 Sylvère Störmann1*†
Sylvère Störmann1*† Sebastian M. Meyhöfer2,3†
Sebastian M. Meyhöfer2,3† Jan B. Groener4†Johanna Faust5
Jan B. Groener4†Johanna Faust5 Katharina Schilbach1†
Katharina Schilbach1† Jochen Seufert6†
Jochen Seufert6† Bruno Vergès7,8†
Bruno Vergès7,8†- 1Medizinische Klinik und Poliklinik IV, LMU Klinikum, Ludwig-Maximilians-Universität München, Munich, Germany
- 2Institute for Endocrinology & Diabetes, University of Lübeck, Lübeck, Germany
- 3German Centre for Diabetes Research (DZD), Munich-Neuherberg, Germany
- 4Zentrum für Diabetes und Hormonerkrankungen Neustadt, Neustadt, Germany
- 5Medicover Neuroendocrinology, Munich, Germany
- 6Klinik für Innere Medizin II, Universitätsklinikum Freiburg, Medizinische Fakultät, Albert-Ludwigs-Universität Freiburg, Freiburg, Germany
- 7Endocrinology Diabetics and Metabolic Disorders Department, Dijon University Hospital, Dijon, France
- 8French National Health and Medical Research Body Unit, Lipid-Nutrition-Cancer-1231, University of Burgundy, Dijon, France
Pasireotide is a somatostatin analogue for the treatment of acromegaly, a chronic condition caused by excess growth hormone. Despite the therapeutic benefits of pasireotide as a second-line treatment for inadequately controlled acromegaly, a major concern is its hyperglycemic side-effect. Here, we provide guidance on how to select appropriate patients with acromegaly for treatment with pasireotide. We summarize baseline characteristics of patients at high risk for pasireotide-associated hyperglycemia and recommend a monitoring strategy based on the risk profile. Self-monitoring of blood glucose levels (SMBG), measurements of fasting plasma glucose (FPG), postprandial plasma glucose (PPG) and regular HbA1c measurements are the foundation of our proposed monitoring approach. The pathophysiology of pasireotide-induced hyperglycemia involves decreased secretion of the incretin hormones GIP (glucose-dependent insulinotropic polypeptide) and GLP-1 (glucagon-like peptide-1). Our expert recommendations address the specific pathophysiology of pasireotide-induced hyperglycemia by recommending the incretin-based therapeutics dipeptidyl peptidase-4 inhibitors (DPP-4i) and glucagon-like peptide-1 receptor agonists (GLP-1 RA) in all appropriate patients as an alternative to first-line monotherapy with metformin. Furthermore, we emphasize the importance of adequate control of acromegaly, excellent diabetes education, nutrition and lifestyle guidance and advise to consult expert diabetologists in case of uncertainty in the management of patients with hyperglycemia under pasireotide.
1 Introduction
Acromegaly is a chronic systemic disease due to an excess of growth hormone (GH) and insulin-like growth factor I (IGF-I), mainly caused by a GH-secreting pituitary adenoma (somatotropinoma). Chronic GH excess leads to numerous systemic sequelae, including cardiovascular disease, osteoarthropathy, metabolic complications, respiratory disease, increased risk for some neoplasms, vertebral fractures, reduced quality of life, and hypopituitarism (1). Growth hormone affects glucose tolerance by an increase in glucose concentrations and insulin resistance due to a bimodal effect on carbohydrate metabolism: On the one hand, GH stimulates beta cell proliferation and insulin synthesis and secretion; on the other hand, it counteracts insulin action and increases lipolysis (2). GH increases glycogenolysis and thus enhances hepatic glucose production (3). Additionally, it counteracts the effects of insulin in the liver. It also impairs muscle glucose uptake and glycogen synthesis, without affecting glucose oxidation (4). Furthermore, GH promotes lipid mobilization and oxidation in adipose tissue and inhibits lipogenesis, counter-acting insulin action. The GH-induced rise in free fatty acids (FFAs) further reduces insulin sensitivity. GH also stimulates inflammation of adipose tissue and induces adipokine secretion, which is though to contribute to systemic insulin resistance in acromegaly (4). Insulin resistance (IR), hyperglycemia and diabetes are therefore common comorbidities of acromegaly and diabetes mellitus prevalence in acromegaly ranges from 16% to 56%, with some patients only having prediabetes (impaired glucose tolerance [IGT] or impaired fasting glucose [IFG]). Less than 30% of patients maintain normoglycemia (5). Despite differing pathophysiology, acromegaly-related diabetes mellitus presents similarly to type 2 diabetes mellitus (T2DM) (2).
Somatostatin, an endogenous peptide hormone, binds to all five somatostatin receptor subtypes (SSTR1 to SSTR5) and physiologically inhibits GH secretion (6). SSTR2 and SSTR5 are highly expressed in somatotroph pituitary adenomas and neuroendocrine tumors and are key targets for pharmacological treatment (7). The first-generation somatostatin receptor ligands, octreotide and lanreotide, are currently the mainstay of acromegaly medical treatment, achieving biochemical control in approximately 40% of patients and tumor shrinkage in over 60% of patients (8). Pasireotide is a second-generation somatostatin analogue (SSA) approved for the treatment of acromegaly. While the first-generation somatostatin analogues, octreotide and lanreotide, act primarily by binding to SSTR2, pasireotide binds with high affinity to the somatostatin receptor subtypes SSTR1, SSTR2, SSTR3 and SSTR5 (9, 10). Pasireotide has a 30- to 40-fold higher affinity for SSTR5 and lower affinity for SSTR2 compared with octreotide, which is why pasireotide has been attributed with potentially greater clinical efficacy in acromegaly than first-generation SSA (9, 11, 12). A study of pasireotide versus octreotide (C2305) in 358 patients with medically naïve acromegaly found biochemical disease control, defined as GH < 2.5 µg/L and IGF-I within the age-related reference interval at 12 months, significantly more often in patients treated with pasireotide (31.3% vs 19.2%; p = 0.007) (13). Another trial (C2402; PAOLA) showed 15-20% of patients inadequately controlled on high doses of octreotide and lanreotide achieved biochemical control after switching to pasireotide 40 mg or 60 mg (14). A retrospective single-center study found pasireotide LAR normalized IGF-I levels in ~54% of acromegaly at least partially resistant to first-generation SSA (15). Using more stringent criteria of biochemical control, in an open-label study of patients with uncontrolled acromegaly on first-generation SSA 18 of 123 patients (14.6%) achieved strict biochemical control with pasireotide (16). Current guidelines and recommendations for the treatment of acromegaly consider long-acting-release pasireotide as a second-line treatment for patients resistant to first-generation SSA and after failure of surgery (17, 18).
Despite pasireotide’s benefits as a second line treatment for uncontrolled acromegaly, one major concern stems from its hyperglycemic side effect. The mechanistic aspects of hyperglycemia induced by pasireotide have been extensively studied and may be attributed to the different binding profiles of pasireotide and octreotide to somatostatin receptors. SSTR5, highly expressed in pancreatic beta cells, inhibits insulin secretion when activated. On the other hand, activation of SSTR2 which is strongly expressed in pancreatic alpha cells mainly inhibits glucagon secretion (9, 19). Consistent with pasireotide’s lower affinity for SSTR2 and higher affinity for SSTR5, hyperglycemia is attributed to reductions in insulin secretion with only mild inhibition of glucagon secretion (11, 20–22). Pasireotide also decreases secretion of the incretin hormones GIP (glucose-dependent insulinotropic polypeptide) and GLP-1 (glucagon-like peptide-1) without altering hepatic or peripheral insulin sensitivity, rendering antihyperglycemic drugs with incretin-based mechanism of action interesting candidates justified by pathophysiology for the treatment of pasireotide-associated hyperglycemia or diabetes (20, 21). Limited clinical data and practice approaches are available on the treatment of pasireotide-induced hyperglycemia, which include frequent monitoring of glucose levels, especially during initiation of treatment, and early and aggressive antidiabetic medical treatment to prevent alterations in glucose homeostasis (23, 24). Hyperglycemia usually occurs early, usually within the first 3 months of treatment (23). However, in rare cases, hyperglycemia may occur at a later time point during pasireotide therapy (25).
Table 1 gives an overview of the prevalence of pasireotide-induced hyperglycemia and diabetes in clinical studies in patients with acromegaly, comparing it with baseline data where possible. Due to varying study populations and methodologies, results are diverse. Generally, irrespective of baseline status, 60-90% of acromegaly patients treated with pasireotide experience hyperglycemia, and 40-70% have diabetes.
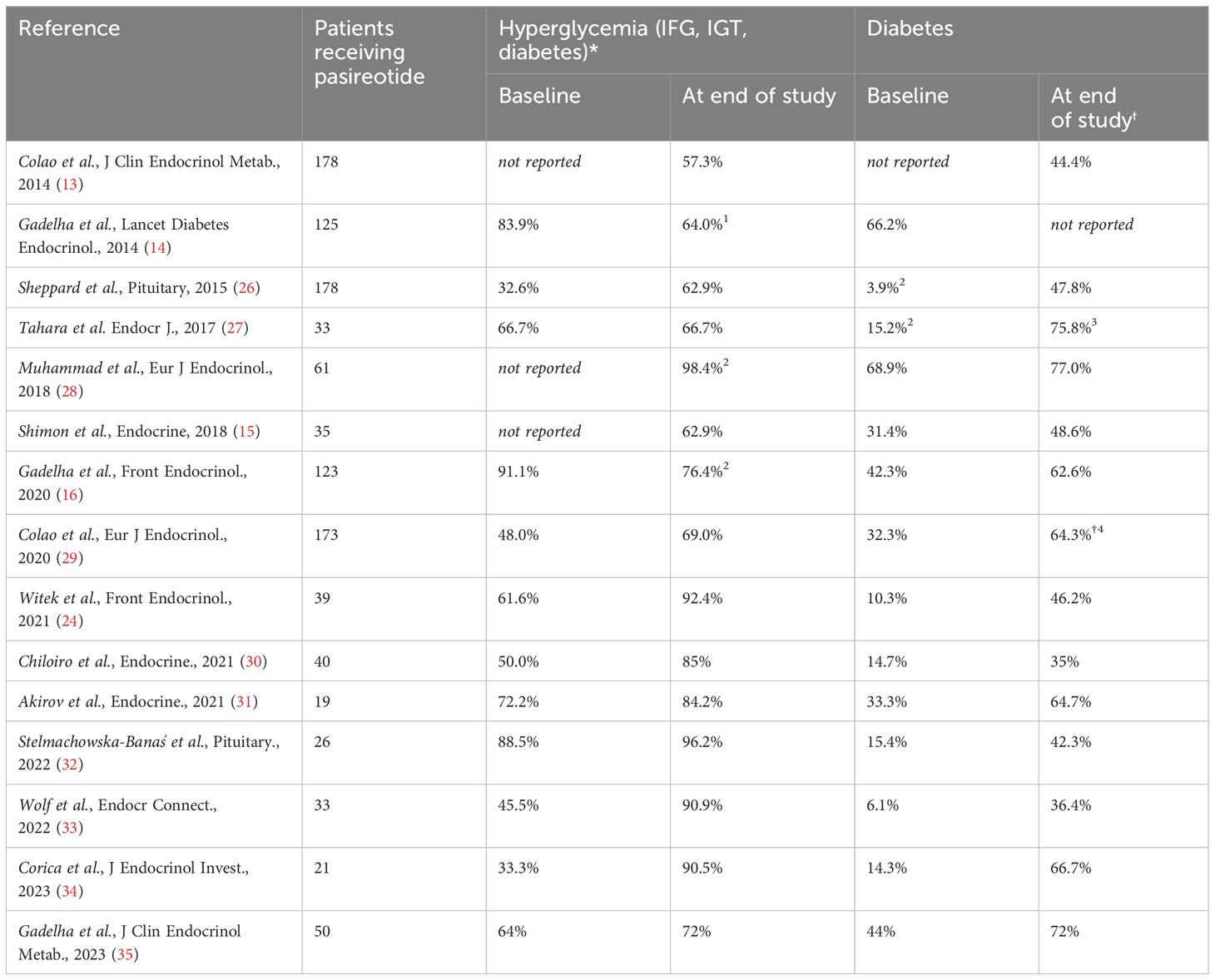
Table 1 Occurrence of hyperglycemia-related adverse events and diabetes in clinical studies of acromegaly patients treated with pasireotide and comparison with baseline data.
Diabetes in patients with acromegaly often results in higher morbidity and mortality (36). Although hyperglycemia is a common side effect of pasireotide treatment, recommendations based on expert consensus have only been published for patients with Cushing’s disease, but not for patients with acromegaly (37, 38). Even though there are some similarities, there are inherent differences between Cushing’s disease and acromegaly and their impact on glycemic status. Thus, expert recommendations derived from consensus discussions on managing pasireotide-induced hyperglycemia in acromegaly patients are crucial and urgently needed.
2 Methods
In May 2022 endocrinologists and diabetologists with expertise in the treatment of patients with acromegaly convened in Munich to discuss approaches to the management of hyperglycemia in patients with acromegaly treated with pasireotide. To identify relevant data, comprehensive literature searches were conducted prior to that meeting using the PubMed database. All published articles satisfying the search terms “pasireotide” and “acromegal*” were assembled (n = 281). All titles and abstracts were screened for relevance: Articles focusing on or at least mentioning glucose metabolism in pasireotide treatment. If an article’s relevance couldn’t be determined from the title and abstract alone, the article was skimmed or read to identify potentially relevant passages. The selected articles (n = 76) were read, summarized, and critically appraised, with key findings being extracted for in-depth discussion.
The entire group received brief plenary overviews on the current state of the field and the specific topics assigned to each participant. Subsequently, the participants collectively evaluated and intensively discussed the optimal strategy and supporting evidence. In the wake of the Munich assembly, additional virtual meetings were organized using standard web conference software. At each iteration, the current state of the recommendations was summarized highlighting unresolved issues. Consensus was finally found and formulated based on the availability of evidence and its quality. Where no evidence was available, expert recommendations were agreed upon when consensus could be reached. All meeting participants approved the final recommendations.
3 Patient selection for the treatment of acromegaly with pasireotide
Specific indicators may predict the response to first-generation somatostatin analogues or pasireotide, summarized in Table 2 (12, 18). The efficacy of somatostatin analogs in somatotroph adenomas is influenced by SSTR2 and SSTR5 expression, consistent with differences in the affinity of pasireotide compared with first-generation SSA. While high SSTR2 density is a good predictor of first-generation SSA efficacy, a high SSTR5/SSTR2 ratio favors pasireotide (39, 40). A hypointense T2-weighted MRI (magnetic resonance imaging) signal of somatotroph adenomas indicates a high percentage of IGF-I reduction with first-generation SSA treatment, whereas hyperintense T2 signals correlate with positive pasireotide response (40, 41). Granulation patterns of somatotroph adenomas are related to T2-weighted MRI signals and may also be used to predict the response to SSA: densely granulated somatotropinomas typically show hypointense T2 signals, whereas sparsely granulated ones tend to show hyperintense signals, indicating potential pasireotide effectiveness (18). Low AIP (aryl hydrocarbon receptor-interacting protein) expression or highly mutated AIP tumors may respond better to pasireotide than first-generation SSA (42). Furthermore, low expression of E-cadherin and high Ki-67 expression favor pasireotide (12, 18, 43, 44). Additionally, GH-secreting adenomas with mutations in the stimulatory G-protein alpha subunit, showing higher SSTR5 expression, may be more responsive to pasireotide (45). Currently, there is a lack of comprehensive studies focusing on the factors mentioned, making them merely potential considerations. Although imaging is widely accessible, the analysis of tumor samples seldomly includes the above-mentioned factors such as SSTR staining and E-cadherin expression. Consequently, clinicians face challenges in selecting patients based on these markers and need to rely on imaging and patient history.
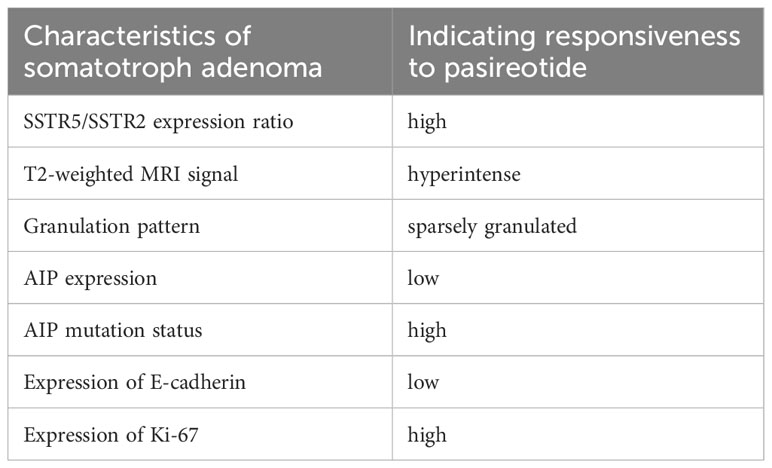
Table 2 Characteristics of somatotroph adenomas predictive of a good response to pasireotide.
Clinical benefits of pasireotide could be seen in patients with headaches unresponsive to first-generation SSA and young patients with tumor growth despite treatment (12, 46).
Given the range of characteristics of somatotrophic adenoma that influence the response to the various SSA, it seems reasonable to assume that tumors that respond poorly to first-generation SSA are more likely to have characteristics that indicate responsiveness to pasireotide. Patients with low response to first-generation SSA should therefore be considered good candidates for treatment with pasireotide.
4 Risk stratification
When considering treatment of acromegaly patients with pasireotide, we suggest stratifying patients by baseline risk status for worsening of glucose control. Risk factors for pasireotide-associated hyperglycemia were identified in an analysis examining baseline characteristics and the occurrence and management of hyperglycemia during treatment with pasireotide for acromegaly in two prospective clinical trials, C2305 and C2402 (PAOLA) (47). Table 3 summarizes baseline characteristics of patients with acromegaly who are at high or low risk for pasireotide-associated hyperglycemia (47): Patients are considered at higher risk if above the age of 40, obese, [pre-]diabetic, and/or having a history of dyslipidemia/hypertension. Accordingly, normal-weight and metabolically healthy young patients are considered being at lower risk. Therefore, it is crucial to recognize preexisting abnormal glucose metabolism and, if necessary, initiate and/or adjust antidiabetic treatments before initiating therapy with pasireotide (37). Clinicians who are not familiar with diabetes therapy should seek expert help.
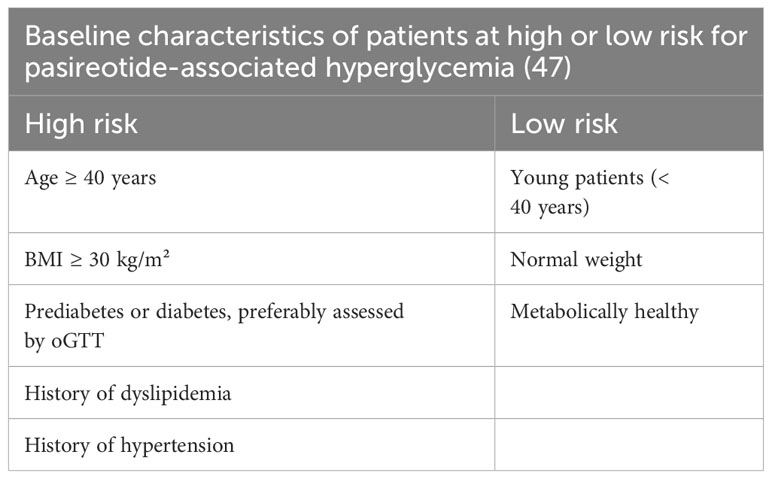
Table 3 Baseline characteristics that determine the risk for pasireotide-associated hyperglycemia.
Despite the identification of some predictive factors for the development of pasireotide-induced hyperglycemia, it should be noted that hyperglycemia under pasireotide treatment can also be observed in patients without known risk factors (14).
Current diabetes classifications have shortcomings and newer cluster-based classifications have been proposed (48). Arguments in favor of these newer classifications are manifold. Firstly, they allow for personalized treatment plans, recognizing the unique hyperglycemia patterns in diverse individuals. Secondly, these classifications enhance understanding of the specific pathophysiological variations of hyperglycemia, which might be especially helpful in a context such as acromegaly where the underlying pathophysiology per se is different from “standard diabetes”. Thirdly, they can help predict individual responses to treatment, guiding preemptive or intensified glucose-lowering strategies. However, these classifications are not widely established and validated yet in clinical practice and therefore should not be used for clinical care at this point. Furthermore, current routine screening of acromegaly patients does not usually collect the data necessary for such classification. In the context of emerging awareness of pathophysiological peculiarities of hyperglycemia in acromegaly more research in this domain is needed and possibly the development of a specific classification warranted.
5 How to monitor for hyperglycemia
As worsening of glycemic control is frequently observed in patients with acromegaly treated with pasireotide, glycemic control should be monitored at the beginning and during follow-up of pasireotide therapy. Self-monitoring of blood glucose (SMBG) is an important cornerstone in monitoring glycemic control. A potential obstacle to frequent self-monitoring of blood glucose levels is that self-testing in patients who are at low risk of hyperglycemia may not be reimbursed by health insurers. Compliance may also be poor, particularly in patients without hyperglycemia, if self-testing must be performed too frequently.
In patients treated with pasireotide, fasting plasma glucose (FPG) and HbA1c levels tend to increase during the first 1-3 months of treatment and stabilize thereafter (23). Especially post-prandial glucose (PPG) measurements are important, as pasireotide-associated hyperglycemia is related to decreases in glucose-stimulated insulin secretion and incretin hormone response which should be most evident after a meal (21). Therefore, SMBG is particularly important in the first three months after starting therapy. SMBG can subsequently be replaced by regular HbA1c measurements. In low-risk patients with no worsening of glycemic control, self-measurement of blood glucose once every two weeks is considered sufficient (FPG and PPG). In high-risk patients who do not have elevated blood glucose levels, weekly blood glucose self-monitoring (FPG and PPG) is recommended in the first three months. In patients with pre-existing hyperglycemia we recommend daily SMBG measurements with at least one FPG and one PPG, ideally though as multiple-point profiles. When possible and economically feasible, high-risk patients should temporarily be equipped with devices allowing continuous glucose monitoring to detect elevated blood glucose levels early and determine deviations from the time in range precisely. This approach offers the advantage to detect glycemic alterations earlier than the use of point measurements with greater ease of use for the patients. Flash glucose monitoring devices may be an economically less challenging alternative. If worsening of blood glucose control is observed, further action should ideally be decided in consultation with a diabetologist. In the situation of development of impaired glucose tolerance (IGT) and/or impaired fasting glucose (IGT) with FPG >100 mg/dl (5.6 mmol/l) and/or 2h PPG >140 mg/dl (7.8 mmol/l) and/or an HbA1c rising to or above 5.7% (38.8 mmol/mol), antidiabetic treatment based on lifestyle recommendations such as nutrition counselling and exercise motivation should be initiated. At the latest, antidiabetic treatment should be initiated when diagnostic criteria of manifest diabetes mellitus are fulfilled with FPG values greater than 126 mg/dl (7.0 mmol/l), blood glucose levels greater than 200 mg/dl (11.1 mmol/l) measured at random or an HbA1c ≥ 6.5% (48 mmol/mol). In general, all patients should be informed of the risk of occurrence of hyperglycemic deviations with pasireotide treatment, ideally explaining basic pathophysiological principles.
During treatment with pasireotide HbA1c measurements should be routinely performed every three months and at least with each IGF-I measurement. Regular HbA1c monitoring is important to detect late-onset hyperglycemic alterations, as there is anecdotic evidence of development of diabetes even after several years of pasireotide treatment (25).
A summary of the recommendations on the monitoring of hyperglycemia in patients with acromegaly treated with pasireotide are displayed in Figure 1.
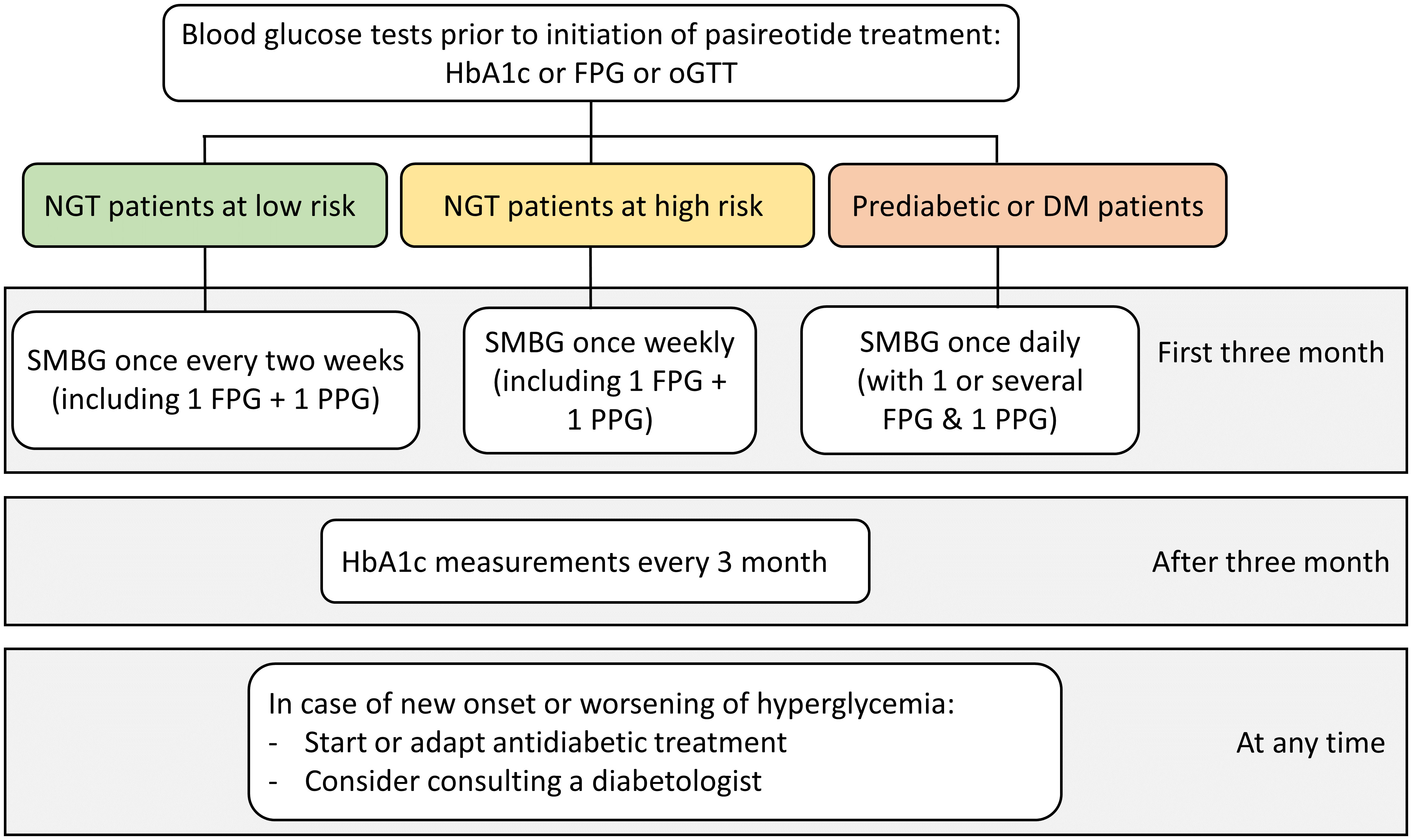
Figure 1 Recommendations on the monitoring of hyperglycemia in patients with acromegaly treated with pasireotide. (DM, Diabetes mellitus; FPG, Fasting plasma glucose; HbA1c, Glycated hemoglobin; NGT, Normal glucose tolerance; oGTT, Oral glucose tolerance test; PPG, Postprandial plasma glucose; SMBG, self-monitoring of blood glucose).
6 Treatment of hyperglycemia in acromegaly patients before and during pasireotide therapy
Adequate treatment of acromegaly is the priority in all patients. As long as an excess of GH is not adequately treated, the baseline for glucose metabolism will likely be suboptimal. All patients with impaired metabolic control during pasireotide therapy should receive diabetes education and nutrition and lifestyle guidance, regardless of whether they are still achieving their individual targets. Education and guidance should include physical activity, healthy sleep, high-quality nutrition, and eating patterns that result in weight loss where appropriate (49). Glycemic targets should be based on an individualized approach for each patient, considering individual risk, life circumstances, and comorbidities. This can be guided by T2DM consensus statements and guidelines (49, 50).
It is recommended that, if there is uncertainty in the management of hyperglycemia associated with pasireotide therapy, an expert diabetologist should be consulted for interdisciplinary treatment approaches. If possible, a panel of endocrinologists, diabetologists, and dieticians/diabetes educators should be scheduled to discuss cases of secondary diabetes.
Metformin should be introduced as a first-line medication when pharmacotherapy for hyperglycemia is necessary. Although metformin does not directly address the pathophysiology of pasireotide-induced hyperglycemia, there is sufficient evidence for a response to metformin. Many patients with pasireotide-induced diabetes can be controlled with metformin monotherapy (13, 14, 51). In addition, acromegaly patients are often overweight, which makes them good candidates for metformin since this medication does not promote further weight gain (47, 49).
High cardiovascular (CV) or renal risk impacts on the choice of antidiabetic therapy, thus evaluation of risks should be performed at the start of therapy (49). Since patients with acromegaly often have a high CV risk, they are prime candidates for early dual medical therapy with proven effects on cardiovascular and renal outcomes. For such patients, the positive effects on cardiovascular risk of some glucagon-like peptide-1 receptor agonists (GLP-1 RA) is particularly valuable. It’s important to recognize that not all GLP-1 RAs are identical in their efficacy. For instance, semaglutide generally shows greater glycemic control and weight loss benefits compared to dulaglutide or liraglutide. Moreover, certain GLP-1 RAs, like exenatide and lixisenatide, have not demonstrated significant cardiovascular benefits. GLP-1 RA directly target the reduced incretin secretion, which is a known mechanism of pasireotide-induced hyperglycemia (20, 21). Therefore, our expert consensus is that GLP-1 RA should be the preferred option for all suitable patients and could also be considered as a first-line treatment. We suggest prioritizing GLP-1 RA with proven superior efficacy. However, it is crucial to note the potential gastrointestinal side effects associated with GLP-1 RA, which are non-trivial in clinical practice. GLP-1 RA may also be helpful to reduce body weight if needed (49).
In patients with low CV risk, the use of dipeptidyl peptidase 4 inhibitors (DPP4i) can be considered as they neither significantly reduce nor increase cardiovascular events in most patients. DPP4i are easy to use and have few side effects, but they only indirectly affect the decreased incretin effect caused by pasireotide, as they prolong the half-life of endogenous GLP-1 but do not compensate for the decreased secretion (49). However, clinical data show promising effects of DPP4i therapy in this situation. This highlights the relevance of considering DPP4 inhibitors as a viable alternative to GLP-1 RA when gastrointestinal side-effects in the latter pose a considerable burden on patients. A recent multicenter, randomized, open-label, phase IV trial evaluated incretin-based therapy (DPP-4i followed by a GLP-1 RA) versus insulin for the treatment of pasireotide-associated hyperglycemia in adults with acromegaly (n = 190) or Cushing’s disease (n = 59) with hyperglycemia inadequately controlled by metformin or other oral antidiabetic agents. In these patients, there was a trend towards better control of HbA1c with incretin-based therapy versus insulin, particularly in patients with acromegaly (51). Since DPP4i at least indirectly influence the pathophysiology of pasireotide-induced hyperglycemia, they may also be considered as first-line treatment in some cases.
There are currently limited data on the use of SGLT-2 (sodium-glucose transport protein 2) inhibitors for the management of hyperglycemia in patients with acromegaly. In contrast to DPP-4i and GLP-1 RA, SGLT-2 inhibitors do not affect the pasireotide-induced decreased incretin effect and therefore have presumably less impact on the specific pathophysiology. Moreover, it is important to note that acromegaly patients are at an increased risk of developing diabetic ketoacidosis (DKA), a common complication of SGLT-2 inhibitors (52–54). Therefore, SGLT-2 inhibitors are not typically recommended for patients with acromegaly. The shift in insulin/glucagon ratio as observed in pasireotide treatment is thought to be especially prone to this side-effect, warranting greater caution (55). However, patients safely treated with pasireotide and SGLT-2 inhibitors have been reported (56). In current T2DM guidelines, SGLT-2 inhibitors may be considered for certain patient groups, especially those with heart failure and renal disease. In these patients, SGLT-2 inhibitors with primary evidence of reducing chronic kidney disease (CKD) progression and heart failure may be an option; accordingly, acromegaly patients harboring these characteristics could benefit from this treatment, but it should be carefully weighed against the potential risk of DKA (49, 55).
The addition of insulin may be considered, but it should ideally be used as an adjunct to metformin and at least one other therapeutic agent. The current consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) advises the consideration of a GLP-1 RA prior to initiation of insulin therapy (49). It’s important to note, in the context of insulin therapy, that several challenges may arise. One of the significant issues is the risk of hypoglycemia, particularly if injection intervals are not consistently maintained or if insulin doses are not properly adjusted to match carbohydrate intake. Additionally, a notable disadvantage of insulin therapy is the potential for weight gain. This risk factor should be carefully weighed, especially in patients for whom weight management is a critical component of their overall health strategy.
A summary of the recommendations on the treatment of hyperglycemia and diabetes in patients with acromegaly treated with pasireotide are displayed in Figure 2.
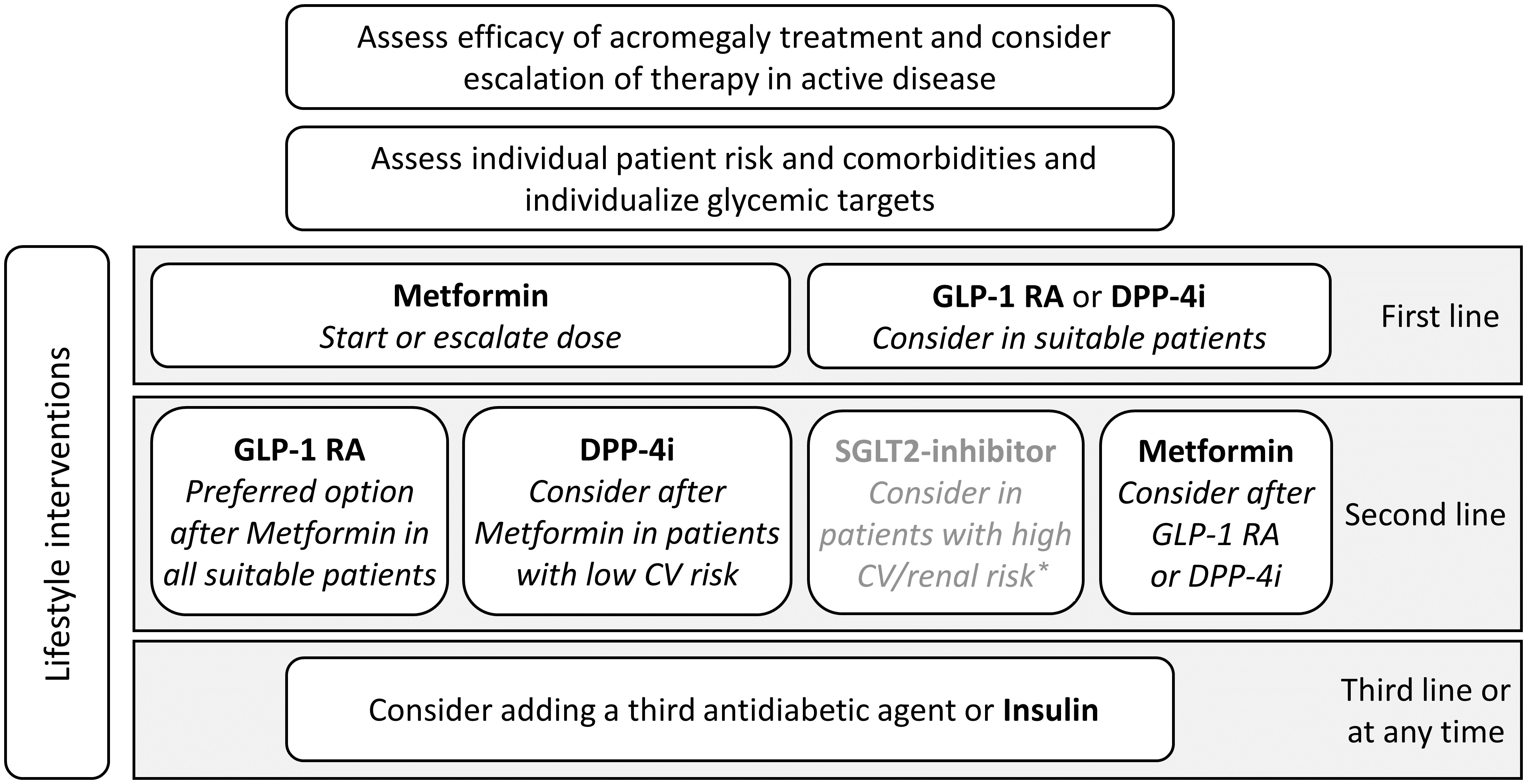
Figure 2 Recommendations on the treatment of hyperglycemia and diabetes in patients with acromegaly treated with pasireotide. *carefully weigh potential benefits on heart failure and renal disease against potential risk of diabetic ketoacidosis (CV, Cardiovascular; DPP-4i, Dipeptidyl peptidase 4 inhibitor; GLP-1 RA, Glucagon-like peptide-1 receptor agonist; SGLT-2, sodium-glucose transport protein 2; T2DM, Type 2 diabetes mellitus).
While co-agonists of GLP-1 and GIP (glucose-dependent insulinotropic polypeptide), such as tirzepatide, present a potentially intriguing therapeutic option for the future, the current lack of extensive precludes a definitive recommendation for their use in managing pasireotide-induced hyperglycemia. However, it is practical to consider these dual incretin agonists as a more feasible alternative to insulin therapy in this context. While acknowledging the limited data, tirzepatide should be included in the discussion about GLP-1 RA as a promising option for patients experiencing hyperglycemia due to pasireotide
In the treatment of hyperglycemia when pasireotide therapy is paused or discontinued, it is useful to distinguish between treatment-associated or pre-existing disease. In the case of pre-existing disease antidiabetic therapy may need to be continued as before the start of pasireotide therapy. Any pasireotide-related hyperglycemia can be expected to improve after pasireotide therapy is stopped. In this case, it may be appropriate to reduce or discontinue antihyperglycemic treatment. Metformin and other antidiabetic medications with low hypoglycemic risk can be discontinued when individual HbA1c targets are reached. Patients receiving insulin therapy are at higher risk of developing hypoglycemia, but usually perform regular SMBG measurements so that these patients can reduce insulin when their target levels are reached. If HbA1c levels are in or near the normal range, de-escalation of antidiabetic treatment should be considered.
There seems to be no clear relationship between the dose of pasireotide and the risk of hyperglycemia, and even low doses can cause worsening of glycemic control (22). Thus, treatment decisions should be made irrespective of the pasireotide dose and primarily guided by blood glucose assessment and individualized targets.
It should also be considered that acromegaly patients with hyperglycemia are often younger than T2DM patients. In clinical studies and real-world cohorts, the mean age of acromegaly patients is often between 40 and 50 years, with non-negligible proportions of female patients of reproductive age (13, 14, 32, 47). This particular risk structure of acromegaly patients should be considered regarding the choice of therapy. In case of pregnancy, management of diabetes should be in concordance with the current ADA guidelines (57).
In summary, we emphasize the importance of adequate control of acromegaly, excellent diabetes education, nutrition and lifestyle counseling as the foundation of management of acromegaly and hyperglycemic adverse events under pasireotide. Importantly, our expert recommendations address the specific pathophysiology of pasireotide-induced hyperglycemia by recommending the incretin-based therapeutics DPP-4i and GLP-1 RA as first-line therapy as an alternative to metformin in all appropriate patients when pharmacotherapy is needed.
7 Summary
The second-generation SSA pasireotide has been attributed with potentially greater clinical efficacy in acromegaly compared to first-generation SSA (9, 11, 12). However, several clinical trials emphasize the occurrence of hyperglycemia-related adverse events and diabetes in acromegaly patients treated with pasireotide (13–16, 24, 26, 27, 29–33). Patients with acromegaly due to somatotroph adenoma with a high expression ratio of the somatostatin receptors SSTR5/SSTR2, a hyperintense T2-weighted MRI signal, sparse granulation, low AIP expression, high AIP mutation status, low expression of E-cadherin and high expression of Ki-67 are considered good candidates to benefit from pasireotide treatment (12, 18, 39–45). Despite the potential of these indicators, limited comprehensive studies and routine clinical practices make it challenging for clinicians to use these markers for patient selection, leading to a reliance on imaging and patient history.
Acromegaly patients who are metabolically healthy, young (<40), and have a BMI <30 kg/m² are considered to be at low risk for pasireotide-associated hyperglycemia (47). Blood glucose tests should be performed prior to initiation of pasireotide to stratify patients by baseline risk for worsening of glucose control.
We recommend close glucose monitoring of fasting and post-prandial glucose levels during the first three month after initiating pasireotide treatment. Baseline risk determines our recommendation for the frequency of self-monitoring of blood glucose (SMBG) as outlined in Figure 1.
Adequate treatment of acromegaly is the priority in all patients. As a preventive measure or after the occurrence of hyperglycemic events, diabetes education, nutrition and lifestyle guidance should be provided to all patients regardless of whether they are achieving their individual blood glucose targets.
When pharmacotherapy for hyperglycemia is necessary, our expert recommendations address the specific pathophysiology of pasireotide-induced hyperglycemia by recommending the incretin-based therapeutics GLP-1 RA and DPP-4i as first-line therapy in all appropriate patients as an alternative to metformin. Figure 2 summarizes key recommendations on our suggested treatment approach.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author contributions
SS: Conceptualization, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing, Data curation. SM: Data curation, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. JG: Data curation, Investigation, Writing – original draft, Writing – review & editing. JF: Data curation, Investigation, Writing – original draft, Writing – review & editing. KS: Data curation, Investigation, Writing – original draft, Writing – review & editing. JS: Data curation, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. BV: Conceptualization, Data curation, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research project received support from Recordati Rare Diseases (RRD), providing sponsorship for the meetings including covering costs for the venue, participant travel, and food services. Furthermore, RRD funded editorial assistance by a professional medical writer. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Acknowledgments
The authors would like to express their sincere gratitude to Dr. Sören Reinhard for his valuable assistance in the drafting of this manuscript. Dr. Reinhard’s expertise and insights greatly contributed to the clarity and coherence of the final document. His meticulous attention to detail and thoughtful suggestions were instrumental in improving the overall quality of the article.
Conflict of interest
SS has received consulting fees from Crinetics and Recordati Rare Diseases RRD as well as honoraria for lectures and conference chairing from Novartis, Ipsen, Hexal/Sandoz, Pfizer, and RRD. He has served as advisory board member for Novartis and RRD. Furthermore, RRD has donated a drug for compassionate use in one of his patients. SM has received lecturing fees and/or consulting fees and/or grants from AstraZeneca, Bayer, Boehringer Ingelheim, Lilly, Novo Nordisk, RRD. JG and JF have received consulting fees from RRD. KS has received lecturing fees and/or consulting fees from Pfizer, RRD, Sandoz, and Novo Nordisk. JS has received honoraria for talks and/or consultancy and/or research funding from Apitope, AstraZeneca, Bayer, Berlin Chemie, Boehringer Ingelheim, Bristol-Meyers Squibb, Eli Lilly, GI-Dynamics, GlaxoSmithKline, Intarcia, Ipsen, Janssen, LifeScan, MedScape, MSD, Novartis, Novo Nordisk, Omniamed, Pfizer, RRD, Roche, Sanofi, Servier, Takeda, and Ypsomed. In the past 3 years BV has received honoraria from Amgen, AstraZeneca, Lilly, Novo Nordisk, Sanofi and RRD for conferences or advisory boards, and received funding for research from AstraZeneca and Novo Nordisk.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Gadelha MR, Kasuki L, Lim DST, Fleseriu M. Systemic complications of acromegaly and the impact of the current treatment landscape: an update. Endocr Rev (2019) 40(1):268–332. doi: 10.1210/er.2018-00115
2. Störmann S, Schopohl J. Drug treatment strategies for secondary diabetes in patients with acromegaly. Expert Opin Pharmacother (2020) 21(15):1883–95. doi: 10.1080/14656566.2020.1789098
3. Vijayakumar A, Novosyadlyy R, Wu Y, Yakar S, LeRoith D. Biological effects of growth hormone on carbohydrate and lipid metabolism. Growth Horm IGF Res (2010) 20(1):1–7. doi: 10.1016/j.ghir.2009.09.002
4. Olarescu NC, Bollerslev J. The impact of adipose tissue on insulin resistance in acromegaly. Trends Endocrinol Metab (2016) 27(4):226–37. doi: 10.1016/j.tem.2016.02.005
5. Maffezzoni F, Mazziotti G, Giustina A. Current and emerging aspects of diabetes mellitus in acromegaly. Trends Endocrinol Metab (2016) 27(7):470–83. doi: 10.1016/j.tem.2016.04.014
6. Barnett P. Somatostatin and somatostatin receptor physiology. Endocrine (2003) 20(3):255–64. doi: 10.1385/endo:20:3:255
7. Günther T, Tulipano G, Dournaud P, Bousquet C, Csaba Z, Kreienkamp HJ, et al. International union of basic and clinical pharmacology. CV. Somatostatin receptors: structure, function, ligands, and new nomenclature. Pharmacol Rev (2018) 70(4):763–835. doi: 10.1124/pr.117.015388
8. Gadelha MR, Wildemberg LE, Kasuki L. The future of somatostatin receptor ligands in acromegaly. J Clin Endocrinol Metab (2022) 107(2):297–308. doi: 10.1210/clinem/dgab726
9. Bruns C, Lewis I, Briner U, Meno-Tetang G, Weckbecker G. SOM230: a novel somatostatin peptidomimetic with broad somatotropin release inhibiting factor (SRIF) receptor binding and a unique antisecretory profile. Eur J Endocrinol (2002) 146(5):707–16. doi: 10.1530/eje.0.1460707
10. Lesche S, Lehmann D, Nagel F, Schmid HA, Schulz S. Differential effects of octreotide and pasireotide on somatostatin receptor internalization and trafficking in vitro. J Clin Endocrinol Metab (2009) 94(2):654–61. doi: 10.1210/jc.2008-1919
11. Schmid HA, Brueggen J. Effects of somatostatin analogs on glucose homeostasis in rats. J Endocrinol (2012) 212(1):49–60. doi: 10.1530/joe-11-0224
12. Bolanowski M, Kałużny M, Witek P, Jawiarczyk-Przybyłowska A. Pasireotide-a novel somatostatin receptor ligand after 20 years of use. Rev Endocr Metab Disord (2022) 23(3):601–20. doi: 10.1007/s11154-022-09710-3
13. Colao A, Bronstein MD, Freda P, Gu F, Shen CC, Gadelha M, et al. Pasireotide versus octreotide in acromegaly: a head-to-head superiority study. J Clin Endocrinol Metab (2014) 99(3):791–9. doi: 10.1210/jc.2013-2480
14. Gadelha MR, Bronstein MD, Brue T, Coculescu M, Fleseriu M, Guitelman M, et al. Pasireotide versus continued treatment with octreotide or lanreotide in patients with inadequately controlled acromegaly (PAOLA): a randomised, phase 3 trial. Lancet Diabetes Endocrinol (2014) 2(11):875–84. doi: 10.1016/s2213-8587(14)70169-x
15. Shimon I, Adnan Z, Gorshtein A, Baraf L, Saba Khazen N, Gershinsky M, et al. Efficacy and safety of long-acting pasireotide in patients with somatostatin-resistant acromegaly: a multicenter study. Endocrine (2018) 62(2):448–55. doi: 10.1007/s12020-018-1690-5
16. Gadelha M, Bex M, Colao A, Pedroza Garcia EM, Poiana C, Jimenez-Sanchez M, et al. Evaluation of the efficacy and safety of switching to pasireotide in patients with acromegaly inadequately controlled with first-generation somatostatin analogs. Front Endocrinol (Lausanne) (2019) 10:931. doi: 10.3389/fendo.2019.00931
17. Melmed S, Bronstein MD, Chanson P, Klibanski A, Casanueva FF, Wass JAH, et al. A Consensus Statement on acromegaly therapeutic outcomes. Nat Rev Endocrinol (2018) 14(9):552–61. doi: 10.1038/s41574-018-0058-5
18. Puig-Domingo M, Bernabéu I, Picó A, Biagetti B, Gil J, Alvarez-Escolá C, et al. Pasireotide in the personalized treatment of acromegaly. Front Endocrinol (Lausanne) (2021) 12:648411. doi: 10.3389/fendo.2021.648411
19. Kumar U, Sasi R, Suresh S, Patel A, Thangaraju M, Metrakos P, et al. Subtype-selective expression of the five somatostatin receptors (hSSTR1-5) in human pancreatic islet cells: a quantitative double-label immunohistochemical analysis. Diabetes (1999) 48(1):77–85. doi: 10.2337/diabetes.48.1.77
20. Henry RR, Ciaraldi TP, Armstrong D, Burke P, Ligueros-Saylan M, Mudaliar S. Hyperglycemia associated with pasireotide: results from a mechanistic study in healthy volunteers. J Clin Endocrinol Metab (2013) 98(8):3446–53. doi: 10.1210/jc.2013-1771
21. Breitschaft A, Hu K, Hermosillo Reséndiz K, Darstein C, Golor G. Management of hyperglycemia associated with pasireotide (SOM230): healthy volunteer study. Diabetes Res Clin Pract (2014) 103(3):458–65. doi: 10.1016/j.diabres.2013.12.011
22. Shenouda M, Maldonado M, Wang Y, Bouillaud E, Hudson M, Nesheiwat D, et al. An open-label dose-escalation study of once-daily and twice-daily pasireotide in healthy volunteers: safety, tolerability, and effects on glucose, insulin, and glucagon levels. Am J Ther (2014) 21(3):164–73. doi: 10.1097/MJT.0b013e31824c3eb4
23. Samson SL. Management of hyperglycemia in patients with acromegaly treated with pasireotide LAR. Drugs (2016) 76(13):1235–43. doi: 10.1007/s40265-016-0615-y
24. Witek P, Bolanowski M, Szamotulska K, Wojciechowska-Luźniak A, Jawiarczyk-Przybyłowska A, Kałużny M. The effect of 6 months' Treatment with pasireotide LAR on glucose metabolism in patients with resistant acromegaly in real-world clinical settings. Front Endocrinol (Lausanne) (2021) 12:633944. doi: 10.3389/fendo.2021.633944
25. Störmann S, Schilbach K, Amereller F, Schweizer J, Schopohl J. Delayed onset of pasireotide-induced hyperglycemia: Report of two cases. Endocrine Abstracts (2023) 90):EP761. doi: 10.1530/endoabs.90.EP761
26. Sheppard M, Bronstein MD, Freda P, Serri O, De Marinis L, Naves L, et al. Pasireotide LAR maintains inhibition of GH and IGF-1 in patients with acromegaly for up to 25 months: results from the blinded extension phase of a randomized, double-blind, multicenter, Phase III study. Pituitary (2015) 18(3):385–94. doi: 10.1007/s11102-014-0585-6
27. Tahara S, Murakami M, Kaneko T, Shimatsu A. Efficacy and safety of long-acting pasireotide in Japanese patients with acromegaly or pituitary gigantism: results from a multicenter, open-label, randomized, phase 2 study. Endocr J (2017) 64(7):735–47. doi: 10.1507/endocrj.EJ16-0624
28. Muhammad A, Coopmans EC, Delhanty PJD, Dallenga AHG, Haitsma IK, Janssen J, et al. Efficacy and Safety of switching to Pasireotide in Acromegaly Patients controlled with Pegvisomant and Somatostatin Analogues: PAPE extension study. Eur J Endocrinol (2018) 179(5):269–77. doi: 10.1530/eje-18-0353
29. Colao A, Bronstein MD, Brue T, De Marinis L, Fleseriu M, Guitelman M, et al. Pasireotide for acromegaly: long-term outcomes from an extension to the Phase III PAOLA study. Eur J Endocrinol (2020) 182(6):583. doi: 10.1530/eje-19-0762
30. Chiloiro S, Giampietro A, Visconti F, Rossi L, DonFrancesco F, Fleseriu CM, et al. Glucose metabolism outcomes in acromegaly patients on treatment with pasireotide-LAR or pasireotide-LAR plus Pegvisomant. Endocrine (2021) 73(3):658–66. doi: 10.1007/s12020-021-02711-3
31. Akirov A, Gorshtein A, Dotan I, Khazen NS, Pauker Y, Gershinsky M, et al. Long-term safety and efficacy of long-acting pasireotide in acromegaly. Endocrine (2021) 74(2):396–403. doi: 10.1007/s12020-021-02782-2
32. Stelmachowska-Banaś M, Czajka-Oraniec I, Tomasik A, Zgliczyński W. Real-world experience with pasireotide-LAR in resistant acromegaly: a single center 1-year observation. Pituitary (2022) 25(1):180–90. doi: 10.1007/s11102-021-01185-w
33. Wolf P, Dormoy A, Maione L, Salenave S, Young J, Kamenicky P, et al. Impairment in insulin secretion without changes in insulin resistance explains hyperglycemia in patients with acromegaly treated with pasireotide LAR. Endocr Connect (2022) 11(12):e220296. doi: 10.1530/ec-22-0296
34. Corica G, Pirchio R, Milioto A, Nista F, Arecco A, Mattioli L, et al. Pasireotide effects on biochemical control and glycometabolic profile in acromegaly patients switched from combination therapies or unconventional dosages of somatostatin analogs. J Endocrinol Invest (2023). doi: 10.1007/s40618-023-02186-1
35. Gadelha M, Marques NV, Fialho C, Scaf C, Lamback E, Antunes X, et al. Long-term efficacy and safety of pasireotide in patients with acromegaly: 14 years' single-center real-world experience. J Clin Endocrinol Metab (2023) 108(12):e1571-e1579. doi: 10.1210/clinem/dgad378
36. Esposito D, Olsson DS, Franzén S, Miftaraj M, Nåtman J, Gudbjörnsdottir S, et al. Effect of diabetes on morbidity and mortality in patients with acromegaly. J Clin Endocrinol Metab (2022) 107(9):2483–92. doi: 10.1210/clinem/dgac400
37. Reznik Y, Bertherat J, Borson-Chazot F, Brue T, Chanson P, Cortet-Rudelli C, et al. Management of hyperglycaemia in Cushing's disease: experts' proposals on the use of pasireotide. Diabetes Metab (2013) 39(1):34–41. doi: 10.1016/j.diabet.2012.10.005
38. Colao A, De Block C, Gaztambide MS, Kumar S, Seufert J, Casanueva FF. Managing hyperglycemia in patients with Cushing's disease treated with pasireotide: medical expert recommendations. Pituitary (2014) 17(2):180–6. doi: 10.1007/s11102-013-0483-3
39. Gatto F, Feelders RA, Franck SE, van Koetsveld PM, Dogan F, Kros JM, et al. In vitro head-to-head comparison between octreotide and pasireotide in GH-secreting pituitary adenomas. J Clin Endocrinol Metab (2017) 102(6):2009–18. doi: 10.1210/jc.2017-00135
40. Coopmans EC, Schneiders JJ, El-Sayed N, Erler NS, Hofland LJ, van der Lely AJ, et al. T2-signal intensity, SSTR expression, and somatostatin analogs efficacy predict response to pasireotide in acromegaly. Eur J Endocrinol (2020) 182(6):595–605. doi: 10.1530/eje-19-0840
41. Heck A, Ringstad G, Fougner SL, Casar-Borota O, Nome T, Ramm-Pettersen J, et al. Intensity of pituitary adenoma on T2-weighted magnetic resonance imaging predicts the response to octreotide treatment in newly diagnosed acromegaly. Clin Endocrinol (Oxf) (2012) 77(1):72–8. doi: 10.1111/j.1365-2265.2011.04286.x
42. Daly AF, Rostomyan L, Betea D, Bonneville JF, Villa C, Pellegata NS, et al. AIP-mutated acromegaly resistant to first-generation somatostatin analogs: long-term control with pasireotide LAR in two patients. Endocr Connect (2019) 8(4):367–77. doi: 10.1530/ec-19-0004
43. Fougner SL, Casar-Borota O, Heck A, Berg JP, Bollerslev J. Adenoma granulation pattern correlates with clinical variables and effect of somatostatin analogue treatment in a large series of patients with acromegaly. Clin Endocrinol (Oxf) (2012) 76(1):96–102. doi: 10.1111/j.1365-2265.2011.04163.x
44. Kasuki L, Wildemberg LE, Neto LV, Marcondes J, Takiya CM, Gadelha MR. Ki-67 is a predictor of acromegaly control with octreotide LAR independent of SSTR2 status and relates to cytokeratin pattern. Eur J Endocrinol (2013) 169(2):217–23. doi: 10.1530/eje-13-0349
45. Wildemberg LE, Henriques D, Elias PCL, Lima CHA, Musolino NRC, Camacho AHS, et al. gsp mutation is not a molecular biomarker of long-term response to first-generation somatostatin receptor ligands in acromegaly. Cancers (Basel) (2021) 13(19):4857. doi: 10.3390/cancers13194857
46. Coopmans EC, Muhammad A, van der Lely AJ, Janssen J, Neggers S. How to position pasireotide LAR treatment in acromegaly. J Clin Endocrinol Metab (2019) 104(6):1978–88. doi: 10.1210/jc.2018-01979
47. Gadelha MR, Gu F, Bronstein MD, Brue TC, Fleseriu M, Shimon I, et al. Risk factors and management of pasireotide-associated hyperglycemia in acromegaly. Endocr Connect (2020) 9(12):1178–90. doi: 10.1530/ec-20-0361
48. Ahlqvist E, Storm P, Käräjämäki A, Martinell M, Dorkhan M, Carlsson A, et al. Novel subgroups of adult-onset diabetes and their association with outcomes: a data-driven cluster analysis of six variables. Lancet Diabetes Endocrinol (2018) 6(5):361–9. doi: 10.1016/s2213-8587(18)30051-2
49. Davies MJ, Aroda VR, Collins BS, Gabbay RA, Green J, Maruthur NM, et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the american diabetes association (ADA) and the european association for the study of diabetes (EASD). Diabetes Care (2022) 45(11):2753–86. doi: 10.2337/dci22-0034
50. Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, Delgado V, et al. ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J (2019) 41(2):255–323. doi: 10.1093/eurheartj/ehz486
51. Samson SL, Gu F, Feldt-Rasmussen U, Zhang S, Yu Y, Witek P, et al. Managing pasireotide-associated hyperglycemia: a randomized, open-label, Phase IV study. Pituitary (2021) 24(6):887–903. doi: 10.1007/s11102-021-01161-4
52. Quarella M, Walser D, Brandle M, Fournier JY, Bilz S. Rapid onset of diabetic ketoacidosis after SGLT2 inhibition in a patient with unrecognized acromegaly. J Clin Endocrinol Metab (2017) 102(5):1451–3. doi: 10.1210/jc.2017-00082
53. Yoshida N, Goto H, Suzuki H, Nagasawa K, Takeshita A, Okubo M, et al. Ketoacidosis as the initial clinical condition in nine patients with acromegaly: a review of 860 cases at a single institute. Eur J Endocrinol (2013) 169(1):127–32. doi: 10.1530/eje-13-0060
54. Prencipe N, Bioletto F, Bona C, Gatti F, Grottoli S. Diabetic ketoacidosis in acromegaly: a case study-somatostatin analogs adverse event or disease complication? Acta Diabetol (2020) 57(4):491–3. doi: 10.1007/s00592-019-01437-z
55. Zaina A, Prencipe N, Golden E, Berton AM, Arad E, Abid A, et al. How to position sodium-glucose co-transporter 2 inhibitors in the management of diabetes in acromegaly patients. Endocrine (2023) 80(3):491–9. doi: 10.1007/s12020-023-03352-4
56. Zaina A, Grober Y, Abid A, Arad E, Golden E, Badarny S. Sodium glucose cotransporter 2 inhibitors treatment in acromegalic patients with diabetes-a case series and literature review. Endocrine (2021) 73(1):65–70. doi: 10.1007/s12020-021-02718-w
Keywords: acromegaly, pasireotide, hyperglycemia, diabetes mellitus, monitoring strategy, patient management
Citation: Störmann S, Meyhöfer SM, Groener JB, Faust J, Schilbach K, Seufert J and Vergès B (2024) Management of pasireotide-induced hyperglycemia in patients with acromegaly: An experts’ consensus statement. Front. Endocrinol. 15:1348990. doi: 10.3389/fendo.2024.1348990
Received: 03 December 2023; Accepted: 25 January 2024;
Published: 09 February 2024.
Edited by:
Lucio Vilar, Federal University of Pernambuco, BrazilReviewed by:
Laurence Katznelson, Stanford University, United StatesClaudia Pivonello, University of Naples Federico II, Italy
Copyright © 2024 Störmann, Meyhöfer, Groener, Faust, Schilbach, Seufert and Vergès. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sylvère Störmann, sylvere.stoermann@med.uni-muenchen.de
†ORCID: Sylvère Störmann, orcid.org/0000-0002-5465-3491
Sebastian M. Meyhöfer, orcid.org/0000-0003-2034-5922
Jan B. Groener, orcid.org/0000-0001-7211-1883
Katharina Schilbach, orcid.org/0000-0002-8667-0296
Jochen Seufert, orcid.org/0000-0001-5654-7310
Bruno Vergès, orcid.org/0000-0001-8957-629X