 Tae-Young Choi
Tae-Young Choi Ji Hee Jun
Ji Hee Jun Hye Won Lee
Hye Won Lee Jong-Min Yun3
Jong-Min Yun3 Min Cheol Joo
Min Cheol Joo Myeong Soo Lee
Myeong Soo Lee- 1KM Science Research Division, Korea Institute of Oriental Medicine, Daejeon, South Korea
- 2KM Convergence Research Division, Korea Institute of Oriental Medicine, Daejeon, South Korea
- 3Department of Korean Internal Medicine, College of Korean Medicine, Wonkwang University, Iksan, South Korea
- 4Department of Rehabilitation Medicine and Institute of Wonkwang Medical Science, Wonkwang University School of Medicine, Iksan, South Korea
Evidence mapping of systematic reviews (SRs) systematically and comprehensively identifies, organizes, and summarizes the distribution of scientific evidence in a field. The aim of this evidence map is to provide a synopsis of the best clinical practices and interventions in stroke rehabilitative care and to identify areas with a paucity of evidence to guide future research. PubMed, EMBASE, CDSR, six Korean databases, and two Chinese databases were searched for SRs evaluating the effectiveness of any stroke rehabilitation intervention through October 2021. The quality of the SRs was assessed using AMSTAR 2. A bubble plot was used to graphically display clinical topics, the number of articles, the number of patients included, confidence, and effectiveness. In total, ninety-five SRs were identified; however, after methodological analysis, only 48 had sufficient quality to be included. In total, forty-eight SRs were included in the evidence mapping. The overall search identified SRs from 2015 to 2021. A total of four SRs focused on post-stroke cognitive impairment, whereas the other forty-four SRs focused on post-stroke motor function. In total, nineteen different traditional Chinese medicine (TCM) intervention modalities were included. Acupuncture was the most commonly used treatment. Overall, the quality of the included SRs was low or very low. Most SRs concluded that TCM interventions may have potential benefits in stroke rehabilitation. The results were more promising when acupuncture was used for shoulder–hand syndrome. However, the identified reviews cautioned that firm conclusions cannot be drawn. The evidence map provides a visual overview of the research volume and content involving TCM interventions in stroke rehabilitation. Evidence mapping can facilitate the process of knowledge translation from scientific findings to researchers and policymakers and possibly reduce waste in research.
Introduction
Stroke is the second leading cause of death and long-term disability worldwide (1). Despite advances in modern medicine and medications, stroke remains a burden affecting disability-adjusted life years (2). Strokes can cause significant impairments that include different degrees of cognitive and behavioral dysfunction, paralysis, dysphagia, aphasia, and motor dysfunction (3). The mortality rate of stroke has been gradually decreasing, but the disability rate of stroke remains high (4). Appropriate stroke rehabilitation treatment is essential to minimize patient disability, promote the return to social activities, and improve quality of life. However, while modern medicine lacks effective treatment for this recovery period, traditional Chinese medicine (TCM) offers great possibilities (5).
TCM has been used for centuries in the treatment of stroke. Because of fewer side effects, TCM has often been sought to provide intervention therapies for the prevention of and rehabilitation from a stroke in China and Korea. Furthermore, TCM is popular not only in other parts of Asia but also in some Western countries, including USA and Australia. TCM mainly includes herbal medications, acupuncture, moxibustion, cupping, and tuina. More than 100 kinds of TCM interventions have been used to prevent and treat stroke (6). Acupuncture in particular is safe and improves cognitive function and depressive disorder in post-stroke patients (7). TCM has the merits of diminishing disability rates, boosting the quality of life, having low toxicity and side effects, and having low therapy costs for patients in post-stroke recovery (8). However, evidence for the efficacy and safety of these interventions remains inconsistent and uncertain. Meanwhile, the quality of the methodology and evidence in the field remains unknown.
There is a vast amount of scientific literature proposing treatment approaches for stroke rehabilitation. Systematic reviews (SRs) are one of the options used to organize and critically assess published studies and summarize the results of the evidence from healthcare-related primary studies to answer specific research questions. Evidence mapping of SRs systematically and comprehensively identifies, organizes, and summarizes the distribution of scientific evidence in a field, aiming to identify gaps in knowledge and future research needs. This evidence mapping aims to provide a synopsis of the best clinical practices and interventions in stroke rehabilitative care and identify areas with a paucity of evidence to guide future research.
Methods
Study Design
Evidence mapping is not associated with an official standardized method (9). The approach in this study was adopted from the methodology that Solloway et al. used in the “Evidence Map of Tai Chi” (10).
Electronic Searches and Search Strategy
SRs were searched in 11 databases, including PubMed, EMBASE, and the Cochrane Database of Systematic Reviews (CDSR), and also six Korean databases [Korea Med, the Oriental Medicine Advanced Search Integrated System (OASIS), DBpia, the Korean Medical Database (KM base), the Research Information Service System (RISS) and the Korean Studies Information Services System (KISS)] and two Chinese databases [the China National Knowledge Infrastructure (CNKI) and Wang Fang], from database inception through October 2021. In addition, the reference lists of potentially eligible articles were searched manually to identify additional relevant articles.
The search terms used were based on the text words “systematic review” or “meta-analysis.” and “stroke rehabilitation,” and database-specific filters for SRs were used to develop the search strategy with no language restrictions (Supplementary Table 1).
Inclusion Criteria
Design
Only SRs focusing on TCM interventions in stroke rehabilitation and summarizing primary research studies for all the clinical indications were included. In this study, we considered SRs containing at least one randomized controlled trial (RCT), which addressed the use of TCM in stroke rehabilitation.
Population
We examined trials, including adults (aged over 18 years) with a clinical diagnosis of stroke (all types, severity levels, and stages of stroke), paresis of the upper, lower, or both sets of limbs (motor function), and confirmed cognitive impairment as specified in each trial (cognitive impairments included disruptions in attention and concentration, memory, orientation, and/or executive functions).
Intervention and Comparators
All types of TCM interventions were considered, including but not limited to the following: acupuncture, electroacupuncture (EA), Chinese herbal medicine (CHM), moxibustion, tai chi, qigong, Chinese herbal bath, and tuina. Combination therapies incorporating TCM interventions were also included. Comparators included non-treatment, sham treatment, placebo treatment, and routine treatments (rehabilitation and positive interventions).
Outcomes
SRs reporting on patients' health outcomes were eligible for inclusion. SRs focused on provider outcomes, study design, or intervention features that did not report patient health outcomes were excluded.
SR Selection
All scoping, rapid, critical, and narrative reviews were excluded. Two reviewers (T-YC and JJ) independently screened all the titles and abstracts and selected full-text articles to exclude irrelevant SRs. Disagreements were resolved through discussion and consensus, and an additional reviewer (MSL) was consulted. Where originals and updates of SRs by the same author group were available, only the most recent version was considered, and multiple publications of the same review were counted as one review, although data were extracted from all the available publications. If multiple reviews of similar clinical topics were identified, the most pertinent and best-performing SR was used for inclusion in evidence maps and was selected based on the results of the Assessing the Methodological Quality of Systematic Reviews 2 (AMSTAR 2) assessment.
Data Extraction
All the articles were read by two independent reviewers (T-YC and JHJ), data were extracted from the articles based on predefined criteria, and a methodological quality assessment was conducted. Disagreements were resolved by consensus, and when necessary, an additional reviewer (MSL) participated in the discussion. Information on PICO (population, intervention, comparison, and outcomes), the number of RCTs included in each SR, summary effect estimates for main outcomes, overall risk of bias (ROB), publication bias, and conclusions (quoted from the original article) were extracted from the included SRs.
Methodological Quality Assessment
The AMSTAR 2 tool was used to critically appraise the quality of reporting for each included SR. A validated 16-item instrument for critically appraising SRs that assesses the quality and bias using ratings of “yes,” “partial yes,” or “no” (11). Overall confidence in the results of an SR is rated according to the following four categories: “high” (no or one non-critical weakness), “moderate” (more than one non-critical weakness), “low” (one critical flaw with or without non-critical weaknesses), and “critically low” (more than one critical flaw with or without non-critical weaknesses).
Evidence Mapping Presentation
We used the topics of the identified SRs to categorize the reviews. We presented the evidence mapping in tables describing the characteristics of the included SRs and a graphic display of the mapping based on bubble plots. Each bubble in the chart represents one included SR. The SR grouping into the clinical topics was drafted by one reviewer and discussed among the review team.
The chart displays information in four dimensions:
1) X-axis: stroke rehabilitative symptoms.
Stroke rehabilitative symptoms were classified. The studies were categorized into those assessing cognitive function and those assessing motor function.
2) Y-axis: AMSTAR 2 assessment/strength of findings/
Confidence was decided based on the results of the AMSTAR 2 assessment, and the reviews were classified into four categories as follows: “high,” “moderate,” “low,” or “critically low.”
3) Bubble size: number of primary studies included in the SR.
Each SR bubble size is proportional to the number of primary studies included in the SR evaluating the effects of a particular intervention.
4) Circle color: effect estimate.
The clinical effectiveness of the rating of the authors' conclusions and overall ROB are described in the selected SR. Clinical effectiveness was categorized as a green circle if “effective” (if effect estimates were significantly positive and the overall ROB was low), a blue circle if “potentially effective” (if effect estimates were significantly positive but the overall ROB was high), or a yellow circle if “unclear” (if effect estimates were negative or the overall ROB was unclear).
Results
Study Selection
The database search identified 847 potentially relevant studies. The research yielded 432 articles after removing duplicates. After title and abstract screening, 146 articles were obtained for the final full-text review. In total, ninety-five SRs were identified for potential inclusion; however, after methodological analysis, only 48 had sufficient quality to be included (Figure 1). Among the forty-eight studies that met the inclusion criteria for use in the evidence map, forty-six bubbles representing the unlimited stage and two bubbles representing the acute stage were created.
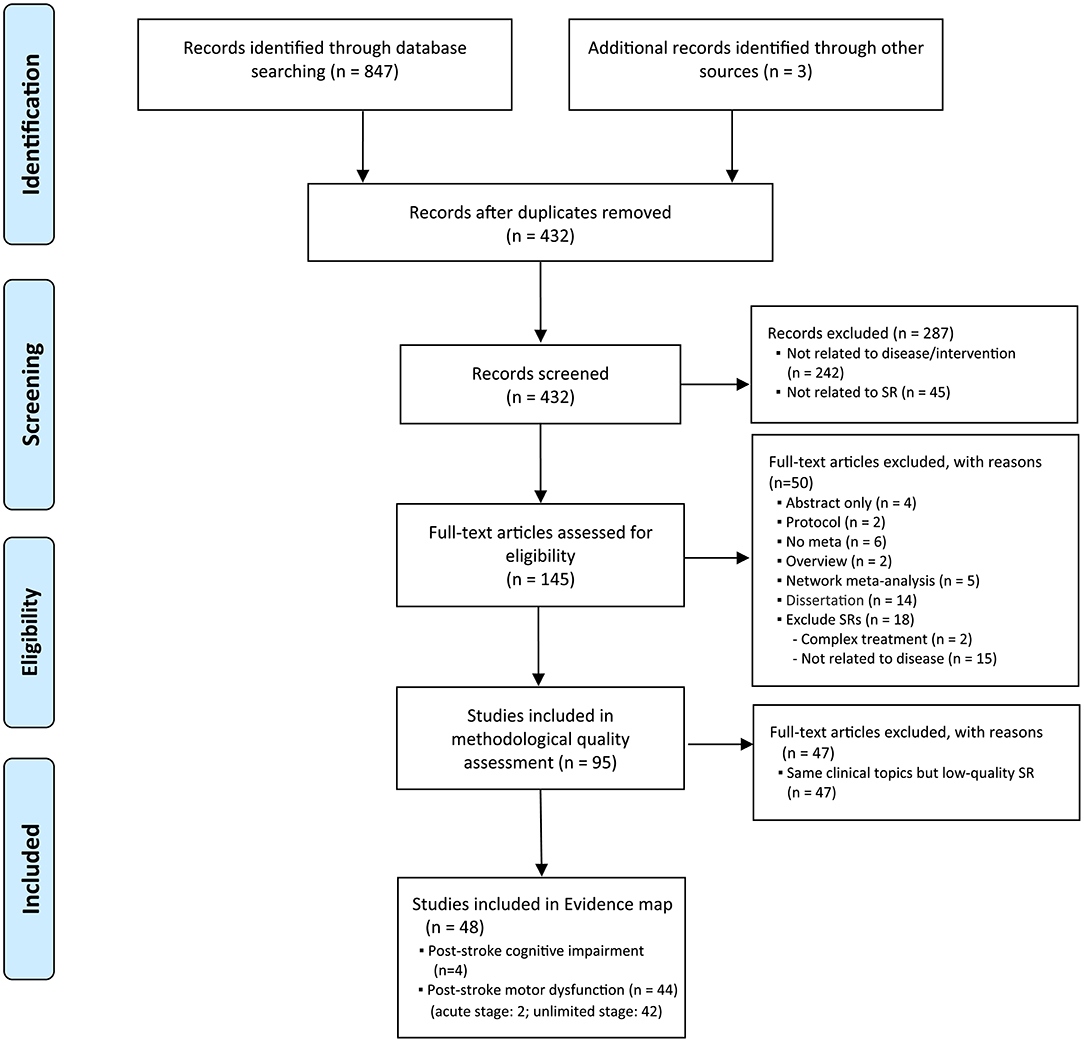
Figure 1. Study flow diagram. SR, systematic review.
Characteristics of the Included SRs
The forty-eight SRs (12–59) included a meta-analysis, and there were forty-five SRs from China and three SRs from Korea published between 2015 and 2021. There were thirty-six SRs published in Chinese, ten in English, and two in Korean. The main characteristics of the forty-eight SRs, including sample size, patient characteristics, interventions, and primary outcomes, are reported in Tables 1, 2. All the SRs contained only RCTs. The number of RCTs included in each SR ranged from 4 (18) to 41 (55). The number of patients included in each SR ranged from 310 (18) to 3,184 (20) adult individuals. The number of databases searched ranged from 2 to 12, and five SRs searched only the Chinese databases (27, 29, 31, 48, 59).
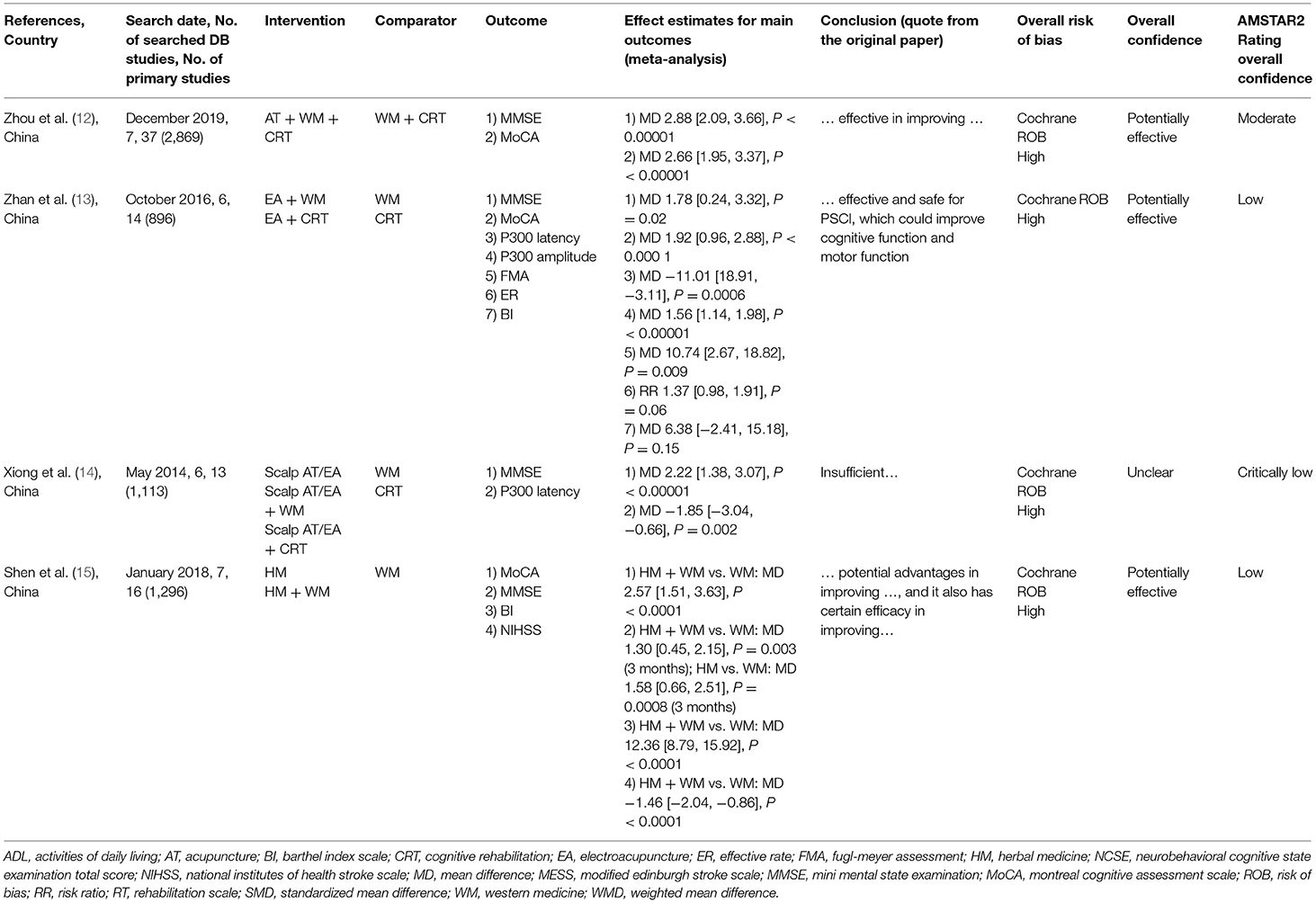
Table 1. Summary of the included systematic reviews of post-stroke cognitive impairment (PSCI).

Table 2. Summary of the included systematic reviews of post-stroke motor dysfunction.
Stroke Rehabilitative Symptoms Included
This article is based on multiple SRs. Four SRs focused on post-stroke cognitive impairment (Table 1), whereas the other 44 SRs focused on post-stroke motor function (Table 2), with shoulder–hand syndrome (n = 10) being the most frequent among them, followed by shoulder pain (n = 4), hand spasm (n = 1), strephenopodia (n = 1), motor dysfunction (n = 5), spasticity (n = 5), spastic hemiplegia (n = 9), hemiplegia (n = 8), and thalamic pain (n = 1).
Intervention Component Description
In total, nineteen different TCM intervention modalities were included: acupuncture (n = 11), EA (n = 5), eye acupuncture (n = 1), floating acupuncture (n = 2), fire-needle acupuncture (n = 2), Jin's three-needle acupuncture (n = 2), scalp acupuncture (n = 1), warm-needle acupuncture (n = 3), appoint catgut embedding (n = 1), bee venom acupuncture (n = 1), needle knife acupuncture (n = 1), moxibustion (n = 2), CHM (n = 5), herbal fumigation (n = 2), herbal socking (n = 1), taichi (n = 2), baduanjin (n = 1), daoyin (n = 1), and tuina (n = 4). Descriptions of the TCM interventions are described in Supplementary Table 2.
Quality of Included Systematic Reviews
Most SRs used the Cochrane handbook for risk or quality assessment. ROB was assessed by the Jadad scale in five SRs (29, 54, 55, 57, 59), while two SRs used the Joanna Briggs Institute's (JBI) critical appraisal tool (25), and two SRs used the Physiotherapy Evidence Database (PEDro) scale (34). Regarding quality assessment for evaluating the overall confidence level of each review, most studies showed moderate to critically low quality (Supplementary Table 3, Supplementary Figure 1). The lowest scores were on item 7 (none of the studies provided a list of excluded studies and justified the exclusions), item 2 (none of the studies reported justifications for any significant deviations from the protocol), and item 16 (5 studies did not report any potential sources of conflicts of interest). Overall confidence was rated as “moderate” for 8 SRs, “low” for 24 SRs, and “critically low” for 16 SRs.
Effectiveness
Overall confidence was considered with respect to overlapping diseases. The conclusions were reflected in individual SRs and confirmed through an internal review. We evaluated the effectiveness, literature size, and confidence level for each intervention identified in the SRs.
Effective
The effects of TCM interventions in stroke rehabilitation, indicated by statistically significant pooled treatment effects in an SR (n = 1) and based on a substantial number of research studies, included findings with acupuncture for shoulder–hand syndrome (20).
Potentially Promising Effects
Promising effects of TCM interventions in stroke rehabilitation, indicated by statistically significant pooled treatment effects in the SRs (n = 43) and based on a substantial number of research studies, included acupuncture for cognitive impairment (12), EA for motor dysfunction (36), CHM for spasticity (40), and moxibustion for hemiplegia (55). Most SRs reached the conclusion that there may be potential benefits of TCM interventions in stroke rehabilitation.
Unclear Effect
The map includes a small number of SRs (n = 4) that provided evidence of the potential lack of effectiveness of TCM interventions in stroke rehabilitation for clinical indications across more than one included study: scalp acupuncture for cognitive impairment (14), bee venom acupuncture for shoulder pain (18), warm-needle acupuncture for shoulder–hand syndrome (23), and eye-acupuncture for hemiplegia (52). These promising results are, however, compromised by the low-quality overall of the clinical trials. The identified reviews cautioned that firm conclusions cannot be drawn.
Evidence Map
Figure 2 presents the results of the evidence mapping process. The evidence map displays each of the 48 included SRs as 48 bubbles. As noted in the Materials and Methods Section, the bubble label represents the TCM intervention in that review. The bubble size represents the effect of the number of included primary studies in the context of stroke rehabilitation. Primary studies may have been included in multiple SRs. Each bubble was plotted based on the effect of the TCM intervention in stroke rehabilitation (color) in the space defined by the symptoms of stroke rehabilitation (x-axis) and the strength of the findings for the TCM intervention in stroke rehabilitation (y-axis). The evidence tables provide details of the included SRs (Tables 1, 2).
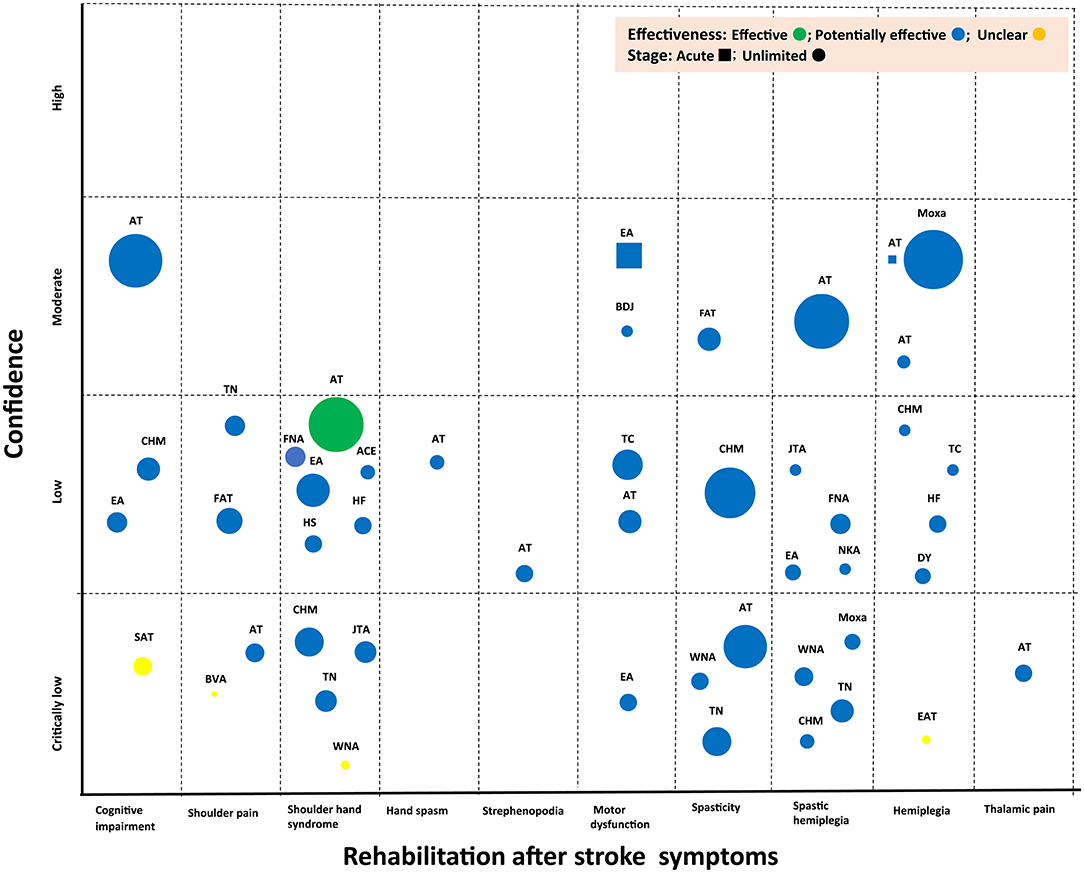
Figure 2. Evidence map of TCM for stroke rehabilitation. ACE, acupoint catgut embedding; AT, acupuncture; BDJ, Baduanjin; BVA, bee venom acupuncture; CHM, Chinese herbal medicine; DY, daoyin; EA: electroacupuncture; EAT, eyes acupuncture; FAT, floating acupuncture; FNA, fire-needle acupuncture; HF, herbal fumigation; HS, herbal socking; JTA, Jin's three-needle acupuncture; NKA, needle knife acupuncture; SAT, scalp acupuncture; TC, Taichi; TN, tuina; WNA, warm-needle acupuncture.
The SR authors concluded across the identified studies that TCM interventions in stroke rehabilitation improved outcomes of interest; however, the number of existing studies in the identified topic areas was small in all of the identified topic areas. The evidence mapping showed that only a limited number of TCM interventions have been assessed in stroke rehabilitation and that the clinical evidence for these interventions is inconclusive, indicating a need for more original research in this area (Figure 2).
Discussion
The 48 published SRs included in our evidence map provide a comprehensive overview of the evidence for TCM interventions in stroke rehabilitation published between 2015 and 2021. The evidence compiled by this overview indicated that TCM interventions (acupuncture, EA, CHM, moxibustion, etc.), in combination with conventional interventions, could improve cognitive and motor function. The results of this evidence map showed that in-line with available evidence, there is a sparsity of SRs evaluating TCM interventions in the context of stroke rehabilitation (cognitive and motor function). Furthermore, acupuncture can be more effective and safer than rehabilitation training in the treatment of post-stroke shoulder–hand syndrome (20). Some identified SRs included a large number of RCTs, but they addressed very broad topics, such as post-stroke motor dysfunction (32–36). On the other hand, evidence on the role of bee venom acupuncture in a number of specific conditions (post-stroke shoulder pain) is very limited due to the small number of published studies (18). The main beneficial treatment reported by the authors for patients with unlimited stage stroke was acupuncture with shoulder–hand syndrome. Evidence about the benefits of treatments for acute-stage stroke rehabilitation is lacking.
This evidence map describes the research foci that were reported in the existing SRs and displays the gaps in evidence so that areas that should be prioritized in future research can be identified. However, this evidence map is unable to answer more refined questions, such as what the best TCM interventions for specific applications and the differences between health services are. To advance our evidence-based knowledge of TCM, we should collect more data on the effectiveness of TCM for rehabilitating stroke symptoms and patient populations through meta-analyses across primary studies. In addition, the large number of treatments that were classified as having potential effectiveness warrants additional primary studies. More studies have been published in some of the areas of interest included in the unclear evidence category, and the currently available SRs must be updated. As there might be other efficient ways of drawing evidence maps, further research should also include developing evidence maps of other research designs.
The evidence map has several limitations. First, most publications are from mainland China and are written in Chinese, which eliminated their inclusion in this mapping of available evidence published in any other language. The generalization of these results to other countries might be limited. Second, the analysis was based on published SRs, and primary studies contributed to more than one included SR. Furthermore, individual review conclusions may have been limited by the quality of the primary studies and susceptible to publication and outcome reporting bias. There may be clinical trials that were included in more than one SR that might have an impact on the synthesized findings. Third, we attempted to retrieve possible eligible studies through comprehensive searches of numerous databases regardless of publication language, but there may have been missed trials related to this topic. Finally, the methodological quality of most included SRs scored “low” and “critically low.” More high-quality RCTs and SRs are needed to support clinical decision-making about the use of TCM interventions in stroke rehabilitation regimens. These findings highlight the need to conduct future research focusing on new treatments and addressing knowledge gaps in this field, and increased efforts are required to improve the methodological quality and reporting process of SRs on treatments to be used in stroke rehabilitation.
Stroke prevention and treatment remain a challenge worldwide. In China and Korea, many stroke patients are treated using traditional medicine, and there have been reports on their functional recovery (60, 61). Most alternative therapies are of unproven benefit in rehabilitation. Well-conducted trials are needed to better define the role of alternative therapies in the process of post-stroke recovery. In addition to future studies, better health education and rehabilitation services are also required.
Conclusion
This evidence map summarized, organized, and provided a visual overview of the currently available research volume and content related to TCM interventions during stroke rehabilitation involving cognitive function and motor function. This visualization facilitates an easy and engaging overview and suggests evidence mapping as a useful tool for a large array of stakeholders and for informing policy and clinical decision-makers. Our results provide policy and clinical decision-makers guidance regarding the interpretation of the current state of evidence regarding the effectiveness of TCM interventions in stroke rehabilitation.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author Contributions
T-YC and MSL conceptualized the study and wrote the original draft. T-YC, JHJ, and MSL contributed to methodology. T-YC and J-MY contributed to the software and resources. HWL and MCJ validated the study and investigated the study. T-YC and JHJ contributed to formal analysis. JHJ and HWL contributed to data curation. JHJ, HWL, J-MY, and MCJ contributed to writing, reviewing, and editing the manuscript. T-YC visualized the study. MCJ and MSL contributed to supervision and funding acquisition. HWL contributed to project administration. All the authors read and approved the final manuscript.
Funding
This study was supported by the Korea Health Industry Promotion Agency's Health and Medical Technology R&D Project (Grant No. HI20C1951) and the Korea Institute of Oriental Medicine (KSN2021210 and NHT2012480). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2022.885095/full#supplementary-material
References
1. Katan M, Luft A. Global burden of stroke. Semin Neurol. (2018) 38:208–11. doi: 10.1055/s-0038-1649503
2. Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, et al. Heart disease and stroke statistics-2018 update: a report from the American heart association. Circulation. (2018) 137:e67–492. doi: 10.1161/CIR.0000000000000573
3. Lattanzi S, Silvestrini M. Future challenges of stroke treatment. Neurol Neurochir Pol. (2018) 52:415–6. doi: 10.1016/j.pjnns.2018.02.004
4. Kim JY, Kang K, Kang J, Koo J, Kim D-H, Kim BJ, et al. Executive summary of stroke statistics in Korea. 2018: A report from the epidemiology research council of the Korean stroke society. J Stroke. (2019) 21:42–59. doi: 10.5853/jos.2018.03125
5. Hao CZ, Wu F, Shen J, Lu L, Fu DL, Liao WJ, et al. Clinical efficacy and safety of buyang huanwu decoction for acute ischemic stroke: a systematic review and meta-analysis of 19 randomized controlled trials. Evid Based Complement Alternat Med. (2012) 2012:630124. doi: 10.1155/2012/630124
6. Gong X, Sucher NJ. Stroke therapy in traditional Chinese medicine (TCM): prospects for drug discovery and development. Phytomedicine. (2002) 9:478–84. doi: 10.1078/09447110260571760
7. Hung CY, Wu XY, Chung VC, Tang EC, Wu JC, Lau AY. Overview of systematic reviews with meta-analyses on acupuncture in post-stroke cognitive impairment and depression management. Integr Med Res. (2019) 8:145–59. doi: 10.1016/j.imr.2019.05.001
8. Zhang X, Zhang X-F, Wang L, Guo D-Y, Zhang J-M, Chen Y-G, et al. Analysis of clinical efficacy of traditional chinese medicine in recovery stage of stroke: a systematic review and meta-analysis. Cardiovasc Ther. (2020) 2020:7172052. doi: 10.1155/2020/7172052
9. Miake-Lye IM, Hempel S, Shanman R, Shekelle PG. What is an evidence map? A systematic review of published evidence maps and their definitions, methods, and products. Syst Rev. (2016) 5:28. doi: 10.1186/s13643-016-0204-x
10. Solloway MR, Taylor SL, Shekelle PG, Miake-Lye IM, Beroes JM, Shanman RM, et al. An evidence map of the effect of Tai Chi on health outcomes. Syst Rev. (2016) 5:126. doi: 10.1186/s13643-016-0300-y
11. Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. (2017) 358:j4008. doi: 10.1136/bmj.j4008
12. Zhou L, Wang Y, Qiao J, Wang QM, Luo X. Acupuncture for improving cognitive impairment after stroke: a meta-analysis of randomized controlled trials. Front Psychol. (2020) 11:549265. doi: 10.3389/fpsyg.2020.549265
13. Zhan J, Wang XW, Cheng NF, Tang F. Electroacupuncture for post stroke cognitive impairment: a systematic review and meta-analyses. Chin Acupunct Moxibust. (2017) 37:1119–25. doi: 10.13703/j.0255-2930.2017.10.025
14. Xiong J, Liao WJ, Liu Q, Zhang Z, Guo Y, Xue L. Scalp acupuncture for improving cognitive dysfunction after stroke: a systematic review Chin J Rehabil Med. (2016) 31:333–9. doi: 10.3969/j.issn.1001-1242.2016.03.017
15. Shen W, Zeng ZX, Jin XL, Lu Y, Wang Y, Li SX, et al. Systematic evaluation of clinical efficacy and safety of traditional chinese medicine for post stroke cognitive impairment. Chin J Exp Trad Med Form. (2020) 26:185–93. doi: 10.13422/j.cnki.syfjx.20201151
16. Lin YF, Li Z, Fu JJ, Liu X. The systematic evaluation of acupuncture combined with rehabilitation training for the treatment of post-strokeshoulder pain. J Nurses Train. (2015) 30:1004–9. doi: 10.16821/j.cnki.hsjx.2015.11.011
17. Wei ZM, Sima ZF, Wu Q, Gong JQ. Systematic reviews of clinical effect of floating needle in the treatment of shoulder pain after stroke. J New Chin Med. (2019) 51:230–4. doi: 10.13457/j.cnki.jncm.2019.10.066
18. Lim SM, Lee SH. Effectiveness of bee venom acupuncture in alleviating post-stroke shoulder pain: a systematic review and meta-analysis. J Integr Med. (2015) 13:241–7. doi: 10.1016/S2095-4964(15)60178-9
19. Oh EW, Lee EJ. The effect of chuna manual therapy for shoulder pain in hemiplegic patients after stroke: a systematic review and meta-analysis. J Kor Med Rehabil. (2020) 30:89–101. doi: 10.18325/jkmr.2020.30.3.89
20. Liu S, Zhang CS, Cai Y, Guo X, Zhang AL, Xue CC, et al. Acupuncture for post-stroke shoulder-hand syndrome: a systematic review and meta-analysis. Front Neurol. (2019) 10:433. doi: 10.3389/fneur.2019.00433
21. Wang YN, Liu XP, Bao YH. Meta-analysis of electroacupuncture combined with rehabilitation training for shoulder-hand syndrome after stroke. Zhejiang J Integ Trad Chin West Med. (2019) 29:952–7. doi: 10.12102/ji.ssn.1672-1349.2020.11.028
22. Li JP, Zhang LX, He J. Systematic review of Jin's 3-needle therapy for shoulder hand syndrome after stroke. J Clin Acupunct Moxibust. (2016) 32:66–72.
23. An JJ. Systemic evaluation and meta-analysis on the effect of warming acupucture in the treatment of shoulder hand syndrome of stroke patients. Prac J Med Pharm. (2017) 34:22–6. doi: 10.14172/j.issn1671-4008.2017.01.008
24. Wu JY, Liu XQ, Gu JH, Li XT. System evaluation and meta-analysis on floating needle in treating shoulder-hand syndrome after stroke. J Guangzhou Univer Trad Chin Med. (2018) 35:637–43. doi: 10.13359/j.cnki.gzxbtcm.2018.04.014
25. Hou YC, Wang JZ, Fan JJ, Zhou Q, ZHang P, Hou PS. Acupoint catgut embedding for early post-stroke shoulder-hand syndrome:a systematic review and meta-analysis. Chin Evid Based Nurs. (2021) 7:174–81. doi: 10.12102/j.issn.2095-8668.2021.02.005
26. Lin WY, Li ZM, Li RQ, Wang M. Meta-analysis of massage on shoulder-hand syndrome after stroke. J Guangxi Univer Chin Med. (2017) 20:104–10.
27. Zheng YP, Zheng DP, Chen B. Effect of chinese herbal soaking on the shoulder-hand syndrome in patients after stroke: a meta-analysis. Chin Evid Based Nurs. (2020) 6:302–7.
28. Wang JR, Liu F, Ding YL, Yu LQ, Liu QY, Fang SZ. Systematic evaluation and meta-analysis of rehabilitation effect of traditional chinese medicine fumigation on shoulder-hand syndrome after stroke. Chin Manipul Rehabil Med. (2020) 11:52–7. doi: 10.15887/j.cnki.13-1389/r.2020.17.016
29. Guo LX, Ni W, Qi F, Ai K, Zhang H. Meta-analysis on clinical study of chinese medicine treatment of shoulder-hand syndrome. J Emerg Trad Chin Med. (2015) 24:390–3. doi: 10.3969/j.issn.1004-745X.2015.03.005
30. Qi CH, Xing X, Tian Y, Cui LH, Yuan Y, Liu SS, et al. Systematic review and meta-analysis of acupuncture treatment for post-stroke hand dysfunction. Shanghai J Acupunct Moxibust. (2018) 37:1444–50. doi: 10.13460/j.issn.1005-0957.2018.12.1444
31. Zhang Y, Fu LX, Wang F, Chen GQ, Li HF, Du YH. Systematic evaluation of acupuncture for the treatment of post-stroke strephenopodia. J Clin Acupunct Moxibust. (2016) 32:66–9.
32. Zhan HJ, Tan F, Cheng NF, Tan JQ. Efficacy of electroacupuncture for post-stroke motor dysfunction: a systematic review of randomized controlled trials. Chin Arch Trad Chin Med. (2016) 34:2117–21. doi: 10.13193/j.issn.1673-7717.2016.09.020
33. Lyu D, Lyu X, Zhang Y, Ren Y, Yang F, Zhou L, et al. Tai chi for stroke rehabilitation: a systematic review and meta-analysis of randomized controlled trials. Front Physiol. (2018) 9:983. doi: 10.3389/fphys.2018.00983
34. Zou LY, Wang CY, Chen XA, Wang HR. Baduanjin exercise for stroke rehabilitation: a systematic review with meta-analysis of randomized controlled trials. Int J Environ Res Public Health. (2018) 15:600. doi: 10.3390/ijerph15040600
35. Zheng Y, Liu WL, Shang GH, Wang X, Lin YJ, Lin MQ, et al. Meta-analysis of the curative effect of acupuncture and moxibustion in the treatment of motor dysfunction in patients with stroke. Chin J Rehabil Med. (2016) 31:217–21. doi: 10.3969/j.issn.1001-1242.2016.02.020
36. Zhan J, Pan RH, Zhou MC, Tan F, Huang Z, Dong J, et al. Electroacupuncture as an adjunctive therapy for motor dysfunction in acute stroke survivors: a systematic review and meta-analyses. BMJ Open. (2018) 8:e017153. doi: 10.1136/bmjopen-2017-017153
37. Ye T, Zhu LW, Tang Q. A meta-analysis of acupuncture combined with rehabilitation training for treatment of limb spasticity after stroke. Chin J Rehabil Med. (2017) 32:318–24. doi: 10.3969/j.issn.1001-1242.2017.03.015
38. Qiu X, Gao Y, Zhang Z, Cheng S, Zhang S. Fire acupuncture versus conventional acupuncture to treat spasticity after stroke: a systematic review and meta-analysis. PLoS ONE. (2021) 16:e0249313. doi: 10.1371/journal.pone.0249313
39. Yang L, Tan JY, Ma H, Zhao H, Lai J, Chen JX, et al. Warm-needle moxibustion for spasticity after stroke: a systematic review of randomized controlled trials. Int J Nurs Stud. (2018) 82:129–38. doi: 10.1016/j.ijnurstu.2018.03.013
40. Cai Y, Zhang CS, Liu S, Wen Z, Zhang AL, Guo X, et al. Add-on effects of chinese herbal medicine for post-stroke spasticity: a systematic review and meta-analysis. Front Pharmacol. (2019) 10:734. doi: 10.3389/fphar.2019.00734
41. Yan LF, Li JA, Zhu Y, Ma X, Jin HZ. Meta-analysis on tuina for treatment of spasm after stroke. J Basic Chin Med. (2015) 21:1566–8.
42. Fan W, Kuang X, Hu J, Chen X, Yi W, Lu L, et al. Acupuncture therapy for post-stroke spastic hemiplegia: a systematic review and meta-analysis of randomized controlled trials. Complement Ther Clin Pract. (2020) 40:101176. doi: 10.1016/j.ctcp.2020.101176
43. Li M, Wang EL. Systematic review and meta-analysis of electro-acupuncture therapy for spastic paralysis after stroke. Clin J Trad Chin Med. (2021) 33:268–74. doi: 10.16448/j.cjtcm.2021.0219
44. You JY, Rao Y, Liu FS, Chen M, Fang T, Jin YL. Fire needle therapy for spastic paralysis after stroke: a systematic review and meta-analysis. Chin J Basic Med Trad Chin Med. (2020) 26:229–34.
45. Xie YL, Fu EE, Yu ZA, Ye Y, Shao XN. Application of needle-knife in spastic paralysis after stroke: a meta-analysis. Clin J Trad Chin Med. (2020) 32:1274–8. doi: 10.16448/j.cjtcm.2020.0722
46. Yu L, Wu P. A meta-analysis of clinical effect of warm acupuncture on spastic hemiplegia patients after stroke. Chin Nurs Res. (2019) 33:2247–52. doi: 10.12102/j.issn.1009-6493.2019.13.014
47. Wen H, Xu XK, Tang CZ. Meta-analysis on the effect of temporal three-needle and spastic three-needle combined with rehabilitation training in the treatment of post-stroke spastic hemiplegia. Asia Pac Trad Med. (2020) 16:149–54. doi: 10.11954/ytctyy.202002050
48. Chen ZW, Tan ZH. Systematic review of stroke spastic hemiplegia patients treated by paeoniae-glycyrrhizae decoction. Yunnan J Trad Chin Med Mater Med. (2016) 37:23–7. doi: 10.16254/j.cnki.53-1120/r.2016.02.008
49. Ma HL, Yang L, Yang CC, Wang J, Xie LY, Liao QJ. Systematic review of randomization controlled trials on moxibustion for spastic paralysis after stroke patients. J Liaon Univer Trad Chin Med. (2017) 19:174–8. doi: 10.13194/j.issn.1673-842x.2017.01.051
50. Fan JH, Huang Y, Wang KL, Ma T, Lei LM. Analysis of massage cunative effect for the treatment of spastic hemiplegia after stroke from the perspectives of evidence-based medicine. J Basic Chin Med. (2016) 22:242–8.
51. Chen LZ, Wang JQ, Xu XF, Huang W, Long CX. Meta-analysis of randomized controlled clinical research on acupuncture treatment of post-stroke numbness. Chin Manipul Rehabil Med. (2020) 11:59. doi: 10.19787/j.issn.1008-1879.2020.09.001
52. Liu LY, Wang PQ. Meta analysis of efficacy for eye acupuncture on apoplectic hemiplegia. J Liaon Univer Trad Chin Med. (2017) 19:102–4. doi: 10.13194/j.issn.1673-842x.2017.02.031
53. Zhang L, Gu QF, Hu ML. A meta analysis of clinical effect of chinese herbal fumigation on hemiplegia after stroke. J Ne Chin Med. (2020) 52:15–8. doi: 10.13457/j.cnki.jncm.2020.11.004
54. Gou Y, Wu JG, Mo XN, Tan LX. Meta-analysis of randomized controlled trials of Buyang Huanwu decoction combined with acupuncture and Buyang Huanwu decoction for treatment of hemiplegia after apoplexy. Asia Pac Trad Med. (2019) 15:153–6. doi: 10.11954/ytctyy.201901054
55. Ji QL, Guan FQ. Meta-analysis of effects of moxibustion on limb motor function in patients with hemiplegia after stroke. China Med Pharm. (2020) 10:28–35.
56. Lee SH, Shin BC, Hwang EY, Heo I, Park SY, Hwang MS. Daoyin exercise therapy for stroke : a systematic review. J Korea CHUNA Manual Med Spine Nerves. (2019) 14:29–42. doi: 10.30581/jkcmm.2019.14.2.29
57. Wang C, Yang J, Wang RW, Zhang Y. A meta-analysis of short-term Taijiquan combined with conventional rehabilitation training in the treatment of stroke patients with hemiplegia and motor function. Chin J Rehabil Med. (2018) 33:1322–8. doi: 10.3969/j.issn.1001-1242.2018.11.014
58. Lin MQ, Liu WL. System review of the efficacy of acupuncture on hemiplegic gait in stroke patients. Rehabil Med. (2015) 25:54–62. doi: 10.3724/SP.J.1329.2015.01054
59. Bu J, Ren L. Meta-analysis of traditional Chinese medicine and acupuncture for treatment of thalamic pain after stroke. Chin Arch Trad Chin Med. (2017) 35:2036–8. doi: 10.13193/j.issn.1673-7717.2017.08.029
60. Leem J. Is acupuncture effective for functional recovery in ischemic stroke? Integr Med Res. (2015) 4:185–8. doi: 10.1016/j.imr.2015.07.001
Keywords: acupuncture, TCM, evidence map, evidence synthesis, overview, stroke rehabilitation, systematic review
Citation: Choi T-Y, Jun JH, Lee HW, Yun J-M, Joo MC and Lee MS (2022) Traditional Chinese Medicine Interventions in the Rehabilitation of Cognitive and Motor Function in Patients With Stroke: An Overview and Evidence Map. Front. Neurol. 13:885095. doi: 10.3389/fneur.2022.885095
Received: 27 February 2022; Accepted: 11 April 2022;
Published: 17 May 2022.
Edited by:
Aristide Merola, The Ohio State University, United StatesReviewed by:
Shaonan Liu, Guangdong Provincial Hospital of Chinese Medicine, ChinaJunmao Wen, Guangzhou University of Chinese Medicine, China
Jiansong Fang, Guangzhou University of Chinese Medicine, China
Copyright © 2022 Choi, Jun, Lee, Yun, Joo and Lee. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Myeong Soo Lee, drmslee@gmail.com