NCI and in order to avoid inclusion of neurological or psychiatric diseases, we focused our query on symptoms (Supplementary Tables S1A) and excluded all preferred terms (PTs) related to neurological or psychiatric diseases (Supplementary Tables S1B). We also classified (EMM and VLB) each of the PTs included in our study into one of the six NCI patterns defined by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5): social cognition, language, executive function, complex attention, learning and memory, and perceptual motor function (Sachdev et al., 2014).
The analysis included ETs (“letrozole,” “anastrozole,” “exemestane,” “tamoxifen,” “toremifene,” and “fulvestrant”) and iCDK4/6s (“palbociclib,” “abemaciclib,” and “ribociclib”). One drug may be associated with several PTs. We excluded GnRH analogs due to their multiple non-oncological indications. To minimize the risk of non-breast cancer indications of ETs and iCDK4/6s, the study population was restricted to females.
The protocol was approved by a hospital committee with competency for research not requiring authorization by an institutional review board (University of Caen Normandy, France; reference: 2646, dated 15 July 2021).
2.2 Statistical analysis and outcomes
We performed a pharmacovigilance disproportionality analysis using R version 4.2.1. Disproportionality analysis is performed to compare the proportion of reporting of a specific AE with a drug of interest to the expected proportion assuming the AE with this drug of interest and is independently reported (Faillie, 2019).
In our primary analysis, we first calculated the reporting odds ratio (ROR) adjusted for age to identify a potential association between NCI and each ET. Second, we calculated ROR adjusted for age to identify a potential association between NCI and each iCDK4/6. In the primary analysis, we restricted the period for the extraction of cases and non-cases from the date of the first AE reported in VigiBase® with iCDK4/6s (1 January 2014) until the date of data extraction (16 March 2022). Case characteristics were summarized with means for quantitative variables and proportions for qualitative variables. First, to avoid confounding by the presence of breast cancer in cases, we performed a sensibility analysis where we restricted non-cases to reports that include antineoplastic agents, ET and immunotherapy. Second, to avoid signal induced by reporters other than health care professionals, we repeated the analyses after restricting reports to those from health care professionals. Third, for cases exposed to ETs, to avoid confounding by the co-prescription of an iCDK4/6, we performed an additional analysis where we extracted cases and non-cases from the date of the first AE reported for each ET to the date of the first AE reported with an iCDK4/6. Fourth, a sensibility analysis was also performed after excluding reports with co-illnesses and co-treatments known to cause NCI (Supplementary Table 2).
For the primary and secondary analyses, we report 95% credibility intervals (CIs), with a lower ROR CI bound >1 denoting an association between a drug and an AE. For the effective interpretation of the signal, RORs were only calculated if there were at least five reports for a drug of interest/AE pair.
3 Results
During the study period (1 January 2014 to 16 March 2022), a total of 12,105,661 AEs were reported in Vigibase®. We identified 262,366 reports related to NCI, of which 2,583 concerned ETs and 1,943 concerned iCDK4/6s (Figure 1). A total of 3,400 reports came from the Americas (75%), 971 from Europe (21%), 64 from Eastern Mediterranean (1%), 52 from Asia (1%), and 39 from Africa (<1%). The most reported PTs were “memory impairment” (27%), “amnesia” (9%), “cognitive disorder” (6%), “disturbance in attention” (6%), and “speech disorder (5%) (Supplementary Tables S1A). After excluding cases without age information, we included 2,093 reports concerning ETs and 1,686 reports concerning iCDK4/6s in the age-adjusted primary analysis.
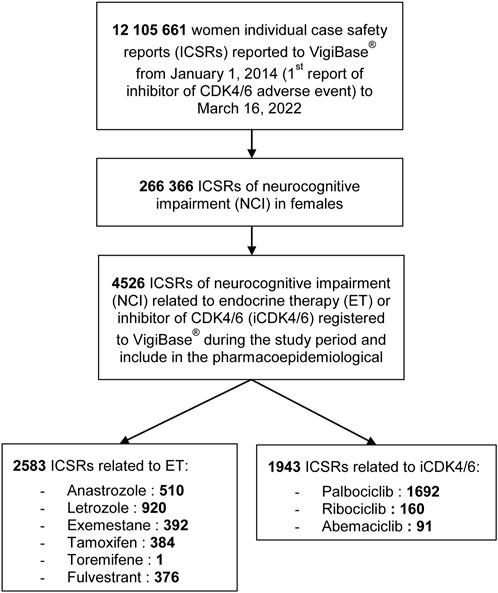
FIGURE 1. Flow chart of the pharmacovigilance study.
Reports of NCI in patients treated with ET and/or iCDK4/6s concerned all age classes: 23% of females were more than 75 years old (n = 800), 26% were between 65 and 74 years old (n = 884), 29% were between 45 and 64 years old (n = 1,009), and 5% were between 18 and 44 years old (n = 158). Age was missing in 17% of reports (n = 595). According to the WHO classification, 57% of reports related to NCI were considered serious by reporters. Treatment was interrupted in one-third of patients with serious NCI. Data on time to onset, reversibility after interruption, and treatment rechallenges were not available.
Regarding ET, anastrozole (aROR 1.52; 95% CI: 1.37–1.67), letrozole (aROR 1.37; 95% CI: 1.27–1.47), exemestane (aROR 1.37; 95% CI: 1.22–1.53), tamoxifen (aROR 1.25; 95% CI: 1.12–1.40), and fulvestrant (aROR 1.19; 95% CI: 1.06–1.33) were significantly associated with higher reporting of NCI (Table 1). Only 207 reports were available for toremifene and one included NCI, so no disproportionality was performed.
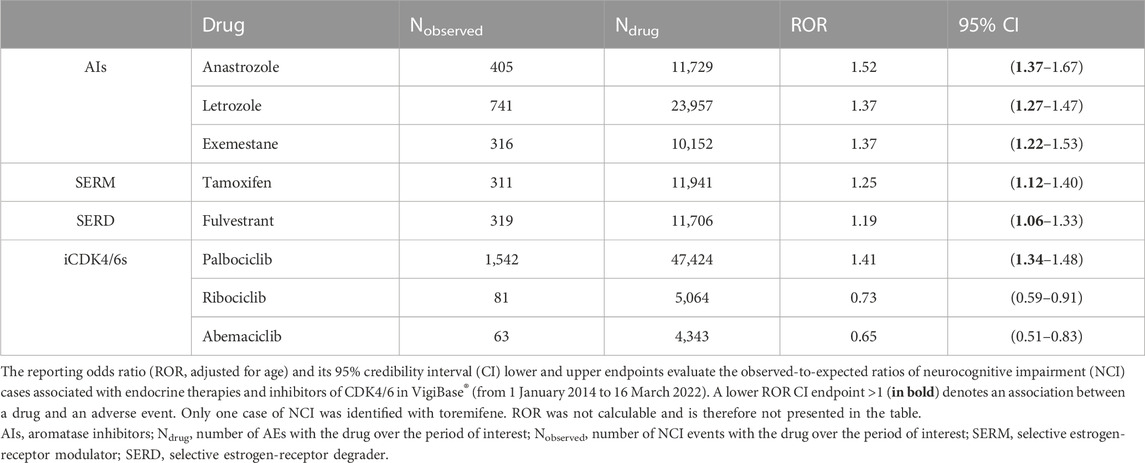
TABLE 1. Disproportionality analysis of neurocognitive impairment with individual endocrine therapies and inhibitors of CDK4/6.
Regarding iCDK4/6s, only palbociclib (aROR 1.41; 95% CI: 1.34–1.48) was significantly associated with a higher reporting of NCI. No signal was found for ribociclib (aROR 0.73; 95% CI: 0.59–0.91) and abemaciclib (aROR 0.65; 95% CI: 0.51–0.83).
After restricting non-cases to reports that include antineoplastic agents, ET, and immunotherapy, results were broadly consistent with the primary analysis except for tamoxifen (ROR 1.07; 95% CI: 0.96–1.18) and fulvestrant (ROR 1.08; 95% CI: 0.97–1.19), which were no longer statistically significant (Supplementary Table S3). After restricting reports to those from healthcare professionals, the results were broadly consistent with the primary analysis except for tamoxifen (ROR 1.11; 95% CI: 0.96–1.28), exemestane (ROR 1.09; 95% CI: 0.94–1.26), and fulvestrant (ROR 1.07; 95% CI: 0.92–1.23), which were no longer statistically significant (Supplementary Table S4). In the additional analysis that only included reports made prior to the first use of iCDK4/6s, the results were no longer statistically significant for letrozole (ROR 1.10; 95% CI: 0.99–1.23), exemestane (ROR 1.01; 95% CI: 0.86–1.18), and tamoxifen (ROR 0.91; 95% CI: 0.84–0.99) (Supplementary Table S5). Co-illnesses and co-treatments known to be associated with NCI were, respectively, present in 84 and 31 of the 4,524 reports. Due to their low number, sensitivity analyses excluding co-illnesses and co-treatments were not performed.
To better describe the cases of NCI with ETs and iCDK4/6s identified in the primary analysis, we calculated aROR for each of the six NCI patterns (Table 2). Anastrozole was significantly associated with a higher reporting of complex attention (aROR 1.36; 95% CI: 1.15–1.60), language (aROR 1.95; 95% CI: 1.65–2.30), and perceptual motor function impairments (aROR 1.25; 95% CI: 1.03–1.52). Letrozole and exemestane were associated with a higher reporting of language (aROR 2.11; 95% CI: 1.89–2.36 and aROR 2.18; 95% CI: 1.84–2.57, respectively) and learning and memory impairments (aROR 1.54; 95% CI: 1.22–1.94 and aROR 1.78; 95% CI: 1.28–2.48, respectively). Tamoxifen and fulvestrant were only associated with a higher reporting of language impairment (aROR 1.39; 95% CI: 1.14–1.70 and aROR 1.92; 95% CI: 1.63–2.27, respectively). Palbociclib was significantly associated with a higher reporting of language and learning and memory impairments (aROR 2.74; 95% CI: 2.55–2.94 and aROR 1.31; 95% CI: 1.10–1.57, respectively). No drugs were associated with a higher reporting of executive function or social cognition impairment.
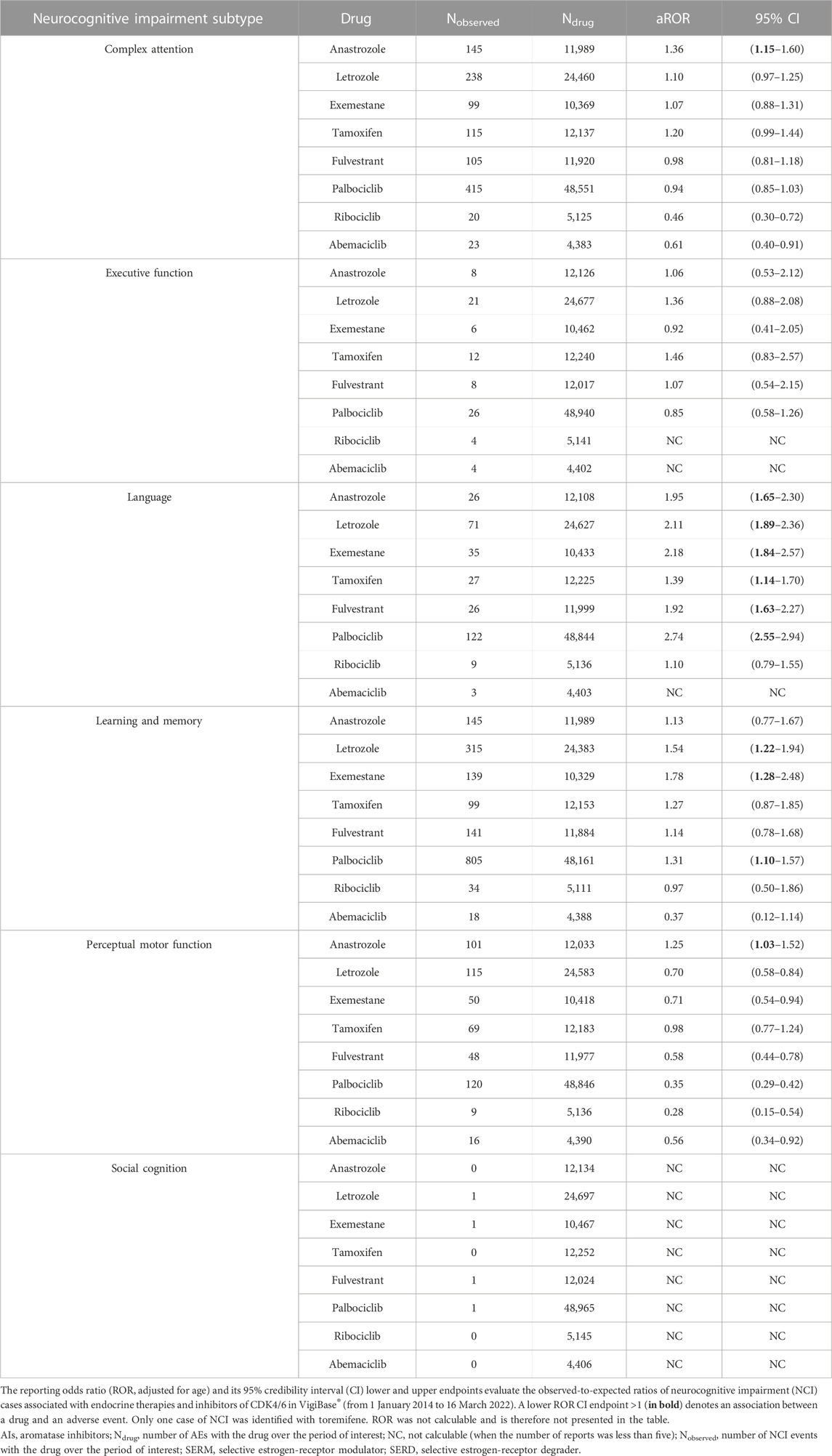
TABLE 2. Analysis of neurocognitive impairment classes with individual endocrine therapies and inhibitors of CDK4/6.
4 Discussion
Using pharmacovigilance data, we identified a significant association between reporting of NCI and AIs, tamoxifen, fulvestrant, and palbociclib. No signal was observed with the other iCDK4/6s. NCI was mainly related to learning and memory as well as language. Reports were not limited to the elderly as one-third concerned females under the age of 65.
4.1 Endocrine therapies
These results provide further evidence that all ET classes may be associated with NCI in females with breast cancer. Our results for AIs are consistent with a meta-analysis of studies that used neurocognitive tests and found the association between AIs and verbal and learning/memory impairments in females with breast cancer (Underwood et al., 2018). Our results suggest that anastrozole and exemestane could also be associated with language impairment. Several studies that used neurocognitive tests support that tamoxifen may negatively impact cognition and language and attention impairments, which is consistent with the findings of our study (Schilder et al., 2010; Boele et al., 2015). Based on neuropsychological assessments of females in randomized clinical trials that compared tamoxifen to AIs, several studies suggest that tamoxifen may lead to NCI more than AIs. In the TEAM trial, females treated with adjuvant tamoxifen had slower information processing speed than those treated with exemestane (p = 0.02; Cohen’s d = 0.36) (Schilder et al., 2010). Similarly, overall cognition of females treated with adjuvant tamoxifen in the BIG-1-98 trial was worse than those treated with letrozole (p = 0.04, Cohen’s d = 0.40) (Phillips et al., 2010). However, due to discordant results, the impact of AIs and tamoxifen on cognition remains controversial (Lange et al., 2019; Novick et al., 2020). Due to the absence of prior clinical studies aiming to assess the neurocognitive impact of fulvestrant therapy, our study provides relevant data on its neurocognitive consequences (Robertson et al., 2016).
GnRH agonists were not investigated in this study due to their wider range of indications. Data regarding the neurocognitive effect of leuprorelin in females with breast cancer remain scarce. Meta-analyses evaluated the effect of leuprorelin on cognition in men with prostate cancer and showed discordant results (Nead et al., 2017; Sun et al., 2018). Using a similar pharmacovigilance methodology, a recent study highlighted an association between androgen deprivation therapies and NCI in prostate cancer, including leuprorelin (ROR 1.47, 95% CI: 1.34; 1.62) (Briggs et al., 2022).
Estrogen receptors are expressed both on breast cancer cells and the central nervous system. Estradiol is involved in central neurotransmission and could have an impact on axonal growth. ETs may lead to NCI due to decreased estradiol activation in areas involved in cognition functions, such as the hypothalamus, amygdala, or hippocampus (Lange et al., 2019; Haggstrom et al., 2022).
4.2 Inhibitors of cyclin-dependent kinases-4/6
Concerning iCDK4/6s, our study identified a signal of NCI associated with palbociclib, mainly related with language and learning and memory impairments. In the PEARL trial, the cognition subscale of the European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire (EORTC-QLQ-C30) favored the palbociclib plus ET arm (hazard ratio = 0.70; 95% CI: 0.54–0.89) (Kahan et al., 2021). However the control arm was capecitabine, which may itself lead to NCI (Lange et al., 2019). In the PALOMA-3 trial, there was no difference in cognitive outcomes between the palbociclib and fulvestrant arms compared to the placebo and fulvestrant arms (Harbeck et al., 2021). However, the EORTC-QLQ-C30 cognition subscale is only based on two out of thirty questions and concerns self-reported cognitive impairment. The absence of a signal with abemaciclib is concordant with the results of the MONARCH-2 trial (Kaufman et al., 2020). For ribociclib, the EORTC-QLQ-C30 cognition subscale was not published in MONALEESA-3 trial. Finally, abemaciclib and ribociclib are reported more recently, and the number of reports is lower. However, the design of disproportionality analyses enables to detect signals with a low number of AEs (Cellier et al., 2023). Moreover, there was no trend toward significance for abemaciclib and ribociclib that might suggest a lack of power.
Whether iCDK4/6s affect the central nervous system is unknown. Cyclin D inhibition may alter neurogenesis and lead to NCI (Urbach and Witte, 2019; Kjoe et al., 2022). However, this does not explain why the signal in our study was isolated to palbociclib. Considering that abemaciclib has good penetrance into the central nervous system, pharmacokinetic parameters likely do not explain this potential differential effect (Hendrychová et al., 2021). The differential kinase affinity spectrum could explain why NCI may be specific to palbociclib. In contrast to abemaciclib and ribociclib, palbociclib inhibits the tropomyosin receptor kinase (TRK), encoded by the neurotrophic receptor tyrosine kinase (NTRK) genes (Hendrychová et al., 2021). Binding to the brain-derived neurotrophic factor (BDNF), TRK is a tyrosine kinase receptor which regulates neuronal development, differentiation, and survival, including those in the hippocampus. In in vitro, BDNF/TRK deprivation is associated with elevations of the β-amyloid peptide in hippocampal neurons, leading to apoptotic death (Matrone et al., 2008). In mice, deficiency of this pathway is associated with neuro-inflammation and impairment of memory and learning (Wang et al., 2019). In humans, reduced BDNF mRNA expression has been observed during post-mortem examination of patients with Alzheimer’s disease (Connor et al., 1997). NTRK fusions are observed in 0.3% of lung cancers and are targeted by two TRK inhibitors approved by the FDA: entrectinib and larotrectinib (Harada et al., 2021). Based on clinical trials, SmPCs of entrectinib and larotrectinib report NCI in, respectively, 27% and 1% of patients. Further studies are needed to determine whether inhibition of the BDNF/TRK pathway mediates NCI in patients treated with palbociclib (FDA, 2019b; FDA, 2019c).
4.3 Strengths and limitations
The present study investigated the association between NCI and ET in isolation or in combination with iCDK4/6s in females with breast cancer using the worldwide pharmacovigilance database Vigibase®, allowing us to isolate 4,526 reports of NCI associated with ET and/or iCDK4/6s. Our primary analysis was adjusted for age and is strengthened by the sensitivity analyses, suggesting that our results are not driven by age or the presence of breast cancer. Sensitivity analysis regarding the type of the reporter was less consistent, probably due to lack of power. Our secondary analysis using DSM-5 neurocognitive patterns allowed a finer description of the NCI symptoms associated with ET and palbociclib. Moreover, we used an original and complementary approach based on pharmacovigilance reports of neurocognitive symptoms rather than neuropsychological tests or self-questionnaires, such as EORTC-QLQ-C30, which are used in clinical trials (Underwood et al., 2018; Kaufman et al., 2020; Harbeck et al., 2021).
Our study had several limitations. Inherent to pharmacovigilance databases is missing data, which did not allow us to more comprehensively describe the reports. Moreover, we were unable to determine the line of treatment, previous chemotherapy, and co-prescribed ET with iCDK4/6, which could have biased the signal. In addition, Vigibase® does not allow access to medical records to confirm the diagnosis of NCI and eliminate differential diagnosis (such as depression and cerebral metastases). To limit non-breast cancer indications, we restricted our analysis to cases in females. It would be necessary to conduct similar analyses to extend these results to males. Last, disproportionality pharmacovigilance analyses identify new AE signals that require confirmation with the high level of evidence studies (Faillie, 2019). They are also necessary to determine the incidence of NCI.
5 Conclusion
This pharmacovigilance study strengthens the association between ET and NCI in females with breast cancer. We highlighted a new signal for iCDK4/6s isolated to palbociclib, which requires further research. NCI impacted all exposed age groups and mostly involved learning, memory, and language. Neurocognitive impact of breast cancer treatments must be better considered. NCI management involves non-pharmacological approaches that need to be developed.
Data availability statement
Publicly available datasets were analyzed in this study. These data can be found at: public access to overview statistics from VigiBase® can be gained through the VigiAccess website, http://www.vigiaccess.org/.
Ethics statement
The studies involving humans were approved by the Institutional review board: University of Caen Normandy, France; reference: 2646, dated 15 July 2021. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
RP: data curation, formal analysis, investigation, software, and writing–original draft. BC: conceptualization, formal analysis, methodology, software, and writing–review and editing. E-MM: formal analysis, methodology, software, and writing–review and editing. CD: methodology, software, and writing–review and editing. AD-S, AN, and FJ: writing–review and editing. VL-B: resources and writing–review and editing. EB: conceptualization, formal analysis, investigation, methodology, project administration, supervision, visualization, and writing–original draft.
Funding
The authors declare that financial support was received for the research, authorship, and/or publication of this article. This study was funded by CHU Caen Normandie and Université de Caen Normandie.
Acknowledgments
The authors thank the custom searches team at the Uppsala Monitoring Centre (Uppsala, Sweden) research section for providing access to VigiBase® (the WHO global database of individual case safety reports), without whom this study would not have been possible. The information presented in this study does not represent the opinion of the Uppsala Monitoring Centre or the World Health Organization.
Conflict of interest
FJ has received consulting fees from AstraZeneca, GSK, Janssen, and Ipsen and declares honoraria for lectures and scientific boards from AstraZeneca.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1278682/full#supplementary-material
References
Boele, F. W., Schilder, C. M. T., de Roode, M. L., Deijen, J. B., and Schagen, S. B. (2015). Cognitive functioning during long-term tamoxifen treatment in postmenopausal women with breast cancer. Menopause 22 (1), 17–25. doi:10.1097/GME.0000000000000271
Briggs, L. G., Reese, S., Herzog, P., Nguyen, D. D., Labban, M., Alkhatib, K., et al. (2022). Neurocognitive impairment associated with traditional and novel androgen receptor signaling inhibitors ± androgen deprivation therapy: a pharmacovigilance study. Prostate Cancer Prostatic Dis. 26, 331–337. doi:10.1038/s41391-022-00541-6
Cardoso, F., Kyriakides, S., Ohno, S., Penault-Llorca, F., Poortmans, P., Rubio, I. T., et al. (2019). Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 30 (8), 1194–1220. doi:10.1093/annonc/mdz173
Cellier, M., Bourneau-Martin, D., Abbara, C., Crosnier, A., Lagarce, L., Garnier, A. S., et al. (2023). Renal safety profile of BCR-ABL tyrosine kinase inhibitors in a real-life setting: a study based on Vigibase®, the WHO pharmacovigilance database. Cancers 15 (7), 2041. doi:10.3390/cancers15072041
Connor, B., Young, D., Yan, Q., Faull, R. L. M., Synek, B., and Dragunow, M. (1997). Brain-derived neurotrophic factor is reduced in Alzheimer’s disease. Mol. Brain Res. 49 (1), 71–81. doi:10.1016/S0169-328X(97)00125-3
Faillie, J. L. (2019). Case–non-case studies: principle, methods, bias and interpretation. Therapies 74 (2), 225–232. doi:10.1016/j.therap.2019.01.006
FDA (2022). FDA approves abemaciclib with endocrine therapy for early breast cancer. Published online January 31 Available at: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-abemaciclib-endocrine-therapy-early-breast-cancer (Accessed August 4, 2023).
FDA (2019b). FDA approves entrectinib for NTRK solid tumors and ROS-1 NSCLC. Published online December 20 Available at: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-entrectinib-ntrk-solid-tumors-and-ros-1-nsclc (Accessed December 19, 2022).
FDA (2019c). FDA approves larotrectinib for solid tumors with NTRK gene fusions. Published online December 20 Available at: https://www.fda.gov/drugs/fda-approves-larotrectinib-solid-tumors-ntrk-gene-fusions-0 (Accessed December 19, 2022).
FDA (2019a). Research C for DE and. Palbociclib (IBRANCE). Published online September 2, 2019 Available at: https://www.fda.gov/drugs/resources-information-approved-drugs/palbociclib-ibrance (Accessed August 4, 2023).
FDA (2023). Research C for DE and. Ribociclib (Kisqali). Published online March 5 Available at: https://www.fda.gov/drugs/resources-information-approved-drugs/ribociclib-kisqali (Accessed August 4, 2023).
Franzoi, M. A., Agostinetto, E., Perachino, M., Del Mastro, L., de Azambuja, E., Vaz-Luis, I., et al. (2021). Evidence-based approaches for the management of side-effects of adjuvant endocrine therapy in patients with breast cancer. Lancet Oncol. 22 (7), e303–e313. doi:10.1016/S1470-2045(20)30666-5
Gouverneur, A., Sanchez-Pena, P., Veyrac, G., Salem, J. E., Bégaud, B., and Bezin, J. (2023). Neurocognitive disorders associated with PCSK9 inhibitors: a pharmacovigilance disproportionality analysis. Cardiovasc Drugs Ther. 37 (2), 271–276. doi:10.1007/s10557-021-07242-7
Guerrero, E., Johnson, D. B., Bachelot, A., Lebrun-Vignes, B., Moslehi, J. J., and Salem, J. E. (2019). Immune checkpoint inhibitor–associated hypophysitis—World Health Organisation VigiBase report analysis. Eur. J. Cancer 113, 10–13. doi:10.1016/j.ejca.2019.03.002
Haggstrom, L. R., Vardy, J. L., Carson, E. K., Segara, D., Lim, E., and Kiely, B. E. (2022). Effects of endocrine therapy on cognitive function in patients with breast cancer: a comprehensive review. Cancers 14 (4), 920. doi:10.3390/cancers14040920
Harada, G., Santini, F. C., Wilhelm, C., and Drilon, A. (2021). NTRK fusions in lung cancer: from biology to therapy. Lung Cancer 161, 108–113. doi:10.1016/j.lungcan.2021.09.005
Harbeck, N., Rastogi, P., Martin, M., Tolaney, S. M., Shao, Z. M., Fasching, P. A., et al. (2021). Adjuvant abemaciclib combined with endocrine therapy for high-risk early breast cancer: updated efficacy and Ki-67 analysis from the monarchE study. Ann. Oncol. 32 (12), 1571–1581. doi:10.1016/j.annonc.2021.09.015
Hendrychová, D., Jorda, R., and Kryštof, V. (2021). How selective are clinical CDK4/6 inhibitors? Med. Res. Rev. 41 (3), 1578–1598. doi:10.1002/med.21769
Hugo, J., and Ganguli, M. (2014). Dementia and cognitive impairment: epidemiology, diagnosis, and treatment. Clin. Geriatric Med. 30 (3), 421–442. doi:10.1016/j.cger.2014.04.001
Ibrance, E. M. A. (2018). European Medicines agency. Published September 17 Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/ibrance (Accessed August 4, 2023).
Kahan, Z., Gil-Gil, M., Ruiz-Borrego, M., Carrasco, E., Ciruelos, E., Muñoz, M., et al. (2021). Health-related quality of life with palbociclib plus endocrine therapy versus capecitabine in postmenopausal patients with hormone receptor–positive metastatic breast cancer: patient-reported outcomes in the PEARL study. Eur. J. Cancer 156, 70–82. doi:10.1016/j.ejca.2021.07.004
Kaufman, P. A., Toi, M., Neven, P., Sohn, J., Grischke, E. M., Andre, V., et al. (2020). Health-related quality of life in MONARCH 2: abemaciclib plus fulvestrant in hormone receptor-positive, HER2-negative advanced breast cancer after endocrine therapy. Oncol. 25 (2), e243–e251. doi:10.1634/theoncologist.2019-0551
Kisqali, E. M. A. (2018). European Medicines agency. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/kisqali (Accessed August 4, 2023).
Kjoe, PRLM, van der Wall, E., and Schagen, S. B. (2022). Endocrine therapy with or without CDK4/6 inhibitors in women with hormone-receptor positive breast cancer: what do we know about the effects on cognition? Clin. Breast Cancer 22 (3), 191–199. doi:10.1016/j.clbc.2021.08.002
Lange, M., Joly, F., Vardy, J., Ahles, T., Dubois, M., Tron, L., et al. (2019). Cancer-related cognitive impairment: an update on state of the art, detection, and management strategies in cancer survivors. Ann. Oncol. 30 (12), 1925–1940. doi:10.1093/annonc/mdz410
Matrone, C., Ciotti, M. T., Mercanti, D., Marolda, R., and Calissano, P. (2008). NGF and BDNF signaling control amyloidogenic route and Abeta production in hippocampal neurons. Proc. Natl. Acad. Sci. 105 (35), 13139–13144. doi:10.1073/pnas.0806133105
Nead, K. T., Sinha, S., and Nguyen, P. L. (2017). Androgen deprivation therapy for prostate cancer and dementia risk: a systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 20 (3), 259–264. doi:10.1038/pcan.2017.10
Novick, A. M., Scott, A. T., Neill Epperson, C., and Schneck, C. D. (2020). Neuropsychiatric effects of tamoxifen: challenges and opportunities. Front. Neuroendocrinol. 59, 100869. doi:10.1016/j.yfrne.2020.100869
Phillips, K. A., Ribi, K., Sun, Z., Stephens, A., Thompson, A., Harvey, V., et al. (2010). Cognitive function in postmenopausal women receiving adjuvant letrozole or tamoxifen for breast cancer in the BIG 1-98 randomized trial. Breast 19 (5), 388–395. doi:10.1016/j.breast.2010.03.025
Robertson, J. F. R., Bondarenko, I. M., Trishkina, E., Dvorkin, M., Panasci, L., Manikhas, A., et al. (2016). Fulvestrant 500 mg versus anastrozole 1 mg for hormone receptor-positive advanced breast cancer (FALCON): an international, randomised, double-blind, phase 3 trial. Lancet 388 (10063), 2997–3005. doi:10.1016/S0140-6736(16)32389-3
Roskoski, R. (2016). Cyclin-dependent protein kinase inhibitors including palbociclib as anticancer drugs. Pharmacol. Res. 107, 249–275. doi:10.1016/j.phrs.2016.03.012
Sachdev, P. S., Blacker, D., Blazer, D. G., Ganguli, M., Jeste, D. V., Paulsen, J. S., et al. (2014). Classifying neurocognitive disorders: the DSM-5 approach. Nat. Rev. Neurol. 10 (11), 634–642. doi:10.1038/nrneurol.2014.181
Schilder, C. M., Seynaeve, C., Beex, L. V., Boogerd, W., Linn, S. C., Gundy, C. M., et al. (2010). Effects of tamoxifen and exemestane on cognitive functioning of postmenopausal patients with breast cancer: results from the neuropsychological side study of the tamoxifen and exemestane adjuvant multinational trial. JCO 28 (8), 1294–1300. doi:10.1200/JCO.2008.21.3553
Siegel, R. L., Miller, K. D., Fuchs, H. E., and Jemal, A. (2022). Cancer statistics, 2022. CA A Cancer J. Clin. 72 (1), 7–33. doi:10.3322/caac.21708
Sun, M., Cole, A. P., Hanna, N., Mucci, L. A., Berry, D. L., Basaria, S., et al. (2018). Cognitive impairment in men with prostate cancer treated with androgen deprivation therapy: a systematic review and meta-analysis. J. Urology 199 (6), 1417–1425. doi:10.1016/j.juro.2017.11.136
Underwood, E. A., Rochon, P. A., Moineddin, R., Lee, P. E., Wu, W., Pritchard, K. I., et al. (2018). Cognitive sequelae of endocrine therapy in women treated for breast cancer: a meta-analysis. Breast Cancer Res. Treat. 168 (2), 299–310. doi:10.1007/s10549-017-4627-4
Urbach, A., and Witte, O. W. (2019). Divide or commit – revisiting the role of cell cycle regulators in adult hippocampal neurogenesis. Front. Cell Dev. Biol. 7, 55. doi:10.3389/fcell.2019.00055
Verzenios, E. M. A. (2018). European Medicines agency. Published September 17 Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/verzenios (Accessed August 4, 2023).
Keywords: breast cancer, endocrine therapy, cyclin-dependent kinase 4/6 inhibitor, neurocognitive impairment, pharmacoepidemiology
Citation: Prevost R, Chretien B, Minoc E-M, Dolladille C, Da-Silva A, Nehme A, Joly F, Lelong-Boulouard V and Bastien E (2023) Neurocognitive impairment in females with breast cancer treated with endocrine therapy and CDK4/6 inhibitors: a pharmacovigilance study using the World Health Organization’s database. Front. Pharmacol. 14:1278682. doi: 10.3389/fphar.2023.1278682
Received: 16 August 2023; Accepted: 04 October 2023;
Published: 20 October 2023.
Edited by:
Yusuf Karatas, Çukurova University, TürkiyeReviewed by:
Yasser Alatawi, University of Tabuk, Saudi ArabiaAlexander T. Sougiannis, Medical University of South Carolina, United States
Copyright © 2023 Prevost, Chretien, Minoc, Dolladille, Da-Silva, Nehme, Joly, Lelong-Boulouard and Bastien. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Etienne Bastien, etienne.bastien.jmc@gmail.com
†ORCID: Rachel Prevost, orcid.org/0000-0003-1342-1720; Basile Chretien, orcid.org/0000-0002-7483-2489; Angélique Da-Silva, orcid.org/0000-0002-8193-5144; Ahmad Nehme, orcid.org/0000-0002-7700-6799; Florence Joly, orcid.org/0000-0001-6168-4942; Véronique Lelong-Boulouard, orcid.org/0000-0002-7876-7266; Etienne Bastien, orcid.org/0000-0002-9390-1523