Ranibizumab for the treatment of retinopathy of prematurity: systematic review and meta-analysis
 Niza Alva1,2
Niza Alva1,2  Alex R. Martínez1,2
Alex R. Martínez1,2  Brando Ortiz-Saavedra3
Brando Ortiz-Saavedra3  Elizbet S. Montes-Madariaga2,3
Elizbet S. Montes-Madariaga2,3  Alonso Cotrina4
Alonso Cotrina4  José A. Caballero-Alvarado5
José A. Caballero-Alvarado5  Ranjit Sah6,7,8
Ranjit Sah6,7,8  Joshuan J. Barboza9*
Joshuan J. Barboza9*
- 1Facultad de Medicina, Universidad Peruana de Ciencias Aplicadas, Lima, Peru
- 2Unidad de Revisiones Sistemáticas y Meta-Análisis, Tau-Relaped Group, Lima, Peru
- 3Facultad de Medicina, Universidad Nacional de San Agustín de Arequipa, Arequipa, Peru
- 4Facultad de Medicina, Universidad Peruana Cayetano Heredia, Lima, Peru
- 5Facultad de Medicina, Universidad Privada Antenor Orrego, Trujillo, Peru
- 6Institute of Medicine, Tribhuvan University Teaching Hospital, Kathmandu, Nepal
- 7Department of Microbiology, Dr. D. Y. Patil Medical College, Hospital and Research Centre, Dr. D. Y. Patil Vidyapeeth, Pune, India
- 8Department of Public Health Dentistry, Dr. D.Y. Patil Dental College and Hospital, Dr. D.Y. Patil Vidyapeeth, Pune, India
- 9Escuela de Medicina, Universidad Cesar Vallejo, Trujillo, Peru
Anti-VEGF drugs like ranibizumab can be used to treat retinopathy of prematurity (ROP) by halting the formation of abnormal blood vessels, or lasers can be used to burn the edges of the retina where these vessels are present. The objective is to compare the efficacy for ROP between ranibizumab and laser therapy.
Material and methods: Electronic searches will be carried out in medical databases with key words and controlled vocabulary terms. Randomized controlled trials (RCT) will be assessed. The primary outcome will be the full ROP regression. Two reviewers will extract the data using predefined forms and, to assess the quality of the study, we will use RoB 2.0, the tool for randomized controlled trials developed by the Cochrane Collaboration. We used a combination of the inverse-variance approach and random-effects models for the meta-analysis.
Results: The eyes of 182 preterm infants who had ranibizumab treatment were assessed in a total of 364 eyes, and 135 infants received laser therapy. The follow-up period was between 6 and 24 months. Ranibizumab was not associated with greater regression of ROP compared to laser therapy in preterm infants (RR: 1.09, CI 95%: 0.95–1.24; p: 0.22). Also, ranibizumab was not associated with recurrence of ROP compared to laser therapy in preterm infants (RR: 3.77, CI 95%: 0.55–25.81; p: 0.22).
Conclusions: The efficacy of ranibizumab compared to laser is very uncertain in terms of ROP regression and decreased ROP recurrence in preterm infants.
Systematic Review Registration: identifier PROSPERO (CRD42022324150).
1. Introduction
Due to the growth of abnormal blood vessels in the retina, retinopathy of prematurity (ROP), a developmental condition in preterm neonates before 31 weeks, can cause low visual acuity or juvenile blindness (1). This condition can be treated with intravitreal injections to stop these vessel growth or laser photocoagulation to ablate the aberrant vascularization and prevent further damage (2). This condition has also been linked to infant morbidities such as sepsis, intraventricular bleeding, respiratory distress syndrome, and low weight gain (3).
By 36–40 weeks of gestation, the normal vessel proliferation is complete, starting around 12 weeks. Prior to that, the optic disc is where normal proliferation begins, before moving on to the ora serrata (4). The retina of newborns is underdeveloped and has an avascular zone. The pathology has two phases: first, it has an avascular zone owing to hyperoxia or fluctuating oxygen levels, and second, the avascular zone of retina results in a high concentration of vascular endothelial growth factor (VEGF), which promotes the formation of abnormal vasculature (5). The medication used for intravitreal injections include ranibizumab and bevacizumab (6), which are anti-VEGF, both have shown low prevalence of developing refractive errors in the future although bevacizumab-treated eyes in severe cases of ROP were linked to a higher likelihood of myopia or neurodevelopmental damage (7).
Currently, anti-VEGF agents are not approved by the Food and Drug Administration (FDA) for the treatment of ROP (8, 9). However, current consensus ROP screening guidelines published by the American Academy of Pediatrics in conjunction with the American Academy of Ophthalmology recommend the use of intravitreal anti-VEGF as a promising treatment for ROP type 1 and other types of ROP (10). In recent clinical trials ranibizumab was revealed to be an effective and safe treatment compared to laser therapy. Despite the fact that it is linked to higher immediate results and lower risk of unfavorable structural changes, it is important to consider the risk of complications that can be proper of the procedure and also the necessity of constant subsequent examinations to prevent late reactivation of ROP or long-term complications.
This systematic review assessed all of the known controlled studies of ranibizumab compared with laser photocoagulation. The aim is to compare the efficacy for ROP between ranibizumab and laser therapy.
2. Materials and methods
2.1. Search of studies
Electronic searches were carried out in EMBASE, Pubmed, Web of Science (WOS) and Scopus. Keywords and controlled vocabulary terms [i.e., medical subheading (MeSH) terms EMTREE terms] included patient-related terms (premature, retinopathy of prematurity) and treatment-related terms (ranibizumab). There was not a limit by year of publication. Two writers conducted the search. This study was reported following the recommendations of PRISMA-2020 guidelines.
2.2. Eligibility criteria
Randomized controlled trials (RCTs) and nonrandomized intervention studies (NRIS) in preterm newborns (<31 weeks of gestational age), studying ranibizumab administration to manage ROP were included but only RCTs comparing ranibizumab use with laser photocoagulation were considered for meta-analysis. We excluded case reports, editorials, narrative reviews, observational studies, and other systematic reviews.
2.3. Search of studies
Two reviewers extracted data using predefined forms. After eliminating duplicates, two independent reviewers examined each article by first considering only the title and abstract of the study, and then two independent reviewers evaluated the full text of the initially included studies.
2.4. Outcomes
We established as the primary outcome the complete regression of ROP and the ones defined as secondaries recurrence of ROP, change of treatment, refractive error, and adverse events (retinal or vitreous hemorrhage, endophthalmitis, conjunctivitis, corneal opacity, cataract, or other complications).
2.5. Data extraction and management
Three reviewers independently extracted relevant data from those included in a pre-established electronic sheet and conflicts were resolved jointly by consensus. The data to evaluate was: principal author, year of publication, clinical trial design, clinical trial phase, country(ies) involved in the study, number of individuals per arm, characteristics of the intervention (ranibizumab) and of the comparison, primary (complete ROP regression) and secondary outcomes.
2.6. Evaluation of the quality
The Cochrane Collaboration tool for randomized controlled trials (RoB 2.0) was utilized for conducting the quality assessment.
2.7. Strategy for data synthesis
We selected the random-effects model and inverse variance method to perform the meta-analysis of our established outcomes (11). Similar to other previous studies applied (12), we evaluated the Paule-Mandel estimator to assess between-study variance (13). The effects of ranibizumab on continuous outcomes were expressed as mean difference (MD) with 95% confidence intervals (95% CI). For dichotomous outcomes, we assessed relative risk (RR) with CI 95%. For each trial arm the baseline values for continuing outcomes have been adjusted. I2 statistic was used to regulate the statistical heterogeneity of effects in the RCTs as it was used in other meta-analyses (14–16), which had 3 categories for the level of heterogeneity: high (>60%), medium (30%–60%), and low (<30%) (17).
The model for analyzing the sensitivity in this meta-analysis was Fixed-effects, and for the methods, the Mantel-Haenszel method for the primary outcomes. In this article, we used the metacont and metabin functions of the meta package of the R 3.5.1 software. In addition to this, to evaluate the quality of evidence (QoE) we utilize the GRADE approach (18). We appraised imprecision, publication bias, risk of bias, quality of evidence and inconsistency among studies. We execute confidence ratings as very low, low, moderate and high. In SoF (summary of results) tables we specified QoE and at the end, we created the SoF tables applying GRADEpro GDT.
3. Results
3.1. Study selection
The method of searching retrieved a total of 471 items. The PRISMA flow chart displays the selection methodology (PRISMA 2020) (19). We reviewed 295 articles after removing duplicates which were 176 in total. Subsequent to an exhaustive review of the titles and abstracts, we chose 28 articles for a full-text read; from them, 6 were deemed suitable for systematic review (20–25) (Figure 1).
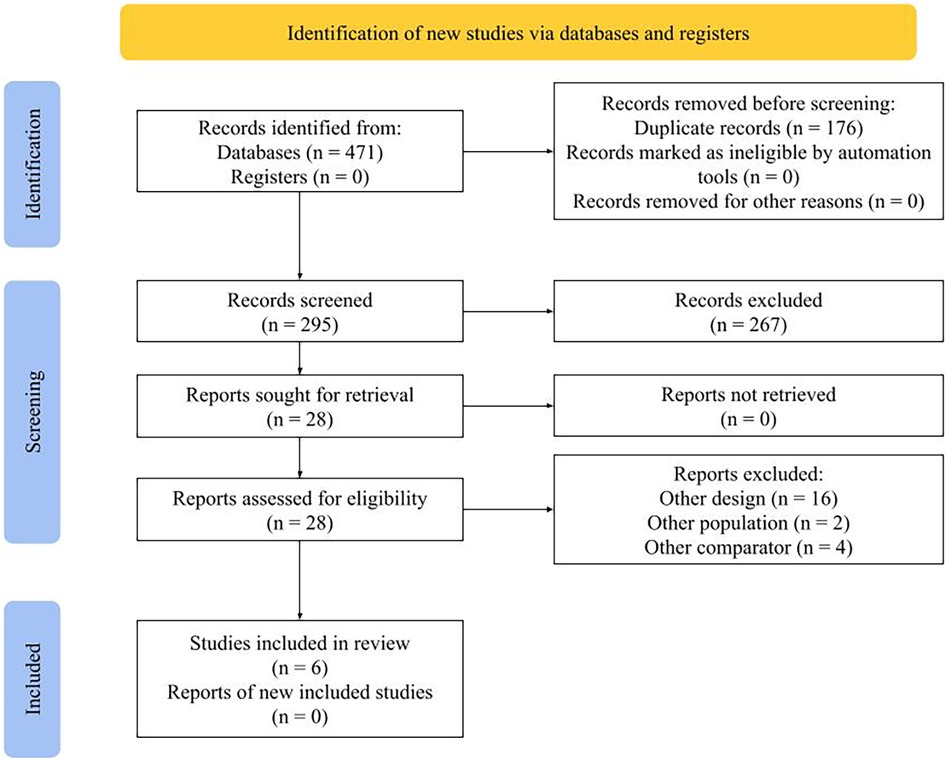
Figure 1. PRISMA-2020 flowchart of study selection.
3.2. Selected studies aspects
Altogether, 364 eyes of 182 preterm newborns treated with ranibizumab were evaluated, and 135 newborns were treated with laser. The mean of gestational age was 26.7 weeks (SD: 1.8). We included two open label RCT's (21, 22). One trial (RAINBOW study) reported results at 6 months (22, 25) and 24 months (23, 24) in 4 articles. Likewise, we founded one NRSI open label study (20). The follow-up time was ranged 6–24 months. The population considered between studies were preterm newborns diagnosed with ROP zone 1, zone 2, or AP-ROP (Table 1).
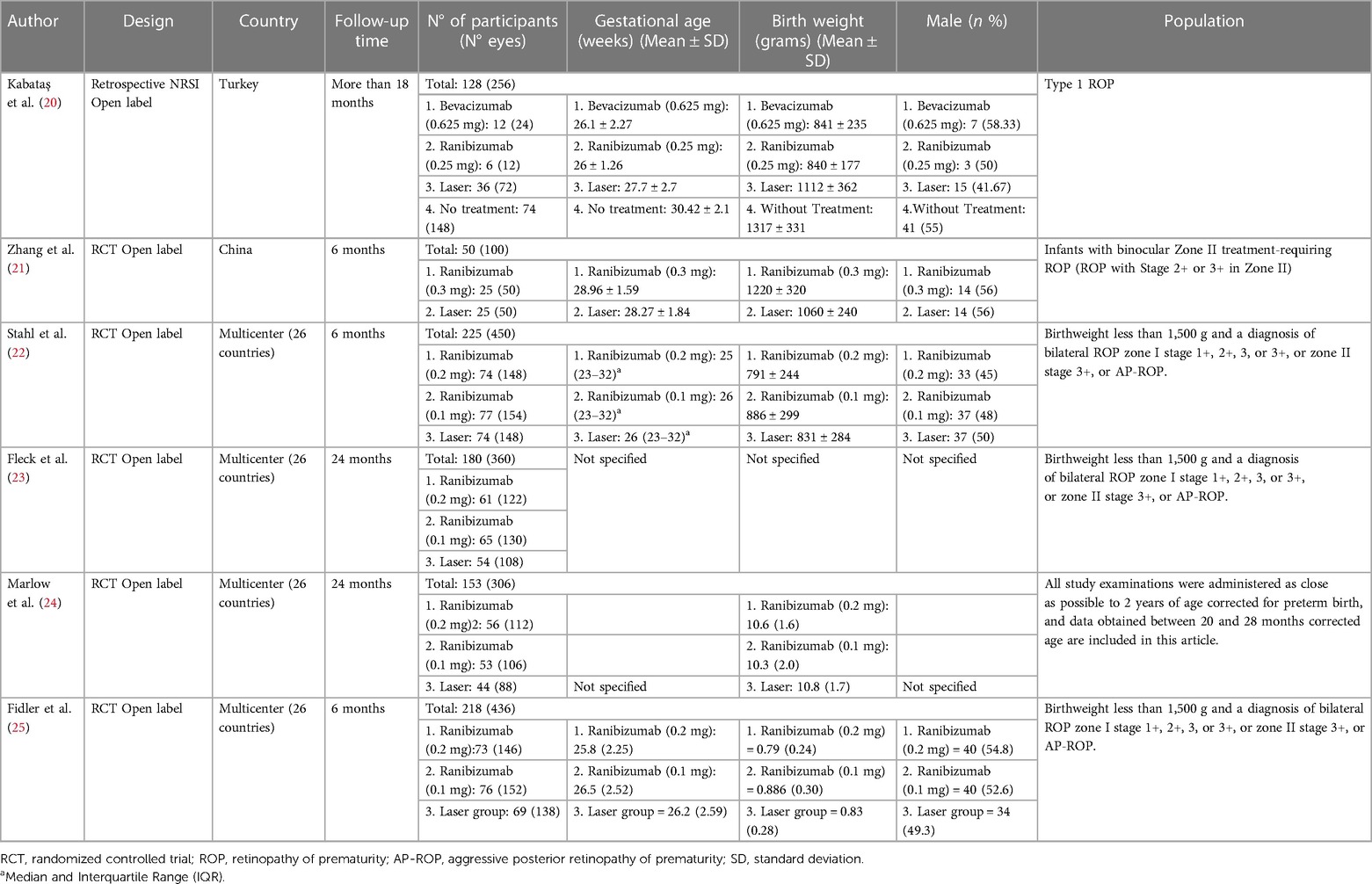
Table 1. Characteristics of included studies.
3.3. Risk of bias
Using the RoB-2 tool to assess the risk of bias, the studies by Zhang et al. (21) and Stahl et al. (22) received a high-risk score due to the presence of high risk in the randomization process and measurement of the outcome (Figure 2).
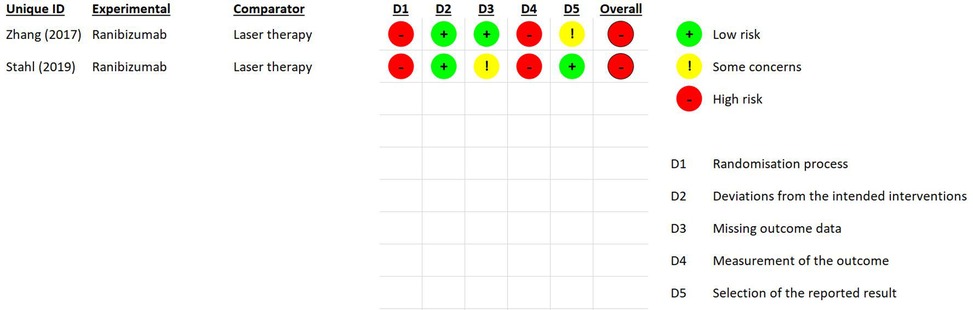
Figure 2. Risk of bias summary.
3.4. Effect of ranibizumab on primary and secondary outcomes
Ranibizumab was not associated with greater regression of ROP compared to laser therapy in preterm infants (RR: 1.09, CI 95%: 0.95–1.24; p: 0.22; Figure 3). Also, ranibizumab was not associated with recurrence of ROP compared to laser therapy in preterm infants (RR: 3.77, CI 95%: 0.55–25.81; p: 0.22; Figure 4).
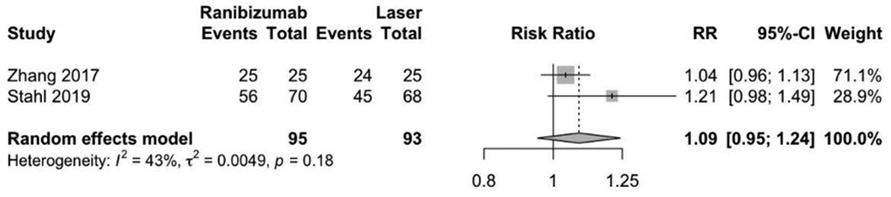
Figure 3. Forest plot of effect of ranibizumab on regression of ROP.
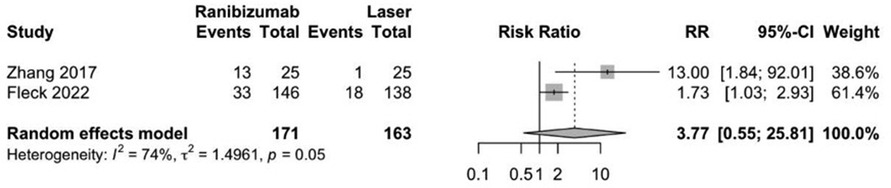
Figure 4. Forest plot of effect of ranibizumab on recurrence of ROP.
3.5. Adverse effects and/or complications
No serious adverse events or serious complications related to ranibizumab treatment were reported. Table 2 shows the adverse events and/or complications reported in the studies.
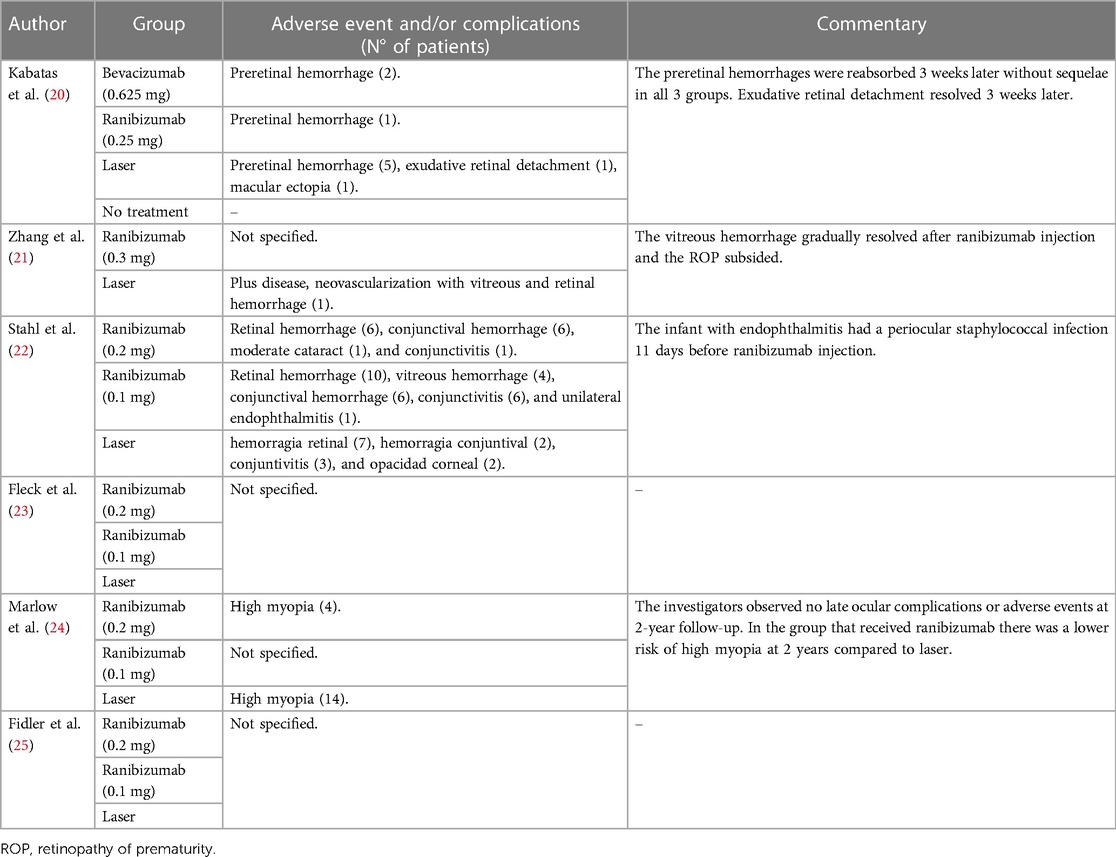
Table 2. Adverse events and/or complications reported.
3.6. Certainty of evidence
There is a very low level of certainty of evidence for the use of ranibizumab compared to laser in the regression and recurrence of ROP. This is related to the risk domains of bias, imprecision, and inconsistency (Table 3).

Table 3. Summary of findings.
4. Discussion
This systematic review and meta-analysis founded that ranibizumab did not increase the regression of ROP and the recurrence of ROP compared to laser therapy.
In the individual results of the RCTs, we founded a few things that were at odds with our overall conclusions. For example, in the study by Fleck et al. (2022), it was stated that ROP decreased significantly faster after an intravitreal injection of ranibizumab than when there was more disease, stage 3 ROP, or ROP-AP (aggressive posterior), compared to laser treatment (23).
The study by Stahl A. et al. discovered that treatment success occurred in 56 (80%) of 70 infants receiving ranibizumab 0–2 mg compared with 57 (75%) of 76 infants receiving ranibizumab 0–1 mg and 45 (66%) of 68 infants following laser therapy, despite the fact that few studies have found specific treatment-related outcomes (22).
ROP is a medical disorder that impacts the retinal development of preterm infants (26). It is caused by abnormal proliferation of blood vessels in the retina, which can result in scarring, retinal detachment, and visual loss. ROP is a dangerous disorder that, if left untreated, can result in irreversible visual impairment or blindness (27).
Infants born extremely early or with an extremely low birth weight have the highest chance of developing ROP. Laser surgery or other methods may be used to halt the aberrant blood vessel development and avoid additional retinal damage (28).
The BEAT-ROP (bevacizumab) (29) and RAINBOW (ranibizumab) (24) trials reported a lower prevalence of very high and high myopia, respectively, compared with laser therapy. The proposed mechanisms that explain why laser therapy increases the risk of high myopia are controversial (30). It was previously reported that intravitreal bevacizumab (anti-VEGF) allows retinal vessel development beyond the neovascular ridges (31), which is minimal after laser use. This event probably allows the expression of signaling pathways necessary for the development of the anterior segment with minimal myopia (29).
The specific etiology of ROP is unknown, however it is believed to be associated with aberrant blood vessel proliferation in preterm newborns’ retinas (32).
The VEGF is a protein that is involved in the pathophysiology of ROP and plays a vital function in the formation of blood vessels (33).
Under normal conditions, VEGF production is tightly controlled to enable healthy development of blood vessels in the retina (34).
However, in preterm infants, the retinal blood vessels may not be fully grown, making them more susceptible to fluctuations in oxygen levels. In an attempt to accelerate the creation of new blood vessels, cells in the retina may release excessive levels of VEGF when the infant encounters hypoxia (35).
Retinal cells generate VEGF, which encourages the formation of new blood vessels. Under normal conditions, VEGF production is tightly controlled to enable healthy development of blood vessels in the retina (36).
In preterm infants, however, VEGF synthesis may be aberrant, resulting in faulty blood vessel development in the retina. This can lead to the development of ROP, which can result in retinal scarring and detachment and visual loss (37).
The dysregulation of VEGF production in response to hypoxia (oxygen deficiency) is believed to have a major role in the development of aberrant blood vessel growth and neovascularization in ROP (38).
VEGF inhibitors, such as ranibizumab, have been utilized to treat ROP by reducing the synthesis of VEGF and halting the aberrant development of blood vessels (39).
Bevacizumab has also been studied as a treatment for ROP with encouraging results (29, 31). However, in preterm infants, use of bevacizumab showed a serum half-life of 21 days and persistent detectable levels after 60 days (40). On the other hand, ranibizumab showed a much shorter serum half-life (5.6 days) and greatly decreased serum levels at 28 days (25). Adequate ocular retention and rapid systemic excretion of ranibizumab may provide satisfactory ocular efficacy and a favorable systemic safety profile (25).
5. Conclusions
The evidence for the efficacy of ranibizumab compared to laser is very uncertain in terms of ROP regression and decreased ROP recurrence in preterm infants. Although individual evidence may support the efficacy of ranibizumab, the differences between studies do not allow us to generalize in its favor. Consideration should be given to analyzing more findings where comparisons are less heterogeneous, so as to ensure quality and certainty of evidence.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
Conceptualization, NA, AM, BO-S, EM-M, AC, JC-A, JJB; methodology, NA, AM, BO-S, EM-M, AC, JC-A, JJB; software, NA, AM, BO-S, EM-M, AC, JC-A, JJB; validation, NA, AM, BO-S, EMM, AC, JC-A, JJB; formal analysis, NA, AM, BO-S, EM-M, AC, JCA, JJB; investigation, NA, AM, BO-S, EM-M, AC, JC-A, JJB; resources, NA, AM, BO-S, EM-M, AC, JC-A, JJB; data curation, NA, AM, BO-S, EM-M, AC, JC-A, JJB; writing—original draft preparation, NA, AM, BO-S, EM-M, AC, JC-A, JJB; writing—review and editing, NA, AM, BO-S, EM-M, AC, JC-A, RS, JJB; visualization, NA, AM, BO-S, EM-M, AC, JC-A, JJB; supervision, NA, AM, BOS, EM-M, AC, JC-A, RS, JJB; project administration, NA, AM, BO-S, EM-M, AC, JC-A, RS, JJB; funding acquisition, JJB. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Neamah GT, Nwuaini MQA, Abd KA, Nasrawi AJM, Hussein SRM. Retinopathy of prematurity, a two-year experience at the ROP screening unit from AL-Zahraa teaching hospital, AL-Najaf, Iraq. J Med Life. (2022) 15:1431–6. doi: 10.25122/jml-2022-0060
2. Magnani JE, Moinuddin O, Pawar M, Sathrasala S, McCaffery H, Vartanian RJ, et al. Quantitative analysis of tear angiogenic factors in retinopathy of prematurity: a pilot biomarker study. J AAPOS. (2023) 27(14):14.e1–e6. doi: 10.1016/j.jaapos.2022.10.007
3. De Las Rivas Ramírez N, Luque Aranda G, Rius Díaz F, Pérez Frías FJ, Sánchez Tamayo T. Risk factors associated with retinopathy of prematurity development and progression. Sci Rep. (2022) 12:21977. doi: 10.1038/s41598-022-26229-4
4. Vishwakarma S, Kaur I. Molecular mediators and regulators of retinal angiogenesis. Semin Ophthalmol. (2023) 38:124–33. doi: 10.1080/08820538.2022.2152706
5. Sehgal P, Narang S, Chawla D, Gupta S, Jain S, Sharma U, et al. Systemic biomarkers of retinopathy of prematurity in preterm babies. Int Ophthalmol. (2022) 43:1751–9. doi: 10.1007/s10792-022-02576-z
6. Süren E, Özkaya D, Çetinkaya E, Kalaycı M, Yiğit K, Kücük MF, et al. Comparison of bevacizumab, ranibizumab and aflibercept in retinopathy of prematurity treatment. Int Ophthalmol. (2022) 42:1905–13. doi: 10.1007/s10792-021-02188-z
7. Xia F, Lyu J, Peng J, Zhao P. Repeated intravitreal ranibizumab for reactivated retinopathy of prematurity after intravitreal ranibizumab monotherapy: vascular development analysis. Graefes Arch Clin Exp Ophthalmol. (2022) 260:2837–46. doi: 10.1007/s00417-022-05628-3
8. Roach L, Hartnett EM, Hutchinson AK, Kim SJ. Fighting ROP with anti-VEGF therapy. EyeNet Magazine (Am Acad Ophthalmol). (2019). Available at: https://www.aao.org/eyenet/article/fighting-rop-with-anti-vegf-therapy (Accessed June 17, 2023).
9. Chiang MF. How does the standard of care evolve? Anti–vascular endothelial growth factor agents in retinopathy of prematurity treatment as an example. Ophthalmology. (2018) 125:1485–7. doi: 10.1016/j.ophtha.2018.04.018
10. Fierson WM, American Academy of Pediatrics Section on Ophthalmology, American Academy of Ophthalmology, American Association for Pediatric Ophthalmology and Strabismus, American Association of Certified Orthoptists. Screening examination of premature infants for retinopathy of prematurity. Pediatrics. (2018) 142:e20183061. doi: 10.1542/peds.2018-3061
11. Langan D, Higgins JPT, Jackson D, Bowden J, Veroniki AA, Kontopantelis E, et al. A comparison of heterogeneity variance estimators in simulated random-effects meta-analyses. Res Syn Meth. (2019) 10:83–98. doi: 10.1002/jrsm.1316
12. Toro-Huamanchumo CJ, Benites-Meza JK, Mamani-García CS, Bustamante-Paytan D, Gracia-Ramos AE, Diaz-Vélez C, et al. Efficacy of colchicine in the treatment of COVID-19 patients: a systematic review and meta-analysis. J Clin Med. (2022) 11:2615. doi: 10.3390/jcm11092615
13. Van Aert RCM, Jackson D. Multistep estimators of the between-study variance: the relationship with the paule-mandel estimator: multi-step estimators of the between-study variance. Stat Med. (2018) 37:2616–29. doi: 10.1002/sim.7665
14. Toro-Huamanchumo CJ, Hilario-Gomez MM, Diaz-Reyes N, Caballero-Alvarado JA, Barboza JJ. The efficacy of CPAP in neonates with meconium aspiration syndrome: a systematic review and meta-analysis. Children. (2022) 9:589. doi: 10.3390/children9050589
15. Barboza JJ, Albitres-Flores L, Rivera-Meza M, Rodriguez-Huapaya J, Caballero-Alvarado J, Pasupuleti V, et al. Short-term efficacy of umbilical cord milking in preterm infants: systematic review and meta-analysis. Pediatr Res. (2021) 89:22–30. doi: 10.1038/s41390-020-0902-x
16. Barboza JJ, Huamán MR, Melgar B, Diaz-Arocutipa C, Valenzuela-Rodriguez G, Hernandez AV. Efficacy of liraglutide in non-diabetic obese adults: a systematic review and meta-analysis of randomized controlled trials. JClin Med. (2022) 11:2998. doi: 10.3390/jcm11112998
17. Cairns M, Prendergast LA. On ratio measures of heterogeneity for meta-analyses. Res Synth Methods. (2022) 13:28–47. doi: 10.1002/jrsm.1517
18. Akl E, Mustafa R, Wiercioch Wojtek NS. GRADE Handbook. GRADEpro.org (2013). Available at: https://gdt.gradepro.org/app/handbook/handbook.html (Accessed June 18, 2023).
19. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
20. Kabataş EU, Kurtul BE, Altıaylık Özer P, Kabataş N. Comparison of intravitreal bevacizumab, intravitreal ranibizumab and laser photocoagulation for treatment of type 1 retinopathy of prematurity in turkish preterm children. Curr Eye Res. (2017) 42:1054–8. doi: 10.1080/02713683.2016.1264607
21. Zhang G, Yang M, Zeng J, Vakros G, Su K, Chen M, et al. Comparison of intravitreal injection of ranibizumab versus laser therapy for zone II treatment-requiring retinopathy of prematurity. Retina. (2017) 37:710–7. doi: 10.1097/IAE.0000000000001241
22. Stahl A, Lepore D, Fielder A, Fleck B, Reynolds JD, Chiang MF, et al. Ranibizumab versus laser therapy for the treatment of very low birthweight infants with retinopathy of prematurity (RAINBOW): an open-label randomised controlled trial. Lancet. (2019) 394:1551–9. doi: 10.1016/S0140-6736(19)31344-3
23. Fleck BW, Reynolds JD, Zhu Q, Lepore D, Marlow N, Stahl A, et al. Time course of retinopathy of prematurity regression and reactivation after treatment with ranibizumab or Laser in the RAINBOW trial. Ophthalmol Retina. (2022) 6:628–37. doi: 10.1016/j.oret.2022.02.006
24. Marlow N, Stahl A, Lepore D, Fielder A, Reynolds JD, Zhu Q, et al. 2-year Outcomes of ranibizumab versus laser therapy for the treatment of very low birthweight infants with retinopathy of prematurity (RAINBOW extension study): prospective follow-up of an open label, randomised controlled trial. Lancet Child Adolesc Health. (2021) 5:698–707. doi: 10.1016/S2352-4642(21)00195-4
25. Fidler M, Fleck BW, Stahl A, Marlow N, Chastain JE, Li J, et al. Ranibizumab population pharmacokinetics and free VEGF pharmacodynamics in preterm infants with retinopathy of prematurity in the RAINBOW trial. Trans Vis Sci Tech. (2020) 9:43. doi: 10.1167/tvst.9.8.43
26. Boskabadi H, Saravi A, Zakerihamidi M. Comparison of retinopathy of prematurity incidence in preterm infants of mothers with preeclampsia and infants of healthy mothers. J Obstet Gynecol India. (2022) 72:409–13. doi: 10.1007/s13224-022-01660-9
27. Xie T, Zhang Z, Cui Y, Shu Y, Liu Y, Zou J, et al. Prostaglandin E2 promotes pathological retinal neovascularisation via EP4R-EGFR-Gab1-AKT signaling pathway. Exp Eye Res. (2021) 205:108507. doi: 10.1016/j.exer.2021.108507
28. Wang S-D. Laser therapy versus intravitreal injection of anti-VEGF agents in monotherapy of ROP: a meta-analysis. Int J Ophthalmol. (2020) 13:806–15. doi: 10.18240/ijo.2020.05.17
29. Geloneck MM, Chuang AZ, Clark WL, Hunt MG, Norman AA, Packwood EA, et al. Refractive outcomes following bevacizumab monotherapy compared with conventional Laser treatment: a randomized clinical trial. JAMA Ophthalmol. (2014) 132:1327. doi: 10.1001/jamaophthalmol.2014.2772
30. Bachu S, Narendran V, Kalpana N, Shah P, Ramakrishnan M, Sadat B. Long term refractive and structural outcome following laser treatment for zone 1 aggressive posterior retinopathy of prematurity. Oman J Ophthalmol. (2014) 7:116. doi: 10.4103/0974-620X.142592
31. Mintz-Hittner HA, Kennedy KA, Chuang AZ. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med. (2011) 364:603–15. doi: 10.1056/NEJMoa1007374
32. Solans Pérez De Larraya AM, Ortega Molina JM, Uberos Fernández J, González Ramírez AR, García Serrano JL. Speed of retinal vascularization in retinopathy of prematurity: risk and protective factors. Biomed Res Int. (2019) 2019:1–5. doi: 10.1155/2019/2721578
33. Sen P, Bhende P, Rishi E, Gopal L, Jain S. Anatomical and visual outcomes in stage 5 retinopathy of prematurity with microincision vitrectomy surgery. Retina. (2021) 41:331–7. doi: 10.1097/IAE.0000000000002837
34. Nguyen V, Vaze A, Fraser-Bell S, Arnold J, Essex RW, Barthelmes D, et al. Outcomes of suspending VEGF inhibitors for neovascular age-related macular degeneration when lesions have been inactive for 3 months. Ophthalmol Retina. (2019) 3:623–8. doi: 10.1016/j.oret.2019.05.013
35. Chen W, He S, Xiang D. Hypoxia-induced retinal pigment epithelium cell-derived bFGF promotes the migration and angiogenesis of HUVECs through regulating TGF-β1/smad2/3 pathway. Gene. (2021) 790:145695. doi: 10.1016/j.gene.2021.145695
36. Sun M, Wadehra M, Casero D, Lin M-C, Aguirre B, Parikh S, et al. Epithelial membrane protein 2 (EMP2) promotes VEGF-induced pathological neovascularization in murine oxygen-induced retinopathy. Invest Ophthalmol Vis Sci. (2020) 61:3. doi: 10.1167/iovs.61.2.3
37. Bertelli PM, Pedrini E, Guduric-Fuchs J, Peixoto E, Pathak V, Stitt AW, et al. Vascular regeneration for ischemic retinopathies: hope from cell therapies. Curr Eye Res. (2020) 45:372–84. doi: 10.1080/02713683.2019.1681004
38. Beharry KD, Valencia GB, Lazzaro DR, Aranda JV. Pharmacologic interventions for the prevention and treatment of retinopathy of prematurity. Semin Perinatol. (2016) 40:189–202. doi: 10.1053/j.semperi.2015.12.006
39. Zou Q, Zhang F-J, Liu Q-P. Efficacy evaluation of intravitreal ranibizumab therapy for three types of retinopathy of prematurity. Int J Ophthalmol. (2022) 15:753–9. doi: 10.18240/ijo.2022.05.10
Keywords: retinopathy of prematurity, systematic review, ranibizumab, meta-analysis, laser therapy
Citation: Alva N, Martínez AR, Ortiz-Saavedra B, Montes-Madariaga ES, Cotrina A, Caballero-Alvarado JA, Sah R and Barboza JJ (2023) Ranibizumab for the treatment of retinopathy of prematurity: systematic review and meta-analysis. Front. Pediatr. 11:1202927. doi: 10.3389/fped.2023.1202927
Received: 9 April 2023; Accepted: 24 July 2023;
Published: 4 August 2023.
Edited by:
MaryAnn Volpe, Tufts University, United StatesReviewed by:
Yao Mun Choo, University of Malaya, MalaysiaC. A. Harper, Austin Retina Associates, United States
© 2023 Alva, Martínez, Ortiz-Saavedra, Montes-Madariaga, Cotrina, Caballero-Alvarado, Sah and Barboza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joshuan J. Barboza jbarbozame@ucvvirtual.edu.pe