Caudal block vs. transversus abdominis plane block for pediatric surgery: a systematic review and meta-analysis
 Michael Hafeman1*
Michael Hafeman1*  Seth Greenspan2 Emiliya Rakhamimova2
Seth Greenspan2 Emiliya Rakhamimova2  Zhaosheng Jin1
Zhaosheng Jin1  Robert P. Moore3
Robert P. Moore3  Ehab Al Bizri3
Ehab Al Bizri3
- 1Department of Anesthesiology, Stony Brook University Renaissance School of Medicine, Stony Brook, NY, United States
- 2Stony Brook University Renaissance School of Medicine, Stony Brook, NY, United States
- 3Division of Pediatric Anesthesiology, Department of Anesthesiology, Stony Brook University Renaissance School of Medicine, Stony Brook, NY, United States
Background: The caudal block and transversus abdominis plane block (TAP) are commonly used in combination with general anesthesia for pediatric lower abdominal, inguinal, and genitourinary surgeries. There is limited data directly comparing the impact of these techniques on recovery. In this meta-analysis, we compare the duration of postoperative analgesia between these two techniques.
Objective: This review examined the duration of analgesia in pediatric patients (age 0–18 years) undergoing surgery who received caudal or TAP block after induction of general anesthesia. The primary outcome was duration of analgesia, defined as the time to first rescue analgesic dose. Secondary outcomes included number of rescue analgesic doses, acetaminophen usage within 24 h postoperatively, 24 h pain score area under the curve, and postoperative nausea and vomiting.
Evidence review: We systematically searched Pubmed, Central, EMBASE, CINAHL, Google Scholar, Web of Science citation index, the US clinical trials register, and abstracts from prominent 2020–2022 anesthesia conferences for randomized controlled trials that compared these blocks and reported analgesia duration.
Findings: Twelve RCTs inclusive of 825 patients were identified. TAP block was associated with longer analgesia duration (Mean difference = 1.76 h, 95% CI: 0.70–2.81, p = 0.001) and reduced doses of rescue analgesic within 24 h (Mean difference = 0.50 doses, 95% CI: 0.02–0.98, p = 0.04). No statistically significant differences were detected in other outcomes.
Conclusion: This meta-analysis suggests that TAP block provides greater duration of analgesia than caudal block after pediatric surgeries. TAP block was also associated with fewer rescue analgesic doses in the first 24 h without increased pain scores.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=380876, identifier: CRD42022380876.
Introduction
Lower abdominal, inguinal, and genitourinary surgeries are common in children and analgesia is a key aspect of perioperative care. Improvements in technology have led to the adoption of several regional anesthesia techniques in diverse clinical settings (1). There is limited comparative efficacy data about the impact of different regional techniques on recovery. This systematic review and meta-analysis sought to compare the caudal block (CB) to the transversus abdominis plane block (TAP) for these pediatric surgeries.
The caudal block is a widely used technique in which a needle traverses the sacral hiatus to deposit local anesthetic into the epidural space. It has traditionally been performed with a landmark-based technique, but ultrasound guidance is occasionally used (2, 3). While studies have shown it to be an effective technique for intraoperative analgesia in surgeries below the umbilicus, its utility may be limited by a short duration of analgesia (4). Additionally, although complications are rare and usually minor, they may be seven times more common in central vs. peripheral regional anesthesia in children and the potential for greater harm exists (5, 6). Caudal blocks may also result in motor blockade or urinary retention (7), which can potentially lengthen recovery. Additionally, caudal blocks can be difficult to place with an approximate 1% failure rate in data reported from a high-volume academic cohort (6).
The transversus abdominis plane block is an interfascial plane block technique in which local anesthetic is deposited between the internal oblique and transversus abdominis muscles, typically under ultrasound guidance (8). Several approaches have been described for this block, but they all involve deposition of anesthetic in this interfascial layer and may provide analgesia from the T10 to the L1 dermatomes (8, 9). The technique and related fascial plane blocks have become increasingly popular with widespread adoption of ultrasound technology for pediatric practice (1). Complications of the TAP block are rare but there is the potential for local anesthetic systemic toxicity and there are case reports of liver trauma and bowel hematoma when performed without ultrasound guidance (10, 11). Analgesia from the TAP block may last up to 48 h (12). This supposed long duration may be due to a longer lasting depot of local anesthetic at the injection site (13), compared to the great vascularity surrounding the epidural space which has been shown to decrease the duration of epidural analgesia (14).
While both techniques can be safely and successfully applied, there is limited data specifically related to the impact on the quality of postoperative analgesia, recovery, and efficiency of care when TAP block or caudal block are part of multimodal analgesia for lower abdominal surgeries in children. Such information is vitally important in an era increasingly focused on cost-effective patient-centered care that can resonate beyond the operating suite, such as enhanced recovery efforts (15, 16). This meta-analysis can help address this gap in the literature.
Materials and methods
Study objectives
The overall objective of this study was to compare analgesic efficacy of TAP block to caudal block in children undergoing lower abdominal, inguinal, or genitourinary surgery. The primary outcome was postoperative duration of analgesia achieved with either block, defined as the time from block or arrival in the recovery room until patients required a rescue analgesic dose. Secondary outcomes are the number of rescue doses, mean 24 h acetaminophen usage, 24 h area under the curve (AUC) pain score, and postoperative nausea and vomiting (PONV). This systematic review was registered under PROSPERO, ID CRD42022380876.
Search strategy
This study was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement (17). Two authors independently searched for references, and any discrepancies were reconciled by the authors. We searched the terms “(Anesthesia, Caudal OR Caudal Anesthesia OR Sacral Epidural Anesthesia OR Caudal Block)” AND “(TAP Block OR Transversus Abdominis)” AND (“Pediatrics” OR Pediatrics OR Children) AND “(Surgery)” in PubMed, Central, EMBASE, CINAHL, Google Scholar, Web of Science citation index, and the US clinical trials register. Additionally, we manually searched the abstracts from prominent anesthesia conferences from the past three years. The search was completed on December 13, 2022.
Study selection criteria
Two authors independently reviewed the title and abstract of the references compiled from the above search criteria and filtered through them based on the following criteria:
Patient population: The population consists of all pediatric patients (age ≤18) undergoing surgery who received either a caudal or TAP block immediately after induction of general anesthesia.
Study design: This meta-analysis compiled data exclusively from randomized controlled trials (RCTs).
Intervention: Pediatric patients who received a TAP block for postoperative analgesia. This meta-analysis excluded studies where patients received multiple blocks or studies that compared different medications administered for the blocks.
Control: Pediatric patients who received a caudal epidural block for postoperative analgesia. This meta-analysis excluded studies where patients received multiple blocks or studies that compared different medications administered for the blocks.
Outcomes: For inclusion in our study, an RCT must include the primary outcome of duration of analgesia.
Data extraction
Data was extracted from each study onto a standardized form and was independently verified by a second author. The data extracted from each study included study title and author, number of participants in each experimental group, primary outcome (duration of analgesia), pain score at which rescue analgesia was administered, secondary outcomes (number of rescue doses, mean 24 h acetaminophen usage, 24 h area AUC pain score, and PONV), rescue analgesia medication and dosage, parent satisfaction, and other adverse events if reported, including urinary retention, hypotension, bradycardia, and block failure. We contacted the RCT authors when data was incomplete or reported with median and interquartile range. If the study authors did not reply, we derived the mean and standard deviation by assuming the normal distribution in accordance with Cochrane methods (18).
Risk of bias assessment was also performed and independently verified by two study authors in accordance with the RoB 2, a Cochrane risk-of-bias tool designed for randomized controlled trials (19). We examined the risk of bias in the RCTs in five domains: randomization and concealment of allocation, deviations form allocated interventions, completeness of outcome data, measurement bias, and the selection of reported results. Based on the summation of the study's risk of bias from these five domains, each study was assessed to be either “low risk,” “some concerns,” or “high risk” [of bias].
Statistical analyses
We conducted meta-analysis for all outcomes. The data was analyzed using Review Manager V5.3. (Cochrane Collaboration, Copenhagen). For continuous variables, we used inverse-variance method to calculate the mean difference (MD) for outcomes that have clinically relevant effect sizes such as length of analgesia. For dichotomous variables, we calculated the risk ratios (RRs) by the Mantel-Haenszel method. Due to the inherent heterogeneous nature of block performance by different practitioners, random effect model was used in the analysis. We also conducted sensitivity analyses on the primary outcome (duration of analgesia) by excluding high-risk-of-bias studies. Small study effect was assessed using Egger's regression, and publication bias was assessed using Duval and Tweedie's trim and fill; both were done using the statistical package provided by Suurmond et al. (20). For all outcomes, the statistical significance was set to p < 0.05 and with 95% confidence intervals. We used GRADEpro Guideline Development Tool (GRADEpro GDT, McMaster University, 2015) to assess the quality of the meta-analysis findings, presented in Supplementary Table S1.
Results
Description of included studies
The literature search identified a total of 69 unique studies. In the screening process, 57 of these studies were excluded and 12 were included in the meta-analysis (Figure 1) (21–32). Justification for exclusion of studies is provided in Supplementary Table S2. Characteristics of the included studies are listed in Table 1. A summary of findings is reported in Table 2. The risk of bias (RoB) assessment is reported in Figure 2, with the randomization process and selection of reported results being the most common sources of potential bias. Justification for RoB assessment is provided in Supplementary Table S3.

Figure 1. Search flow chart.
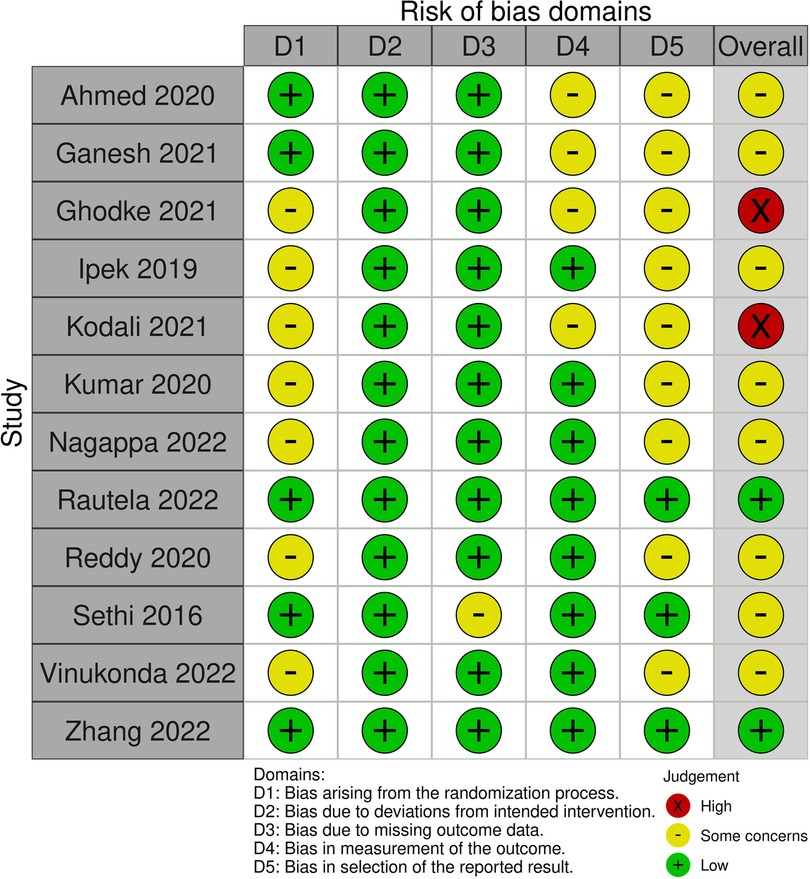
Figure 2. Risk of bias assessment for included randomized controlled trials.
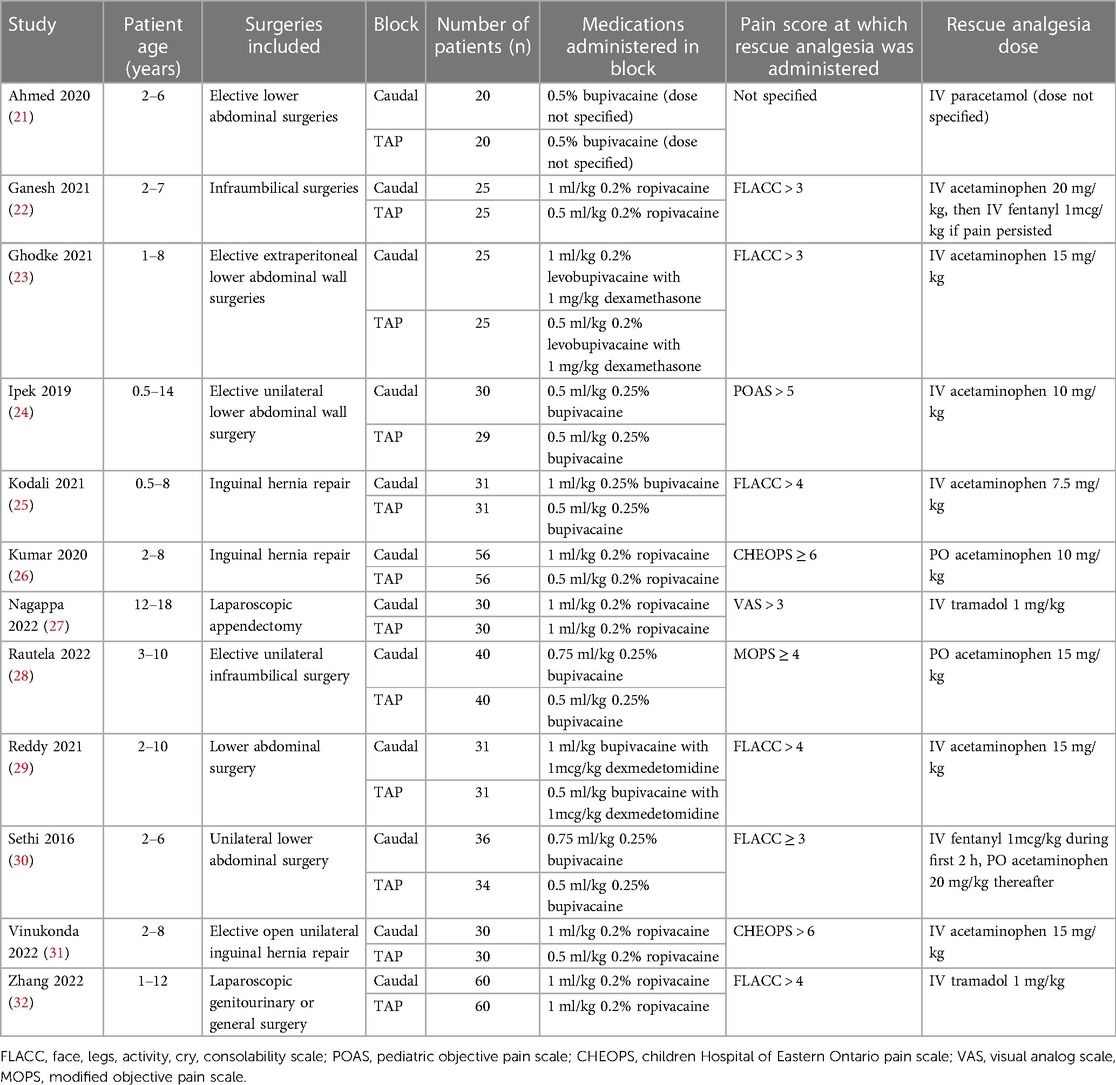
Table 1. Characteristics of included studies.
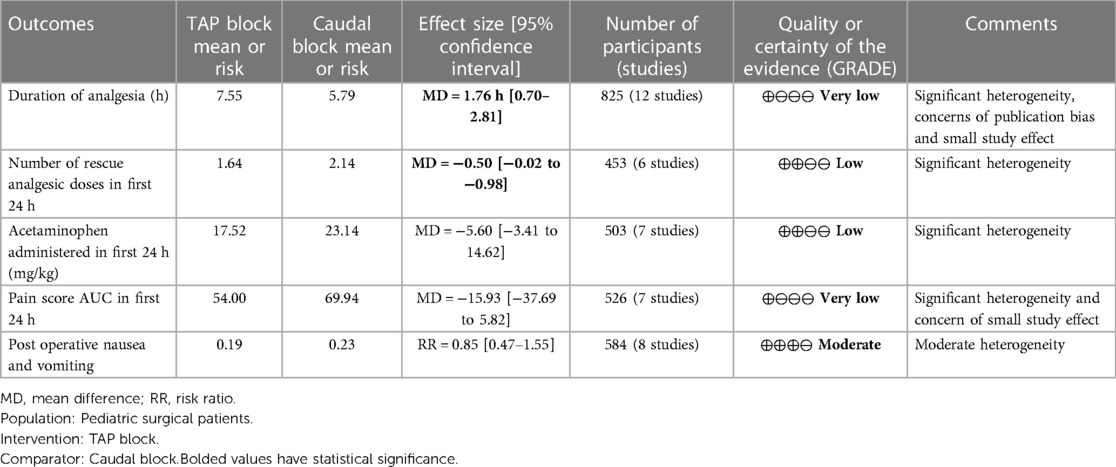
Table 2. Summary of findings.
Duration of analgesia
Duration of analgesia was the primary outcome in this study and was reported in 12 trials. It was defined as the duration (from time of block or from time of arrival in recovery unit) before a dose of rescue analgesia was given; however, individual studies used different pain scores and scales to determine when this rescue should be administered (Table 1). Pooled results inclusive of 825 patients showed that the TAP block was favored [Mean difference (MD) = 1.76 h, 95% CI: 0.70–2.81, I2 = 97%, p = 0.001, Figure 3]. Excluding the high risk studies (per the RoB assessment) did not significantly alter the conclusion (MD = 1.32, 95% CI: 0.24–2.4, Figure 4). Egger's regression suggested significant risk of small study effect (p < 0.01); while the trim and fill predicted three missing studies. Quality of evidence is very low on account of the high heterogeneity and significant risk of publication bias.

Figure 3. Forest plots of primary outcome of duration of analgesia (hours).
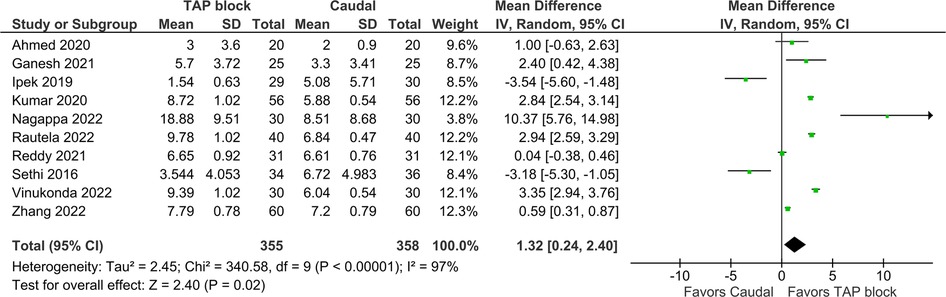
Figure 4. Forest plot of duration of analgesia, high risk of bias studies excluded.
Number of rescue doses and 24 h acetaminophen usage
Number of rescue doses was reported in six studies inclusive of 453 patients, with pooled results showing TAP block favored (MD = −0.50 doses, 95% CI: −0.02 to −0.98, I2 = 96%, p = 0.04, Figure 5). Egger's regression p = 0.42, trim and fill predicted no missing studies. The quality of evidence is low due to significant heterogeneity.

Figure 5. Forest plot of number of rescue analgesic doses in first 24 h.
Mean total acetaminophen in the first 24 h postoperatively was reported in seven studies inclusive of 503 patients, with pooled results showing no statistically significant difference [MD = −5.60 mg/kg (TAP block favored), 95% CI: −14.62−3.41, I2 = 99%, p = 0.22, Figure 6]. Egger's regression p = 0.41, trim and fill predicted no missing studies. The quality of evidence is low due to significant heterogeneity.
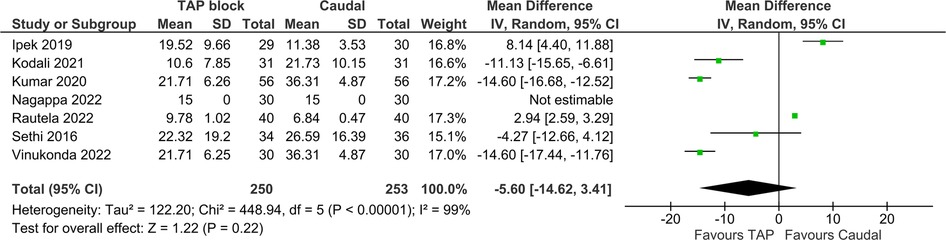
Figure 6. Forest plot of Acetaminophen usage in first 24 h (mg/kg).
Pain scores in first 24 h
Of the 12 studies included in the primary analysis, seven studies inclusive of 526 patients reported pain scores up to 24 h postoperatively. Pooled results did not show a statistically significant difference between the pain score AUC of two blocks [MD = −15.93 (TAP block favored), 95% CI: −37.69–5.82, I2 = 100%, p = 0.15, Figure 7]. However, the study by Vinukonda et al. was an outlier and was the only study favoring CB in this metric. Egger's regression p = 0.01, trim and fill predicted no missing studies. The quality of evidence is very low due to significant heterogeneity and concern of small study effect.
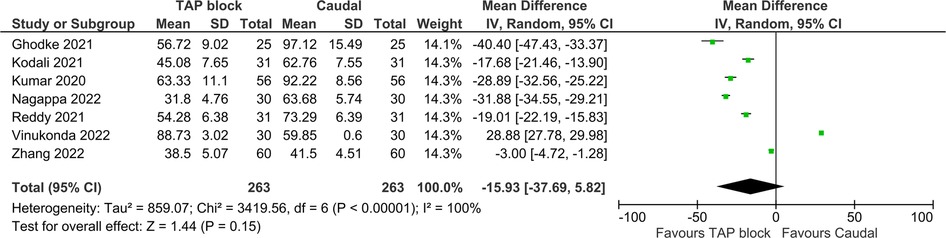
Figure 7. Forest plot of 24 h pain score AUC.
Post-operative nausea and vomiting
Post-operative nausea and vomiting (PONV) was the only adverse outcome that was consistently reported, in a total of eight studies inclusive of 584 patients. Pooled analysis showed no statistically significant difference between the blocks [RR = 0.85 (TAP block favored), 95% CI: 0.47–1.55, I2 = 42%, p = 0.61, Figure 8]. Egger's regression p = 0.99, trim and fill predicted no missing studies. The quality of evidence moderate due to moderate heterogeneity. Of note, among the studies which reported PONV, Ganesh 2021 and Sethi 2016 were the only studies with a risk ratio favoring CB, and they were also the only studies to include IV fentanyl in the rescue analgesia regimen.
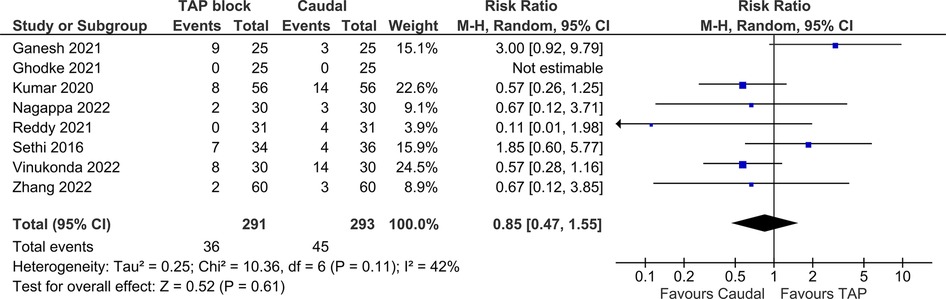
Figure 8. Forest plot of post operative nausea and vomiting.
Discussion
Pooled results demonstrated a significantly increased duration of analgesia of 1.76 h with techniques incorporating TAP block as compared to caudal blockade. This trend was associated with a statistically significant reduction in number of rescue analgesic doses in the first 24 h postoperatively (MD = −0.50 doses) with TAP block but no difference in the total weight-based acetaminophen in the first 24 h. This increased duration of analgesia was associated with a non-significant trend toward overall reduction in pain scores for the first 24 h (seen in six of seven analyzed studies). Additionally, there was a non-significant trend toward reduction in PONV amongst TAP block recipients. Parent/patient satisfaction was only reported in three of 12 studies and was not formally analyzed in this meta-analysis, however this metric also favored TAP block in all three studies. These results are thought-provoking and could have an immediate clinical impact while serving as a springboard for further research.
Analgesia is a key aspect of recovery from pediatric surgery and the addition of regional anesthesia has been particularly impactful. Regional techniques have been associated with reduced general anesthetic requirements with subsequent reduction in associated side effects and the potential for faster and smoother emergence, reduced opioid use, faster return of gut function, and reduced hormonal stress response (33). These benefits may be especially impactful for lower abdominal surgeries that are both commonly performed and associated with a non-trivial incidence of chronic pain after surgery (34). Both neuraxial and fascial plane blocks have been successfully applied in this context but there is limited data especially related to duration and quality of analgesia. This meta-analysis compares the impact of these techniques on the duration and impact of analgesia.
Clinical implications
The application of TAP blocks to provide prolonged analgesia in comparison to caudal blockade without leading to an increase in postoperative pain scores or the need for rescue medications could support the expansion of regional techniques in pediatric practice at a time of significant change within the subspecialty (35, 36). In addition to serving as a reliable option for analgesia, the TAP block may be a more accessible technique relying on the transfer of skills commonly employed in adult practice to produce a block that is reliable and has a broad margin of safety. While no specific studies address comparative ease of pediatric vs. adult TAP block placement, pediatric anatomy may result in a technically simpler intervention due to favorable conditions to visualize anatomic landmarks and local anesthetic spread.
TAP blocks may have a greater margin of safety compared to caudal blockade especially when performed by non-subspecialty trained generalists. The application of fascial plane blocks obviates the risk of dural puncture, urinary retention, and neuraxial hematoma that can be associated with a neuraxial technique. They may have a greater window of safety related to placement-associated hematoma risk (37). Large studies have shown that complications are more frequent with neuraxial anesthesia and peripheral regional techniques may be preferred when appropriate (5, 38).
Similarly, TAP blocks may be placed more reliably, with lower rate of block failure or abandoned block. A large study by Polaner et al. showed only one block that was failed or abandoned out of 140 (0.7%). Of these 140 blocks, 92% were performed under ultrasound guidance. The caudal block has been more extensively studied. The same study by Polaner et al. examined over 6,000 caudal blocks, 97% with the landmark technique and 3% ultrasound guided, and found a complication rate of 3%. The majority of these complications (2%) were failed or abandoned blocks, but also reported were positive test doses, dural punctures, and vascular punctures (2). Another study of 750 caudal blocks in children without ultrasound guidance reported an overall success rate of 96%, with 70% successful on first attempt and 26% requiring multiple attempts (39). While the speed of placing a caudal block without ultrasound guidance may potentially be greater, this advantage would be negated by the significantly higher rate of failure, abandonment, and other complications.
This pooled analysis suggests a number of possible benefits of the significantly prolonged duration of analgesia associated with TAP block. Patients receiving TAP block received fewer rescue analgesia doses, and while not statistically significant, other possible benefits include a trend toward reduced pain scores and reduced PONV. Overall, this data combined with great ease of placement and a broad margin of safety support the application of TAP blocks for pediatric lower abdominal surgeries. It also suggests numerous areas for further research.
Implications for further research
The pooled data support a significant increase in duration of analgesia when TAP block is applied as opposed to caudal blockade. The clinical implications of this difference and their impact on the perioperative care and overall quality of recovery are key questions to be addressed. Trends toward improved pain scores, reduced number of rescue doses, and PONV are suggestive of key areas for study. This information could be impactful for the design, implementation, and success of enhanced recovery after surgery (ERAS) pathways (15, 16, 40). The impact of prolonged duration of anesthesia on the progression to persistent pain is another key question for exploration. Although this study examines a wide variety of surgeries, further studies could elucidate the optimal surgeries for the TAP block, which provides mainly somatic analgesia and may be a poor choice for surgeries which involve extensive intraabdominal manipulation (41). Other fascial plane blocks, such as the erector spinae plane (ESP) block, may be further investigated as well. It has been suggested that the ESP block provides visceral analgesia (42, 43), and it has been successfully employed for a number of painful abdominal interventions (44, 45). Translational research could attempt to explain the mechanism for the different recovery profile between peripheral and neuraxial blocks. Specifically, are the observed benefits simply the product of different distribution and absorption of local anesthetic, or are they related to impact on the neurohormonal and inflammatory response to surgery?
Strengths and limitations
Our pooled analysis is rooted in a thoughtful and systematic search process that included independent verification and extraction of data by two authors. This allowed for the analysis of 12 studies that enrolled a total of 825 patients. Results generated by this large cohort are important as it is difficult to complete large pediatric trials that are required to address questions related to recovery profiles. It can be challenging to enroll pediatric patients in clinical trials (46). Our process also allowed for the collection of data from several studies related to secondary outcomes including AUC for pain scores, rescue analgesia use, and incidence of PONV. This could provide insight into the differential impact of these techniques in the overall recovery profile. Pooling of data allowed for examination of these data points and is suggestive of the need for further research.
The primary limitation of this study is the heterogeneity of studies included. A number of different surgery types were included and performed on children of a variety of ages. Due to this heterogeneity, certainty of evidence ranged from low to very low. A more focused study on a particular age group or surgical population may reveal different results. There was also significant variability in the dosing of local anesthetic, adjuvants, and intraoperative opioid regimens (which were rarely reported). Additionally, included studies used different pain scales and thresholds for pain scores when defining their duration of analgesia and administering rescue medication. While this heterogeneity is a concern related to the quality of included studies, it is a clear reflection of the diversity of pediatric anesthesia practice and suggests that our primary outcome is the product of daily real-world conditions allowing for ease of clinical application. Similarly, there may be concern toward publication bias in the included studies. However, the large pooled number of included patients and overall support for the use of regional analgesia techniques in the context of lower abdominal surgeries (33) could blunt these concerns.
Conclusion
Our large pooled analysis supports increased duration of analgesia with the application of TAP blocks as compared to caudal blockade for pediatric lower abdominal, inguinal, and genitourinary surgeries. Increased duration of analgesia was associated with fewer rescue analgesic doses and was not associated with increased pain scores. In fact, there were trends suggestive of reduced pain scores and reduced PONV when TAP was employed. Although this data has limitations and may not be applied universally, it generally supports usage of the TAP block, a technique with a wide margin of safety and ease of application.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
MH, ZJ, RM, and EA were responsible for the conception and design of the study. MH, SG, ER, and ZJ and were responsible for study selection. MH, SG, and ER performed the data extraction. ZJ performed the statistical analysis. MH, SG, ZJ, RM, and EA drafted sections of the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2023.1173700/full#supplementary-material
References
1. Walker BJ, Long JB, De Oliveira GS, Szmuk P, Setiawan C, Polaner DM, et al. Peripheral nerve catheters in children: an analysis of safety and practice patterns from the pediatric regional anesthesia network (Pran). Br J Anaesth. (2015) 115(3):457–62. doi: 10.1093/bja/aev220
2. Polaner DM, Taenzer AH, Walker BJ, Bosenberg A, Krane EJ, Suresh S, et al. Pediatric regional anesthesia network (Pran): a multi-institutional study of the use and incidence of complications of pediatric regional anesthesia. Anesth Analg. (2012) 115(6):1353–64. doi: 10.1213/ANE.0b013e31825d9f4b
3. Menzies R, Congreve K, Herodes V, Berg S, Mason DG. A survey of pediatric caudal extradural anesthesia practice. Paediatr Anaesth. (2009) 19(9):829–36. doi: 10.1111/j.1460-9592.2009.03116.x
4. de Beer DA, Thomas ML. Caudal additives in children–solutions or problems? Br J Anaesth. (2003) 90(4):487–98. doi: 10.1093/bja/aeg064
5. Ecoffey C, Lacroix F, Giaufre E, Orliaguet G, Courreges P, Association des anesthésistes réanimateurs pédiatriques d'expression française. Epidemiology and morbidity of regional anesthesia in children: a follow-up one-year prospective survey of the French-language society of paediatric anaesthesiologists (Adarpef). Paediatr Anaesth. (2010) 20(12):1061–9. doi: 10.1111/j.1460-9592.2010.03448.x
6. Suresh S, Long J, Birmingham PK, De Oliveira GS Jr. Are caudal blocks for pain control safe in children? An analysis of 18,650 caudal blocks from the pediatric regional anesthesia network (Pran) database. Anesth Analg. (2015) 120(1):151–6. doi: 10.1213/ANE.0000000000000446
7. Shanthanna H, Singh B, Guyatt G. A systematic review and meta-analysis of caudal block as compared to noncaudal regional techniques for inguinal surgeries in children. Biomed Res Int. (2014) 2014:890626. doi: 10.1155/2014/890626
8. Dontukurthy S, Mofidi R. The role of interfascial plane blocks in paediatric regional anaesthesia: a narrative review of current perspectives and updates. Anesthesiol Res Pract. (2020) 2020:8892537. doi: 10.1155/2020/8892537
9. Willschke H, Marhofer P, Machata AM, Lonnqvist PA. Current trends in paediatric regional anaesthesia. Anaesthesia. (2010) 65(Suppl 1):97–104. doi: 10.1111/j.1365-2044.2010.06242.x
10. Taylor R Jr, Pergolizzi JV, Sinclair A, Raffa RB, Aldington D, Plavin S, et al. Transversus abdominis block: clinical uses, side effects, and future perspectives. Pain Pract. (2013) 13(4):332–44. doi: 10.1111/j.1533-2500.2012.00595.x
11. Frigon C, Mai R, Valois-Gomez T, Desparmet J. Bowel hematoma following an iliohypogastric-ilioinguinal nerve block. Paediatr Anaesth. (2006) 16(9):993–6. doi: 10.1111/j.1460-9592.2006.01909.x
12. Carney J, Finnerty O, Rauf J, Curley G, McDonnell JG, Laffey JG. Ipsilateral transversus abdominis plane block provides effective analgesia after appendectomy in children: a randomized controlled trial. Anesth Analg. (2010) 111(4):998–1003. doi: 10.1213/ANE.0b013e3181ee7bba
13. Latzke D, Marhofer P, Kettner SC, Koppatz K, Turnheim K, Lackner E, et al. Pharmacokinetics of the local anesthetic ropivacaine after transversus abdominis plane block in healthy volunteers. Eur J Clin Pharmacol. (2012) 68(4):419–25. doi: 10.1007/s00228-011-1139-8
14. Higuchi H, Adachi Y, Kazama T. Factors affecting the spread and duration of epidural anesthesia with ropivacaine. Anesthesiology. (2004) 101(2):451–60. doi: 10.1097/00000542-200408000-00027
15. Rove KO, Strine AC, Wilcox DT, Vricella GJ, Welch TP, VanderBrink B, et al. Design and development of the pediatric urology recovery after surgery endeavor (Pursue) multicentre pilot and exploratory study. BMJ Open. (2020) 10(11):e039035. doi: 10.1136/bmjopen-2020-039035
16. Roberts K, Brindle M, McLuckie D. Enhanced recovery after surgery in paediatrics: a review of the literature. BJA Educ. (2020) 20(7):235–41. doi: 10.1016/j.bjae.2020.03.004
17. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The prisma statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. (2009) 6(7):e1000100. doi: 10.1371/journal.pmed.1000100
18. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. 2nd ed. Hoboken, NJ: The Cochrane Collaboration (2019).
19. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. Rob 2: a revised tool for assessing risk of bias in randomised trials. Br Med J. (2019) 366:l4898. doi: 10.1136/bmj.l4898
20. Suurmond R, van Rhee H, Hak T. Introduction, comparison, and validation of meta-essentials: a free and simple tool for meta-analysis. Res Synth Methods. (2017) 8(4):537–53. doi: 10.1002/jrsm.1260
21. Ahmed OH, Ali WM, Hassan IE. Ultrasound-guided transversus abdominis plane block versus ultrasound-guided caudal block for pain relief in children undergoing lower abdominal surgeries. Egypt J Hosp Med. (2020) 78(2):227–33. doi: 10.21608/ejhm.2020.69683
22. Ganesh B, Swain S, Banerjee S. Comparison of ultrasound-guided transversus abdominis plane block and caudal epidural block for pain relief in children undergoing infraumbilical surgeries. Anesth Essays Res. (2021) 15(2):161–6. doi: 10.4103/aer.aer_37_21
23. Ghodke S, Madhavi N, Hiremath RN. A comparative study of caudal block and ultrasound-guided transversus abdominis plane block with levobupivacaine and dexamethasone as additive in extraperitoneal lower abdominal surgeries in pediatrics. Asian J Pharm Clin Res. (2021) 14(6):173–6. doi: 10.22159/ajpcr.2021.v14i6.41386
24. Ipek CB, Kara D, Yilmaz S, Yesiltas S, Esen A, Dooply S, et al. Comparison of ultrasound-guided transversus abdominis plane block, quadratus lumborum block, and caudal epidural block for perioperative analgesia in pediatric lower abdominal surgery. Turk J Med Sci. (2019) 49(5):1395–402. doi: 10.3906/sag-1812-59
25. Kodali VRK, Kandimalla A, Vakamudi M. Comparison of analgesic efficacy of ultrasound-guided transversus abdominus plane block and caudal block for inguinal hernia repair in pediatric population: a single-blinded, randomized controlled study. Anesth Essays Res. (2020) 14(3):478–84. doi: 10.4103/aer.AER_77_20
26. Kumar A, Dogra N, Gupta A, Aggarwal S. Ultrasound-guided transversus abdominis plane block versus caudal block for postoperative analgesia in children undergoing inguinal hernia surgery: a comparative study. J Anaesthesiol Clin Pharmacol. (2020) 36(2):172–6. doi: 10.4103/joacp.JOACP_100_19
27. Nagappa S, Nanjundaswamy N, Maralusiddappa V, Nayak V. Comparing the intraoperative and postoperative analgesic effect of transabdominal block versus caudal block in children undergoing laparoscopic appendectomy. Indian Anaesth Forum. (2022) 23(1):19–24. doi: 10.4103/TheIAForum.TheIAForum_6_21
28. Rautela M, Sahni A, Dalal N. Is ultrasound-guided transversus abdominis plane block superior to a caudal epidural or wound infiltration for intraoperative and postoperative analgesia in children undergoing unilateral infraumbilical surgery? A double-blind randomized trial. J Indian Assoc Pediatr Surg. (2022) 27(3):323–8. doi: 10.4103/jiaps.JIAPS_54_21
29. Reddy A, Bhandary A, Shetty SR, Harish BG. Comparative study between an ultrasound-guided transversus abdominis plane block and an ultrasound-guided caudal block for postoperative analgesia in children undergoing lower abdominal surgeries—a prospective randomised study. South African J Anaesth Analg. (2021) 27(5):223–7. doi: 10.36303/SAJAA.2021.27.5.2489
30. Sethi N, Pant D, Dutta A, Koul A, Sood J, Chugh PT. Comparison of caudal epidural block and ultrasonography-guided transversus abdominis plane block for pain relief in children undergoing lower abdominal surgery. J Clin Anesth. (2016) 33:322–9. doi: 10.1016/j.jclinane.2016.03.067
31. Vinukonda M, Kumar KS, Suggala KK. A comparative randomized study of usg guided transversus abdominis plane block versus usg guided caudal block for post-operative analgesia in paediatric unilateral open inguinal hernia repair. Eur J Mol Clin Med. (2022) 9(4):3909–18.
32. Zhang Y, Wang YP, Wang HT, Xu YC, Lv HM, Yu Y, et al. Ultrasound-guided quadratus lumborum block provided more effective analgesia for children undergoing lower abdominal laparoscopic surgery: a randomized clinical trial. Surg Endosc Other Interv Tech. (2022) 36:9046–53. doi: 10.1007/s00464-022-09370-z
33. Bosenberg A. Benefits of regional anesthesia in children. Paediatr Anaesth. (2012) 22(1):10–8. doi: 10.1111/j.1460-9592.2011.03691.x
34. Kristensen AD, Ahlburg P, Lauridsen MC, Jensen TS, Nikolajsen L. Chronic pain after inguinal hernia repair in children. Br J Anaesth. (2012) 109(4):603–8. doi: 10.1093/bja/aes250
35. Cladis FP, Lockman JL, Lupa MC, Chatterjee D, Lim D, Hernandez M, et al. Pediatric anesthesiology fellowship positions: is there a mismatch? Anesth Analg. (2019) 129(6):1784–6. doi: 10.1213/ANE.0000000000004431
36. Ambardekar AP, Schwartz AJ. Availability of pediatric surgery: implications for planning pediatric anesthesiology education. Anesthesiology. (2021) 134(6):826–7. doi: 10.1097/ALN.0000000000003771
37. Tsui BCH, Kirkham K, Kwofie MK, Tran Q, Wong P, Chin KJ, et al. Practice advisory on the bleeding risks or peripheral nerve and interfascial plane blockade: evidence review and expert consensus. Can J Anaesth. (2019) 66(11):1356–84. doi: 10.1007/s12630-019-01466-w
38. Giaufre E, Dalens B, Gombert A. Epidemiology and morbidity of regional anesthesia in children: a one-year prospective survey of the French-language society of pediatric anesthesiologists. Anesth Analg. (1996) 83(5):904–12. doi: 10.1097/00000539-199611000-00003
39. Dalens B, Hasnaoui A. Caudal anesthesia in pediatric surgery: success rate and adverse effects in 750 consecutive patients. Anesth Analg. (1989) 68(2):83–9. doi: 10.1213/00000539-198902000-00002
40. Loganathan AK, Joselyn AS, Babu M, Jehangir S. Implementation and outcomes of enhanced recovery protocols in pediatric surgery: a systematic review and meta-analysis. Pediatr Surg Int. (2022) 38(1):157–68. doi: 10.1007/s00383-021-05008-8
41. Chin KJ, McDonnell JG, Carvalho B, Sharkey A, Pawa A, Gadsden J. Essentials of our current understanding: abdominal wall blocks. Reg Anesth Pain Med. (2017) 42(2):133–83. doi: 10.1097/AAP.0000000000000545
42. Chin KJ, Lirk P, Hollmann MW, Schwarz SKW. Mechanisms of action of fascial plane blocks: a narrative review. Reg Anesth Pain Med. (2021) 46(7):618–28. doi: 10.1136/rapm-2020-102305
43. Chin KJ, Malhas L, Perlas A. The erector spinae plane block provides visceral abdominal analgesia in bariatric surgery: a report of 3 cases. Reg Anesth Pain Med. (2017) 42(3):372–6. doi: 10.1097/AAP.0000000000000581
44. Moore RP, Liu CJ, George P, Welch TP, AuBuchon JD, Jiao Y, et al. Early experiences with the use of continuous erector spinae plane blockade for the provision of perioperative analgesia for pediatric liver transplant recipients. Reg Anesth Pain Med. (2019) 44:679–82. doi: 10.1136/rapm-2018-100253
45. Holland EL, Bosenberg AT. Early experience with erector spinae plane blocks in children. Paediatr Anaesth. (2020) 30(2):96–107. doi: 10.1111/pan.13804
Keywords: acute postoperative pain, nerve block, anesthesia, caudal, pediatrics, abdominal muscles, inguinal hernia, genitourinary surgery
Citation: Hafeman M, Greenspan S, Rakhamimova E, Jin Z, Moore RP and Al Bizri E (2023) Caudal block vs. transversus abdominis plane block for pediatric surgery: a systematic review and meta-analysis. Front. Pediatr. 11:1173700. doi: 10.3389/fped.2023.1173700
Received: 7 March 2023; Accepted: 12 May 2023;
Published: 30 May 2023.
Edited by:
Joris Lemson, Radboud University, NetherlandsReviewed by:
Andres Gomez Fraile, University Hospital October 12, SpainIvana Budic, University of Niš, Serbia
Marieke Voet, Radboud University Medical Centre, Netherlands
© 2023 Hafeman, Greenspan, Rakhamimova, Jin, Moore and Al Bizri. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michael Hafeman michaelrhafeman@gmail.com