 Nathan Benzazon1,2*
Nathan Benzazon1,2* Julie Colnot1,2,3François de Kermenguy1,2Samir Achkar2Florent de Vathaire4
Julie Colnot1,2,3François de Kermenguy1,2Samir Achkar2Florent de Vathaire4 Eric Deutsch1,2
Eric Deutsch1,2 Charlotte Robert1,2†Ibrahima Diallo1,2*†
Charlotte Robert1,2†Ibrahima Diallo1,2*†- 1Unité Mixte de Recherche (UMR) 1030 Radiothérapie Moléculaire et Innovation Thérapeutique, ImmunoRadAI, Université Paris-Saclay, Institut Gustave Roussy, Inserm, Villejuif, France
- 2Department of Radiation Oncology, Gustave Roussy, Villejuif, France
- 3THERYQ, PMB-Alcen, Peynier, France
- 4Unité Mixte de Recherche (UMR) 1018 Centre de Recherche en épidémiologie et Santé des Populations (CESP), Radiation Epidemiology Team, Université Paris-Saclay, Institut Gustave Roussy, Inserm, Villejuif, France
A growing body of scientific evidence indicates that exposure to low dose ionizing radiation (< 2 Gy) is associated with a higher risk of developing radio-induced cancer. Additionally, it has been shown to have significant impacts on both innate and adaptive immune responses. As a result, the evaluation of the low doses inevitably delivered outside the treatment fields (out-of-field dose) in photon radiotherapy is a topic that is regaining interest at a pivotal moment in radiotherapy. In this work, we proposed a scoping review in order to identify evidence of strengths and limitations of available analytical models for out-of-field dose calculation in external photon beam radiotherapy for the purpose of implementation in clinical routine. Papers published between 1988 and 2022 proposing a novel analytical model that estimated at least one component of the out-of-field dose for photon external radiotherapy were included. Models focusing on electrons, protons and Monte-Carlo methods were excluded. The methodological quality and potential limitations of each model were analyzed to assess their generalizability. Twenty-one published papers were selected for analysis, of which 14 proposed multi-compartment models, demonstrating that research efforts are directed towards an increasingly detailed description of the underlying physical phenomena. Our synthesis revealed great inhomogeneities in practices, in particular in the acquisition of experimental data and the standardization of measurements, in the choice of metrics used for the evaluation of model performance and even in the definition of regions considered out-of-the-field, which makes quantitative comparisons impossible. We therefore propose to clarify some key concepts. The analytical methods do not seem to be easily suitable for massive use in clinical routine, due to the inevitable cumbersome nature of their implementation. Currently, there is no consensus on a mathematical formalism that comprehensively describes the out-of-field dose in external photon radiotherapy, partly due to the complex interactions between a large number of influencing factors. Out-of-field dose calculation models based on neural networks could be promising tools to overcome these limitations and thus favor a transfer to the clinic, but the lack of sufficiently large and heterogeneous data sets is the main obstacle.
1 Introduction
New technological development in external radiotherapy currently allows, in particular through intensity modulation or stereotactic techniques, an accurate delivery of dose to the target volumes, while minimizing toxic effects on neighboring healthy organs (1, 2). This has led to an increase in overall survival for a large majority of cancer diseases (3). The assessment of the doses delivered outside the high-energy photon treatment field (out-of-field dose) has been an active research area in radiotherapy physics since the 1980s. The increased interest in out-of-field doses coincided with the publication in 1980 of the United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) report on the Biological Effects of Ionizing Radiations (BEIR) which provided data supporting a slight increase in the risk of radiation-induced second cancers from dose levels of few milligrays [BEIR III (4)]. The implementation of solutions for a comprehensive evaluation of out-of-field doses became therefore essential, initially for epidemiological studies on the potential induction of second cancers at distance from the radiotherapy target volume, in particular among patients treated during childhood (5–8). The concern about the risk of second cancers further increased in recent years with the generalization of intensity modulated radiation therapy (IMRT), significantly increasing the volumes of healthy tissues receiving low doses of ionizing radiation (9, 10), especially since the number of cancer survivors increases (11), in particular among children (12). However, even today, radiotherapy treatment planning systems (TPS) do not allow accurate evaluation of the doses delivered at distance from the target volume because they are specifically commissioned for precise dose calculation within the beams (13). This has been demonstrated for 3-D conformal radiotherapy (13, 14), for IMRT (15–20) and also for the CyberKnife system (Accuray, Sunnyvale, USA) (21, 22).
Different strategies have been developed by radiotherapy physics research teams as an alternative to TPS to precisely estimate out-of-field doses and to provide large amounts of data for epidemiological studies. To this aim, outstanding experimental works have been performed first (23, 24), paving the way to software implementing analytical modeling (25, 26) or implementation of Monte Carlo simulations (27, 28). Yet, to the best of our knowledge, the use of these calculation software remains so far confined to dosimetry for epidemiological research programs. This might be either due to a potential unsatisfactory quality compared to the clinical expectations because of limitations inherent to the implemented models, or simply to the fact that the clinical need is not proven for out-of-field dosimetry.
Regarding the clinical need, the context is now evolving favorably. Indeed, by recommending reporting the dose to the remaining volume at risk (RVR), the International Commission on Radiation Units and Measurements (ICRU) in its report 83 released in 2010, encourages clinicians to widen the dose calculation area so as to encompass the whole patient imaged volume (29). To implement this recommendation, TPS manufacturers will have to upgrade their dose calculation to enable accurate estimation of the dose at greater distances from the target volume than is currently done. In addition, these last years, research on immunotherapy and its association with radiotherapy triggers a renewed interest in out-of-field dose determination, with the goal to assess their potential impact on the patient’s immune system. This is especially important since lymphocytes, including T cells, are known to be particularly radiosensitive (30–33). As a matter of fact, one of the side effects commonly observed in radiotherapy patients is radiation-induced lymphopenia, which is characterized by a significant drop in the quantity of lymphocytes circulating in the blood after irradiation (34). Numerous studies tend to show that severe lymphopenia during radiotherapy is a poor prognostic factor for overall survival and progression-free survival in several tumor locations (35–38). However, the underlying mechanisms related to its severity and duration are still poorly understood, and the effect of irradiation on immune cells in the circulating blood and lymphoid organs, which requires the use of out-of-field dose calculation algorithms, could be an avenue of study for the understanding of radiation-induced lymphopenia, and more generally, the iatrogenic effects of radiotherapy on the immune response (39).
In this work, we conduct, as recommended (40, 41), a scoping review for the purpose of: (1) identifying and defining key concepts, (2) identifying available analytical models for out-of-field dose calculation and evidence of their methodological quality and limitations with regard to their applicability in a clinical workflow, (3) identifying priority areas of work, (4) identifying the role that artificial intelligence and in particular neural networks could play in this context.
2 Materials and methods
2.1 Key concepts and definitions
In 1941, Clarkson (42) proposed a method to calculate the dose at any point within the volume receiving radiation from a photon beam even outside its geometrical limit. The dose was decomposed into two components: the dose due to primary radiation and the dose due to secondary radiation. The doses due to primary and secondary radiation were defined as the dose delivered by a theoretical zero radius circular field, and the additional dose due to the increase in field radius, respectively. Then, in the early 1980s, the group of (23) adapted the notions of primary and secondary radiation for their application on dose outside the photon treatment field. According to Kase, the primary dose is confined within the treatment field while the secondary radiation can be decomposed into three main distinct elements: the patient scatter corresponding to particles which have already interacted once into the treatment field and are scattered; the collimator scatter (or head scatter), corresponding to particles which have already interacted once into the accelerator head and are scattered; and finally, the leakage radiation, which corresponds to primary particles passing through the accelerator head, to finally deposit their energy out of the treatment field. Kase also studied the magnitude of the scatter component from the room and concluded that this component is negligible compared to the three others (Figure 1). For medical linear accelerators operating above 10 MV, it is necessary to consider in addition a neutron dose component from (γ, n)-type reactions (43, 44).
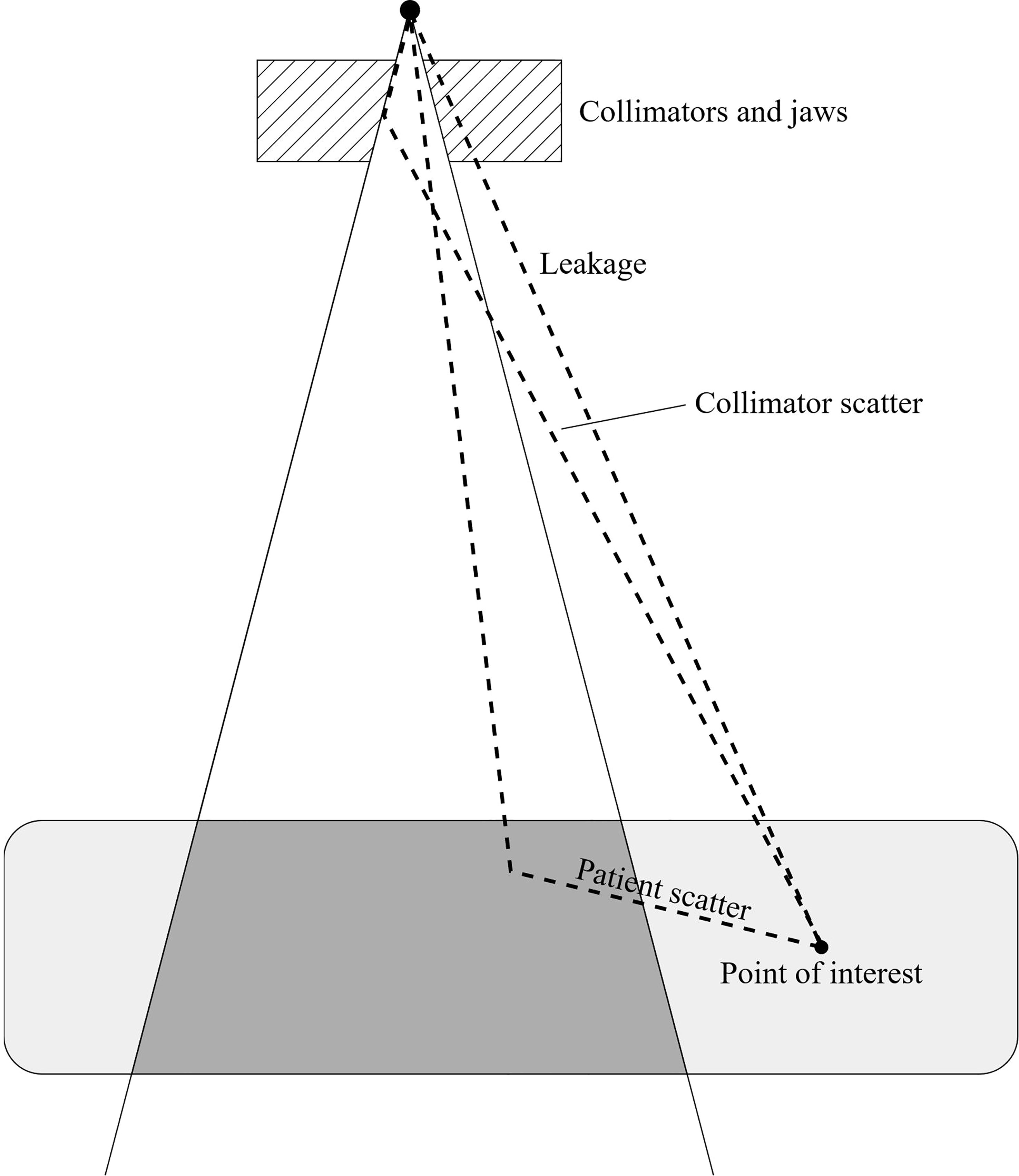
Figure 1 Secondary dose components for a point of interest located outside the treatment field (inspired from (23)).
2.2 Search strategy and inclusion criteria
A search through PubMed/MEDLINE database with the search terms “out-of-field dose”, “stray radiation”, and “peripheral dose” was run. In addition, previous reviews on the topic (45–48) were examined and the list of references of each eligible paper was screened to identify studies potentially missed with the search terms. We included articles published in English, between January 1988 and December 2022, reporting a novel analytical formalism for the evaluation of at least one component of the out-of-field dose in photon external beam radiation therapy (EBRT), or providing information supporting the potential for clinical application of a previously reported model. We have deliberately concentrated our work on photon treatments, as this is the treatment modality still used in the majority of cases today (49). It should be noted that other similar studies have addressed the issue of dose modeling in the scientific literature for other particles (e.g. for protons (50)) and are therefore complementary to this work. Thus, articles focusing on protons or electrons beams were excluded. Similarly, with the goal to move to clinics, we also excluded articles reporting studies primarily designed for out-of-field dose calculations with a MC method and studies limited to experimental investigations. Indeed, if MC simulation is considered by many research teams as the gold standard for dose calculation and has been successfully used in various research areas, the computational resources and time required for dose estimation are too high to be compatible with the constraints of clinical routine, even more so to obtain a sufficiently low statistical uncertainty of type A for voxels located outside the radiation field (51). While significant literature exists on experimental measurements dedicated to out-of-field dose (52), publications that did not perform these for the adaptation of an analytical method were not reviewed.
2.3 Data extraction, synthesis, and study quality assessment
The methodological quality and potential limitations of the included articles were assessed with respect to the compatibility of the model with the clinical workflow. We have identified four key criteria that a model must meet in order to be considered compatible with clinical routine workflow. These criteria include accuracy, robustness, calculation time, and convenience. Thus, in addition to accurate dose estimation for each new patient anatomy in a time frame compatible with clinical management, the model must be effective across a wide range of irradiation configurations, while integrating seamlessly into the conventional patient management process, i.e., without imposing an additional burden. A data abstraction form was developed to collect all relevant information: year of publication, country, description of the mathematical formalism of the model, experimental conditions and setup used for measurements, evaluation metrics, associated results and limits. A comments section was used to capture any remaining relevant information not filled in by the existing fields. Missing data were treated as not reported. Data synthesis and study quality assessment were performed independently by two reviewers (NB, ID) who then cross-checked their reports to reach a consensus on quality assessment.
3 Results
3.1 Selected studies
The flowchart in Figure 2 depicts the flow of information through our article identification and selection process. 101 publications identified through the database search were reviewed against our inclusion criteria and 21 were retained for synthesis analyses. The median publication year was 2015 (range: 1988-2022) (Table 1).
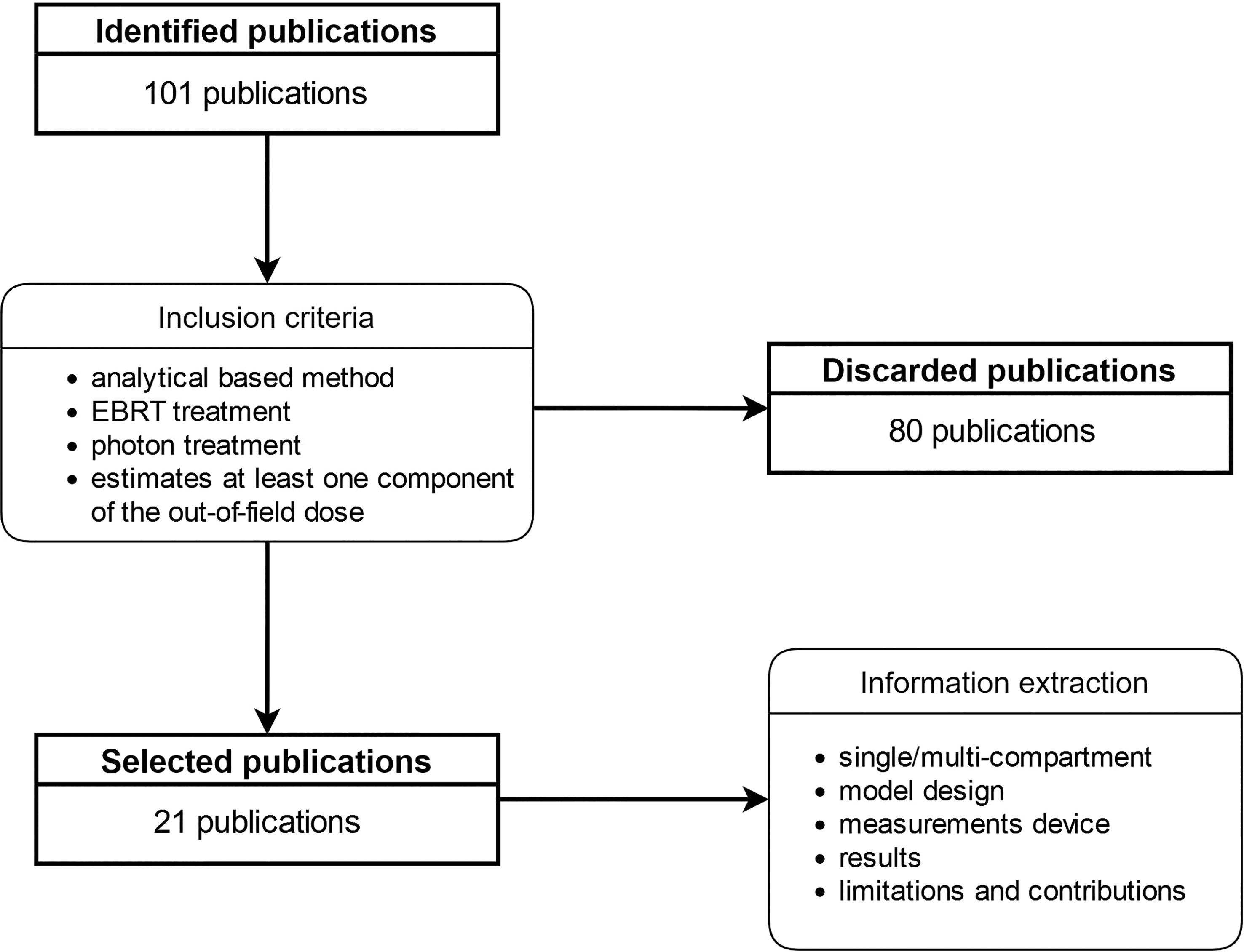
Figure 2 Information extraction and inclusion criteria pipeline.

Table 1 Methods implemented for acquisitions of experimental data used to set the model basic physical aspects and parameters in the 21 selected articles.
We have referred to Gilbert & Boulter (56) to state our definition of the term “model”. Thus, the term “analytical model” denotes the mathematical representation, in general simplified, describing the out-of-field dose distribution. In this work, “Single-Compartment” refers to models derived by fitting experimental data from in-phantom dose measurements, without addressing each component separately. In contrast, models implementing a mathematical formulation intended to fit the different contributions to the out-of-field dose were categorized as “Multi-Compartment”. Both approaches can be based on empirical or semi-empirical/physical mathematical formalisms.
Table 1 summarizes the methods used for experimental data acquisitions in the 21 selected articles. Seven were reported as single-compartment models: the oldest (25) and the most recent model (57) belong to this category. The remaining articles were multi-compartment models with sub-models dedicated to each of the dose components. One model (43) also included features for secondary neutron dose component.
Although all the models allow the calculation of out-of-field doses for 3-D conformal radiotherapy, only 7 claimed to be suitable for modern techniques as well, in particular IMRT and volumetric arc therapy (VMAT) (Table 2). Two articles have a specific approach as they are restricted to model the head scatter component (59) or the head scatter and leakage components (60). Another specific group concerns the articles whose purpose is to implement new features to extend the scope of previously published models, like the utilization of method already developed on new data, the implementation of methods into a software, or into a TPS (61–63).
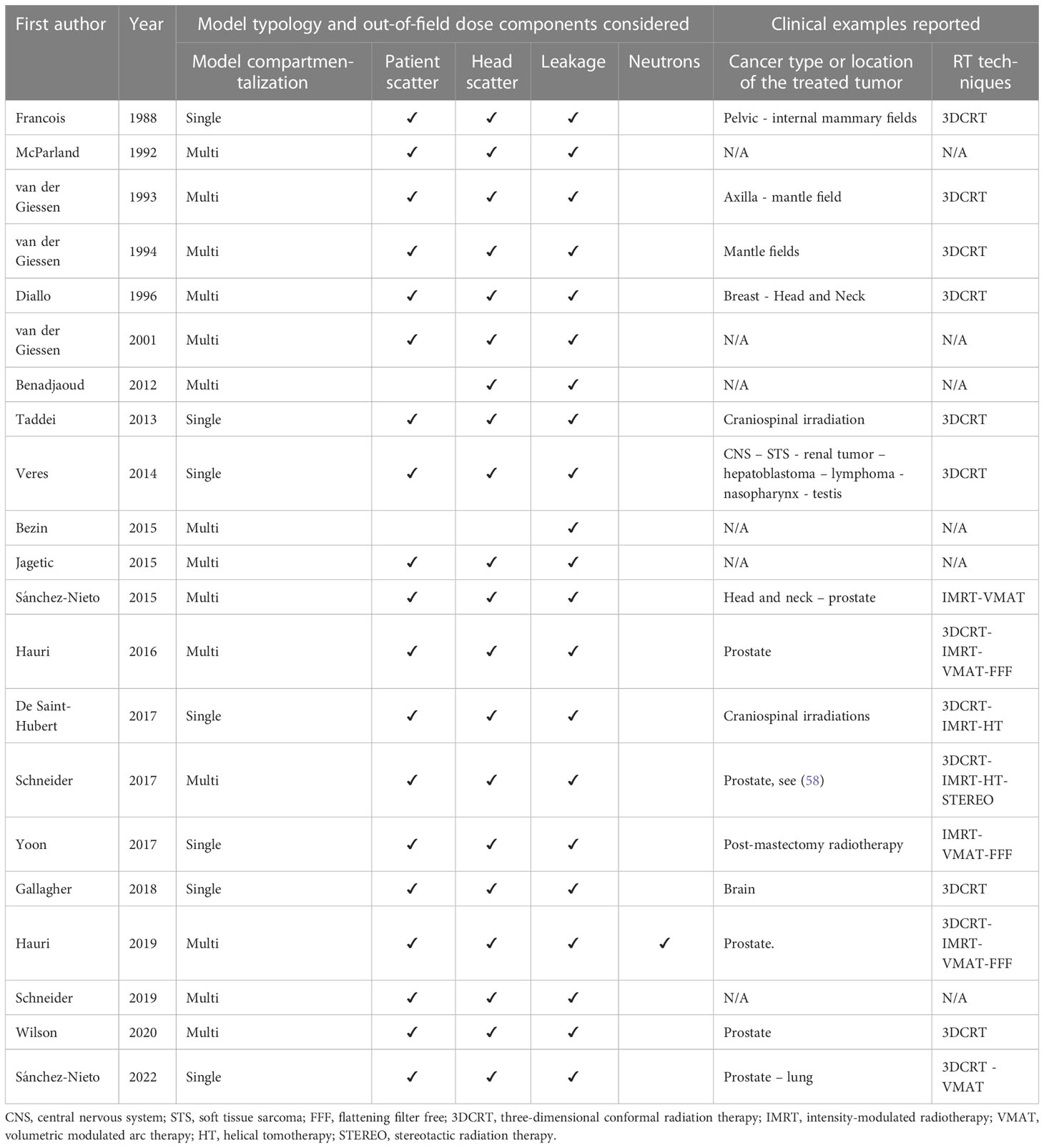
Table 2 Modeling approaches and realistic clinical situations considered in order to test the possibility of clinical transfer of the models presented in the 21 selected articles.
3.2 Experimental device
The characteristics of the treatment machines investigated, the phantoms and the detectors used are summarized in Table 1. Among the 21 selected articles, 16 detailed the experimental device used for the acquisition of input data for the model development. The remaining 5 are about implementation of already existing models.
3.2.1 Treatment machines investigated
Depending on the research groups, measurements were performed by an orthovoltage unit operated at 200 kVp and a cobalt-60 machines (25), different medical accelerators operated at 6 MV (20, 53, 57, 61, 64), 10 MV (20) and 25 MV (25). Measurements could have been made for a set of simple geometry open square and rectangular fields (25, 65) or, for a set of reference treatment plans-specific beam settings (20, 53, 57, 61, 64).
3.2.2 Phantoms
The analytical models presented all share the need for absorbed dose measurements at a set of carefully selected relevant out-of-field locations either in a simple geometry water or water-equivalent solid phantom or in an anthropomorphic phantom. In addition, in-air measurements are sometimes carried-out by some authors (6, 59, 66, 67). Among the experimental methods reported, the tendencies in decreasing order of frequency, appeared to be the use of a water tank or a water equivalent slab phantom of simple geometry (9 out of 16 publications), an anthropomorphic phantom (5 out of 16) or even direct in-air measurements (2 out of 16).
3.2.3 Detectors
Ionization chambers and thermoluminescent dosimeters (TLDs) are the two most commonly used types of detectors for these measurements, with similar frequencies of use, each being involved in 50% of the publications. In case of measurements in an anthropomorphic phantom, TLDs of type TLD-100 (20, 53, 57, 61) or an ultra-sensitive MCP-N type TLDs (64) were employed. Diamond detectors (55, 63, 67) or solid-state diode dosimeter (67) were also used. Less often, radiophotoluminescent (RPL) and optically stimulated luminescence (OSL) detectors were involved (55). In specific situations where the objective was to assess secondary neutrons contribution to the out-of-field dose, combinations of different TLDs types i.e. TLD100 (LiF:Mg,Ti), TLD100H (LiF:Mg,Cu,P), TLD600/700 (LiF:Mg,Ti) and TLD700H (7LiF:Mg,Cu,P) were used synergistically (43, 68). In addition, MC simulations were performed by some groups, as a surrogate or to supplement their experimental data (43, 57, 67).
3.3 Single-compartment models
Experimental protocol to measure all the components of the out-of-field dose as a whole.
The methodologies implemented by the different research groups for single-compartment models development consisted in an experimental measurement campaign of the total out-of-field dose.
3.3.1 Mathematical formalisms
Two types of models can be observed:
One approach discriminates the near field and the distant regions (25, 53, 57, 61, 64). In this case, the sector integration method, proposed by (42) and investigated by (69), was implemented by the Gustave Roussy’s group (25), whilst the group from MD Anderson Cancer Center (53, 61, 64) opted for the double-Gaussian description originally proposed by (70). The group from the Pontificia Universidad Católica de Chile (57) used an expression combining an exponential attenuation and the inverse square law. For distant regions, formula fitting the isodoses using either a combination of parametric elliptical equations (25), a (70) Gaussian function (53, 61, 64), or a constant background (57) were implemented. Let us illustrate this model family with (53). In (53), the normalized out-of-field dose (in cGy.Gy-1) was expressed as a function of the distance from the field edge (), by the sum of two gaussians (equation 1). The resulting absorbed dose, , correspond to the absorbed dose normalized to the prescribed therapeutic dose.
With and the means of each gaussian, and the associated standard deviations, and and two magnitude factors. In this expression, one gaussian modeled the dose near the field edges, and the second one modeled the dose at a greater distance from the field.
Another one addressed the whole volume by a unique formula (20, 65). The out-of-field dose was thus deduced from the central axis depth dose or by the prescribed dose by applying a multiplicative coefficient defined as a polynomial function of order two depending on the inverse of the distance to the edge of the field (20) or from out-of-field dose profiles obtained from water phantom measurements (65). Model developed by (20) illustrates this approach. In (20), the out-of-field dose was mathematically expressed as follows:
With the prescription dose, the distance from the field edge, and , , and fitting parameters.
3.4 Multi-compartment models
Experimental protocol implemented to separate the out-of-field dose components
All the research groups proposing multi-compartmental models, except (6) and (59), have referred to the (23) experimental protocol. In this protocol, illustrated in Figure 3, collimator scatter and head leakage are measured in water by directing the primary beam outside the phantom, the head leakage being assessed by closing the jaws. The contribution of patient scattering is evaluated by subtracting the measurements performed with the primary beam irradiating the phantom from the values obtained previously with the open field. Other strategies were proposed such as in-air measurements to map the incident photons energy fluence around the treatment beam (6), to assess collimator scatter and head leakage photons characteristics (26) or to map head leakage (59).
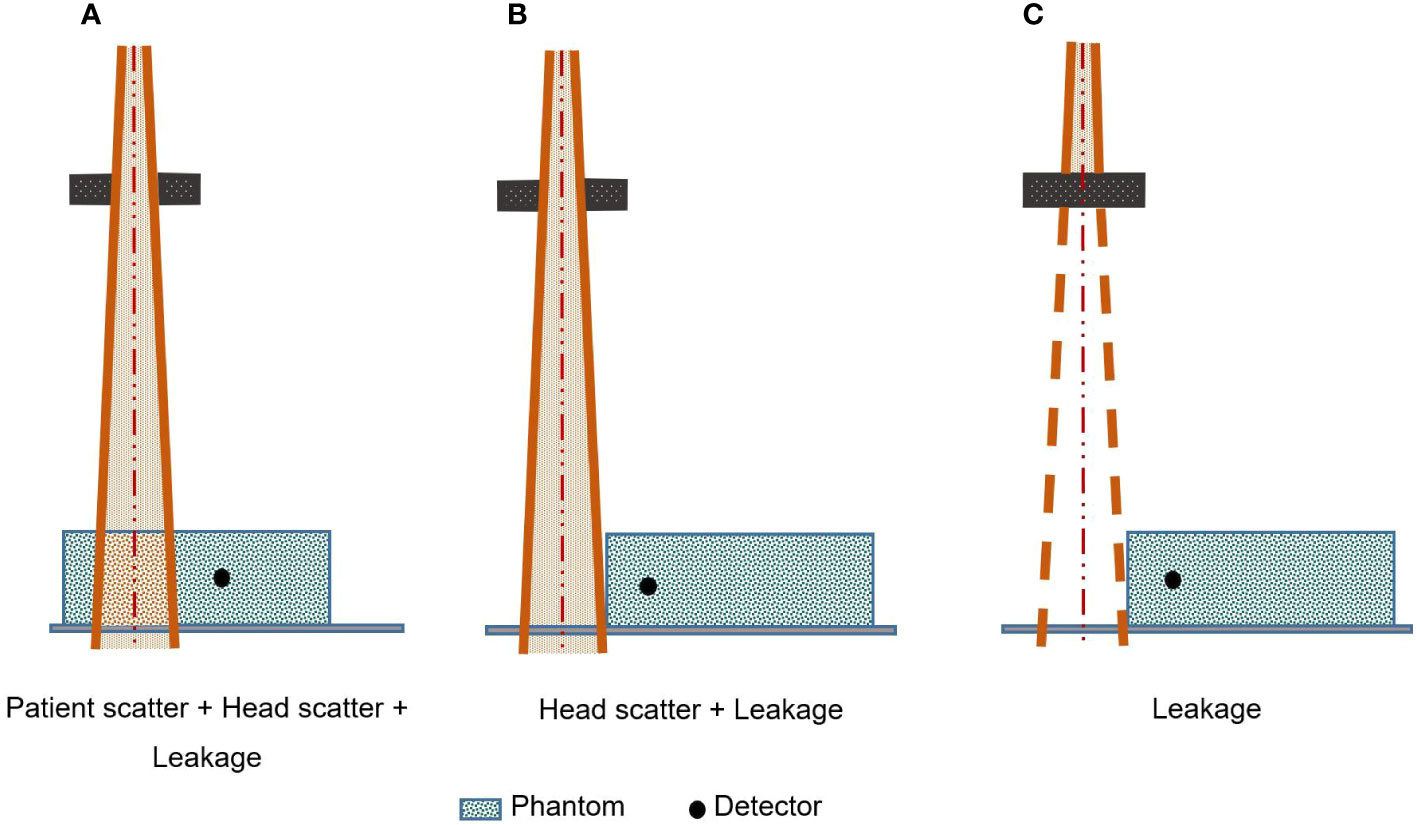
Figure 3 Kase’s experimental protocol in order to estimate different out-of-field-dose components separately [inspired from (23)].
3.4.1 General characteristics and model design
Semi-empirical models for out-of-field dose calculation are typically designed in the form of a two-stage mathematical formalism: an empirical description of the photon fluence based on a simplified representation of the treatment head is combined with a simplified physics theory regarding radiation and matter interaction to derive the absorbed dose distribution in the patient. In a more empirical approach, the Gustave Roussy’s group model (6) escapes any representation of the treatment head by choosing direct measurements of attenuation curves around the treatment beam with films to derive an extended empirical model of the spatial distribution of the incident photons fluence. This leads to account for head leakage and scatter, and even scatter from the treatment room as well, as a whole.
3.4.2 Describing head scatter
The spatial distribution of the photon fluence resulting from the treatment head scatter was modeled by assimilating either the treatment machine head with a virtual isotropic radiation point source (68), or with a combination of virtual plan sources (26, 60). In these two last papers, angular distribution of scattered photons was driven by the Henyey-Greenstein phase function (71) and photon energies followed the standard Compton scattering expressed by the Klein–Nishina formula (72, 73). Like in other models (66, 67), it was assumed that the primary photons were emanating from a virtual source located near the target with a spatial fluence distribution driven by the sum of several Gaussians. In contrast, an empirical formula was developed by the University of Zurich group (26) assuming a field size-dependent virtual source for the collimator scattering located at the rear jaw. Alternatively, a group from Louisiana State University and Agricultural and Mechanical College (55) reported another descriptive analytical formula accounting for the dependence of the head scatter upon beam energy, depth, and field size, through a combination of linear and exponential functions.
3.4.3 Describing leakage
The most sophisticated mathematical formalisms to derive the leakage component (66, 67) address separately the transmission through the primary collimator, the flattening filter, the secondary collimator, the jaws and the MLC, taking into account the geometrical and physical characteristics of these elements, through an exponential decrease. In an extensive study of the leakage component, a model used a graphics library and 3D rendering to model the linear accelerator shielding elements and accelerating waveguide, and implementing the build-up factor corrected by the exponential attenuation (59). However, most of the leakage models were greatly simplified as it has been modeled either by a constant background dose (68) or as originating from a field size independent virtual source at the target location (26, 60). An alternative approach considered that the leakage was attenuated by the secondary collimator close to the primary beam and additionally by the primary collimator in distant regions (55).
For instance, reference (68) modeled the head scatter and leakage components as a whole as follows:
With the peripheral dose per machine unit (MU) due to leakage and head scattered photons, that depends on the distance to the treatment isocenter (), depth (), field size (f), and which is a correction factor for treatment efficiency that takes into account the differences of MU when using a modulated treatment compared to a reference treatment for the same delivered dose. represents a correction factor for field sizes. represents the leakage component, and is an adjustment parameter. and are respectively the linear attenuation coefficients in air and tissues, while and being respectively the distance travelled in tissue or air.
3.4.4 Describing patient scatter
To model patient scatter, diverse options were considered: formula combining the Klein-Nishina coefficients for Compton scattering, the inverse square law and attenuation factors (74) and annihilation photons (75). Some authors assumed a virtual circular source of photons located on the beam central axis and consisting of infinitely small sources. The contributions from each infinitely small source are attenuated exponentially and the inverse square law is applied (26). Similarly, a virtual point source combined with transmission factors in water (66) or a single exponential component (76) were assumed to describe patient scatter. Another alternative was an empirical expression implementing different beam energy- and depth-dependent scaling factors to adjust the transmission and attenuation for radiation from patient scattering (55). Some authors have even chosen to neglect the patient scatter dose and have therefore limited the range of validity of their model to the volumes beyond 10 cm from the field edge (68), which present important limitations, especially for treatments with large fields, where patient scatter can have a major contribution well beyond 10 cm (23, 77). Let us illustrate this representation with (74) which analytically modeled the patient scatter component of the out-of-field dose as follows:
With the patient scattering component from at point , the Klein-Nishina coefficient, the inverse square law corresponding to the distance , the attenuation coefficient, the photon fluence at point , the energy of scattered photons and the mass energy absorption coefficient.
3.4.5 Describing secondary neutrons contribution
Authors studying out-of-field doses for beam energies greater than 10 MV systematically mention the existence of photoneutrons but consider that the equivalent dose from photoneutrons is negligible compared to that generated by photons. Particular attention should however be given to the results of the University of Seville group (78) which reported neutron equivalent doses obtained on 1377 adult patients in more than 30 different institutions using a digital neutron detector located inside the treatment room (79). The research team pointed out that although the neutron dose contribution inside the treatment field was negligible, it contributed to the total dose outside the field by about 25%, with this value decreasing rapidly with depth. Beyond 50 cm from the treatment field, the neutron dose is of the same order of magnitude as the leakage (43). Thus, neutron contribution should not be neglected, especially far away from the treatment field (43, 80, 81). The amount of neutrons produced has been shown to correlate with the complexity of the linac head, e.g., the presence of jaws and MLC (80), and with the number of MU (81).
However, we identified models in which neutrons were not taken into account in spite of energies used greater than or equal to 10 MV (25, 55) and only one paper provided an analytical model for the neutron component. In this aim, the University of Zurich (43) assumed a point source of neutrons located in the target and converted the fluence to a neutron equivalent dose through the Siebert and Schumacher quality factors (82).
3.5 Model performance evaluation and inter-comparability
Our investigation revealed that several factors make quantitative comparisons of the performance of the reported analytical models impossible.
First, the definition of out-of-field dose depends on the authors. The following definitions were reported:
- Doses below 5% of the prescribed dose (13, 19, 57, 67, 83),
- Doses below 50% of the prescribed dose (20, 53, 64).
- An alternative approach consisted in excluding all voxels where the TPS calculated dose was above 50% of the prescribed dose, and within the beam path and considering all remaining locations as out-of-field (63).
- In addition, some authors (43) defined the measurement points locations for model development or evaluation according to specific recommendations (84).
Our investigation also revealed that dose reporting rules depended on the research group, with measurements normalized in different ways. For instance, doses relative to the maximum central axis dose (60), or relative to the prescribed dose (53) have been reported depending on the studies.
Finally, model performances were assessed and reported in many ways, i.e., using:
- the root mean square deviation (RMSD) (20, 53, 61, 64, 66, 68),
- the mean, maximum or median differences both absolute and relative (6, 25, 26, 43, 55, 60, 66, 74, 75, 85),
- a generalized gamma index including an additional parameter for the low dose regions (87) was preferred in several studies (55, 63, 66, 67).
This observation makes it very difficult to compare the performance of the models, especially as this performance is quantified by comparing predictions with measurements, for which the number of experimental points and the position of the detectors vary drastically from one study to another.
Our investigation showed that TLDs were the most widely used dosimeters for assessing model performance through anthropomorphic phantom measurements (Table 1) in spite of their limitations. For instance,TLD-100s associated with high voltages superior to 15 MV (88), can overrespond by 4% to 12%, and correction factors are required (89).
3.6 Model versatility
A series of limitations related to model versatility have been identified by the authors themselves. Among these, extensive out-of-field dose measurements required for model implementation are technically demanding and laborious. Inclusion of neutron contribution is possible but nontrivial and at the cost of much more demanding measurements (76). Nevertheless, an out-of-field dose calculation model initially developed for static radiotherapy and IMRT with a 6 MV photon beam (26) has been successfully improved and adapted to incorporate a neutron equivalent dose component through additional measurements at 15 MV (43). A broadly applicable method was developed by generalizing an existing physics-based method, in which the model may be adapted for a large variety of devices without using proprietary configuration parameters, but with easily accessible dosimetric data (55). It appears to be a strong argument showing the relevance of future research towards a universally applicable model for estimating the out-of-field dose. Our analysis, however, evidenced that, the more a model is fitted to heterogeneous data, i.e., from different accelerators, or corresponding to different energies or irradiation techniques, the worse the performance will be. For instance, the generalization of a model initially developed from data obtained with a 60Co machine (74) to irradiation configurations from 6 MV, 10 MV and 23 MV linear accelerators (75) has resulted to a 20% loss of accuracy.
3.7 Clinical translation ability
As shown in Table 2, we found as expected that the further we go in time, the more frequent are the authors who claimed that their model would be suitable for complex radiotherapy techniques, in particular IMRT and VMAT. A total of 8 models are reported to be compatible with modern radiotherapy techniques (20, 26, 43, 55, 57, 60, 64, 68). Among these, clinical examples were reported for all but (60), because this last was restricted to the modeling of the MLC system. We can also notice that devices such as CyberKnife, Gamma Knife (Elekta Instruments, Stockholm, Sweden), TomoTherapy unit, or Halcyon (Varian Medical Systems, Palo Alto, USA) have been little used for the realization of measurements in the context of the development of analytical models (see Table 2). Nevertheless, it should be noted that some publications have addressed the assessment of out-of-field dose from an experimental point of view for the Halcyon device (15), for the Gamma Knife (90), or for CyberKnife and TomoTherapy devices (22). Several groups have developed bridging techniques with hybrid approaches using TPS-estimated doses for the in-field dose and analytical models for the out-of-field dose to obtain a whole body dose estimate (26, 43, 53, 61, 63, 65). Regarding the computation time, which is a critical parameter for clinical transfer, a few authors presented clear values. Reported computation times were 8 hours and 10 minutes per patient on a single CPU or a 64-core workstation (61), and four minutes (66) or 9 minutes per field (26).
4 Discussion
The aim of this exploratory research was to examine, through the available scientific publications, the key concepts underlying the analytical models dedicated to out-of-field dose calculation in external photon radiotherapy and to summarize the current state of the art in this field. Our work provides an overview of the typology of existing models, the extent of available experimental data and the knowledge to date.
First, existing analytical models for out-of-field dose calculations fall into two categories. Single-compartment models include all out-of-field dose components into a single general empirical mathematical formula. In contrast, multi-compartment models separate patient scatter from collimator scatter and leakage. Fourteen (almost 67%) out of the 21 selected articles reported multi-compartment models, showing that research efforts are directed towards an increasingly detailed description of the underlying physical phenomena. We have identified remarkable efforts to model the out-of-field dose component related to the photons scattering on the treatment beam collimating system (60), transmission and leakage through the beam limiting device (67) and also scattering in the patient (26).
Unfortunately, there is a lack of homogeneity in the definitions of some basic concepts, in particular the definition of the out-of-field dose itself. This, together with the lack of homogeneity in the normalization processes and the metrics used to present the results, makes it impossible to quantitatively compare model performance. It is therefore difficult to identify methods that are more efficient than others. Nevertheless, the synthesis that we provided in the paragraph devoted to general concepts and definitions are a step in encouraging the different research teams involved in this research field to move towards common practices. The practices that stand out the most could be accepted as the standard approach - such as the definition of the out-of-field as the dose below the 5% isodose, or the RMSD as the conventional performance evaluation metric. Of note, the recommendation for evaluating the dose to the RVR (29) is also an important step towards the harmonization of the practices. In addition, we note that the uncertainties related to the measurement processes allowing the fit of the analytical methods were not described in the analyzed publications, which makes it difficult to assess their accuracy. In (91), it was clearly stated however that one of the main sources of uncertainty in the estimation of the out-of-field dose comes from the measurements themselves. Indeed, these uncertainties are known to be higher than in-field ones, due to the unknown photon spectra. The maximum overall uncertainty in out-of-field dose measurements has been reported to be about 15% by authors using TLDs, ionization chambers, and radiophotoluminescent dosimeters (92). The creation of an international working group to provide guidelines regarding good practices would allow an harmonization of reported results, necessary for a more widespread use of this research topic in clinical practice. Let us note the Working Group 9 (WG9 - Radiation dosimetry in radiotherapy) of the European Radiation Dosimetry Group, which is already interested in out-of-field doses in brachytherapy.
Finally, the problems of versatility of most of the analytical methods, and the cumbersome nature of their implementation, is undoubtedly an obstacle to their widespread use in clinical routine, despite their obvious clinical interest and the fact that UNSCEAR emphasized the need for a systematic assessment of out-of-field doses in relation to second primary cancer after radiotherapy during its 69th session in 2022. The new possibilities offered by artificial intelligence methods, that are already revolutionizing various fields in radiotherapy planning (93–95), could be an interesting avenue to overcome this drawback. Neural Network-based models (NNs) have proven good performance in solving complex tasks, for various applications in medical physics, such as automatic segmentation (96), automatic planning (97) or the generation of virtual images (98), but, to our knowledge, there is currently no NNs developed for out-of-field dose calculation, although they have already proven their ability in estimating the in-field dose (95, 99–103). It should be noted, however, that the current lack of a publicly available dataset large enough and versatile enough to properly train a neural network may be a serious obstacle that will be difficult to overcome.
While there have been a number of interesting reviews published on similar topics in the past, it’s worth noting that our paper takes a unique approach and offers a fresh perspective. For instance, the work of (48) gave an almost exhaustive overview of the applications of the available methods for dose reconstructions for therapeutic and diagnostic exposures for use in retrospective epidemiological studies. This publication has of course examined all the outstanding analytical models used before 2006 for dosimetry in retrospective epidemiological studies (47). provided a slightly more recent overview on dosimetry for second cancers studies, while (46) analyzed the main contributing factors to out-of-field doses, including linear accelerator type, field size, beam quality, leakage, collimator scatter, treatment technique, and their clinical implications, with the aim of highlighting ways to reduce the risk of associated radiation-induced cancers. Even more recently, a review presenting existing data from measurements and calculations of out-of-field doses in external photon beam radiotherapy and discussing its clinical implications has been published (45). Our research stands out as original due to its scoping review design. This approach complements and enriches the existing scientific literature by providing up-to-date, and specific information on all published mathematical models. This information is crucial for designing future research that aims to develop a universally applicable software package for out-of-field dose calculations usable in clinical practice.
5 Conclusion
In this scoping review, we have comprehensively presented the published articles on analytical models for out-of-field dose calculation in photon external radiotherapy and highlighted the remarkable efforts that have been made in the field. Through this work, we have also highlighted some of the pitfalls that currently hinder their widespread use in clinical workflow and the need for standardization in order to simplify comparisons. In a clinical context where modulated irradiation is becoming the standard of care and where combination treatments suggest that doses received by healthy organs located at a distance from the irradiation field may play a key role, efforts must be made to find solutions versatile enough to be compatible with clinical practice. The neural network approach could be a relevant candidate provided that an adequate data set is available.
Author contributions
NB collected the data, analyzed publications, drafted the figures and table, and wrote the manuscript. SA and FdK gave targeted expertise. CR, ID, and JC helped with thematic expertise and for the publication structure. CR and ID helped with the general writing and the structure of the document and gave final approval of the submitted version. All authors contributed to the article and approved the submitted version.
Funding
This work has benefited from a French government grant managed by the National Research Agency (ANR) and integrated into the France 2030 program with the reference ANR-21-RHUS-0005.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Chargari C, Soria JC, Deutsch E. Controversies and challenges regarding the impact of radiation therapy on survival. Ann Oncol (2013) 24(1):38–46. doi: 10.1093/annonc/mds217
2. Mukesh MB, Barnett GC, Wilkinson JS, Moody AM, Wilson C, Dorling L, et al. Randomized controlled trial of intensity-modulated radiotherapy for early breast cancer: 5-year results confirm superior overall cosmesis. J Clin Oncol (2013) 31(36):4488–95. doi: 10.1200/JCO.2013.49.7842
3. Arnold M, Rutherford MJ, Bardot A, Ferlay J, Andersson TML, Myklebust TÅ, et al. Progress in cancer survival, mortality, and incidence in seven high-income countries 1995-2014 (ICBP SURVMARK-2): a population-based study. Lancet Oncol (2019) 20(11):1493–505. doi: 10.1016/S1470-2045(19)30456-5
4. Geraci JP, Jackson KL, Mariano MS. An estimate of the radiation-induced cancer risk from the whole-body stray radiation exposure in neutron radiotherapy. Eur J Cancer Clin Oncol (1982) 18(11):1187–95. doi: 10.1016/0277-5379(82)90101-8
5. de Vathaire F, Hawkins M, Campbell S, Oberlin O, Raquin MA, Schlienger JY, et al. Second malignant neoplasms after a first cancer in childhood: temporal pattern of risk according to type of treatment. Br J Cancer. (1999) 79(11–12):1884–93. doi: 10.1038/sj.bjc.6690300
6. Diallo I, Lamon A, Shamsaldin A, Grimaud E, de Vathaire F, Chavaudra J. Estimation of the radiation dose delivered to any point outside the target volume per patient treated with external beam radiotherapy. Radiother Oncol (1996) 38(3):269–71. doi: 10.1016/0167-8140(96)01713-6
7. Francois P, Beurtheret C, Dutreix A, De Vathaire F. A mathematical child phantom for the calculation of dose to the organs at risk. Med Phys (1988) 15(3):328–33. doi: 10.1118/1.596226
8. Stovall M, Smith SA, Rosenstein M. Tissue doses from radiotherapy of cancer of the uterine cervix. Med Phys (1989) 16(5):726–33. doi: 10.1118/1.596331
9. Hall EJ, Wuu CS. Radiation-induced second cancers: the impact of 3D-CRT and IMRT. Int J Radiat Oncol Biol Phys (2003) 56(1):83–8. doi: 10.1016/S0360-3016(03)00073-7
10. Tao Y, Lefkopoulos D, Ibrahima D, Bridier A, Polizzi MDP, Wibault P, et al. Comparison of dose contribution to normal pelvic tissues among conventional, conformal and intensity-modulated radiotherapy techniques in prostate cancer. Acta Oncol (2008) 47(3):442–50. doi: 10.1080/02841860701666055
11. Miller KD, Nogueira L, Mariotto AB, Rowland JH, Yabroff KR, Alfano CM, et al. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin (2019) 69(5):363–85. doi: 10.3322/caac.21565
12. Phillips SM, Padgett LS, Leisenring WM, Stratton KK, Bishop K, Krull KR, et al. Survivors of childhood cancer in the united states: prevalence and burden of morbidity. Cancer Epidemiol Biomarkers Prev (2015) 24(4):653–63. doi: 10.1158/1055-9965.EPI-14-1418
13. Howell RM, Scarboro SB, Kry SF, Yaldo DZ. Accuracy of out-of-field dose calculations by a commercial treatment planning system. Phys Med Biol (2010) 55(23):6999–7008. doi: 10.1088/0031-9155/55/23/S03
14. Shine NS, Paramu R, Gopinath M, Jaon Bos RC, Jayadevan PM. Out-of-Field dose calculation by a commercial treatment planning system and comparison by Monte Carlo simulation for Varian TrueBeam®. J Med Phys (2019) 44(3):156–75. doi: 10.4103/jmp.JMP_82_18
15. Colnot J, Zefkili S, Gschwind R, Huet C. Out-of-field doses from radiotherapy using photon beams: a comparative study for a pediatric renal treatment. J Appl Clin Med Phys (2021) 22(3):94–106. doi: 10.1002/acm2.13182
16. Huang JY, Followill DS, Wang XA, Kry SF. Accuracy and sources of error of out-of field dose calculations by a commercial treatment planning system for intensity-modulated radiation therapy treatments. J Appl Clin Med Phys (2013) 14(2):4139. doi: 10.1120/jacmp.v14i2.4139
17. Joosten A, Matzinger O, Jeanneret-Sozzi W, Bochud F, Moeckli R. Evaluation of organ-specific peripheral doses after 2-dimensional, 3-dimensional and hybrid intensity modulated radiation therapy for breast cancer based on Monte Carlo and convolution/superposition algorithms: implications for secondary cancer risk assessment. Radiother Oncol (2013) 106(1):33–41. doi: 10.1016/j.radonc.2012.11.012
18. Sánchez-Nieto B, Medina-Ascanio KN, Rodríguez-Mongua JL, Doerner E, Espinoza I. Study of out-of-field dose in photon radiotherapy: a commercial treatment planning system versus measurements and Monte Carlo simulations. Med Phys (2020) 47(9):4616–25. doi: 10.1002/mp.14356
19. Wang L, Ding GX. The accuracy of the out-of-field dose calculations using a model based algorithm in a commercial treatment planning system. Phys Med Biol (2014) 59(13):N113–128. doi: 10.1088/0031-9155/59/13/N113
20. Yoon J, Heins D, Zhao X, Sanders M, Zhang R. Measurement and modeling of out-of-field doses from various advanced post-mastectomy radiotherapy techniques. Phys Med Biol (2017) 62(23):9039–53. doi: 10.1088/1361-6560/aa94b5
21. Colnot J, Barraux V, Loiseau C, Berejny P, Batalla A, Gschwind R, et al. A new Monte Carlo model of a cyberknife® system for the precise determination of out-of-field doses. Phys Med Biol (2019) 64(19):195008. doi: 10.1088/1361-6560/ab38e5
22. Schneider U, Hälg RA, Hartmann M, Mack A, Storelli F, Joosten A, et al. Accuracy of out-of-field dose calculation of tomotherapy and cyberknife treatment planning systems: a dosimetric study. Z Med Phys (2014) 24(3):211–5. doi: 10.1016/j.zemedi.2013.10.008
23. Kase KR, Svensson GK, Wolbarst AB, Marks MA. Measurements of dose from secondary radiation outside a treatment field. Int J Radiat Oncol Biol Phys (1983) 9(8):1177–83. doi: 10.1016/0360-3016(83)90177-3
24. Stovall M, Blackwell CR, Cundiff J, Novack DH, Palta JR, Wagner LK, et al. Fetal dose from radiotherapy with photon beams: report of AAPM radiation therapy committee task group no. 36. Med Phys (1995) 22(1):63–82. doi: 10.1118/1.597525
25. Francois P, Beurtheret C, Dutreix A. Calculation of the dose delivered to organs outside the radiation beams. Med Phys (1988) 15(6):879–83. doi: 10.1118/1.596170
26. Hauri P, Hälg RA, Besserer J, Schneider U. A general model for stray dose calculation of static and intensity-modulated photon radiation. Med Phys (2016) 43(4):1955. doi: 10.1118/1.4944421
27. De Saint-Hubert M, Suesselbeck F, Vasi F, Stuckmann F, Rodriguez M, Dabin J, et al. Experimental validation of an analytical program and a Monte Carlo simulation for the computation of the far out-of-Field dose in external beam photon therapy applied to pediatric patients. Front Oncol (2022) 12:882506. doi: 10.3389/fonc.2022.882506
28. Kry SF, Titt U, Followill D, Pönisch F, Vassiliev ON, White RA, et al. A Monte Carlo model for out-of-field dose calculation from high-energy photon therapy. Med Phys (2007) 34(9):3489–99. doi: 10.1118/1.2756940
29. Prescribing, recording, and reporting photon-beam intensity-modulated radiation therapy (IMRT). (2010) 10(1):1–3. doi: 10.1093/jicru/ndq002
30. Heylmann D, Ponath V, Kindler T, Kaina B. Comparison of DNA repair and radiosensitivity of different blood cell populations. Sci Rep (2021) 11(1):2478. doi: 10.1038/s41598-021-81058-1
31. Nakamura N, Kusunoki Y, Akiyama M. Radiosensitivity of CD4 or CD8 positive human T-lymphocytes by an in vitro colony formation assay. Radiat Res (1990) 123(2):224–7. doi: 10.2307/3577549
32. Cai S, Fan Y, Guo Q, Sun Y, Zhao P, Tian Y, et al. Impact of radiation dose to circulating immune cells on tumor control and survival in esophageal cancer. Cancer Biother Radiopharm (2021). doi: 10.1089/cbr.2021.0250
33. Lambin P, Lieverse RIY, Eckert F, Marcus D, Oberije C, van der Wiel AMA, et al. Lymphocyte-sparing radiotherapy: the rationale for protecting lymphocyte-rich organs when combining radiotherapy with immunotherapy. Semin Radiat Oncol (2020) 30(2):187–93. doi: 10.1016/j.semradonc.2019.12.003
34. Terrones-Campos C, Ledergerber B, Vogelius IR, Helleberg M, Specht L, Lundgren J. Hematological toxicity in patients with solid malignant tumors treated with radiation - temporal analysis, dose response and impact on survival. Radiother Oncol (2021) 158:175–83. doi: 10.1016/j.radonc.2021.02.029
35. Abravan A, Eide HA, Helland Å, Malinen E. Radiotherapy-related lymphopenia in patients with advanced non-small cell lung cancer receiving palliative radiotherapy. Clin Transl Radiat Oncol (2020) 22:15–21. doi: 10.1016/j.ctro.2020.02.005
36. Damen PJJ, Kroese TE, van Hillegersberg R, Schuit E, Peters M, Verhoeff JJC, et al. The influence of severe radiation-induced lymphopenia on overall survival in solid tumors: a systematic review and meta-analysis. Int J Radiat Oncol Biol Phys (2021) 111(4):936–48. doi: 10.1016/j.ijrobp.2021.07.1695
37. Davuluri R, Jiang W, Fang P, Xu C, Komaki R, Gomez DR, et al. Lymphocyte nadir and esophageal cancer survival outcomes after chemoradiation therapy. Int J Radiat Oncol Biol Phys (2017) 99(1):128–35. doi: 10.1016/j.ijrobp.2017.05.037
38. Venkatesulu BP, Mallick S, Lin SH, Krishnan S. A systematic review of the influence of radiation-induced lymphopenia on survival outcomes in solid tumors. Crit Rev Oncol Hematol (2018) 123:42–51. doi: 10.1016/j.critrevonc.2018.01.003
39. Dawood A, Mothersill C, Seymour C. Low dose ionizing radiation and the immune response: what is the role of non-targeted effects? Int J Radiat Biol (2021) 97(10):1368–82. doi: 10.1080/09553002.2021.1962572
40. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol (2018) 18(1):143. doi: 10.1186/s12874-018-0611-x
41. Pollock D, Peters MDJ, Khalil H, McInerney P, Alexander L, Tricco AC, et al. Recommendations for the extraction, analysis, and presentation of results in scoping reviews. JBI Evidence Synthesis (2022) 21(3):520. doi: 10.11124/JBIES
42. Clarkson JR. A note on depth doses in fields of irregular shape. BJR (1941) 14(164):265–8. doi: 10.1259/0007-1285-14-164-265
43. Hauri P, Schneider U. Whole-body dose equivalent including neutrons is similar for 6 MV and 15 MV IMRT, VMAT, and 3D conformal radiotherapy. J Appl Clin Med Phys (2019) 20(3):56–70. doi: 10.1002/acm2.12543
44. Vega C HR, Martinez O SA, Benites R JL, Lallena AM. Photon and photoneutron spectra produced in radiotherapy linacs . Available at: http://inis.iaea.org/Search/search.aspx?orig_q=RN:43009454.
45. Newhauser WD, Schneider C, Wilson L, Shrestha S, Donahue W. A review of analytical models of stray radiation exposures from photon and proton beam radiotherapies. Radiat Prot Dosimetry (2018) 180(1–4):245–51. doi: 10.1093/rpd/ncx245
46. Taylor ML, Kron T. Consideration of the radiation dose delivered away from the treatment field to patients in radiotherapy. J Med Phys (2011) 36(2):59–71. doi: 10.4103/0971-6203.79686
47. Xu XG, Bednarz B, Paganetti H. A review of dosimetry studies on external-beam radiation treatment with respect to second cancer induction. Phys Med Biol (2008) 53(13):R193–241. doi: 10.1088/0031-9155/53/13/R01
48. Stovall M, Weathers R, Kasper C, Smith SA, Travis L, Ron E, et al. Dose reconstruction for therapeutic and diagnostic radiation exposures: use in epidemiological studies. Radiat Res (2006) 166(1 Pt 2):141–57. doi: 10.1667/RR3525.1
49. Chen Z, Dominello MM, Joiner MC, Burmeister JW. Proton versus photon radiation therapy: a clinical review. Front Oncol (2023) 13:1133909. doi: 10.3389/fonc.2023.1133909
50. De Saint-Hubert M, Verbeek N, Bäumer C, Esser J, Wulff J, Nabha R, et al. Validation of a Monte Carlo framework for out-of-Field dose calculations in proton therapy. Front Oncol (2022) 12:882489. doi: 10.3389/fonc.2022.882489
51. Cravo Sá A, Barateiro A, Bednarz B, Borges C, Pereira J, Baptista M, et al. Assessment of out-of-field doses in radiotherapy treatments of paediatric patients using Monte Carlo methods and measurements. Phys Med (2020) 71:53–61. doi: 10.1016/j.ejmp.2020.02.008
52. Miljanić S, Bordy JM, d’Errico F, Harrison R, Olko P. Out-of-field dose measurements in radiotherapy – an overview of activity of EURADOS working group 9: radiation protection in medicine. Radiat Measure (2014) 71:270–5. doi: 10.1016/j.radmeas.2014.04.026
53. Taddei PJ, Jalbout W, Howell RM, Khater N, Geara F, Homann K, et al. Analytical model for out-of-field dose in photon craniospinal irradiation. Phys Med Biol (2013) 58(21):7463–79. doi: 10.1088/0031-9155/58/21/7463
54. Hauri P, Schneider U. Whole-body dose and energy measurements in radiotherapy by a combination of LiF : Mg,Cu,P and LiF : Mg,Ti. Z Med Phys (2018) 28(2):96–109. doi: 10.1016/j.zemedi.2017.07.002
55. Schneider CW, Newhauser WD, Wilson LJ, Schneider U, Kaderka R, Miljanić S, et al. A descriptive and broadly applicable model of therapeutic and stray absorbed dose from 6 to 25 MV photon beams. Med Phys (2017) 44(7):3805–14. doi: 10.1002/mp.12286
56. Gilbert JK, Boulter CJ. Learning science through models and modelling. In: International handbook of science education. London: Kluwer Academic (1998). p. 53–6. Available at: https://link.springer.com/book/9780792335313.
57. Sánchez-Nieto B, López-Martínez IN, Rodríguez-Mongua JL, Espinoza I. A simple analytical model for a fast 3D assessment of peripheral photon dose during coplanar isocentric photon radiotherapy. Front Oncol (2022) 12:872752. doi: 10.3389/fonc.2022.872752
58. Halg RA, Besserer J, Schneider U. Systematic measurements of whole-body dose distributions for various treatment machines and delivery techniques in radiation therapy. Med Phys (2012) 39(12):7662–76. doi: 10.1118/1.4767773
59. Bezin JV, Veres A, Lefkopoulos D, Chavaudra J, Deutsch E, de Vathaire F, et al. Field size dependent mapping of medical linear accelerator radiation leakage. Phys Med Biol (2015) 60(5):2103–6. doi: 10.1088/0031-9155/60/5/2103
60. Benadjaoud MA, Bezin J, Veres A, Lefkopoulos D, Chavaudra J, Bridier A, et al. A multi-plane source model for out-of-field head scatter dose calculations in external beam photon therapy. Phys Med Biol (2012) 57(22):7725–39. doi: 10.1088/0031-9155/57/22/7725
61. Gallagher KJ, Tannous J, Nabha R, Feghali JA, Ayoub Z, Jalbout W, et al. Supplemental computational phantoms to estimate out-of-field absorbed dose in photon radiotherapy. Phys Med Biol (2018) 63(2):025021. doi: 10.1088/1361-6560/aa9838
62. van der Giessen PH. Peridose, a software program to calculate the dose outside the primary beam in radiation therapy. Radiother Oncol (2001) 58(2):209–13. doi: 10.1016/S0167-8140(00)00326-1
63. Wilson LJ, Newhauser WD, Schneider CW, Kamp F, Reiner M, Martins JC, et al. Method to quickly and accurately calculate absorbed dose from therapeutic and stray photon exposures throughout the entire body in individual patients. Med Phys (2020) 47(5):2254–66. doi: 10.1002/mp.14018
64. De Saint-Hubert M, Verellen D, Poels K, Crijns W, Magliona F, Depuydt T, et al. Out-of-field doses from pediatric craniospinal irradiations using 3D-CRT, IMRT, helical tomotherapy and electron-based therapy. Phys Med Biol (2017) 62(13):5293–311. doi: 10.1088/1361-6560/aa6c9e
65. Veres C, Allodji RS, Llanas D, Vu Bezin J, Chavaudra J, Mège JP, et al. Retrospective reconstructions of active bone marrow dose-volume histograms. Int J Radiat Oncol Biol Phys (2014) 90(5):1216–24. doi: 10.1016/j.ijrobp.2014.08.335
66. Jagetic LJ, Newhauser WD. A simple and fast physics-based analytical method to calculate therapeutic and stray doses from external beam, megavoltage x-ray therapy. Phys Med Biol (2015) 60(12):4753–75. doi: 10.1088/0031-9155/60/12/4753
67. Schneider CW, Newhauser WD, Wilson LJ, Kapsch RP. A physics-based analytical model of absorbed dose from primary, leakage, and scattered photons from megavoltage radiotherapy with MLCs. Phys Med Biol (2019) 64(18):185017. doi: 10.1088/1361-6560/ab303a
68. Sanchez B, El-Far R, Irazola L, Romero-Expósito M, Lagares JI, Mateos J, et al. Analytical model for photon peripheral dose estimation in radiotherapy treatments analytical model for photon peripheral dose estimation in radiotherapy treatments. Biomed Phys Eng Express. (2015) 1:045205. doi: 10.1088/2057-1976/1/4/045205
69. Cunningham JR. Scatter-air ratios. Phys Med Biol (1972) 17(1):42–51. doi: 10.1088/0031-9155/17/1/005
70. Zhang Z, PA A, Jd F, Pj T, Wd N. An analytic model of neutron ambient dose equivalent and equivalent dose for proton radiotherapy. Phys Med Biol (2010) 55(23):6975. doi: 10.1088/0031-9155/55/23/S01
71. Henyey LG, Greenstein JL. Diffuse radiation in the galaxy. Astrophys J (1941) 93:70–83. doi: 10.1086/144246
72. Compton AH. A quantum theory of the scattering of X-rays by light elements. Phys Rev (1923) 21(5):483–502. doi: 10.1103/PhysRev.21.483
73. Klein O, Nishina Y. Über die streuung von strahlung durch freie elektronen nach der neuen relativistischen quantendynamik von Dirac. Z Physik. (1929) 52(11):853–68. doi: 10.1007/BF01366453
74. van der Giessen PH, Hurkmans CW. Calculation and measurement of the dose to points outside the primary beam for CO-60 gamma radiation. Int J Radiat Oncol Biol Phys (1993) 27(3):717–24. doi: 10.1016/0360-3016(93)90401-G
75. van der Giessen PH. Calculation and measurement of the dose at points outside the primary beam for photon energies of 6, 10, and 23 MV. Int J Radiat Oncol Biol Phys (1994) 30(5):1239–46. doi: 10.1016/0360-3016(94)90335-2
76. McParland BJ, Fair HI. A method of calculating peripheral dose distributions of photon beams below 10 MV. Med Phys (1992) 19(2):283–93. doi: 10.1118/1.596858
77. Sherazi S, Kase KR. Measurements of dose from secondary radiation outside a treatment field: effects of wedges and blocks. Int J Radiat Oncol Biol Phys (1985) 11(12):2171–6. doi: 10.1016/0360-3016(85)90100-2
78. Expósito MR, Sánchez-Nieto B, Terrón JA, Domingo C, Gómez F, Sánchez-Doblado F. Neutron contamination in radiotherapy: estimation of second cancers based on measurements in 1377 patients. Radiother Oncol (2013) 107(2):234–41. doi: 10.1016/j.radonc.2013.03.011
79. Nath R, Epp ER, Laughlin JS, Swanson WP, Bond VP. Neutrons from high-energy x-ray medical accelerators: an estimate of risk to the radiotherapy patient. Med Phys (1984) 11(3):231–41. doi: 10.1118/1.595497
80. Biltekin F, Yeginer M, Ozyigit G. Investigating in-field and out-of-field neutron contamination in high-energy medical linear accelerators based on the treatment factors of field size, depth, beam modifiers, and beam type. Phys Med (2015) 31(5):517–23. doi: 10.1016/j.ejmp.2015.03.015
81. Kaderka R, Schardt D, Durante M, Berger T, Ramm U, Licher J, et al. Out-of-field dose measurements in a water phantom using different radiotherapy modalities. Phys Med Biol (2012) 57(16):5059–74. doi: 10.1088/0031-9155/57/16/5059
82. Siebert BRL, Schuhmacher H. Quality factors, ambient and personal dose equivalent for neutrons, based on the new ICRU stopping power data for protons and alpha particles. Radiat Prot Dosimetry (1995) 58(3):177–83. doi: 10.1093/oxfordjournals.rpd.a082612
83. Almberg SS, Frengen J, Lindmo T. Monte Carlo Study of in-field and out-of-field dose distributions from a linear accelerator operating with and without a flattening-filter. Med Phys (2012) 39(8):5194–203. doi: 10.1118/1.4738963
84. Wrixon AD. New ICRP recommendations. J Radiol Prot (2008) 28(2):161–8. doi: 10.1088/0952-4746/28/2/R02
85. Van der Giessen PH. A simple and generally applicable method to estimate the peripheral dose in radiation teletherapy with high energy x-rays or gamma radiation. Int J Radiat Oncol Biol Phys (1996) 35(5):1059–68. doi: 10.1016/0360-3016(96)00254-4
86. Van der Giessen PH, Bierhuizen HW. Comparison of measured and calculated peripheral doses in patients undergoing radiation therapy. Radiother Oncol (1997) 42(3):265–70. doi: 10.1016/S0167-8140(96)01885-3
87. Wilson LJ, Newhauser WD, Schneider CW. An objective method to evaluate radiation dose distributions varying by three orders of magnitude. Med Phys (2019) 46(4):1888–95. doi: 10.1002/mp.13420
88. Kry SF, Price M, Followill D, Mourtada F, Salehpour M. The use of LiF (TLD-100) as an out-of-field dosimeter. J Appl Clin Med Phys (2007) 8(4):169–75. doi: 10.1120/jacmp.v8i4.2679
89. Kry SF, Alvarez P, Cygler JE, DeWerd LA, Howell RM, Meeks S, et al. AAPM TG 191: clinical use of luminescent dosimeters: TLDs and OSLDs. Med Phys (2020) 47(2):e19–51. doi: 10.1002/mp.13839
90. De Saint-Hubert M, Majer M, Hršak H, Heinrich Z, Kneževic Ž, Miljanic S, et al. Out-of-field doses in children treated for large arteriovenous malformations using hypofractionated gamma knife radiosurgery and intensity-modulated radiation therapy. Radiat Prot Dosimetry (2018) 181(2):100–10. doi: 10.1093/rpd/ncx301
91. Vũ Bezin J, Allodji RS, Mège JP, Beldjoudi G, Saunier F, Chavaudra J, et al. A review of uncertainties in radiotherapy dose reconstruction and their impacts on dose-response relationships. J Radiol Prot (2017) 37(1):R1–18. doi: 10.1088/1361-6498/aa575d
92. Bordy JM, Bessieres I, d’Agostino E, Domingo C, d’Errico F, di Fulvio A, et al. Radiotherapy out-of-field dosimetry: experimental and computational results for photons in a water tank. Radiat Measure (2013) 57:29–34. doi: 10.1016/j.radmeas.2013.06.010
93. Biswas M, Kuppili V, Saba L, Edla DR, Suri HS, Cuadrado-Godia E, et al. State-of-the-art review on deep learning in medical imaging. Front Biosci (Landmark Ed). (2019) 24(3):392–426. doi: 10.2741/4725
94. Boldrini L, Bibault JE, Masciocchi C, Shen Y, Bittner MI. Deep learning: a review for the radiation oncologist. Front Oncol (2019) 9:977. doi: 10.3389/fonc.2019.00977
95. Kearney V, Chan JW, Haaf S, Descovich M, Solberg TD. DoseNet: a volumetric dose prediction algorithm using 3D fully-convolutional neural networks. Phys Med Biol (2018) 63(23):235022. doi: 10.1088/1361-6560/aaef74
96. Shi F, Hu W, Wu J, Han M, Wang J, Zhang W, et al. Deep learning empowered volume delineation of whole-body organs-at-risk for accelerated radiotherapy. Nat Commun (2022) 13(1):6566. doi: 10.1038/s41467-022-34257-x
97. McIntosh C, Conroy L, Tjong MC, Craig T, Bayley A, Catton C, et al. Clinical integration of machine learning for curative-intent radiation treatment of patients with prostate cancer. Nat Med (2021) 27(6):999–1005. doi: 10.1038/s41591-021-01359-w
98. Lerner M, Medin J, Jamtheim Gustafsson C, Alkner S, Olsson LE. Prospective clinical feasibility study for MRI-only brain radiotherapy. Front Oncol (2021) 11:812643. doi: 10.3389/fonc.2021.812643
99. Akhavanallaf A, Shiri I, Arabi H, Zaidi H. Whole-body voxel-based internal dosimetry using deep learning. Eur J Nucl Med Mol Imaging (2020) 48(3):670–82. doi: 10.1109/NSS/MIC42677.2020.9507983
100. Chen X, Men K, Li Y, Yi J, Dai J. A feasibility study on an automated method to generate patient-specific dose distributions for radiotherapy using deep learning. Med Phys (2019) 46(1):56–64. doi: 10.1002/mp.13262
101. Kontaxis C, Bol GH, Lagendijk JJW, Raaymakers BW. DeepDose: towards a fast dose calculation engine for radiation therapy using deep learning. Phys Med Biol (2020) 65(7):075013. doi: 10.1088/1361-6560/ab7630
102. Ma M, Buyyounouski M K, Vasudevan V, Xing L, Yang Y. Dose distribution prediction in isodose feature-preserving voxelization domain using deep convolutional neural network. Med Phys (2019) 46(7):2978–87. doi: 10.1002/mp.13618
Keywords: out-of-field dose, peripheral dose, whole-body dose, analytical models, external radiotherapy
Citation: Benzazon N, Colnot J, de Kermenguy F, Achkar S, de Vathaire F, Deutsch E, Robert C and Diallo I (2023) Analytical models for external photon beam radiotherapy out-of-field dose calculation: a scoping review. Front. Oncol. 13:1197079. doi: 10.3389/fonc.2023.1197079
Received: 30 March 2023; Accepted: 24 April 2023;
Published: 09 May 2023.
Edited by:
Humberto Rocha, University of Coimbra, PortugalReviewed by:
Raquel Bar-Deroma, Rambam Health Care Campus, IsraelJames C. L. Chow, University of Toronto, Canada
Copyright © 2023 Benzazon, Colnot, de Kermenguy, Achkar, de Vathaire, Deutsch, Robert and Diallo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nathan Benzazon, nathan.benzazon@gustaveroussy.fr; Ibrahima Diallo, ibrahim.diallo@gustaveroussy.fr
†These authors have contributed equally to this work and share last authorship