 Raphaële Renard-Penna1,2*
Raphaële Renard-Penna1,2* Jules Zhang-Yin3Sarah Montagne1,2Laurene Aupin1Eric Bruguière4
Jules Zhang-Yin3Sarah Montagne1,2Laurene Aupin1Eric Bruguière4 Mouna Labidi5Igor Latorzeff6Christophe Hennequin5
Mouna Labidi5Igor Latorzeff6Christophe Hennequin5- 1Academic Department of Radiology, Hôpital Pitié-Salpétrière, Assistance Publique des Hôpitaux de Paris, Paris, France
- 2Sorbonne University, Paris, France
- 3Nuclear Medicine Department, Tenon Hospital, Assistance Publique des Hôpitaux de Paris (APHP), Paris, France
- 4Department of Imaging, Clinique Pasteur, Toulouse, France
- 5Department of Oncology, Saint-Louis Hospital, Université de Paris, Assistance Publique des Hôpitaux de Paris, Paris, France
- 6Department of Radiotherapy, Clinique Pasteur, Toulouse, France
Magnetic resonance imaging (MRI) is being increasingly used for imaging suspected recurrence in prostate cancer therapy. Functional MRI with diffusion and perfusion imaging has the potential to demonstrate local recurrence even at low PSA value. Detection of recurrence can modify the management of postprostatectomy biochemical recurrence. MRI scan acquired before salvage radiotherapy is useful for the localization of recurrent tumors and also in the delineation of the target volume. The objective of this review is to assess the role and potential impact of MRI in targeting local recurrence after surgery for prostate cancer in the setting of salvage radiation therapy.
Highlights
● MRI can diagnose local prostate cancer recurrence after radical prostatectomy even at low PSA value.
● DWI-MR is almost comparable with DCE-MRI in detecting local recurrence.
● MRI enables a better delineation of identified recurrence and a precise anatomical analysis of the prostate bed than CT.
Introduction
Radical prostatectomy (RP) is a standard treatment for localized prostate cancer (PCa). Of 100 men treated with RP, approximatively 15–60 will develop biochemical recurrence (BCR) within 10 years (1, 2). The measurement of prostate-specific antigen (PSA) is a key component in follow-up after RP because of the so-called BCR which precedes clinical recurrence (3, 4). BCR is defined as PSA ≥0.2 ng/ml, followed by a second confirmatory serum PSA measurement of greater than or equal to 0.2 ng/ml (5). Commonly, BCR signed an early recurrent disease and include local recurrence (LR) in the prostate fossa as well as lymph node and/or bone metastases. The pattern of recurrence after RP is predominantly local (≈60%) with a relatively low incidence of metastatic failure (6).
Some clinico-pathological features and characteristics of PSA recurrence represent important variables when trying to distinguish between a local and distant recurrence. Indeed, Gleason score (GS) ≥8, seminal vesicle involvement, or pelvic lymph node (LN) invasion at the time of surgery seem to be correlated with distant recurrences. Similarly, a BCR occurring within 6 months of RP or a PSA doubling time of less than 12 months are strong indicators of metastases (7, 8). On the contrary, PSA increases of more than 3 years post-RP, PSA doubling time greater than 12 months, original Gleason score ≤7, pT3a stage (extracapsular extension without seminal vesicle infiltration), and positive surgical margins suggest that the relapse is more likely to be local (9–12).
The options for treatment of recurrence after RP are, according to the European Association of Urology (EAU), salvage radiotherapy (SRT) at least to the prostatic fossa, continuous or intermittent hormonal therapy (HT), or simple monitoring (5). Proper identification of recurrence location is important for subsequent treatment decisions because, in local recurrence or loco-regional LN metastasis, curative local treatments as SRT can still be feasible and improve disease-free survival and overall survival (8, 13, 14). In the case of distant metastasis, the patient would get most of the time only of palliative treatment (15). Imaging is a staple tool for discovering the site(s) of recurrence and distinguishing between local and distant metastatic disease.
Positron emission tomography (PET) with choline or PSMA has become the reference in detecting metastases in the skeleton, in distant lymph nodes, and in the viscera (16).
Prostate magnetic resonance imaging (MRI) with functional sequences allows early detection of local recurrence and may also be a valuable correlative imaging modality for equivocal PET findings (17). MRI provides a better anatomical delineation of recurrence for the CTV delineation (18), and it allows the delivery of higher radiation doses to a specific recurrence site.
However, the role of MRI in this indication is still discussed and has not been validated (19). The aim of this review is to address the role of MRI for the diagnosis and targeting of local recurrence after surgery in the setting of SRT.
MRI After RP: The Optimal PSA Cut–off
If the disease recurrence is suspected to be local and/or regional, the most common approach is to irradiate the surgical bed as early as possible with cutoff PSA values for referral of 0.1–0.5 ng/ml usually suggested. It has been shown that the best results of SRT are obtained when PSA values are low (20). However, with those PSA values, the probability of finding exact location of the recurrence is low. In a series reporting a high sensitivity (80%–95%) of MRI, usually the PSA value is over 1 ng/ml or local recurrence is palpable on digital rectal examination (DRE) (21, 22). For lower PSA values, Buergy et al. (23) were able to detect local recurrence at PSA values below 0.5 ng/ml with a minimum level of 0.31 ng/ml but were not able to detect recurrence for PSA level below 0.3 ng/ml. In a cohort of 183 patients with BCR after RP, Dirix et al. (24) found that MRI indicated a suspected macroscopic recurrence for 46 (25%) patients which was local in 22 (49%), mainly in the peri-anastomotic region for 11 patients (6%) and in pelvic lymph nodes in 23 (50%). The mean PSA value was higher for patients with a positive MRI (1.4 ng/ml vs. 0.4 ng/ml; p < 0.001), but relapse could be located in 13 (7%) patients with a PSA <0.5 ng/ml. When the PSA value was ≤0.3 ng/ml, Liauw et al. (25) observed a local recurrence on MRI only in 11/88 patients (13%) of the patients. Linder et al. (26) showed in their study of 132 patients with a median PSA of 0.59 ng/ml (range <0.1–13.1) that local recurrence was identified by multiparametric magnetic resonance imaging (mpMRI) in 124 patients (94%) with a median lesion size on MRI of 1 cm. The sensitivity of MRI was 91% with a specificity of 45%; the positive predictive value (PPV) and negative predictive value (NPV) were respectively 85% and 60%. For identifying local recurrence on MRI, the optimal PSA cutoff appears to range from 0.3 to 0.54 ng/ml and the PSA kinetic is also a strong predictor for positive MRI findings even with low PSA values (27).
MRI After RP: How?
The protocol is the same as that performed for tumor detection, compliant with European Society of Uro-Radiology guidelines with T1-weighted, T2-weighted, diffusion-weighted (DW), and dynamic contrast-enhanced (DCE) imaging sequences (28). T2W imaging is always used for anatomy orientation and evaluation of signal patterns after surgery. Functional imagery including diffusion with high b-value and perfusion imaging allow the important differentiation between recurrent cancer, residual prostate tissue, inflammatory tissue, and fibrosis.
Normal Pelvic Anatomy After Radical Prostatectomy
RP includes total removal of the prostate and seminal vesicles, along with pelvic lymph node dissection. Postradical prostatectomy MRI findings include descent of the bladder which is anastomosed to extra prostatic distal urethra. The vesico-urethral-anastomosis (VUA) should be visualized as a ring of postoperative fibrosis with low signal intensity on all sequences (Figure 1). Seminal vesicle (SV) which are supposed to be removed, may be retained in part with postoperative findings highly variable: 20% of the patients had SV remnants, with similar location of the preoperative SV position, with an additional 38% with fibrotic SV tips (21) (Figure 1).
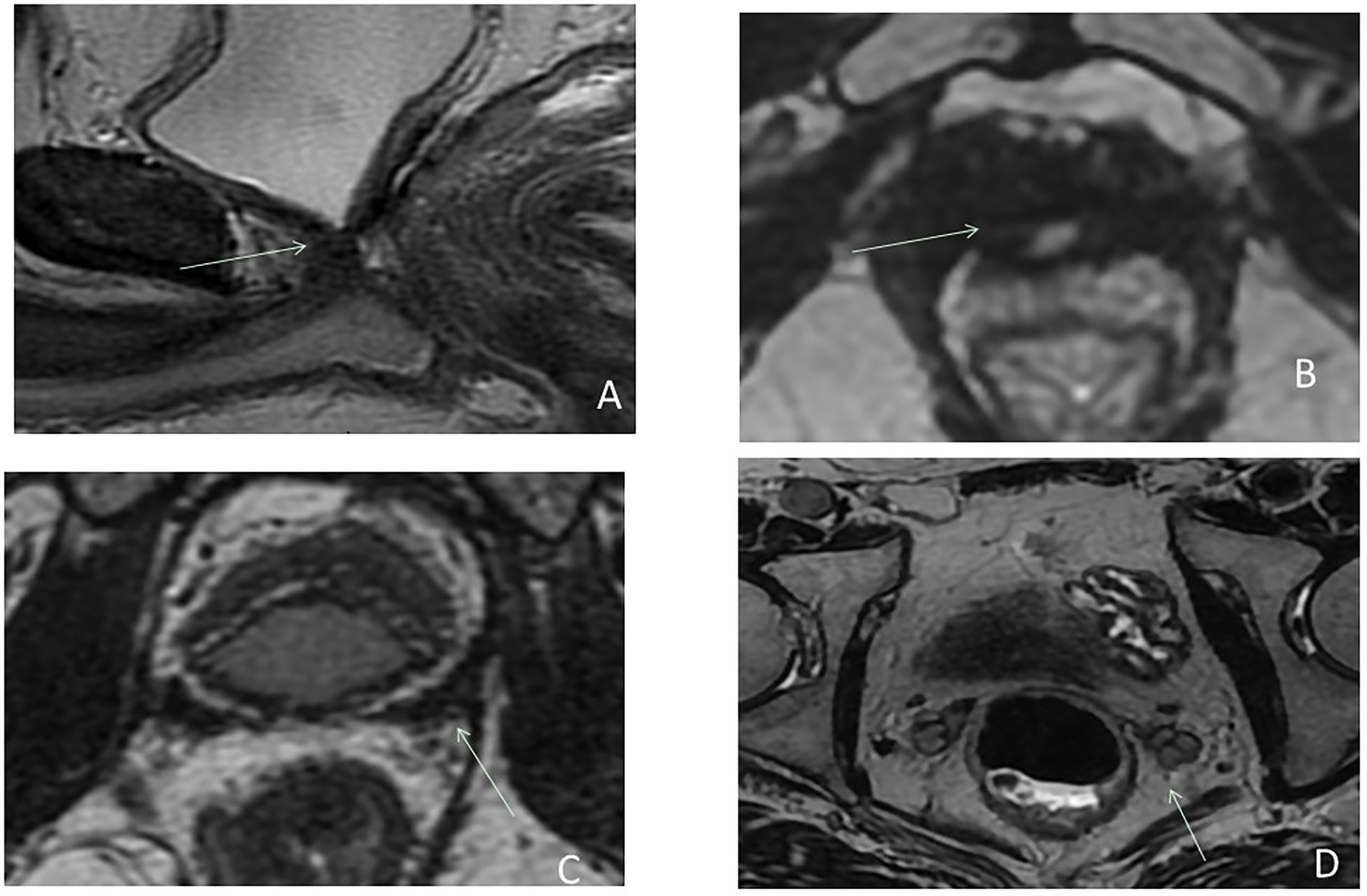
Figure 1 Postsurgical imaging findings after radical prostatectomy on sagittal (A) and axial (B–D) T2-weighted imaging: bladder neck descended into the prostatectomy fossa with a more conical shape (A); the VUA anastomosis (arrow) (A, B) visualized as a ring of postoperative fibrosis on low signal intensity inferior to the bladder neck. Seminal vesicles which are supposed to be removed in a classical RP demonstrate a low signal intensity (C) (postoperative fibrosis), but may be retained in part and can be seen in their presurgical locations with their characteristic tubular structure on T2W (D).
Location of Recurrence
The most common site of local recurrence after RP is the VUA, but recurrent masses can occur anywhere in the prostatectomy bed, including the retrovesical space, the bladder neck, near the seminal vesicles bed, or adjacent to the vas deferens (27, 29). In a series of 114 patients with a biological relapse after RP, local recurrence was seen on ultrasound at the anastomotic site (66%), the bladder neck (16%), and posterior to the trigone (13%) (30). MRI could help to define more accurately the target volume and so decrease toxicity (31). Moreover, the identification of a local recurrence is predictive of a better efficiency of SRT (32). The main series of local recurrence detected in MRI are presented in Table 1.
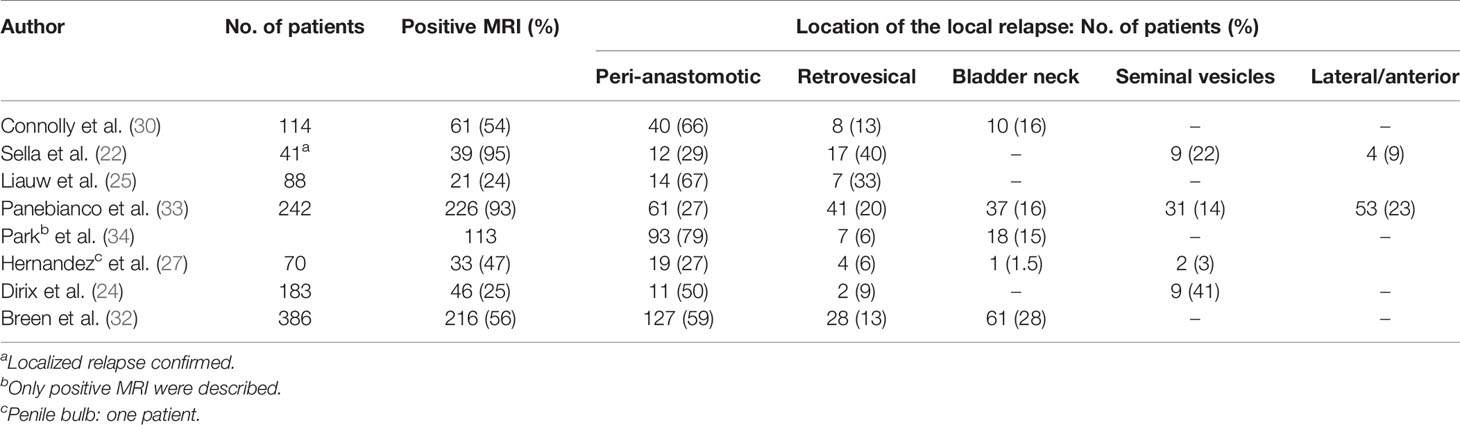
Table 1 Locations by MRI of local recurrences after radical prostatectomy.
Presentation of Recurrence on MRI
Local recurrence usually presents as a nodular, semicircumferential to ill-defined soft-tissue mass of intermediate T2-weighted signal intensity with associated diffusion restriction and rapid, early enhancement on dynamic contrast-enhanced imaging; signal characteristics are similar to those of the initial tumor (35) (Figure 2).
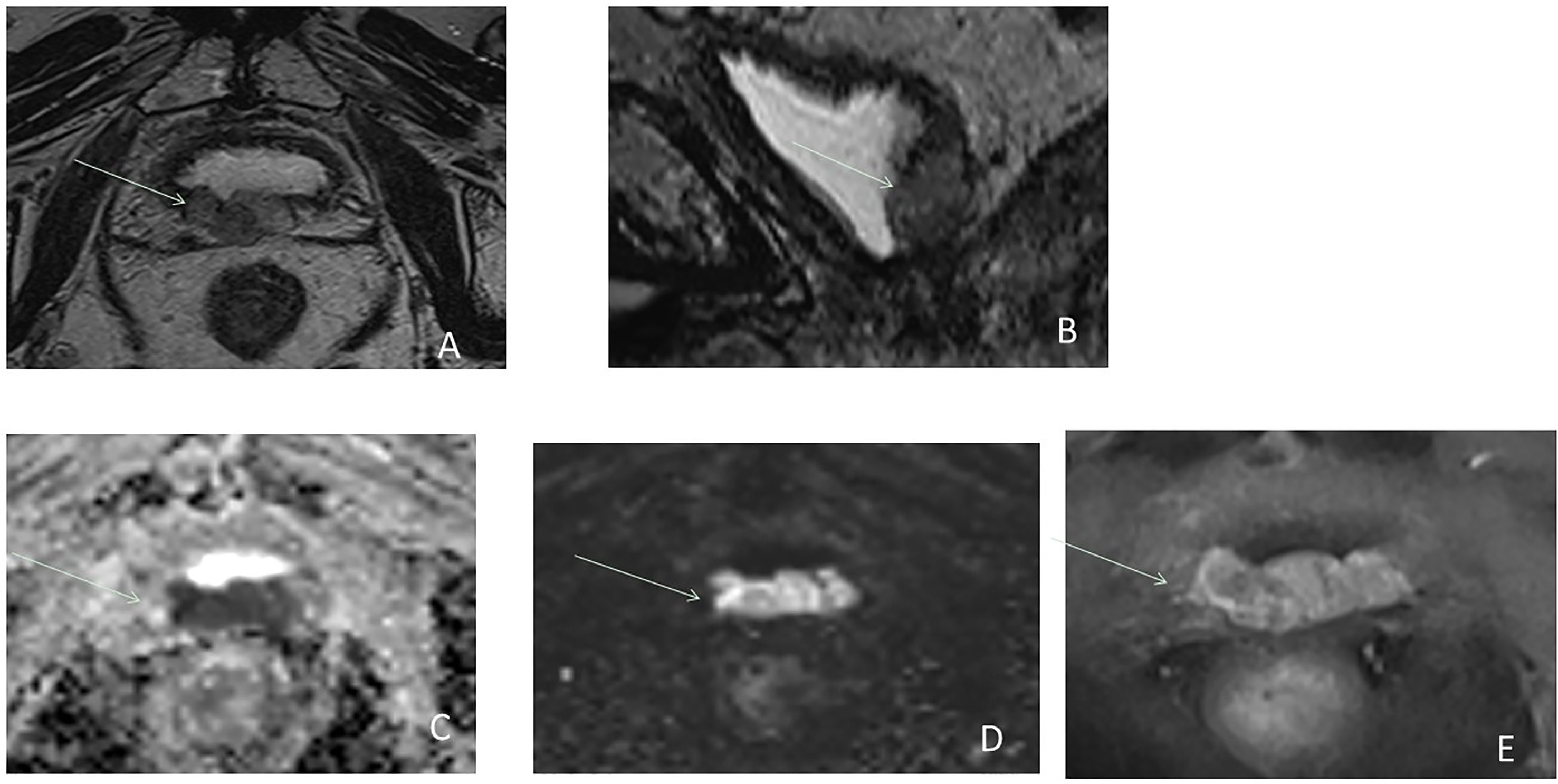
Figure 2 Postsurgical lesion recurrence (arrow) in a 63-year-old male with serum PSA = 0.8 ng/ml. Axial T2W MRI (A), sagittal T2W (B), ADC map (C), b2000 DW MRI (D), and DCE MRI (E) show a large lobulated mass relatively hyperintense on T2W, hypointense area on the ADC map, hyperintense area on b2000, and with early hyperenhancement located in the postpart of the bladder neck.
The value of DW MRI is very variable after RP. Diffusion imaging can be distorted by the presence of surgical clips and susceptibility artifacts. However, DWI can be useful for distinguishing tumor from mimicking etiologies, such as inflammation or residual benign tissue (33) (Figures 3, 4). The performance of diffusion imaging has been evaluated and showed good results, especially with the use of high b-values (that reflects the strength and timing of the gradients used to generate diffusion-weighted images). In this specific indication, the values of b must be greater than 1,400 s/mm2 and up to 3,000 s/mm2 (33). In a recent study of 118 patients, Kwon et al. (36) found DW imaging is accurate in distinguishing recurrence from slowly enhancing benign tissue on DCE MRI. Barchetti et al. (37), in a review, concluded its good diagnostic accuracy in detecting local recurrence after RP when combined with other sequences. In a recent systematic review, Sandgren et al. (38) found that DWI combined with T2W imaging had a pool sensitivity of 84% and a pool specificity of 89%. Nevertheless, the addition of DWI was of limited incremental value for detection, especially of small lesions (17). The sensitivity for nodules of sized ≥1 cm is better (39).
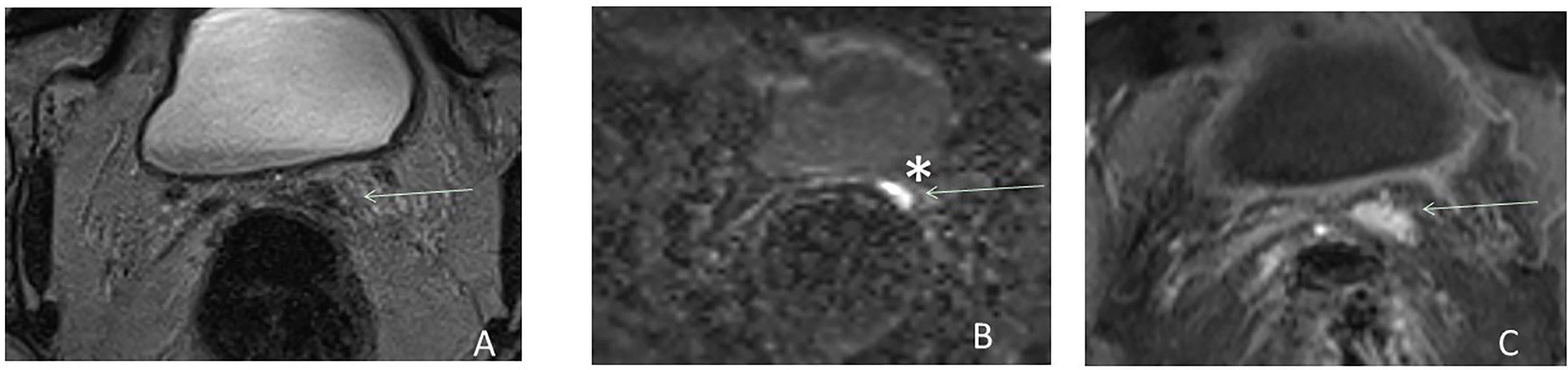
Figure 3 Postsurgical recurrence after RP. Axial T2W MRI (A), b2000 DW MRI (B), and DCE MRI (C) show the benefit of functional imaging to detect local recurrence in the left seminal vesicle bed (arrow) and particularly the benefit of high b-value *. *Highlight the benefit of high b value.
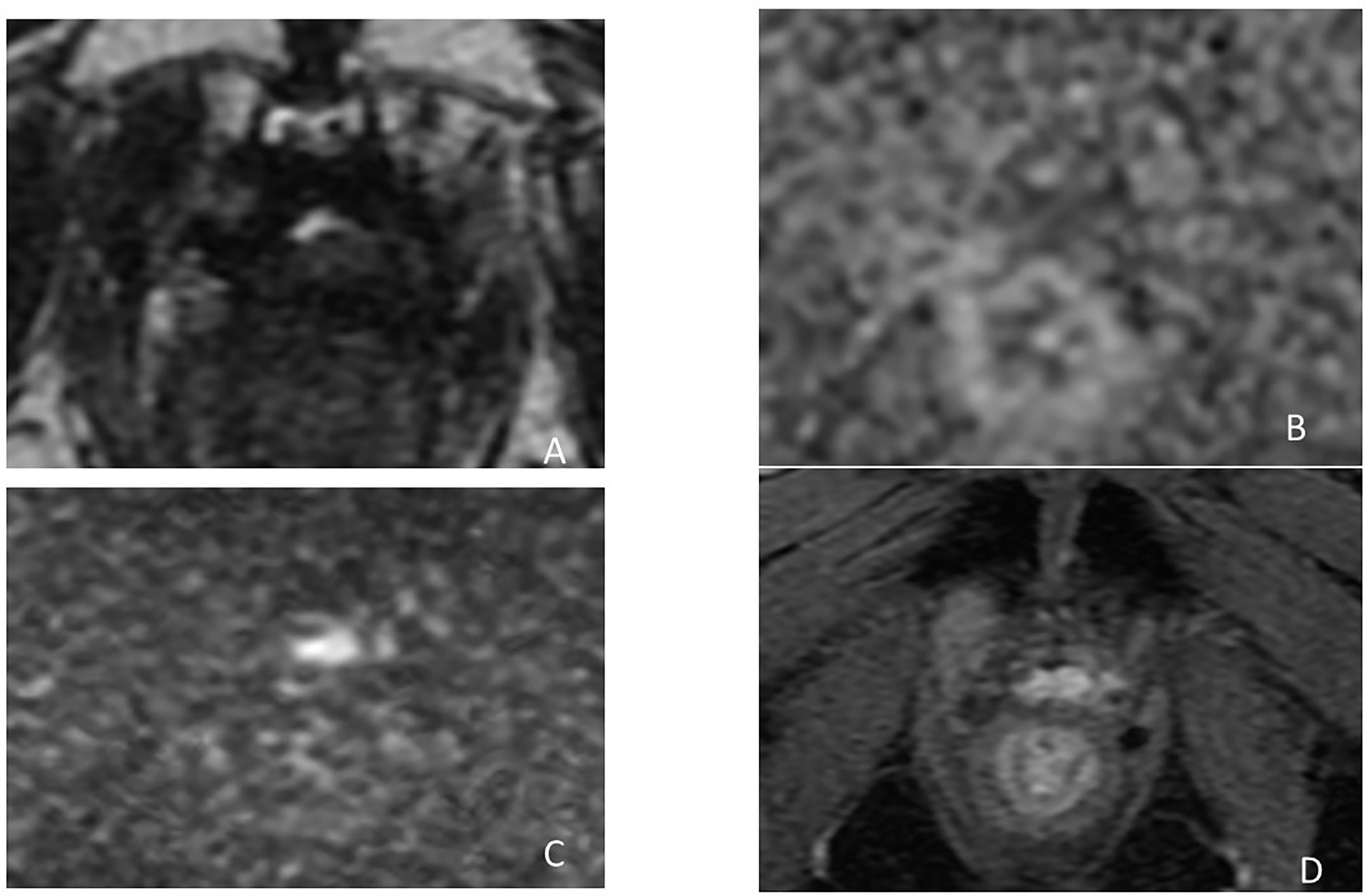
Figure 4 Postsurgical lesion recurrence (arrows) in a 63-year-old male with serum PSA = 0.6 ng/ml after radical prostatectomy. Axial T2W MRI (A), ADC map (B), b2000 DW MRI (C), and DCE MRI (D) show a soft tissue lesion at the posterior part of VUA, relatively hyperintense on T2W best seen on high b-value and DCE imaging with a focal nodular enhancement that contrasts sharply with the general background low-level venous enhancement.
DCE is more reliable than DWI and has long been considered the most useful sequence for detecting recurrence. Panebianco et al. (33) found a sensitivity and specificity of 98% and 94% for the detection of a local recurrence for an average PSA of 1.3 ng/ml (0.5–1.7 ng/ml) and an average size of 5 ± 0.6 mm (4 to 8 mm). Similarly, Kitajima et al. (17) found an AUC, sensitivity, and accuracy of mpMRI for detecting local recurrence of 0.91%, 88.5%, and 87.4%, respectively. The authors concluded that the addition of DCE to T2-weighted imaging improves the accuracy of detection of local cancer recurrence after RP and was significantly better than that of PET/CT with choline. De Visschere et al. (40) highlighted that even tiny recurrence “foci” that may not be visible on T2-weighted imaging tends to show a significant enhancement in the early arterial phase, often with contrast washout. Lastly, post-RP recurrences enhance sooner and faster than normal postoperative changes, allowing to distinguish from fibrotic or granulation tissue. Two meta-analyses evaluated the performance of mpMRI for the detection of local recurrence after RP and showed, for DCE combined with T2-weighted imaging, a pooled sensitivities and specificities of 85% and 95% (6) and 84% and 92%, respectively (38).
Performance of Anastomotic Biopsy After RP
No optimal TRUS-guided biopsy strategy has been defined. Even with TRUS guidance, the sensitivity of anastomotic biopsies is low 40%–71% for PSA levels >1 ng/ml and 14%–45% for PSA levels <1 ng/ml (41, 42).
Combination of MRI and PET-CT for Detection of Local Recurrence
The use of choline or PSMA PET-CT may help to identify regional or distant recurrences. PSMA PET-CT provides superior accuracy to the conventional imaging CT and bone scanning and is now proposed as a suitable replacement to the conventional imaging (5, 16). However, LR with close proximity and/or infiltration of the bladder is at risk to be missed in 68Ga-PSMA-11-PET as the radioactivity in the bladder may obliterate the visualization of the recurrence (43). The addition of MRI to PET may be useful in the early detection of these occult lesions developing in the bladder neck.
Counago et al. (44), in a retrospective analysis of 38 patients with BCR after RP showed that the combination of both MRI and 18FCH PET-CT gives a better LR detection rate versus choline PET/CT alone. Inferiority for 18F-FCH-PET compared with 68GaPSMA-11-PET was demonstrated for imaging of recurrent PC due to the excellent diagnostic accuracy of 68Ga-PSMA11 for PC-related tissue (45). This underlying potential benefit of the combination of MRI to PET-CT combining the advantage of MRI in obtaining morpho-functional information of local relapse with those of PET to detect nodal or distant recurrences. The use of PSMA-PET/MRI technologies allows the realization of this staging in a single session (46).
Eiber et al. (47) showed that 11C-choline PET/MRI improved the detection rate of local relapse compared with 11C-choline PET/CT in a prospective study of 75 patients: mean detection rates were respectively 84.7% versus 77.3%. In a study of 119 patients, the detection rate of 68Ga-PSMA-11-PET/MRI improved compared with PET/CT, particularly for LR close to the bladder (43). In a recent meta-analysis, PET/MRI had a high sensitivity rate (80.9%–95% CI, 73.0%–86.9%) in detecting relapse (48).
Delineation of the Clinical Target Volume
Various questions remain unresolved with regard to optimal target volume definition and RT doses that can vary depending on whether the recurrence is micro- or macroscopic (24).
However, most of the time recurrence remains microscopic and the volume definition of the CTV corresponds to the prostate bed. Nonetheless, even if MRI is negative, all potential recurrence sites listed in Table 1 must be included in the CTV. Published consensus guidelines are considering CT as reference imaging system to contribute in CTV delineation (29, 49, 50), except for the Princess Margaret Hospital (PMH) (51), which used postoperative MRI. Potential benefit of MRI is to enable a precise anatomical analysis of the prostate bed, cut end of the vas deferens, SV bed (SV remnants or fibrotic), and bladder neck, all common sites of recurrences (Figure 5).

Figure 5 Biological recurrence in a 58-year-old male. Axial T2-weighted images (A, B) and CT (C, D) showing the benefit of MRI to enable a better delineation of anatomical analysis of the VUA (A, C), cut end of the vas deferens and SV bed (B, D), and bladder neck, all common sites of recurrences.
Croke et al. (52) showed that current CTV consensus definition does not adequately cover prostate bed, and that application of the current CTV guidelines results in a localization error in approximately one-third of the target volume base on preoperative MRI-defined prostate volumes.
MRI could transform an invisible target in a visible target volume (18). In the case of an identified recurrence, modification of the CTV could be necessary to avoid underdosage of the recurrence area (53). Image registration between mpMRI and planning CT scan helps to identify accurately the target and decreases the CTV and the doses delivered to organs at risk (54). Moreover, it allows intensification of radiotherapy: Zilli et al. (55) treated 131 patients with a dose of 64 Gy on a surgical bed and added a 10-Gy boost on the recurrence site. Toxicity was not increased and local relapse-free survival was 100%. A concomitant integrated boost is also feasible without increasing toxicity (56). However, the benefit of this boost dose was not demonstrated (55–57).
Identification of a local recurrence on MRI is associated with a better efficacy of SRT. So, negative MRI is an argument to the use of androgen deprivation therapy (ADT), in combination with SRT, particularly if the PSA is higher than 0.5 ng/ml (32, 34, 58).
Conclusion
Multiparametric MRI could be a useful tool before SRT, showing local or regional relapse with sensitivity and specificity reaching 90%. Combined with PSMA PET-CT, ideally during the same session, it allows to spare some patients with distant relapse from a futile SRT. In the future, it could be proposed to patients with BCR, particularly when the PSA is higher than 0.3–0.5 ng/ml, to facilitate the delineation of target volume and allow dose escalation on a specific area.
Author Contributions
All authors have participated in the conception and drafting of the manuscript under the supervision of RP, IL, and CH. All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ADC, apparent diffusion coefficient; ADT, androgen deprivation therapy; DCE, dynamic contrast-enhanced; DWI, diffusion-weighted imaging; EAU, European Association of Urology; ISUP, International Society of Urological Pathology; LR, local recurrence; mpMRI, multiparametric magnetic resonance imaging; NPV, negative predictive value; PPV, positive predictive value; RP, radical prostatectomy; SRT, salvage radiation therapy; SV, seminal vesicle; T2W, T2-weighted; VUA, vesico-urethro-anastomis; yo, years old.
References
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global Cancer Statistics, 2012: Global Cancer Statistics, 2012. CA: A Cancer J Clin (2015) 65:87–108. doi: 10.3322/caac.21262
2. Pfister D, Bolla M, Briganti A, Carroll P, Cozzarini C, Joniau S, et al. Early Salvage Radiotherapy Following Radical Prostatectomy. Eur Urol (2014) 65:1034–43. doi: 10.1016/j.eururo.2013.08.013
3. Stephenson AJ, Kattan MW, Eastham JA, Dotan ZA, Bianco FJ Jr, Lilja H, et al. Defining Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy: A Proposal for a Standardized Definition. J Clin Oncol (2006) 24:3973–8. doi: 10.1200/JCO.2005.04.0756
4. Horwitz EM, Thames HD, Kuban DA, Levy LB, Kupelian PA, Martinez AA, et al. Definitions Of Biochemical Failure That Best Predict Clinical Failure In Patients With Prostate Cancer Treated With External Beam Radiation Alone: A Multi-Institutional Pooled Analysis. J Urol (2005) 173:797–802. doi: 10.1097/01.ju.0000152556.53602.64
5. Mottet N, van den Bergh RCN, Briers E, Van den Broeck T, Cumberbatch MG, De Santis M, et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment With Curative Intent. Eur Urol (2021) 79:243–62. doi: 10.1016/j.eururo.2020.09.042
6. Wu LM, Xu JR, Gu HY, Hua J, Zhu J, Chen J, et al. Role of Magnetic Resonance Imaging in the Detection of Local Prostate Cancer Recurrence After External Beam Radiotherapy and Radical Prostatectomy. Clin Oncol (R Coll Radiol) (2013) 25:252–64. doi: 10.1016/j.clon.2012.11.010
7. Lange PH, Ercole CJ, Lightner DJ, Fraley EE, Vessella R. The Value of Serum Prostate Specific Antigen Determinations Before and After Radical Prostatectomy. J Urol (1989) 141:873–9. doi: 10.1016/S0022-5347(17)41037-8
8. Van den Broeck T, van den Bergh RCN, Arfi N, Gross T, Moris L, Briers E, et al. Prognostic Value of Biochemical Recurrence Following Treatment With Curative Intent for Prostate Cancer: A Systematic Review. Eur Urol (2019) 75:967–87. doi: 10.1016/j.eururo.2019.03.027
9. Jhaveri FM, Klein EA. How to Explore the Patient With a Rising PSA After Radical Prostatectomy: Defining Local Versus Systemic Failure. Semin Urol Oncol (1999) 17:130–4.
10. Yossepowitch O, Briganti A, Eastham JA, Epstein J, Graefen M, Montironi R, et al. Positive Surgical Margins After Radical Prostatectomy: A Systematic Review and Contemporary Update. Eur Urol (2014) 65:303–13. doi: 10.1016/j.eururo.2013.07.039
11. Moul JW. Prostate Specific Antigen Only Progression of Prostate Cancer. J Urol (2000) 163:1632–42. doi: 10.1016/S0022-5347(05)67511-8
12. Neulander EZ, Soloway MS. Failure After Radical Prostatectomy. Urology (2003) 61:30–6. doi: 10.1016/S0090-4295(02)01918-0
13. Trock BJ, Han M, Freedland SJ, Humphreys EB, DeWeese TL, Partin AW, et al. Prostate Cancer-Specific Survival Following Salvage Radiotherapy vs Observation in Men With Biochemical Recurrence After Radical Prostatectomy. JAMA (2008) 299:2760–9. doi: 10.1001/jama.299.23.2760
14. Stish BJ, Pisansky TM, Harmsen WS, Davis BJ, Tzou KS, Choo R, et al. Improved Metastasis-Free and Survival Outcomes With Early Salvage Radiotherapy in Men With Detectable Prostate-Specific Antigen After Prostatectomy for Prostate Cancer. J Clin Oncol (2016) 34:3864–71. doi: 10.1200/JCO.2016.68.3425
15. Cornford P, van den Bergh RCN, Briers E, Van den Broeck T, Cumberbatch MG, De Santis M, et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Part II-2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur Urol (2021) 79:263–82. doi: 10.1016/j.eururo.2020.09.046
16. Rozet F, Mongiat-Artus P, Hennequin C, Beauval JB, Beuzeboc P, Cormier L, et al. French ccAFU Guidelines - Update 2020-2022: Prostate Cancer. Prog Urol (2020) 30:S136–251. doi: 10.1016/S1166-7087(20)30752-1
17. Kitajima K, Murphy RC, Nathan MA, Froemming AT, Hagen CE, Takahashi N, et al. Detection of Recurrent Prostate Cancer After Radical Prostatectomy: Comparison of 11C-Choline PET/CT With Pelvic Multiparametric MR Imaging With Endorectal Coil. J Nucl Med (2014) 55:223–32. doi: 10.2967/jnumed.113.123018
18. Latorzeff I, Sargos P, Loos G, Supiot S, Guerif S, Carrie C. Delineation of the Prostate Bed: The "Invisible Target" Is Still an Issue? Front Oncol (2017) 7:108. doi: 10.3389/fonc.2017.00108
19. Mottet N, Bellmunt J, Bolla M, Briers E, Cumberbatch MG, De Santis M, et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local Treatment With Curative Intent. Eur Urol (2017) 71:618–29. doi: 10.1016/j.eururo.2016.08.003
20. Tendulkar RD, Agrawal S, Gao T, Efstathiou JA, Pisansky TM, Michalski JM, et al. Contemporary Update of a Multi-Institutional Predictive Nomogram for Salvage Radiotherapy After Radical Prostatectomy. J Clin Oncol (2016) 34:3648–54. doi: 10.1200/JCO.2016.67.9647
21. Cirillo S, Petracchini M, Scotti L, Gallo T, Macera A, Bona MC, et al. Endorectal Magnetic Resonance Imaging at 1.5 Tesla to Assess Local Recurrence Following Radical Prostatectomy Using T2-Weighted and Contrast-Enhanced Imaging. Eur Radiol (2009) 19:761–9. doi: 10.1007/s00330-008-1174-8
22. Sella T, Schwartz LH, Swindle PW, Onyebuchi CN, Scardino PT, Scher HI, et al. Suspected Local Recurrence After Radical Prostatectomy: Endorectal Coil MR Imaging. Radiology (2004) 231:379–85. doi: 10.1148/radiol.2312030011
23. Buergy D, Sertdemir M, Weidner A, Shelan M, Lohr F, Wenz F, et al. Detection of Local Recurrence With 3-Tesla MRI After Radical Prostatectomy: A Useful Method for Radiation Treatment Planning? In Vivo (2018) 32:125–31. doi: 10.21873/invivo.11214
24. Dirix P, van Walle L, Deckers F, Van Mieghem F, Buelens G, Meijnders P, et al. Proposal for Magnetic Resonance Imaging-Guided Salvage Radiotherapy for Prostate Cancer. Acta Oncol (2017) 56:27–32. doi: 10.1080/0284186X.2016.1223342
25. Liauw SL, Pitroda SP, Eggener SE, Stadler WM, Pelizzari CA, Vannier MW, et al. Evaluation of the Prostate Bed for Local Recurrence After Radical Prostatectomy Using Endorectal Magnetic Resonance Imaging. Int J Radiat Oncol Biol Phys (2013) 85:378–84. doi: 10.1016/j.ijrobp.2012.05.015
26. Linder BJ, Kawashima A, Woodrum DA, Tollefson MK, Karnes J, Davis BJ, et al. Early Localization of Recurrent Prostate Cancer After Prostatectomy by Endorectal Coil Magnetic Resonance Imaging. Can J Urol (2014) 21:7283–9.
27. Hernandez D, Salas D, Giménez D, Buitrago P, Esquena S, Palou J, et al. Pelvic MRI Findings in Relapsed Prostate Cancer After Radical Prostatectomy. Radiat Oncol (2015) 10:262. doi: 10.1186/s13014-015-0574-6
28. Turkbey B, Rosenkrantz AB, Haider MA, Padhani AR, Villeirs G, Macura KJ, et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur Urol (2019) 76:340–51. doi: 10.1016/j.eururo.2019.02.033
29. Poortmans P, Bossi A, Vandeputte K, Bosset M, Miralbell R, Maingon P, et al. Guidelines for Target Volume Definition in Post-Operative Radiotherapy for Prostate Cancer, on Behalf of the EORTC Radiation Oncology Group. Radiother Oncol (2007) 84:121–7. doi: 10.1016/j.radonc.2007.07.017
30. Connolly JA, Shinohara K, Presti JC Jr, Carroll PR. Local Recurrence After Radical Prostatectomy: Characteristics in Size, Location, and Relationship to Prostate-Specific Antigen and Surgical Margins. Urology (1996) 47:225–31. doi: 10.1016/S0090-4295(99)80421-X
31. Miralbell R, Vees H, Lozano J, Khan H, Mollà M, Hidalgo A, et al. Endorectal MRI Assessment of Local Relapse After Surgery for Prostate Cancer: A Model to Define Treatment Field Guidelines for Adjuvant Radiotherapy in Patients at High Risk for Local Failure. Int J Radiat Oncol Biol Phys (2007) 67:356–61. doi: 10.1016/j.ijrobp.2006.08.079
32. Breen WG, Stish BJ, Harmsen WS, Froemming AT, Mynderse LA, Choo CR, et al. The Prognostic Value, Sensitivity, and Specificity of Multiparametric Magnetic Resonance Imaging Before Salvage Radiotherapy for Prostate Cancer. Radiother Oncol (2021) 161:9–15. doi: 10.1016/j.radonc.2021.05.015
33. Panebianco V, Barchetti F, Sciarra A, Musio D, Forte V, Gentile V, et al. Prostate Cancer Recurrence After Radical Prostatectomy: The Role of 3-T Diffusion Imaging in Multi-Parametric Magnetic Resonance Imaging. Eur Radiol (2013) 23:1745–52. doi: 10.1007/s00330-013-2768-3
34. Park JS, Park W, Pyo HR, Park BK, Park SY, Choi HY, et al. Suggestion for the Prostatic Fossa Clinical Target Volume in Adjuvant or Salvage Radiotherapy After a Radical Prostatectomy. Radiother Oncol (2014) 110:240–4. doi: 10.1016/j.radonc.2014.01.001
35. Oppenheimer DC, Weinberg EP, Hollenberg GM, Meyers SP. Multiparametric Magnetic Resonance Imaging of Recurrent Prostate Cancer. J Clin Imaging Sci (2016) 6:18. doi: 10.4103/2156-7514.181494
36. Kwon T, Kim JK, Lee C, Jung J, Ahn H, Kim CS, et al. Discrimination of Local Recurrence After Radical Prostatectomy: Value of Diffusion-Weighted Magnetic Resonance Imaging. Prostate Int (2018) 6:12–7. doi: 10.1016/j.prnil.2017.05.002
37. Barchetti F, Panebianco V. Multiparametric MRI for Recurrent Prostate Cancer Post Radical Prostatectomy and Postradiation Therapy. BioMed Res Int (2014) 2014:316272. doi: 10.1155/2014/316272
38. Sandgren K, Westerlinck P, Jonsson JH, Blomqvist L, Thellenberg Karlsson C, Nyholm T, et al. Imaging for the Detection of Locoregional Recurrences in Biochemical Progression After Radical Prostatectomy-A Systematic Review. Eur Urol Focus (2019) 5:550–60. doi: 10.1016/j.euf.2017.11.001
39. Panebianco V, Villeirs G, Weinreb JC, Turkbey BI, Margolis DJ, Richenberg J, et al. Prostate Magnetic Resonance Imaging for Local Recurrence Reporting (PI-RR): International Consensus -Based Guidelines on Multiparametric Magnetic Resonance Imaging for Prostate Cancer Recurrence After Radiation Therapy and Radical Prostatectomy. Eur Urol Oncol (2021) S2588-9311:00027–4. doi: 10.1016/j.euo.2021.01.003
40. De Visschere PJL, Standaert C, Fütterer JJ, Villeirs GM, Panebianco V, Walz J, et al. A Systematic Review on the Role of Imaging in Early Recurrent Prostate Cancer. Eur Urol Oncol (2019) 2:47–76. doi: 10.1016/j.euo.2018.09.010
41. Rouvière O, Vitry T, Lyonnet D. Imaging of Prostate Cancer Local Recurrences: Why and How? Eur Radiol (2010) 20:1254–66. doi: 10.1007/s00330-009-1647-4
42. Deliveliotis C, Manousakas T, Chrisofos M, Skolarikos A, Delis A, Dimopoulos C, et al. Diagnostic Efficacy of Transrectal Ultrasound-Guided Biopsy of the Prostatic Fossa in Patients With Rising PSA Following Radical Prostatectomy. World J Urol (2007) 25:309–13. doi: 10.1007/s00345-007-0167-6
43. Freitag MT, Radtke JP, Afshar-Oromieh A, Roethke MC, Hadaschik BA, Gleave M, et al. Local Recurrence of Prostate Cancer After Radical Prostatectomy is at Risk to be Missed in 68Ga-PSMA-11-PET of PET/CT and PET/MRI: Comparison With mpMRI Integrated in Simultaneous PET/MRI. Eur J Nucl Med Mol Imaging (2017) 44:776–87. doi: 10.1007/s00259-016-3594-z
44. Couñago F, Recio M, Maldonado A, Del Cerro E, Díaz-Gavela AA, Thuissard IJ, et al. Evaluation of Tumor Recurrences After Radical Prostatectomy Using 18F-Choline PET/CT and 3T Multiparametric MRI Without Endorectal Coil: A Single Center Experience. Cancer Imaging (2016) 16:42. doi: 10.1186/s40644-016-0099-8
45. Hofman MS, Lawrentschuk N, Francis RJ, Tang C, Vela I, Thomas P, et al. Prostate-Specific Membrane Antigen PET-CT in Patients With High-Risk Prostate Cancer Before Curative-Intent Surgery or Radiotherapy (proPSMA): A Prospective, Randomised, Multicentre Study. Lancet (2020) 395:1208–16. doi: 10.1016/S0140-6736(20)30314-7
46. Afshar-Oromieh A, Zechmann CM, Malcher A, Eder M, Eisenhut M, Linhart HG, et al. Comparison of PET Imaging With a (68)Ga-Labelled PSMA Ligand and (18)F-Choline-Based PET/CT for the Diagnosis of Recurrent Prostate Cancer. Eur J Nucl Med Mol Imaging (2014) 41:11–20. doi: 10.1007/s00259-013-2525-5
47. Eiber M, Rauscher I, Souvatzoglou M, Maurer T, Schwaiger M, Holzapfel K, et al. Prospective Head-to-Head Comparison of (11)C-Choline-PET/MR and (11)C-Choline-PET/CT for Restaging of Biochemical Recurrent Prostate Cancer. Eur J Nucl Med Mol Imaging (2017) 44:2179–88. doi: 10.1007/s00259-017-3797-y
48. Evangelista L, Zattoni F, Cassarino G, Artioli P, Cecchin D, Dal Moro F, et al. PET/MRI in Prostate Cancer: A Systematic Review and Meta-Analysis. Eur J Nucl Med Mol Imaging (2021) 48:859–73. doi: 10.1007/s00259-020-05025-0
49. Sidhom MA, Kneebone AB, Lehman M, Wiltshire KL, Millar JL, Mukherjee RK, et al. Post-Prostatectomy Radiation Therapy: Consensus Guidelines of the Australian and New Zealand Radiation Oncology Genito-Urinary Group. Radiother Oncol (2008) 88:10–9. doi: 10.1016/j.radonc.2008.05.006
50. Michalski JM, Lawton C, El Naqa I, Ritter M, O'Meara E, Seider MJ, et al. Development of RTOG Consensus Guidelines for the Definition of the Clinical Target Volume for Postoperative Conformal Radiation Therapy for Prostate Cancer. Int J Radiat Oncol Biol Phys (2010) 76:361–8. doi: 10.1016/j.ijrobp.2009.02.006
51. Wiltshire KL, Brock KK, Haider MA, Zwahlen D, Kong V, Chan E, et al. Anatomic Boundaries of the Clinical Target Volume (Prostate Bed) After Radical Prostatectomy. Int J Radiat Oncol Biol Phys (2007) 69:1090–9. doi: 10.1016/j.ijrobp.2007.04.068
52. Croke J, Malone S, Roustan Delatour N, Belanger E, Avruch L, Morash C, et al. Postoperative Radiotherapy in Prostate Cancer: The Case of the Missing Target. Int J Radiat Oncol Biol Phys (2012) 83:1160–8. doi: 10.1016/j.ijrobp.2011.09.039
53. Wang J, Kudchadker R, Choi S, Pettaway CA, Choi H, Hobbs BD, et al. Local Recurrence Map to Guide Target Volume Delineation After Radical Prostatectomy. Pract Radiat Oncol (2014) 4:e239–e46. doi: 10.1016/j.prro.2014.02.007
54. Sardaro A, Turi B, Bardoscia L, Ferrari C, Rubini G, Calabrese A, et al. The Role of Multiparametric Magnetic Resonance in Volumetric Modulated Arc Radiation Therapy Planning for Prostate Cancer Recurrence After Radical Prostatectomy: A Pilot Study. Front Oncol (2021) 10. doi: 10.3389/fonc.2020.603994
55. Zilli T, Jorcano S, Peguret N, Caparrotti F, Hidalgo A, Khan HG, et al. Results of Dose-Adapted Salvage Radiotherapy After Radical Prostatectomy Based on an Endorectal MRI Target Definition Model. Am J Clin Oncol (2017) 40:194–9. doi: 10.1097/COC.0000000000000130
56. Zaine H, Vandendorpe B, Bataille B, Lacornerie T, Wallet J, Mirabel X, et al. Salvage Radiotherapy for Macroscopic Local Recurrence Following Radical Prostatectomy. Front Oncol (2021) 11. doi: 10.3389/fonc.2021.669261
57. Bruni A, Ingrosso G, Trippa F, Di Staso M, Lanfranchi B, Rubino L, et al. Macroscopic Locoregional Relapse From Prostate Cancer: Which Role for Salvage Radiotherapy. Clin Trans Oncol (2019) 21:1532–7. doi: 10.1007/s12094-019-02084-0
Keywords: prostate cancer, prostatectomy, MRI, diffusion magnetic resonance imaging, local neoplasm recurrence, radiation therapy
Citation: Renard-Penna R, Zhang-Yin J, Montagne S, Aupin L, Bruguière E, Labidi M, Latorzeff I and Hennequin C (2022) Targeting Local Recurrence After Surgery With MRI Imaging for Prostate Cancer in the Setting of Salvage Radiation Therapy. Front. Oncol. 12:775387. doi: 10.3389/fonc.2022.775387
Received: 13 September 2021; Accepted: 05 January 2022;
Published: 15 February 2022.
Edited by:
Felix Preisser, Universitätsklinikum Frankfurt, GermanyReviewed by:
Mack Roach III, University of California, San Francisco, United StatesCozzarini Cesare, San Raffaele Hospital (IRCCS), Italy
Benedikt Hoeh, University Hospital Frankfurt, Germany
Copyright © 2022 Renard-Penna, Zhang-Yin, Montagne, Aupin, Bruguière, Labidi, Latorzeff and Hennequin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raphaële Renard-Penna, raphaele.renardpenna@aphp.fr