 Per Eriksson
Per Eriksson Oliver Skoglund
Oliver Skoglund Cecilia Hemgren
Cecilia Hemgren Christopher Sjöwall
Christopher Sjöwall- 1Department of Biomedical and Clinical Sciences, Division of Inflammation and Infection/Rheumatology, Linköping University, Linköping, Sweden
- 2Department of Internal Medicine, Division of Rheumatology, County Hospital Ryhov, Jönköping, Sweden
The Janus kinase (JAK)–STAT signaling pathway is relevant in both Takayasu and giant cell arteritis (GCA), and the use of JAK inhibitors (JAKi) in arthritis, psoriasis, and inflammatory bowel disease is nowadays common. Some evidence of the clinical efficacy of JAKi in GCA exists and a phase III randomized controlled trial (RCT) of upadacitinib is currently recruiting. In 2017, we started using barcitinib in a GCA patient with inadequate response to corticosteroids, and later on, we treated other 14 GCA patients with baricitinib/tofacitinib during intense follow-up. The retrospective data of these 15 individuals are here summarized. GCA was diagnosed based on the ACR criteria and/or imaging techniques combined with increased C-reactive protein (CRP) and/or erythrocyte sedimentation rate (ESR) followed by a good initial response to corticosteroids. JAKi was initiated based on inflammatory activity, with increased CRP, presumably dependent on GCA with clinical symptoms, despite unsatisfying high doses of prednisolone. The mean age at JAKi initiation was 70.1 years and the mean exposure to JAKi was 19 months. From initiation, significant reductions in CRP were seen already at 3 (p = 0.02) and 6 (p = 0.02) months. A slower decrease was observed regarding ESR at 3 (p = 0.12) and 6 (p = 0.02) months. Furthermore, the daily prednisolone doses were reduced at 3 (p = 0.02) and 6 (p = 0.004) months. No GCA relapses were observed. Two patients were affected by serious infections, but JAKi therapy was retained or reintroduced after recovery. We present encouraging observational data on JAKi in GCA in one of the hitherto largest case series with long-term follow-up. Our clinical experiences will complement the results from the awaited RCT.
Introduction
Giant cell arteritis (GCA) and Takayasu arteritis (TAK) constitute two different types of large vessel vasculitis (1). In the elderly, GCA is often localized to the temporal arteries. However, GCA may be more widespread than generally assumed including the arteries extending from the aortic arch (2). Aortitis without the inclusion of the temporal arteries may also occur. Temporal artery biopsy (TAB) is valuable for the diagnosis of GCA and was included in the 1990 American College of Rheumatology (ACR) classification criteria (3). More recent diagnostic tools, including ultrasound (US) and computed tomography (CT) with or without the addition of positron emission tomography (PET), have improved diagnostic performance (4).
Immunomechanistic studies of GCA and TAK have revealed that dendritic cells in the arterial wall attract T cells and macrophages, and subsequently, granulomatous inflammation is formed. Several cytokines are involved in this process, for example, interleukin (IL)-6, IL-17, TNF, and interferon (IFN)-γ (5, 6). In 2017, tocilizumab (TCZ; a humanized monoclonal antibody targeting the IL-6 receptor) proved to be efficient in a randomized controlled trial (RCT) of GCA (7). Nonetheless, potentially dangerous, IL-6-blocking regimens also diminish or abolish the increase of C-reactive protein (CRP) in cases with serious infections (8–11). Patients with GCA are often old and could have multiple comorbidities combined with increased susceptibility to infection, which may hamper the enthusiasm of using IL-6-blocking therapy.
Many cytokines bind to extracellular receptors. Intracellularly, the pro-inflammatory signal of IL-6 and many other cytokines is mediated by the Janus kinase (JAK)/STAT pathway, and JAK–STAT signaling has proved important in both TAK and GCA (12–14). JAKs are subdivided into JAK1, JAK2, JAK3, and TYK2, and the effects of different cytokine receptors are mediated by pairs of these JAKs. The JAK inhibitor (JAKi) tofacitinib is considered a pan-JAKi and has shown signs of efficacy in TAK (15, 16). In 2022, Rathore et al. published a systematic review of cohort studies and case reports using JAKi in TAK or GCA (17).
The JAKi baricitinib is more selective to JAK1 and JAK2, and baricitinib has been studied in 15 GCA patients in a pilot study with promising results (18, 19). Furthermore, there are only a few case series or case reports describing the performance of baricitinib in GCA (20–22). One case of GCA treated with upadacitinib has been reported, and a randomized phase III study of upadacitinib in GCA is ongoing (SELECT-GCA) (ClinicalTrials.gov; NCT03725202) (23). In addition, one case of GCA treated with ruxolitinib has also been published (24).
By tradition, treatment of GCA starts with corticosteroids. High doses are effective, but in some patients, tapering the dose is difficult without getting a rebound of inflammation. In 2017, we started using baricitinib in a GCA patient with inadequate response to corticosteroids and where the abolishment of CRP reaction by TCZ in case of infection would have caused problems. Since then, we have treated other 14 GCA patients (who had failed on corticosteroids and/or TCZ, or where IL-6-blocking regimen with TCZ was considered inappropriate due to increased risk of, or impaired ability to diagnose, infections) with baricitinib or tofacitinib for ≥6 months, and the retrospective data of these patients are summarized herein.
Methods
Subjects
All subjects were diagnosed with GCA if the 1990 ACR criteria were fulfilled and/or if patients had typical US features of arteritis characterized by hypo- or medium echogenic, homogeneous, circumferential wall thickening combined with increased levels of CRP and/or erythrocyte sedimentation rate (ESR) and initially a good clinical response to corticosteroids (2). Attribution of US features to GCA was considered in each patient at follow-up, and those with other definitive or potential causes of US findings were excluded. As an alternative to US, a CT scan showing increased arterial wall thickness, or positron emission tomography CT (PET-CT) showing increased uptake of radioactive glucose in the arterial wall, was considered a sign of inflammatory activity at diagnosis.
In this retrospective study from the Swedish Rheumatology Units at the University Hospital in Linköping and the County Hospital in Jönköping, 15 consecutive GCA patients treated for at least 6 months with JAKi were included, with 14 individuals treated with baricitinib. JAKi was initiated based on inflammatory activity suspected to depend on GCA, reflected by systemic inflammation and clinical symptoms, despite unsatisfying high doses of prednisolone. For evaluation of clinical efficacy, ≥6 months of JAKi therapy was required. Patients were followed from inclusion, at 3 and 6 months, and for most of the patients, there was at least one additional time point of assessment referred to as the “last follow-up.”
Assessments
The disease activity of GCA was evaluated by clinical investigation, including inflammatory parameters (CRP and ESR), and in two cases, imaging with US or CT was conducted. US is useful in the assessment of inflammatory activity in TAK, but the small arteries like the temporal artery are less studied (25). PET-CT was not used for the assessment of disease activity herein. All CRP levels below 5 mg/L were reported as 2.5 mg/L.
Outcomes
The composite outcome “therapeutical benefit” was reached in subjects without suspicion of clinical activity and with the absence of new GCA symptoms (suspected to be related to GCA) and decreasing or stable CRP combined with decreasing daily prednisolone dose at 3 and 6 months post-initiation of JAKi.
In addition, 6 months after the start of JAKi, two rheumatologists independently re-evaluated if the inflammatory activity at the initiation of JAKi was attributed to GCA or if other concomitant diseases had caused the inflammation. In the latter case, the patient was withdrawn from the study.
Relapse of GCA was defined as suspicion of clinical activity based on relevant symptoms and increasing CRP (in the absence of other concomitant diseases) leading to an increase of daily prednisolone dose.
Statistics
Data from patients exposed to JAKi were evaluated using the Wilcoxon signed-rank test to study changes over time in comparison with baseline values (SPSS software version 28.0.0.0; SPSS Inc., Chicago, IL, USA). In addition, descriptive statistics were used to display patient characteristics and laboratory values (Prism 9.3.1; GraphPad Software Inc., La Jolla, USA).
Ethics statement
The study complied with the ethical principles of the Declaration of Helsinki. Informed consent was obtained from all patients. In Sweden, drugs are allowed to be used off-label.
Results
Patient characteristics
The clinical data of the 15 participants are summarized in Table 1. The mean age at initiation of JAKi was 70.1 (range 61−80) years, and nine (60%) were women. All patients were of Caucasian origin. None of the included patients received any other disease-modifying anti-rheumatic drugs concomitantly with JAKi.
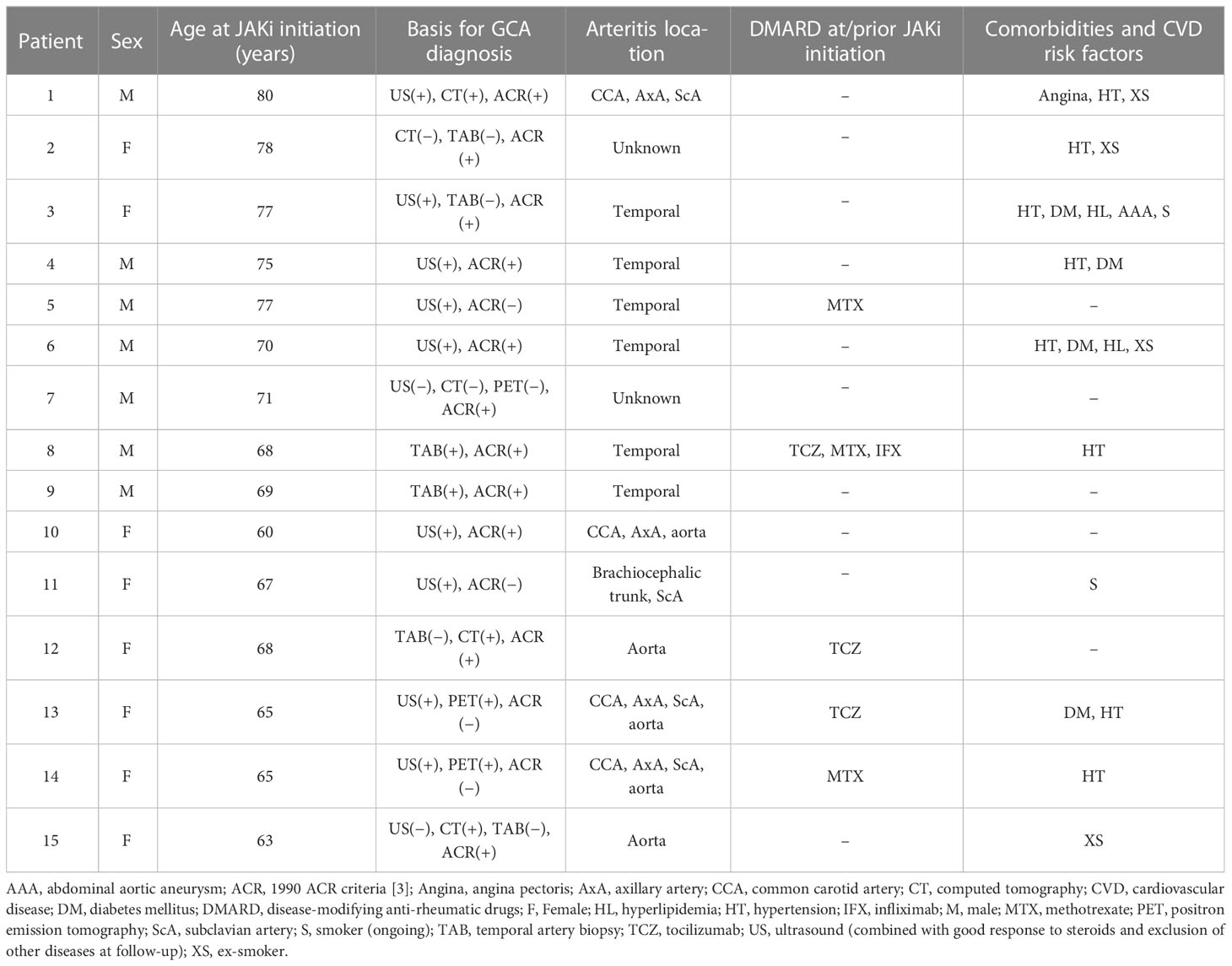
Table 1 Clinical background data of the 15 study participants with giant cell arteritis (GCA).
The mean time from GCA diagnosis to initiation of JAKi was 26.9 (range 0−80) months, and the clinical manifestations at the time point of JAKi initiation (baseline) are shown in Table 2. The mean daily dose of baricitinib was 3.86 (range 2−4) mg, and the patients receiving tofacitinib were prescribed 10 mg daily.

Table 2 Individual giant cell arteritis (GCA) features and therapeutic outcomes of JAKi for the 15 study participants.
Efficacy
The mean length of exposure to JAKi was 19 (range 6−38) months. From the initiation of JAKi, significant reductions of CRP were seen at 3 (p = 0.02) and 6 (p = 0.02) months, as well as at the last available follow-up date (p = 0.007) (Figure 1A). A slower decrease was observed regarding ESR at 3 (p = 0.12) and 6 (p = 0.02) months and at the last follow-up (p = 0.02) (Figure 1B). In addition, compared with baseline, the prednisolone doses were reduced at 3 (p = 0.02) and 6 (p = 0.004) months and at the last follow-up visit (p = 0.002) (Figure 1C).
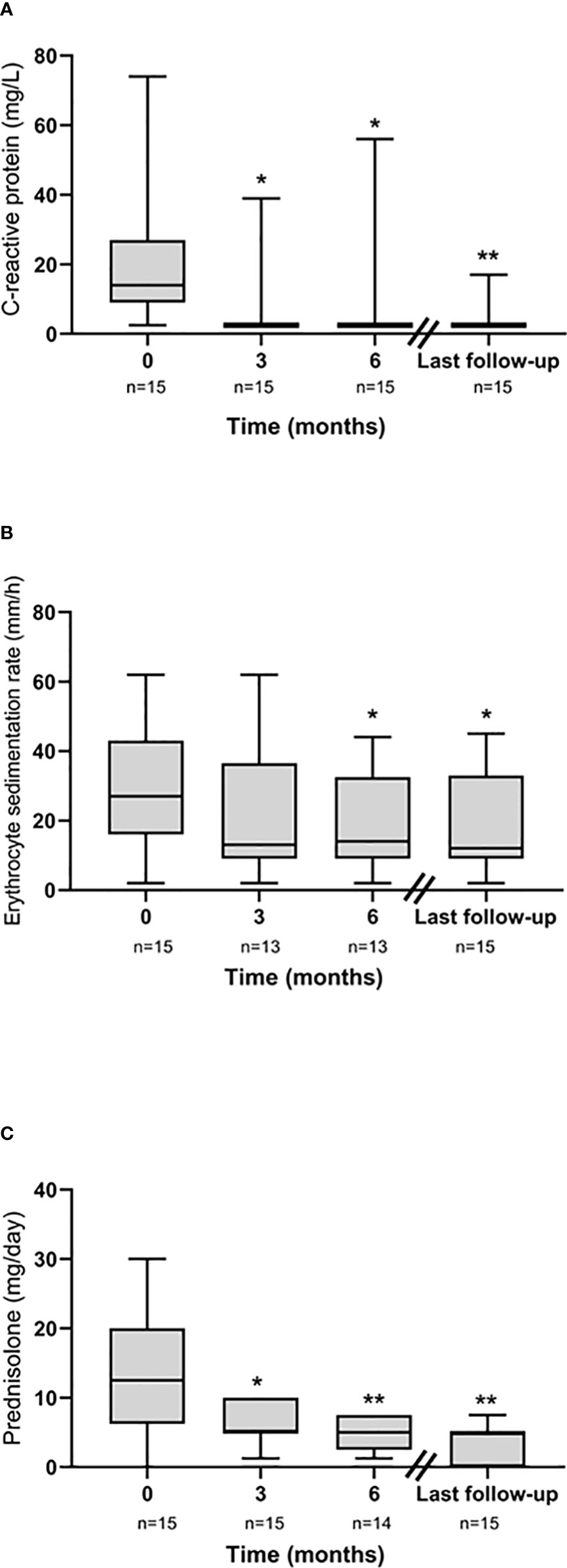
Figure 1 Longitudinal efficacy data from JAKi initiation (baseline) illustrated by (A) C-reactive protein (CRP), (B) erythrocyte sedimentation rate (ESR), and (C) daily prednisolone dose. *p < 0.05, **p < 0.01.
No GCA relapses were observed during the observed time. At the 3-month follow-up, 9 of 15 (60%) subjects fulfilled our definition of therapeutic benefit. This percentage increased at the 6-month follow-up when 11 of 15 (73%) individuals fulfilled the outcome of therapeutic benefit. At the last follow-up, 12 of 15 (80%) patients were still on daily treatment with JAKi. Three patients had ceased due to sustained remission after having been on the drug for more than 2 years (range 26−29 months) (Table 2). One of these patients experienced a GCA relapse with headache, jaw claudication, and temporal tenderness 1 month after ending JAKi. However, baricitinib 4 mg daily was reintroduced promptly in combination with a low dose of prednisolone (7.5 mg per day) to bring his symptoms under control. Consequently, he improved, and the remaining prednisolone could be tapered out over time.
Safety
During our study, no cases of malignancy nor gastrointestinal perforation were observed. Only minor effects were observed on blood cell counts over time (Figures 2A−C). Alterations of blood lipid profile, resulting in the initiation of statin therapy, were not observed in any subject. Moreover, no elevation of liver enzymes was seen, and no cases of herpes zoster were found. Nevertheless, two patients were affected by serious side effects (Aspergillus fumigatus infection and Enterococcus faecalis bacteremia, respectively). The first patient was a previously healthy 69-year-old man with GCA verified by TAB in 2020. One year later, before the initiation of baricitinib, he performed a chest CT which showed three pulmonary nodules. The nodules prompted a PET-CT, showing uptake of radioactive glucose considered a possible sign of malignancy. In February 2022 (1 month after the start of baricitinib), the size of the nodules had increased and begun to cavitate. Cultures from broncho-alveolar lavage at bronchoscopy showed A. fumigatus. Baricitinib was continued, and isavuconazonium was initiated, in parallel to rapidly decreasing doses of prednisolone, which led to improvement in pulmonary CT. The second patient was a 78-year-old lady with diabetes and hypertension. She had been prescribed tofacitinib for 20 months without prior episodes of infection when she was admitted to the hospital with 1 day’s duration of fevers and abdominal pain. CRP was increased (120 mg/ml) and abdominal CT showed dilated bile ducts. Enterococcus faecalis grew in blood cultures. The infection was successfully treated with piperacillin/tazobactam followed by amoxicillin/clavulanic acid. Tofacitinib was reintroduced to the patient as soon as she had ended the antibiotics.

Figure 2 Longitudinal safety data from JAKi initiation (baseline) illustrated by (A) hemoglobin concentration, (B) leukocyte count, and (C) platelet count. *p <0.05, **p < 0.01.
Dropouts
Aside from the 15 patients described above, three individuals were excluded from the case series as they did not prevail on JAKi for 6 months or had poor adherence to therapy.
One 85-year-old man was diagnosed with polymyalgia rheumatica in 2016. Two years later, a diagnosis of GCA was settled based on positive US findings. He also suffered from gout, recurrent infections, and chronic headaches. After 2 years, baricitinib was started in an attempt to treat headaches and systemic inflammation (increasing CRP levels). In a follow-up 2.5 months later, he had ceased baricitinib and did not notice any difference. At re-evaluation, GCA activity at the initiation of baricitinib was considered unlikely. Due to this, in combination with poor adherence to therapy, this patient was excluded from the study.
Another man was diagnosed with GCA in 2013 at the age of 74 years. Seven years later, relapse was suspected based on disturbed vision combined with a minor CRP elevation (7.5 mg/L). However, after re-evaluation 4 months later, retinal central venous occlusion per se without GCA activity was considered to explain his symptoms. Baricitinib was used for 4 months, but the patient was not included herein since attribution to GCA could not be confirmed.
Finally, a 77-year-old man with several comorbidities was diagnosed with GCA based on positive US findings and positive TAB in 2021. After 1 year on corticosteroids, baricitinib was added in order to reduce the prednisolone doses. Two months later, the patient developed shortness of breath, and a minor pulmonary embolus was observed on CT. He was treated with anticoagulation, baricitinib was ceased, and TCZ was initiated.
Discussion
This case series, including 15 Swedish individuals above the age of 60, provides an observational real-life experience of JAKi treatment in GCA for subjects where prednisolone alone was not sufficient or when the IL-6-blocking regimen was considered inappropriate. Our study population was highly selected since the subjects had failed on corticosteroids and that IL-6-blocking regimens such as TCZ were considered inappropriate due to a lack of CRP reaction in case of an infection. Still, the majority of the patients were able to decrease their daily corticosteroids significantly after the initiation of JAKi, and the beneficial effect remained over time. Although the prednisolone doses could be tapered, CRP values were stable or decreased, and the clinical status was improved or stable for all patients.
Overall, and as indicated in Table 2, JAKi was well tolerated in the 15 subjects who remained on JAKi for ≥6 months. The clinical efficacy of JAKi herein appeared to be similar to that reported by Koster et al. in their 52-week proof-of-concept study using baricitinib 4 mg/day for patients with relapsing GCA (19). We observed no additional safety issues.
Assessment of inflammatory activity in GCA is not always straightforward. US as well as CT and PET-CT can support the evaluation but must be combined with laboratory and clinical data. Especially in the elderly, concomitant diseases may indeed blur the clinical picture, as illustrated by the cases with Aspergillus infection starting subclinically before JAKi initiation and by the dropouts where concurrent comorbidities, such as gout, confounded the evaluation of the clinical efficacy.
Aside from the two serious infections described, pulmonary embolism was observed in one patient suffering from several comorbidities after only 2 months of exposure to baricitinib. Obviously, causality between JAKi and pulmonary embolism in this patient cannot be excluded. Increased incidence of venous thrombosis and pulmonary embolism has indeed been reported in patients with rheumatoid arthritis (RA) treated with JAKi, both by the Food and Drug Administration’s adverse event reporting system and the Swedish Rheumatology Quality registers (26, 27). With regard to other adverse events and despite careful follow-up, we observed surprisingly few side effects considering that most of our patients were monitored for more than 1 year. Experience from JAKi studies on RA indicates an association with lipid profile alterations, including both high-density and low-density lipoproteins (28, 29). However, among our 15 patients, this was not observed during follow-up.
This case series must be interpreted in the context of its limitations, e.g., the absence of relevant controls. In addition, the retrospective design of the study limits the possibility to draw firm conclusions regarding efficacy. However, given the fact that the participants had failed on corticosteroids and were judged inappropriate for TCZ, relevant comparators were impossible to find. In the RCT for TCZ in the Giant Cell Arteritis trial (GiACTA), the median daily prednisolone dose in the placebo group that underwent the 26-week steroid tapering was approximately 18 mg compared with 8 mg in our study population. However, this is indeed not a perfect comparator group, especially since the same placebo group in GiACTA had a GCA duration of 365 days compared with 804 days in our study.
Safety is important but particularly challenging in the elderly population. As a reflection of this, in TCZ in GiACTA, adverse events were observed in more than 95% of the participants both in the treatment and placebo study arms (7). Another limitation of the current case series is the lack of a systematic follow-up with US or other imaging techniques. At least in arteries with a larger size than the temporal arteries, US could have given valuable information regarding the temporal development of inflammatory activity in GCA. In contrast, a major strength is the Swedish healthcare system, which is public and tax-funded and offers universal access. This significantly reduces the risk of selection bias and ensures a very high coverage of cases. Furthermore, in Sweden, existing drugs are allowed to be used off-label which is not the case for all countries.
To conclude, in line with the pilot study by Koster et al. and several independent observations, we report the encouraging efficacy data of JAKi in GCA (17, 19). The safety was comparable with prior reports in GCA. In the absence of published randomized controlled trials, clinical experience regarding efficacy and safety is important to convey to colleagues. This is one of the hitherto largest case series of JAKi in GCA with longer follow-up compared with existing reports. The clinical experiences of efficacy and safety reported by Koster et al. and us will complement the results from the awaited RCT and indicate that JAKi could be a therapeutic option in subjects with multiple comorbidities where high doses of corticosteroids and/or TCZ are considered inappropriate.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
PE: original idea, patient characterization, manuscript writing, and supervision. OS: patient characterization, manuscript writing, and statistics. CH: patient characterization and manuscript writing. CS: patient characterization, manuscript writing, and supervision. All authors reviewed the manuscript and approved the final version.
Funding
This work was supported by grants from the Swedish Rheumatism Association, the Region Östergötland (ALF Grants), the Gustafsson Foundation, the King Gustaf V’s 80-year Anniversary Foundation, and the King Gustaf V and Queen Victoria’s Freemasons Foundation.
Acknowledgments
Associate Professor Jonas Wetterö is acknowledged for valuable feedback on the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, et al. 2012 revised international chapel hill consensus conference nomenclature of vasculitides. Arthritis Rheum (2013) 65(1):1–11. doi: 10.1002/art.37715
2. Skoog J, Svensson C, Eriksson P, Sjöwall C, Zachrisson H. The diagnostic performance of an extended ultrasound protocol in patients with clinically suspected giant cell arteritis. Front Med (Lausanne) (2021) 8:807996. doi: 10.3389/fmed.2021.807996
3. Hunder GG, Bloch DA, Michel BA, Stevens MB, Arend WP, Calabrese LH, et al. The American college of rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum (1990) 33(8):1122–8. doi: 10.1002/art.1780330810
4. Haaversen AB, Brekke LK, Bakland G, Rødevand E, Myklebust G, Diamantopoulos AP. Norwegian Society of rheumatology recommendations on diagnosis and treatment of patients with giant cell arteritis. Front Med (Lausanne) (2022) 9:1082604. doi: 10.3389/fmed.2022.1082604
5. Zhang H, Watanabe R, Berry GJ, Tian L, Goronzy JJ, Weyand CM. Inhibition of JAK-STAT signaling suppresses pathogenic immune responses in medium and Large vessel vasculitis. Circulation (2018) 137(18):1934–48. doi: 10.1161/circulationaha.117.030423
6. Pugh D, Karabayas M, Basu N, Cid MC, Goel R, Goodyear CS, et al. Large-Vessel vasculitis. Nat Rev Dis Primers. (2022) 7(1):93. doi: 10.1038/s41572-021-00327-5
7. Stone JH, Tuckwell K, Dimonaco S, Klearman M, Aringer M, Blockmans D, et al. Trial of tocilizumab in giant-cell arteritis. N Engl J Med (2017) 377(4):317–28. doi: 10.1056/NEJMoa1613849
8. Chalaris A, Garbers C, Rabe B, Rose-John S, Scheller J. The soluble interleukin 6 receptor: generation and role in inflammation and cancer. Eur J Cell Biol (2011) 90(6-7):484–94. doi: 10.1016/j.ejcb.2010.10.007
9. Sjöwall C, Ernerudh J, Bengtsson AA, Sturfelt G, Skogh T. Reduced anti-TNFalpha autoantibody levels coincide with flare in systemic lupus erythematosus. J Autoimmun (2004) 22(4):315–23. doi: 10.1016/j.jaut.2004.02.003
10. Lally L, Forbess L, Hatzis C, Spiera R. Brief report: a prospective open-label phase IIa trial of tocilizumab in the treatment of polymyalgia rheumatica. Arthritis Rheumatol (2016) 68(10):2550–4. doi: 10.1002/art.39740
11. Rose-John S. Blocking only the bad side of IL-6 in inflammation and cancer. Cytokine (2021) 148:155690. doi: 10.1016/j.cyto.2021.155690
12. Deng J, Younge BR, Olshen RA, Goronzy JJ, Weyand CM. Th17 and Th1 T-cell responses in giant cell arteritis. Circulation (2010) 121(7):906–15. doi: 10.1161/circulationaha.109.872903
13. Régnier P, Le Joncour A, Maciejewski-Duval A, Desbois AC, Comarmond C, Rosenzwajg M, et al. Targeting JAK/STAT pathway in takayasu's arteritis. Ann Rheum Dis (2020) 79(7):951–9. doi: 10.1136/annrheumdis-2019-216900
14. Watanabe R, Hashimoto M. Perspectives of jak inhibitors for Large vessel vasculitis. Front Immunol (2022) 13:881705. doi: 10.3389/fimmu.2022.881705
15. Li J, Li M, Tian X, Zeng X. Tofacitinib in patients with refractory takayasu's arteritis. Rheumatol (Oxford) (2020) 59(11):e95–e8. doi: 10.1093/rheumatology/keaa281
16. Kong X, Sun Y, Dai X, Wang L, Ji Z, Chen H, et al. Treatment efficacy and safety of tofacitinib versus methotrexate in takayasu arteritis: a prospective observational study. Ann Rheum Dis (2022) 81(1):117–23. doi: 10.1136/annrheumdis-2021-220832
17. Rathore U, Thakare DR, Patro P, Agarwal V, Sharma A, Misra DP. A systematic review of clinical and preclinical evidences for janus kinase inhibitors in large vessel vasculitis. Clin Rheumatol (2022) 41(1):33–44. doi: 10.1007/s10067-021-05973-4
18. Damsky W, Peterson D, Ramseier J, Al-Bawardy B, Chun H, Proctor D, et al. The emerging role of janus kinase inhibitors in the treatment of autoimmune and inflammatory diseases. J Allergy Clin Immunol (2021) 147(3):814–26. doi: 10.1016/j.jaci.2020.10.022
19. Koster MJ, Crowson CS, Giblon RE, Jaquith JM, Duarte-García A, Matteson EL, et al. Baricitinib for relapsing giant cell arteritis: a prospective open-label 52-week pilot study. Ann Rheum Dis (2022) 81(6):861–7. doi: 10.1136/annrheumdis-2021-221961
20. Camellino D, Dejaco C, Giusti A, Martini F, Cosso R, Girasole G, et al. Ab0379 baricitinib in polymyalgia rheumatica and giant cell arteritis: report of six cases. Ann Rheumatic Dis (2021) 80(Suppl 1):1216–7. doi: 10.1136/annrheumdis-2021-eular.3435
21. Régent A, Terrier B, Legendre P, Wartski M, Cohen P, Mouthon L, et al. Efficacy of baricitinib for refractory large-vessel vasculitis. Rheumatol (Oxford) (2021) 60(11):e389–e91. doi: 10.1093/rheumatology/keab541
22. Prigent K, Aouba A, Aide N, de Boysson H. JAK inhibitor effectiveness in giant-cell arteritis with Large-vessel involvement assessed by 18F-FDG PET-CT. Clin Nucl Med (2022) 47(3):234–5. doi: 10.1097/rlu.0000000000003913
23. Sanada A, Abe N, Bohgaki M, Kasahara H. Therapeutic effectiveness of upadacitinib combined with glucocorticoid on remission induction and maintenance in giant cell arteritis. Rheumatol (Oxford) (2022) 61(9):e274–e6. doi: 10.1093/rheumatology/keac203
24. Herlihy N, Curto-Garcia N, O'Sullivan J, Radia D, McLornan D, Pye S, et al. Successful treatment of chronic neutrophilic leukaemia and associated giant cell arteritis with the combination of ruxolitinib and azacytidine. Supplement Article Br J Haematol (2019) 185(S1):3–202. doi: 10.1111/bjh.15854
25. Svensson C, Eriksson P, Zachrisson H. Vascular ultrasound for monitoring of inflammatory activity in takayasu arteritis. Clin Physiol Funct Imaging (2020) 40(1):37–45. doi: 10.1111/cpf.12601
26. Dong Z, Ye X, Chen C, Wang R, Liu D, Xu X, et al. Thromboembolic events in janus kinase inhibitors: a pharmacovigilance study from 2012 to 2021 based on the food and drug administration's adverse event reporting system. Br J Clin Pharmacol (2022) 88(9):4180–90. doi: 10.1111/bcp.15361
27. Molander V, Bower H, Frisell T, Delcoigne B, Di Giuseppe D, Askling J. Venous thromboembolism with JAK inhibitors and other immune-modulatory drugs: a Swedish comparative safety study among patients with rheumatoid arthritis. Ann Rheum Dis (2023) 82(2):189–97. doi: 10.1136/ard-2022-223050
28. Genovese MC, Kremer J, Zamani O, Ludivico C, Krogulec M, Xie L, et al. Baricitinib in patients with refractory rheumatoid arthritis. N Engl J Med (2016) 374(13):1243–52. doi: 10.1056/NEJMoa1507247
29. Fleischmann R, Schiff M, van der Heijde D, Ramos-Remus C, Spindler A, Stanislav M, et al. Baricitinib, methotrexate, or combination in patients with rheumatoid arthritis and no or limited prior disease-modifying antirheumatic drug treatment. Arthritis Rheumatol (2017) 69(3):506–17. doi: 10.1002/art.39953
Keywords: large vessel vasculitis, giant cell (temporal) arteritis, Janus kinase inhibitor (JAKI), baricitinib, inflammation, corticosteroids, interleukin - 6, therapy -
Citation: Eriksson P, Skoglund O, Hemgren C and Sjöwall C (2023) Clinical experience and safety of Janus kinase inhibitors in giant cell arteritis: a retrospective case series from Sweden. Front. Immunol. 14:1187584. doi: 10.3389/fimmu.2023.1187584
Received: 16 March 2023; Accepted: 10 May 2023;
Published: 25 May 2023.
Edited by:
Ryu Watanabe, Osaka Metropolitan University, JapanReviewed by:
Shuji Sumitomo, Kobe City Medical Center General Hospital, JapanEamonn Molloy, St Vincent’s University Hospital, Ireland
Copyright © 2023 Eriksson, Skoglund, Hemgren and Sjöwall. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christopher Sjöwall, christopher.sjowall@liu.se