Global trends and hotspots on childhood obstructive sleep apnea: a 10-year bibliometric analysis
 Chao Wang
Chao Wang Kai Sun2
Kai Sun2  Huiying Hu
Huiying Hu Zhenkun Yu
Zhenkun Yu- 1School of Medicine, Southeast University, Nanjing, China
- 2Department of Otolaryngology Head and Neck Surgery, BenQ Medical Center, The Affiliated BenQ Hospital of Nanjing Medical University, Nanjing, China
Background: Obstructive sleep apnea (OSA) is children's most common sleep-related breathing disorder. It may develop a wide range of severe complications if not diagnosed promptly and treated effectively. However, Childhood OSA has not specifically been analyzed using a bibliometric approach.
Methods: We respectively collected the research results of childhood OSA from 2013 to 2022 through Web of Science and PubMed. Vosviewer, CiteSpace, and bibliometric online analysis platforms were used for visualizing and analyzing the literature. The MeSH terms were bi-clustered using the Bibliographic Item co-occurrence Matrix Builder (BICOMB) and graph clustering toolkit (gCLUTO) to identify the hotspots.
Results: 4022 publications were finally identified on childhood OSA from 2013 to 2022. The United States has the largest number of publications (1902), accounting for 47.29%. University of Cincinnati is the most productive organization (196), followed by the University of Pennsylvania (151). The most prolific journal was the International Journal of Pediatric Otorhinolaryngology, with 311 documents published. In comparison, Pediatrics is the most cited journal (6936). Gozal D ranked highest among all authors in publication (192). Burst detection shows continuous positive airway pressure, Robin sequence, and nocturnal oximetry are recent keywords of great interest to researchers. Five hotspots were identified by co-word biclustering.
Conclusion: Research over the past ten years has been fruitful, establishing the foundation for childhood OSA. Clusters (0-4) of high-frequency Major Mesh topics have attracted extensive attention. Evaluation and treatment methods of childhood OSA remain major focuses. We believe this article will provide other researchers with new directions and may contribute to a future breakthrough in this field.
1. Introduction
Obstructive sleep apnea (OSA) is the most common sleep-related breathing disorder in children and is characterized by repetitive partial or complete collapse of the upper airways during sleep (1). In the past decade, it has undoubtedly received increasing attention around the world. Children with obstructive sleep apnea may develop a wide range of severe complications if not diagnosed promptly and treated effectively, including abnormal maxillofacial development (adenoid face), behavioral problems, learning disabilities, growth retardation, neurocognitive impairment, metabolic disorders, hypertension, pulmonary hypertension, and even increased risk of cardiovascular events in adulthood (2–5). However, Pediatric OSA has never been analyzed using a bibliometric approach.
Bibliometric analysis is now the most effective tool for examining historical research trends in a specific field (6). By using qualitative and quantitative analysis, it presents the research contributions of different countries, institutions, journals, and authors in scientific fields and forecasts research trends and hotspots (7). Meanwhile, it is imperative to clarify that hotspots and frontiers refer to problems that are not yet resolved in a specific field and are highly concerned by global scholars. Also, the research directions need to be identified urgently and with great importance in the future. Overall, bibliometric analysis has been instrumental in the formulation of policy and clinical guidelines on various diseases.
In this study, we aim to comprehensively assess the global academic status and hotspots relevant to childhood OSA, and to predict future trends in this field.
2. Methods
2.1. Data sources and search strategies
A comprehensive online search of the literature on childhood OSA from 2013 to 2022 was conducted using the Science Citation Index Expanded (SCI-EXPANDED) database via the Web of Science (WoS) Core Collection. For the precaution of bias in database updates, all searches were completed on January 2, 2023. The search strategy was TS = (“obstructive sleep apn*”) AND ALL = (pediatri* OR child*). We set the language to English and only saved original articles and reviews. Medical Subject Headings (MeSH) terms are standardized vocabulary terms for reflecting the main thrust of a literature review. Moreover, it could be used for performing continuous biclustering analysis. Similarly, we searched PubMed based on the screening criteria of (Sleep Apnea, Obstructive[MeSH]) AND (Pediatri* OR Child*), which was developed by the National Center for Biotechnology Information (NCBI) of the National Library of Medicine (NLM).
2.2. Data collection and statistical analysis
Two authors (LK and SK) independently collected all data, with an agreement rate of 0.95, which implies a high level of agreement (8). After converting Web of Science data to txt format, Vosviwer version 1.6.18 (Leiden University, Leiden, The Netherlands) and CiteSpace version 6.1.R3 (Drexel University, Philadelphia, PA, USA) were used to screen and compute the data, as well as the Online Analysis Platform of Literature Metrology (9–11). The data downloaded from PubMed were imported into Bibliographic Item Cooccurrence Matrix Builder (BICOMB), which was developed by China Medical University (12). Eventually, gCLUTO version 1.0, Graphical Clustering Toolkit, was applied for biclustering analysis for MeSh major topics (13).
All literature characteristics were selected to analyze respectively. VOSviewer was applied to analyze and visualize bibliometric data, such as countries, institutions, journals, and authors. Further, we created network visualization plots and density visualization. In the meantime, CiteSpace has a special analysis method called burst-time analysis, a computational technique for identifying the time point when a certain research direction becomes a hotspot. Therefore, we generated a plot of authorship-keyword bursts from a collection of bibliographic records, which will allow us to explore historical points and potential future directions. Additionally, clustering with different numbers of clusters was redirected so that the matrix visualization would result in the most reasonable outcome. In the clusters, we illustrated the semantic relationships between MeSH major topics and the source literature using matrix and mountain visualizations.
3. Results
3.1. Analysis of annual publications
As shown in the flowchart (Figure 1), the initial search retrieved a total of 4,819 publications. After excluding the literature that does not belong to articles and reviews and further limiting language to English, 4,022 articles were finally identified. Publications related to Childhood OSA showed an overall increasing trend from 2013 to 2022, despite a slight decrease in 2015, 2018, 2019, and 2022 (Figure 2).
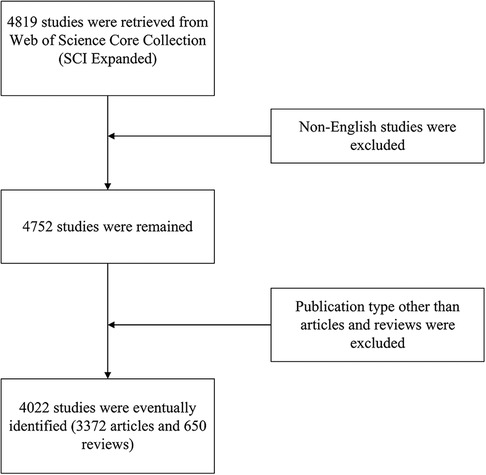
Figure 1. Flow chart of the inclusion process.
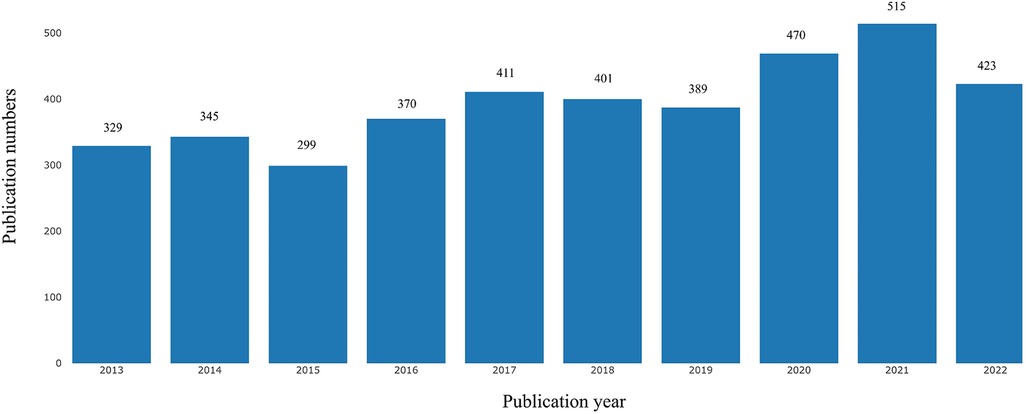
Figure 2. Growth trends of publications on childhood OSA from 2013 to 2022.
3.2. Performance of countries/regions
Over the past decade, at least 64 countries or regions have published studies on childhood OSA. The top 10 national publication is presented in Table 1 and Figure 3. The United States (1,902, 47.29%) was the largest publication contributor, followed by China (510, 12.68%), Canada (326, 8.11%), Italy (276, 6.86%), and Australia (264, 6.56%). Figure 4 demonstrates the cooperation among the countries/regions. The cooperation between the United States and Canada was the closest, followed by the cooperation between the United States and China. Furthermore, Figure 4 also indicates that there is a lack of academic exchange between countries with abundant publications and countries with a limited number of publications.
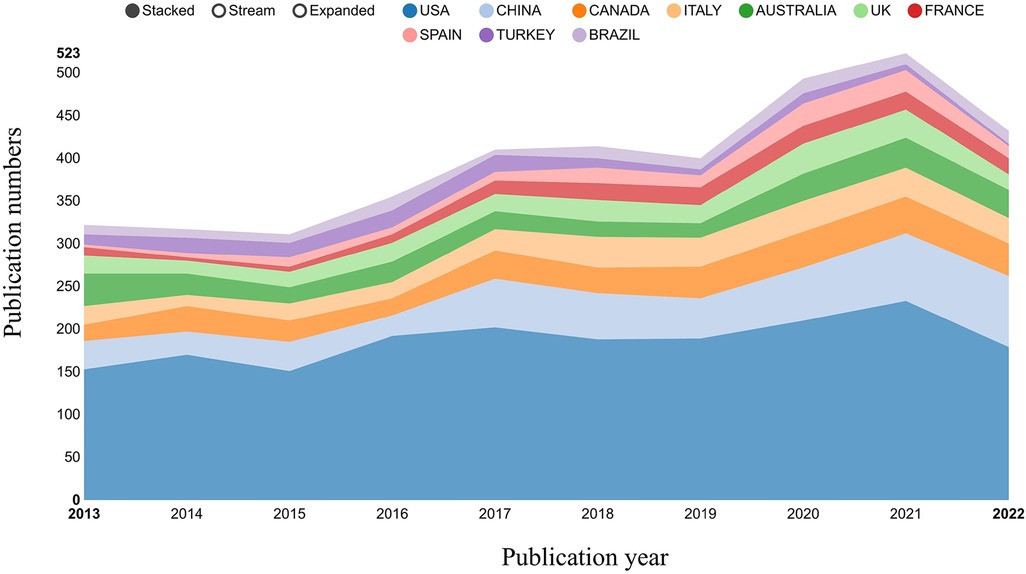
Figure 3. Growth trends of the top 10 countries on childhood OSA from 2013 to 2022.
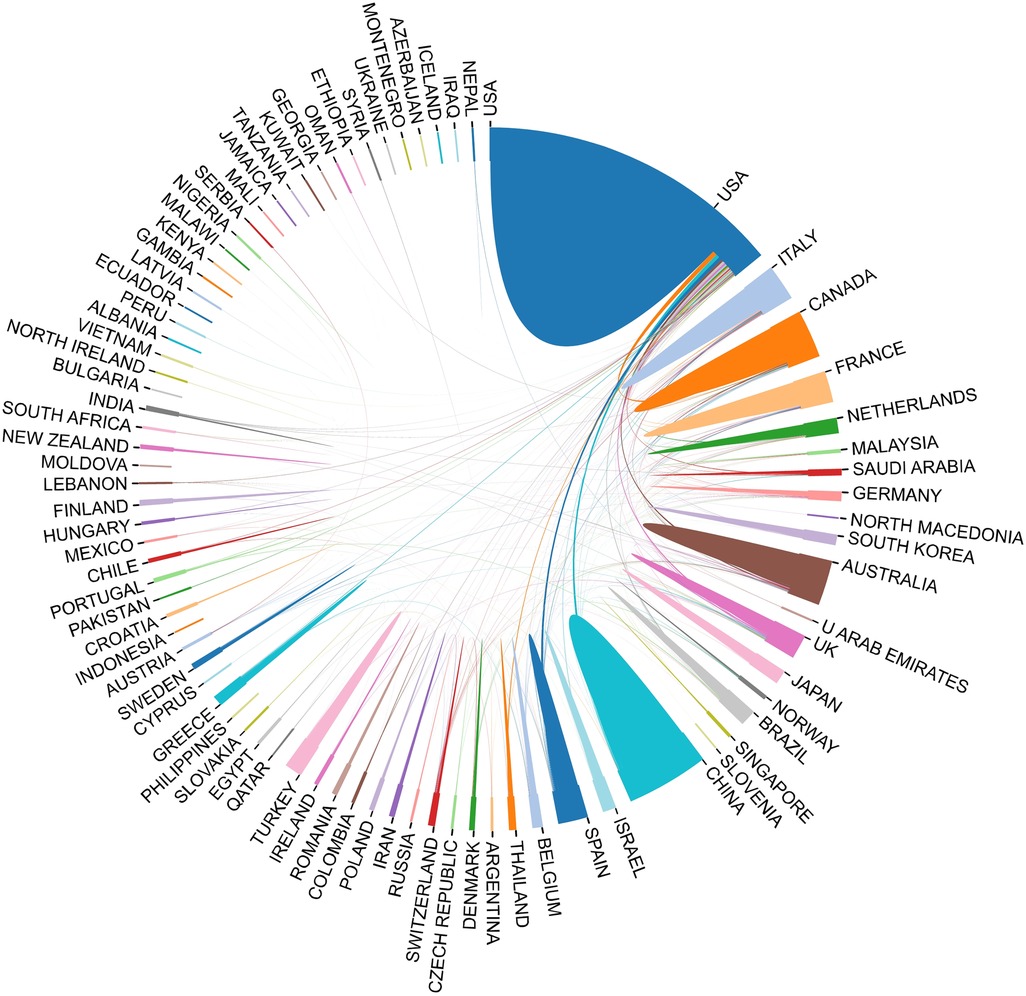
Figure 4. The cooperation between countries on childhood OSA. The thickness of the line between two countries indicates their cooperative relationship strength.
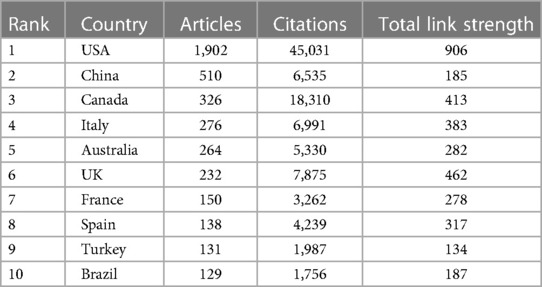
Table 1. Top 10 productive countries and regions.
3.3. Performance of organization
Our study showed that 3,759 organizations had published studies on childhood OSA. We list the top 10 most productive organizations in Table 2. The most prolific organization was the University of Cincinnati (196), followed by the University of Pennsylvania (151) and the University of Chicago (135). Among the top 10 institutions, 7 of 10 were from the United States, corresponding to the distribution by country and region. Further, the research density visualization was plotted by Vosviewer (Figure 5).
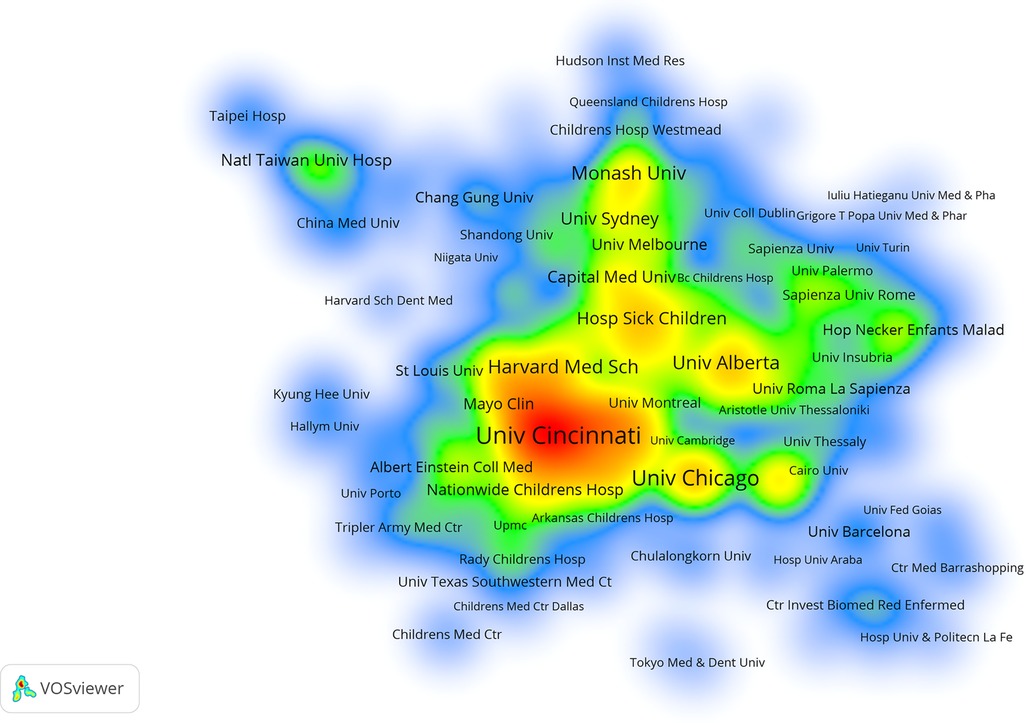
Figure 5. The network visualization of institutions that contributed at least 5 articles on childhood OSA. A gradual increase in the number of publications is represented by color changes from blue to green to yellow to red.
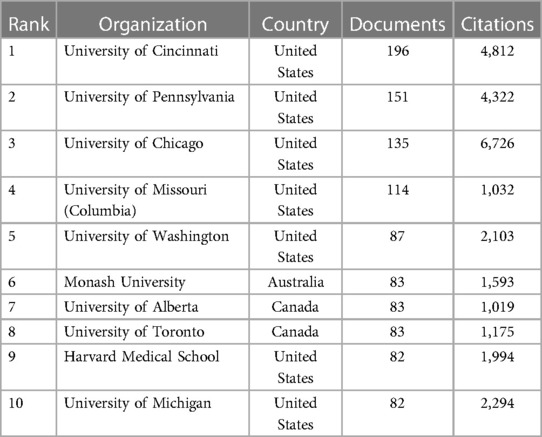
Table 2. Top 10 productive organizations.
3.4. Performance of journals
There were a total of 771 journals that published articles on childhood OSA. We list the top 10 journals of publication in Table 3. The most prolific journal was the International Journal of Pediatric Otorhinolaryngology, with 311 documents published. Then it comes to Journal of Clinical Sleep Medicine, with 207 documents published. Two journals have the characteristic of IF > 5: Otolaryngology-Head and Neck Surgery (5.591) and Sleep (6.313). In addition, the top 10 journals of citation in childhood OSA research are listed in Table 4. We also conducted a co-citation analysis and plotted a network visualization (Figure 6) for journals by Vosviewer. Pediatrics is the most cited journal (6,936 citations), followed by Sleep (6,761 citations) and American Journal of Respiratory and Critical Care Medicine(5,491 citations).
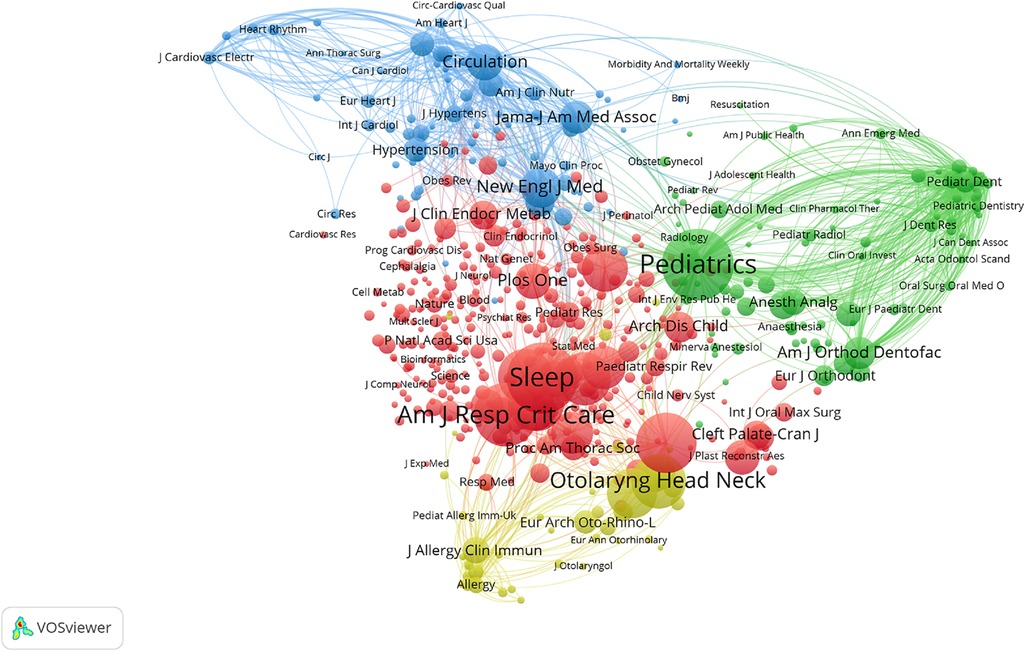
Figure 6. The co-citation network of journals cited at least 50 times on childhood OSA. In network visualization, colors show clustering. The red cluster mainly represents sleep-related journals; the Green cluster mainly represents pediatric journals; the Blue cluster mainly represents cardiovascular journals; the Yellow cluster mainly represents Otorhinolaryngology and Allergy journals.

Table 3. Top 10 journals of publication in childhood OSA research.
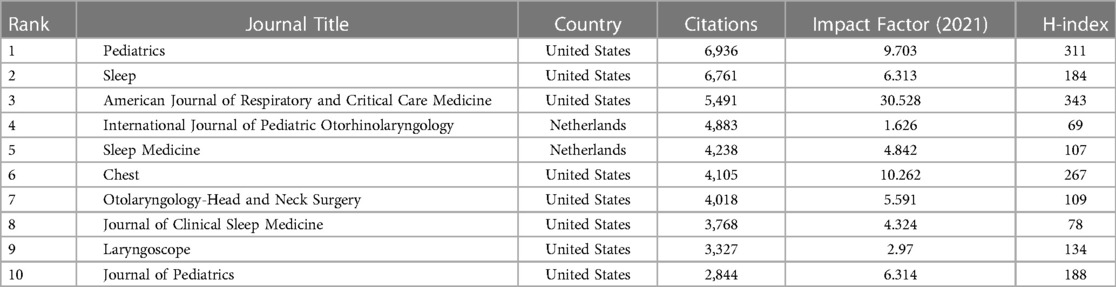
Table 4. Top 10 journals of citation in childhood OSA research.
3.5. Performance of author
Based on our study, 4,022 articles were published by 15,947 authors with at least one article. Table 5 shows the top 10 most productive authors who published articles or reviews in the childhood OSA field. Gozal D ranked highest among all authors (192 articles), followed by Ishman SL (84 articles), Kheirandish-Gozal L (77 articles), and Nixon GM (60 articles).
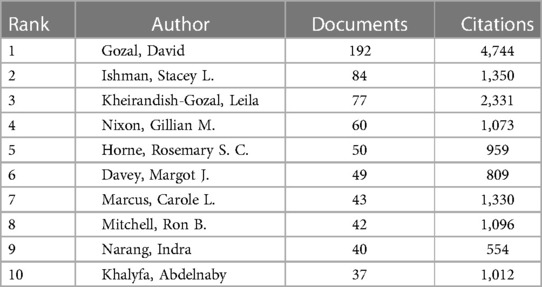
Table 5. Top 10 authors of publication in childhood OSA research.
3.6. Burst detection with keywords
The term “burst words” refers to keywords whose frequency of citations suddenly increases within a short period, providing insight into areas of research that are on the verge of breakthroughs (14). In Figure 7, the green line sliced by year represents the timeline, while the red grid represents the beginning and ending year and the time interval of citation bursts. Apnea/hypopnea syndrome itself ranked first, with the strongest burst strength over the past decade (8.78), followed by meta-analysis (5.88), craniofacial morphology (5.65), community (5.41), magnetic resonance imaging (5.34), and Robin sequence (5.28). From 2020 to 2022, OSA-related research has focused on continuous positive airway pressure (CPAP), Robin sequence, and nocturnal oximetry, suggesting that these topics are currently of great interest to researchers.
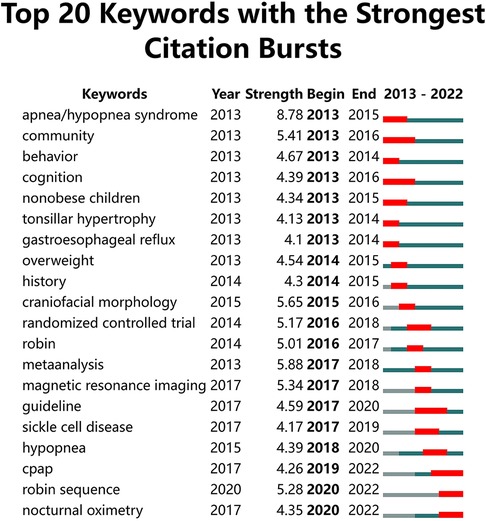
Figure 7. Top 20 keywords with the strongest citation burst. The green line sliced by year represents the timeline, while the red grid represents the beginning and ending year and the time interval of citation bursts.
3.7. Research hotspots based on MeSH term clusters
In our study, 1,387 MeSH major topics were retrieved with a cumulative frequency of 8,830. Based on H index evaluation, we defined terms that appear more than 31 times as high-frequent terms. Table 6 summarizes 30 terms extracted from publications that account for 56.74% (5010/8830) of all terms found in publications. Following that, we derived the high-frequency Major MeSH terms 31 rows × 2,627 columns of the co-word matrix. Subsequently, We imported the matrix into the gCluto software for a biclustering analysis. To promote similar row convergence, we reset the rows of the initial matrix and divide each cluster horizontally by a black line. Eventually, The matrix visualization (Figure 8) and mountain visualization (Figure 9) generated by biclustering analysis were divided into 5 clusters, representing different hotspot directions.
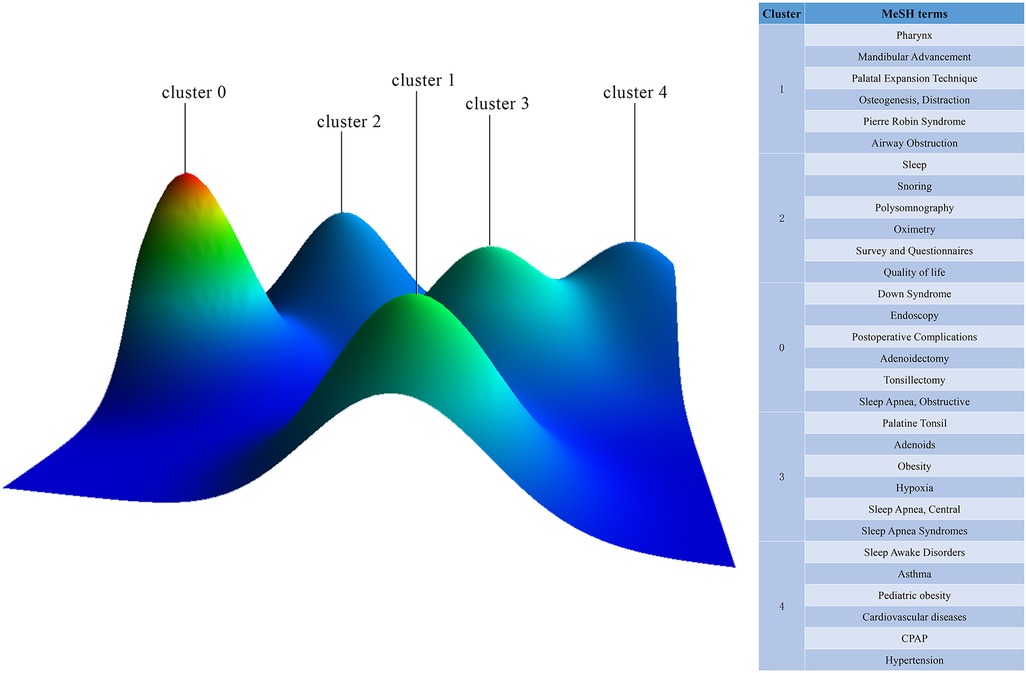
Figure 8. Mountain visualization of the five hot spots by biclustering analysis. The volume of the peaks indicates the quantity of highly frequent Major MeSH terms. A peak's height and color are proportional to its internal similarity and the standard deviation (blue for high deviations and red for low deviations). An interval indicates the degree of similarity between two peaks.
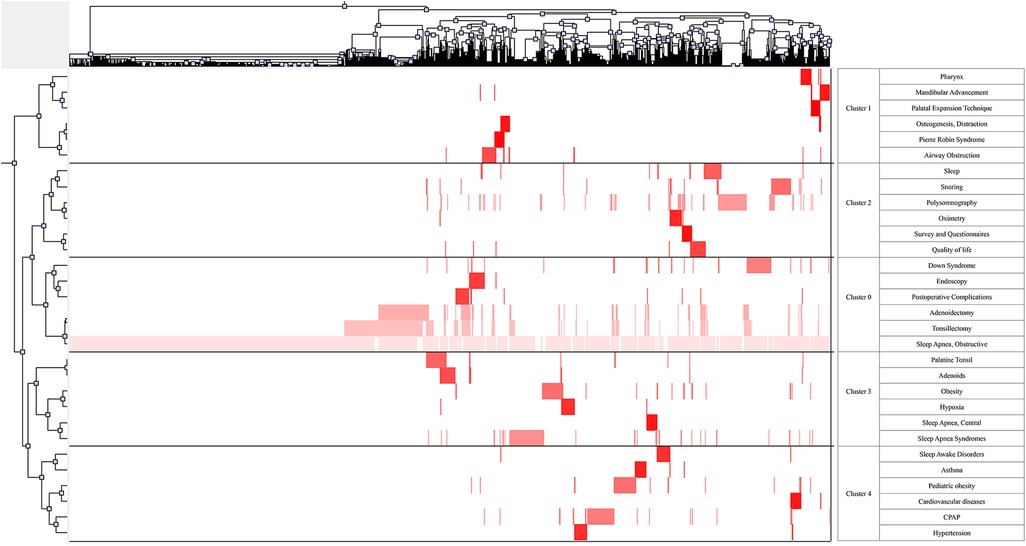
Figure 9. Matrix visualization of the five hot spots by biclustering analysis. Literature is shown at the top, and highly frequent Major MeSH terms are shown on the left. The color of the grid is determined by its frequency (dark red is significant, and white is close to non-significant).

Table 6. Highly frequent major meSH terms.
OSA-related surgery and postoperative complication (cluster 0); New insights into airway obstruction and new techniques for treatment (cluster 1); Evaluation and diagnosis for childhood OSA (cluster 2); Etiology and pathophysiological mechanisms of OSA (cluster 3); Common complications and comorbidities of OSA (cluster 4).
4. Discussion
In recent years, childhood OSA has received increasing attention as more children seek treatment for sleep problems. The statistical and quantitative analysis we conducted revealed that there had been a remarkable improvement in research on childhood OSA from 2013 to 2022, and a growing number of researchers are entering the field. The United States has an absolute leading position in the field of childhood OSA research. Most institutions and authors who have contributed to this field originate in the United States. In comparison with other countries, the United States has advanced equipment, a high-quality experimental environment, and superior clinical trial conditions. In spite of this, countries do not cooperate well among themselves, and research results are not shared efficiently, which impedes global understanding and research efficiency related to childhood OSA. Research on childhood OSA will surely make greater progress if cooperation between countries is strengthened, thereby preventing a great deal of invalid work. Even though there has been a large amount of research on childhood OSA, it remains relatively chaotic and does not include a hotspot analysis. Based on this study, we identified burst keywords in the last decade. Meanwhile, we also interpreted five hot spots on childhood OSA, which are obtained from co-word biclustering. By utilizing these two practical analyses, we could identify hotspots and frontiers in this field.
Cluster 0 focuses on OSA-related surgery and postoperative complication. Adenotonsillectomy (AT) has long been considered the first-line treatment for OSA in children (15). In 2013, The New England Journal of Medicine published a landmark multi-center, randomized controlled trial of adenotonsillectomy (16). This trial compared outcomes in children with OSA who were randomized to watchful waiting or early adenotonsillectomy. After 7months, neurocognitive outcomes were similar in the two groups. However, children in the AT group experienced greater improvements in polysomnography (PSG) parameters, behavior, and quality of life (QoL) scores than those observed. AT has many possible postoperative complications, such as bleeding, hoarseness, difficulty swallowing, and respiratory compromise (17). Children with Down syndrome are at very high risk for OSA, with prevalence rates of 40%–80% compared with prevalence rates of 1%–4% in otherwise healthy children (18). Although AT leads to the successful resolution of OSA in 79% of the general pediatric population, resolution in children with Down syndrome ranges from 6 to 33% (19, 20). Adenotonsillectomy should be considered as a first-line treatment for this population while keeping in mind that monotherapy may not be sufficient in some cases (21). Future studies should further quantify AT outcome indicators and explore other effective adjuvant treatments.
Cluster 1 provides new insights into airway obstruction and techniques for treatment. Pierre Robin Sequence (PRS) is diagnosed by a constellation of characteristics, including micrognathia, glossoptosis, and varying degrees of upper airway obstruction (22, 23). Based on its characteristics, PRS is a leading cause of OSA in newborns. Distraction osteogenesis, like mandibular distraction osteogenesis, is a surgical technique that gradually lengthens the mandible after an osteotomy by using an internal or external distraction device, directly correcting the micrognathia (24). Orthodontists perform rapid palatal expansion on children to reduce nasal resistance, increase nasal volume, elevate tongue posture, and enlarge the pharyngeal airway to treat obstructive sleep apnea (25). Also, mini-implant-assisted rapid palatal expansion has been proven to promote functional breathing (26). Mandibular advancement device (MAD) is a primary treatment alternative for patients with mild to moderate OSA and severe OSA patients who cannot tolerate CPAP (27). By advancing the mandible and tongue towards an anterior position, MAD enlarges the upper airway and reduces its collapsibility while sleeping. Along with technological innovations, an increasing number of alternative treatments for OSA have emerged. Future studies should focus on specific populations, particularly those children with maxillofacial developmental malformations.
Cluster 2 investigates to evaluation and diagnosis of pediatric OSA. PSG parameters, such as AHI, oAHI, PaCO2, and SaO2, have long been considered the gold standard for diagnosing pediatric OSA (28, 29). As a result, doctors and researchers pay more attention to the outcome of PSG, ignoring the real feelings of children. Studies have shown that OSA profoundly affects a child's QoL and behavior (30). Interestingly, the severity of OSA, measured by the obstructive AHI score, does not correlate with the QoL of children with OSA. Consequently, the AHI score does not fully reflect OSA's impact on a child's health and well-being. Thus, it is high time to pay more attention to QoL instruments, such as the OSA-18 questionnaire, to help determine the most appropriate treatment for children with OSA.
Cluster 3 reflects on the etiology and pathophysiological mechanisms of OSA. Traditionally, adenoid and tonsil hypertrophy is considered the most prominent cause of OSA in children. However, several studies have shown that overweight/obese children are more likely to experience the persistence of OSA after an adenotonsillectomy than children within a normal weight range, indicating that obesity is critical in the pathogenesis of OSA (31, 32). There are two main mechanisms through which obesity contributes to OSA. Firstly, the presence of fat at the level of pharyngeal soft tissue reduces lumen caliber and contributes to structural collapse. Secondly, patients have decreased respiratory function due to fat accumulation in the thoracic and abdominal walls (33). Weight-loss management may be critical in treating obesity-related OSA in children, especially for patients who have previously undergone adenotonsillectomy surgery without achieving a satisfactory outcome (34). Despite this, parents do not pay enough attention to their children's weight control (35). Obese-related OSA clinical trials should be expanded, and it is necessary to gather more evidence in the future for this claim.
Cluster 4 focuses on complications and comorbidities of OSA. It has been reported that OSA prevalence can range from 40% to 80% in patients suffering from hypertension, heart failure, coronary artery disease, pulmonary hypertension, atrial fibrillation, and stroke (36). Even though OSA is commonly observed among patients with heart disease, and there is a high risk of adverse cardiovascular outcomes due to OSA-related stressors, OSA is often underrecognized and undertreated in cardiovascular care (37). CPAP should be offered to patients with severe OSA. In this area, future research should focus more on the prevention of OSA-related cardiovascular disease. Asthma and OSA are closely related, which could be attributable to their coexistence, shared risk factors, or distinct interaction mechanisms (38). There should be a better understanding of the relationship between OSA and asthma as soon as possible, both in terms of etiology and therapeutic effects.
5. Strength and limitations
Currently, this study represents the first bibliometric analysis of publications specifically focused on childhood OSA, providing directions regarding hotspots and future directions. Despite this, we realized there still has potential limitations to this study. There might be a difference between the bibliographic analysis data and actual research progress because of the rapid increase in related papers on childhood OSA. Further, the computational error of the database may cause a deviation in the result. For example, Web of Science may mislabel document types, resulting in a dataset containing papers that should be filtered out but missing papers that should be included.
6. Conclusions
In conclusion, global research over the past ten years has also been fruitful, establishing the foundation for childhood OSA. Our bibliometric visualization analysis reveals childhood OSA research's core power and hotspot evolution. Clusters (0–4) of high-frequency Major Mesh topics have attracted extensive attention. Evaluation and treatment methods of childhood OSA remain major focuses. It is worth noting that numerous clinical trials have focused on a specific group of OSA children, and it should be expanded in the future. We believe this article will provide other researchers with new directions and may contribute to a future breakthrough in this field.
Data availability statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding authors.
Author contributions
WC designed the study and drafted the manuscript. LK and SK searched strategy. ZSY, HHY, and LYY completed the statistical analysis. YZK reviewed and modified the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This research was supported by 2019 medical research projects from Jiangsu Commission of Health (key program 14).
Acknowledgments
The authors sincerely thank all reviewers and editors for their comments and help.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Incerti Parenti S, Fiordelli A, Bartolucci ML, Martina S, D'Antò V, Alessandri-Bonetti G. Diagnostic accuracy of screening questionnaires for obstructive sleep apnea in children: a systematic review and meta-analysis. Sleep Med Rev. (2021) 57:101464. doi: 10.1016/j.smrv.2021.101464
2. Chan KC, Au CT, Hui LL, Wing YK, Li AM. Childhood OSA is an independent determinant of blood pressure in adulthood: longitudinal follow-up study. Thorax. (2020) 75(5):422–31. doi: 10.1136/thoraxjnl-2019-213692
3. Shen Y, Xu Z, Shen K. Urinary leukotriene E4, obesity, and adenotonsillar hypertrophy in Chinese children with sleep disordered breathing. Sleep. (2011) 34(8):1135–041. doi: 10.5665/sleep.1178
4. Tseng PH, Lee PL, Hsu WC, Ma Y, Lee YC, Chiu HM, et al. A higher proportion of metabolic syndrome in Chinese subjects with sleep-disordered breathing: a case-control study based on electrocardiogram-derived sleep analysis. PLoS One. (2017) 12(1):e0169394. doi: 10.1371/journal.pone.0169394
5. Kaditis AG, Alonso Alvarez ML, Boudewyns A, Alexopoulos EI, Ersu R, Joosten K, et al. Obstructive sleep disordered breathing in 2- to 18-year-old children: diagnosis and management. Eur Respir J. (2016) 47(1):69–94. doi: 10.1183/13993003.00385-2015
6. Cooper ID. Bibliometrics basics. J Med Libr Assoc. (2015) 103(4):217–8. doi: 10.3163/1536-5050.103.4.013
7. Rosas SR, Kagan JM, Schouten JT, Slack PA, Trochim WM. Evaluating research and impact: a bibliometric analysis of research by the NIH/NIAID HIV/AIDS clinical trials networks. PLoS One. (2011) 6(3):e17428. doi: 10.1371/journal.pone.0017428
8. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. (1977) 33(1):159–74. doi: 10.2307/2529310
9. van Eck NJ, Waltman L. Software survey: vOSviewer, a computer program for bibliometric mapping. Scientometrics. (2010) 84(2):523–38. doi: 10.1007/s11192-009-0146-3
10. Synnestvedt MB, Chen C, Holmes JH. Citespace II: visualization and knowledge discovery in bibliographic databases. AMIA Annu Symp Proc. (2005) 2005:724–8. 16779135
11. Online Analysis Platform: BIBLIOMETRC. 2013. Available at: http://bibliometric.com
12. Lei C WL, Lei Y, Han Z, Yuefang H, Yingna H, Hao Z. Development of a text mining system based on the co-occurrence of bibliographic items in literature databases. New Technol of Library and Infor Ser. (2008) 8:70–5. doi: 10.3969/j.issn.1003-3513.2008.08.013
13. Lab K. gCLUTO-Graphical Clustering Toolkit. 2014. Available at: http://glaros.dtc.umn.edu/gkhome/cluto/gcluto/download
14. Hao KJ, Jia X, Dai WT, Huo ZM, Zhang HQ, Liu JW, et al. Mapping intellectual structures and research hotspots of triple negative breast cancer: a bibliometric analysis. Front Oncol. (2021) 11:689553. doi: 10.3389/fonc.2021.689553
15. Marcus CL, Brooks LJ, Draper KA, Gozal D, Halbower AC, Jones J, et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. (2012) 130(3):576–84. doi: 10.1542/peds.2012-1671
16. Marcus CL, Moore RH, Rosen CL, Giordani B, Garetz SL, Taylor HG, et al. A randomized trial of adenotonsillectomy for childhood sleep apnea. N Engl J Med. (2013) 368(25):2366–76. doi: 10.1056/NEJMoa1215881
17. De Luca Canto G, Pachêco-Pereira C, Aydinoz S, Bhattacharjee R, Tan HL, Kheirandish-Gozal L, et al. Adenotonsillectomy complications: a meta-analysis. Pediatrics. (2015) 136(4):702–18. doi: 10.1542/peds.2015-1283
18. Marcus CL, Keens TG, Bautista DB, von Pechmann WS, Ward SL. Obstructive sleep apnea in children with down syndrome. Pediatrics. (1991) 88(1):132–9. doi: 10.1542/peds.88.1.132
19. Maris M, Verhulst S, Wojciechowski M, Van de Heyning P, Boudewyns A. Outcome of adenotonsillectomy in children with down syndrome and obstructive sleep apnoea. Arch Dis Child. (2017) 102(4):331–6. doi: 10.1136/archdischild-2015-310351
20. Nation J, Brigger M. The efficacy of adenotonsillectomy for obstructive sleep apnea in children with down syndrome: a systematic review. Otolaryngol Head Neck Surg. (2017) 157(3):401–8. doi: 10.1177/0194599817703921
21. Seither K, Helm BM, Heubi C, Swarr D, Suhrie KR. Sleep apnea in children with down syndrome. Pediatrics. (2023) 151(3):e2022058771. doi: 10.1542/peds.2022-058771
22. Robin P. A fall of the base of the tongue considered as a new cause of nasopharyngeal respiratory impairment: pierre robin sequence, a translation. 1923. Plast Reconstr Surg. (1994) 93(6):1301–3. doi: 10.1097/00006534-199405000-00032
23. Hsieh ST, Woo AS. Pierre robin sequence. Clin Plast Surg. (2019) 46(2):249–59. doi: 10.1016/j.cps.2018.11.010
24. Breugem CC, Logjes RJH, Nolte JW, Flores RL. Advantages and disadvantages of mandibular distraction in robin sequence. Semin Fetal Neonatal Med. (2021) 26(6):101283. doi: 10.1016/j.siny.2021.101283
25. Fernández-Barriales M, Lafuente-Ibáñez de Mendoza I, Alonso-Fernández Pacheco JJ, Aguirre-Urizar JM. Rapid maxillary expansion versus watchful waiting in pediatric OSA: a systematic review. Sleep Med Rev. (2022) 62:101609. doi: 10.1016/j.smrv.2022.101609
26. Brunetto DP, Moschik CE, Dominguez-Mompell R, Jaria E, Sant'Anna EF, Moon W. Mini-implant assisted rapid palatal expansion (MARPE) effects on adult obstructive sleep apnea (OSA) and quality of life: a multi-center prospective controlled trial. Prog Orthod. (2022) 23(1):3. doi: 10.1186/s40510-021-00397-x
27. Uniken Venema JAM, Rosenmöller B, de Vries N, de Lange J, Aarab G, Lobbezoo F, et al. Mandibular advancement device design: a systematic review on outcomes in obstructive sleep apnea treatment. Sleep Med Rev. (2021) 60:101557. doi: 10.1016/j.smrv.2021.101557
28. Sateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. (2014) 146(5):1387–94. doi: 10.1378/chest.14-0970
29. [Chinese guideline for the diagnosis and treatment of childhood obstructive sleep apnea (2020)]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. (2020) 55(8):729–47. doi: 10.3760/cma.j.cn115330-20200521-00431
30. Baldassari CM, Mitchell RB, Schubert C, Rudnick EF. Pediatric obstructive sleep apnea and quality of life: a meta-analysis. Otolaryngol Head Neck Surg. (2008) 138(3):265–73. doi: 10.1016/j.otohns.2007.11.003
31. Mitchell RB, Kelly J. Outcome of adenotonsillectomy for obstructive sleep apnea in obese and normal-weight children. Otolaryngol Head Neck Surg. (2007) 137(1):43–8. doi: 10.1016/j.otohns.2007.03.028
32. Andersen IG, Holm JC, Homøe P. Obstructive sleep apnea in children and adolescents with and without obesity. Eur Arch Otorhinolaryngol. (2019) 276(3):871–8. doi: 10.1007/s00405-019-05290-2
33. Fiorino EK, Brooks LJ. Obesity and respiratory diseases in childhood. Clin Chest Med. (2009 Sep) 30(3):601–8. x. doi: 10.1016/j.ccm.2009.05.010
34. Ersu R, Chen ML, Ehsan Z, Ishman SL, Redline S, Narang I. Persistent obstructive sleep apnoea in children: treatment options and management considerations. Lancet Respir Med. (2023) 11(3):283–96. doi: 10.1016/s2213-2600(22)00262-4
35. Andersen IG, Holm JC, Homøe P. Impact of weight-loss management on children and adolescents with obesity and obstructive sleep apnea. Int J Pediatr Otorhinolaryngol. (2019) 123:57–62. doi: 10.1016/j.ijporl.2019.04.031
36. Yeghiazarians Y, Jneid H, Tietjens JR, Redline S, Brown DL, El-Sherif N, et al. Obstructive sleep apnea and cardiovascular disease: a scientific statement from the American heart association. Circulation. (2021) 144(3):e56–67. doi: 10.1161/cir.0000000000000988
37. Kwok KL, Ng DK, Chan CH. Cardiovascular changes in children with snoring and obstructive sleep apnoea. Ann Acad Med Singap. (2008) 37(8):715–21. doi: 10.47102/annals-acadmedsg.V37N8p715
Keywords: obstructive sleep apnea, children, global trends, hotspots, bibliometric analysis
Citation: Wang C, Sun K, Zhang S, Hu H, Lu Y, Liu K and Yu Z (2023) Global trends and hotspots on childhood obstructive sleep apnea: a 10-year bibliometric analysis. Front. Pediatr. 11:1160396. doi: 10.3389/fped.2023.1160396
Received: 14 February 2023; Accepted: 24 April 2023;
Published: 10 May 2023.
Edited by:
Seyed Aria Nejadghaderi, Tabriz University of Medical Sciences, IranReviewed by:
David Ingram, Children's Mercy Kansas City, United StatesSeyed Ehsan Mousavi, Tabriz University of Medical Sciences, Iran
© 2023 Wang, Sun, Zhang, Hu, Lu, Liu and Yu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kai Liu assimy1986@126.com Zhenkun Yu yuzhenkun@yahoo.com