 Chadia Mizab1†
Chadia Mizab1† Enric Sánchez2,3,4†Liliana Gutiérrez-Carrasquilla1Núria Balsells2Anaïs Arqué2Raquel Ruano2,3Magda Mateu2
Enric Sánchez2,3,4†Liliana Gutiérrez-Carrasquilla1Núria Balsells2Anaïs Arqué2Raquel Ruano2,3Magda Mateu2 Marta Zorzano-Martínez2,3Anna Pomés2Esther García-Aguilera2Raquel Martí2,3
Marta Zorzano-Martínez2,3Anna Pomés2Esther García-Aguilera2Raquel Martí2,3 José María Manzanares1
José María Manzanares1 Cristina Hernández5,6,7
Cristina Hernández5,6,7 Rafael Simó5,6,7*
Rafael Simó5,6,7* Albert Lecube2,3,4*
Albert Lecube2,3,4*- 1Endocrinology and Nutrition Department, University Hospital Sant Joan de Reus, Reus, Spain
- 2Endocrinology and Nutrition Department, University Hospital Arnau de Vilanova, Lleida, Spain
- 3Obesity, Diabetes and Metabolism (ODIM) Research Group, Institut de Recerca Biomèdica de Lleida (IRBLleida), Lleida, Spain
- 4Medicine and Surgery Department, University of Lleida, Lleida, Spain
- 5Endocrinology and Nutrition Department, Hospital Universitari Vall d’Hebron, Barcelona, Spain
- 6Diabetes and Metabolism Research Unit, Vall d’Hebron Institut de Recerca (VHIR), Barcelona, Spain
- 7Centro de Investigación Biomédica en Red de Diabetes y Enfermedades Metabólicas Asociadas (CIBERDEM), Instituto de Salud Carlos III (ISCIII), Madrid, Spain
Introduction: Individuals with type 2 diabetes (T2D) should be considered a susceptible group for pulmonary dysfunction. So, we aimed to evaluate the sensation of breathlessness in this population by administering two well-validated questionnaires.
Methods: This is a crosssectional study with 592 people without known respiratory disease (353 with T2D) who answered the modified Medical Research Council (mMRC) questionnaire. In addition, 47% also responded to the St George Respiratory Questionnaire, a specific instrument designed to be applied to patients with obstructive airway disease.
Results: Patients with T2D showed a higher mMRC score in comparison to the control group [1.0 (0.0 – 4.0) vs. 0.0 (0.0 – 4.0), p<0.001]. A higher prevalence of subjects with mMRC ≥2 was observed in T2D that in the control group (20.2% vs. 11.6%, p=0.004). Participants with T2D and mMRC ≥2 showed a higher HbA1c (8.2 ± 1.6% vs. 7.8 ± 1.6%, p=0.048), longer T2D evolution and higher prevalence of nephropathy. In the multivariate analysis, the presence of T2D [OR=1.95 (1.19 to 3.22), p=0.008] in all the population, and HbA1c [OR=1.19 (1.01 to 1.41), p=0.034] and the presence of diabetic nephropathy [OR=2.00 (1.14 to 3.52), p=0.015] in patients with T2D, predicted a mMRC ≥2. Finally, no differences were observed regarding the SGRQ score among groups.
Conclusions: Patients with T2D showed a greater sensation of dyspnea than subjects with normal carbohydrate metabolism. Risk factors included poor metabolic control and the presence of renal disease.
Introduction
Over the last decade, ample evidence has accumulated suggesting that type 2 diabetes (T2D) has a negative impact on lung function and nocturnal breathing (1, 2). Thus, different population-based studies have recurrently reported a decrease in spirometric results in patients with T2D, which is between 8 and 10% of the theoretical values (2, 3). A decrease in forced vital capacity, forced expiratory volume in first second, and diffusing capacity of the lungs for carbon monoxide have been described (4). Likewise, it has been described how pulmonary function impairment is present even in the prediabetes state (5). It has also been shown that the deterioration of lung function is associated with the degree of metabolic control (4, 6). In this way, optimization of metabolic control, independent of weight loss, has been associated with an improvement in spirometric values (7). In addition, data from the Fremantle Diabetes Study also showed that the duration of T2D was associated with reduced forced expiratory volume in first second and peak expiratory flow (8).
In the other hand, when the sleep period is evaluated, T2D also appears as an independent risk factor for experiencing greater hypoxemia, with a greater percentage of the sleep period with oxygen saturations below 90%, a greater number of episodes of desaturation and even a greater number of micro awakenings (4, 9). The deleterious impact of T2D on sleep breathing has also been revealed in the prediabetes stage (10). In fact, questionnaires as the Pittsburgh Sleep Quality Index (PSQI) and the Epworth Sleepiness Scale (ESS) have revealed how the presence of T2D adversely affect sleep quality and are independent risk factors for daytime sleepiness (11).
However, there are few data on the impact of altered spirometric parameters on the sensation of breathlessness in patients with T2D, and whether it is associated with the other late complications of diabetes. In addition, these studies have been conducted using different tools and including patients with pulmonary disease or cardiac disease (12, 13). For this reason, our aim was to evaluate the clinical impact of T2D on dyspneic sensation by administering two well-validated questionnaires as the modified medical research council (mMRC) dyspnea scale and the Saint George’s Respiratory Questionnaire (SGRQ) (14, 15). In addition, the coexistence of other classical chronic complications of T2D has also been evaluated.
Material and methods
Statement on ethics
The human ethics committee from the Arnau de Vilanova University Hospital and the Sant Joan de Reus University Hospital (CEIC-2173 and CEIM173/2019, respectively) approved the study. Written informed consent was obtained from all participants and the study was conducted according to the ethical guidelines of the Helsinki Declaration.
Design of the study and description of the study population
This is a crosssectional study to assess the dyspnea sensation in patients with T2D. Therefore, 476 patients were invited to participate from both University Hospitals from June 2020 to July 2022. The inclusion criteria were: (i) men and women, (ii) type 2 diabetes with at least three years of known disease, (iii) age between 45 and 75 years old, and (iv) available clinical and analytical data. Among the 446 participants who met the inclusion criteria, we excluded 93 for the following reasons: known chronic pulmonary disease or asthma (n=25), inability to answer the questionnaire correctly (n=11), clinically significant heart failure (n=9), dementia or suspicion of cognitive impairment (n=6), active cancer (n=5), and concomitant treatment with corticosteroid (n=3). In addition, 34 patients refused to participate in the study. No pregnant women were evaluated (Figure 1). In addition, data from 239 healthy subjects with normal carbohydrate metabolism and without pulmonary disease were recruited among the employees of our institutions and relatives of patients with T2D. We tried to match these individuals with patients with T2D by age (within 3 years range) and BMI (within 2.0 kg/m range). However, it was not possible to match both populations by sex. The main clinical features of the entire population are displayed in Table 1.
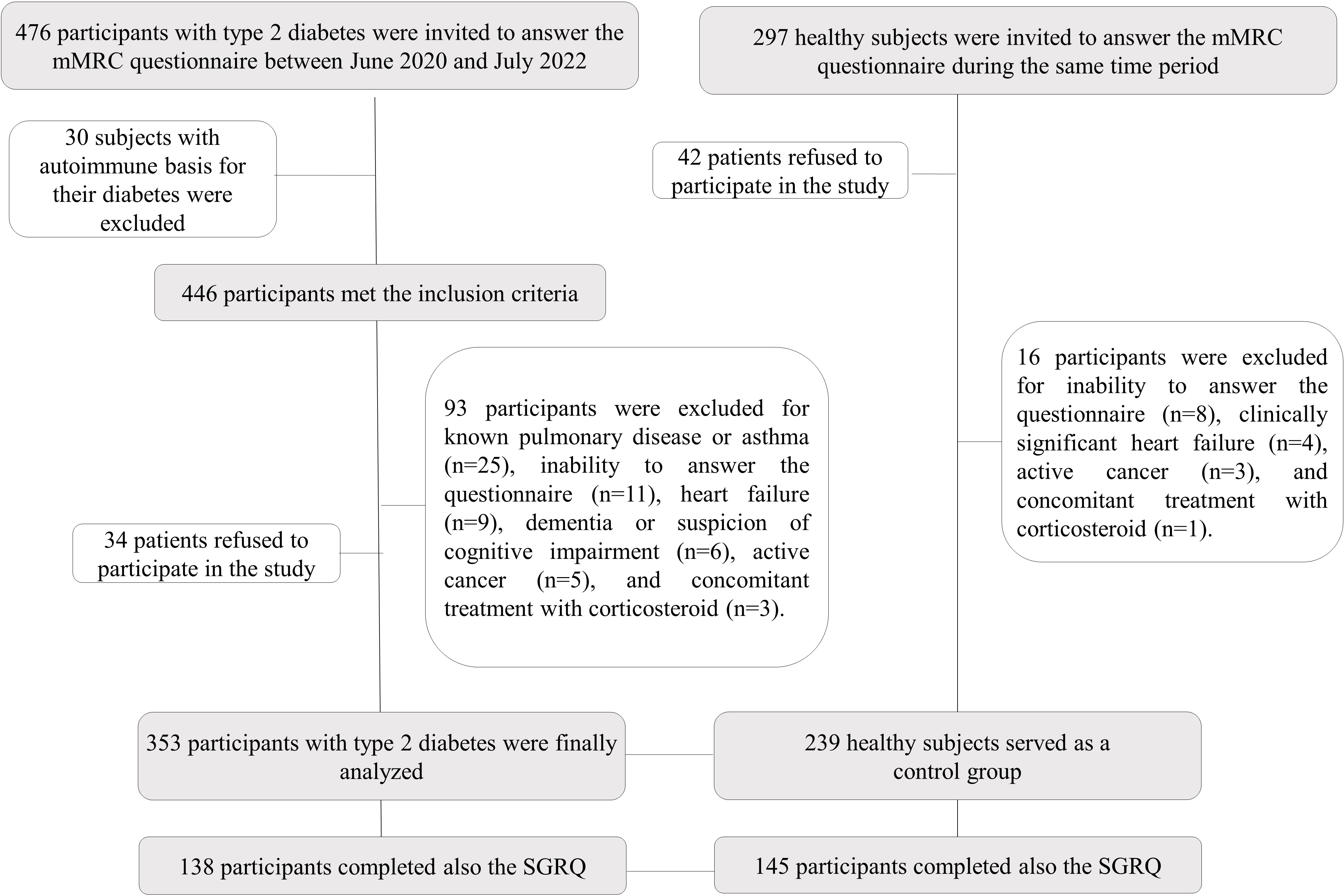
Figure 1 Flow Diagram for the study population.
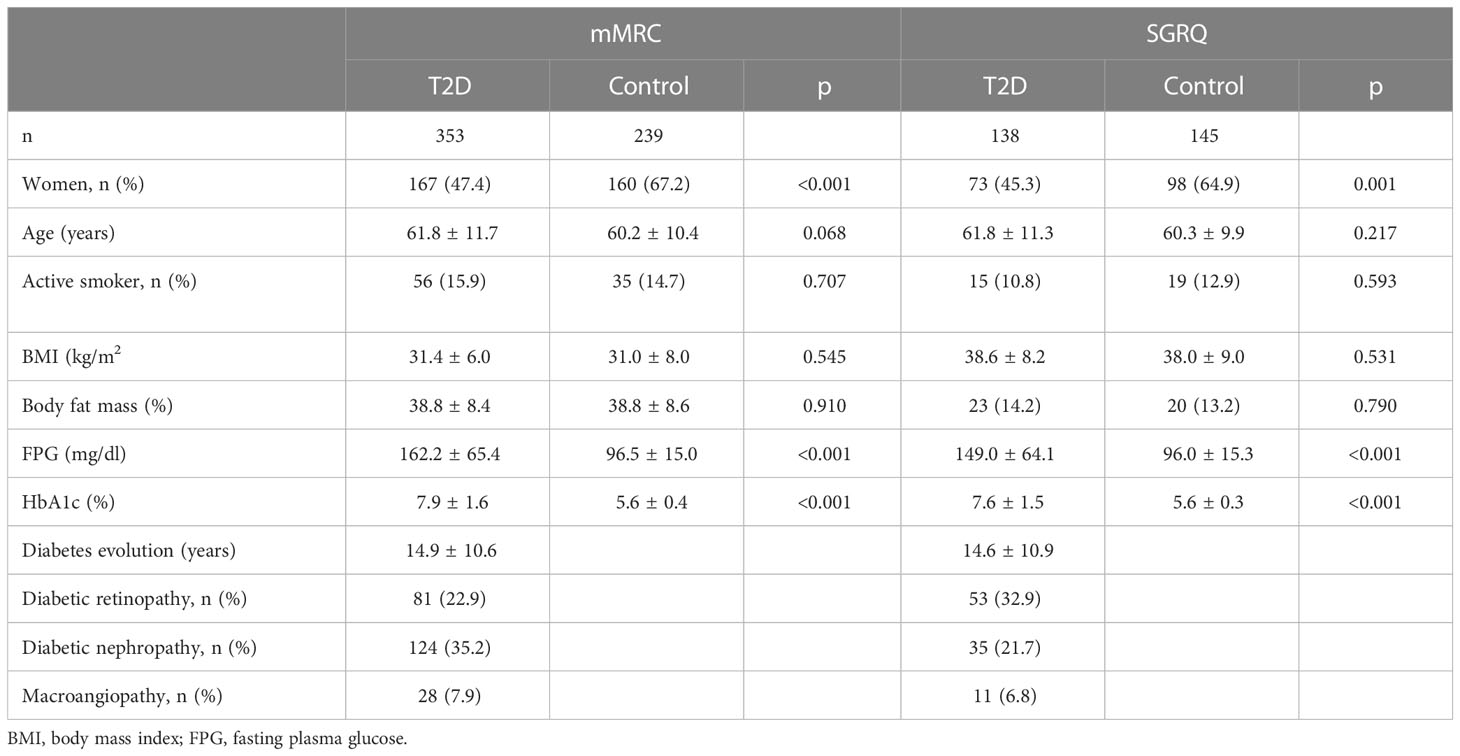
Table 1 Main clinical characteristics and comorbidities of the study population responding to the modified medical research council (mMRC) dyspnea scale and the Saint George’s Respiratory Questionnaire (SGRQ) according to the presence of type 2 diabetes.
Diagnosis of diabetes was done as stated by the American Diabetes Association guidelines (16). The study variables were obtained from the computerized clinical history of both centers: sex, age, anthropometry, and analytical parameters (glucose, HbA1c, glomerular filtration rate and albuminuria). Smoking habit (smokers who stopped smoking ≥1 year prior to recruitment were considered former smokers) was also assessed. Diabetic retinopathy was diagnosed whether a fundus examination done by indirect ophthalmoscopy or fundus photographs within at least two years before inclusion documented vascular abnormalities. Kidney disease was diagnosed according to KDIGO guidelines (17). No data were available on the presence of neuropathy. Finally, we used the Clínica Universidad de Navarra-Body Adiposity Estimator (CUN-BAE) to calculate the percentage of total body fat (18).
Questionnaires to evaluate dyspneic sensation
The modified medical research council (mMRC) dyspnea Scale is a questionnaire that assess perceived breathlessness on daily activities (14). The mMRC is a 5-point (0–4) scale based on the severity of dyspnea that ranges from grade 0 (“I only get breathless with strenuous exercise”) to grade 4 (“I am too breathless to leave the house or I am breathless when dressing”). Intermediate grades include “I get short of breath when hurrying on level ground or walking up a slight hill” (grade 1), “On level ground, I walk slower than people of the same age because of breathlessness, or I have to stop for breath when walking at my own pace on the level” (grade 2), and “I stop for breath after walking about 100 yards or after a few minutes on level ground” (grade 3). A total score of three or more can be used to predict hospitalization and exacerbation in patients with chronic obstructive pulmonary disease (19). In our population of patients with T2D without known pulmonary diseases we used the grade 2 as a cutoff point to diagnose positive dyspnea sensation (20). Moreover, the SGRQ is a standardized selfcompleted questionnaire for measuring impaired health and perceived wellbeing in respiratory tract diseases (15). It has 50 items with 76 weighted responses. Total score ranges from 0 to 100, with higher results indicating more respiratory limitations. This questionnaire also assesses dyspnea in 3 dimensions: (i) frequency and severity of respiratory symptoms (symptoms), (ii) limitation of activity owing to the symptoms (activity), and (iii) psychological and social functioning modifications (impact). The mMRC, the simplest questionnaire, was administered first, followed by the SGRQ to all participants. As described, the SGRQ is a longer and more complex questionnaire, which finally only 47.8% of the study population was able to complete correctly (Table 1).
Statistical analysis
A normal distribution of the variables was verified via the Kolmogorov–Smirnov test. Consequently, data were expressed as the mean ± SD, median (range) or as percentages. The major clinical data across the two groups were compared using Student’s t-test for continuous variables, and the Mann-Whitney U test for skewed data. Chi-squared test was done for categorical variables. Moreover, the link between variables was evaluated using the Pearson correlation test or ANOVA. A multivariable logistic regression model for the presence of a positive dyspnea sensation (mMRC ≥2) was done both in the entire population (including age, sex, BMI, smoking habit and the presence of T2D as confounding variables) and in patients with T2D (including known evolution of T2D, sex, BMI, smoking habit, HbA1c and the presence of diabetic nephropathy as confounding variables). Calibration of model was assessed using the Hosmer–Lemeshow test of fit and the area under the Receiver Operating Characteristic (ROC) curve. All p values were based on a 2-sided test for statistical significance. Significance was accepted as a p value less than 0.05. Statistical analyses were performed using the SPSS software (IBM SPSS Statistics for Windows, Version 27, Armonk, NY, USA).
Results
Patients with T2D showed a statistically higher mMRC score in comparison to the control group [1.0 (0.0 – 4.0) vs. 0.0 (0.0 – 4.0), p<0.001] (Table 2). Additionally, a higher prevalence of subjects with mMRC ≥2 was observed in patients with T2D than in the control group (20.2% vs. 11.6%, p=0.004) (Figure 2). When only participants with T2D were assessed, those with mMRC ≥2 were mainly women, older and heavier, showed a higher HbA1c (8.2 ± 1.6% vs. 7.8 ± 1.6%, p=0.048) without differences in FPG, more years with diabetes and higher prevalence of nephropathy (Table 3).
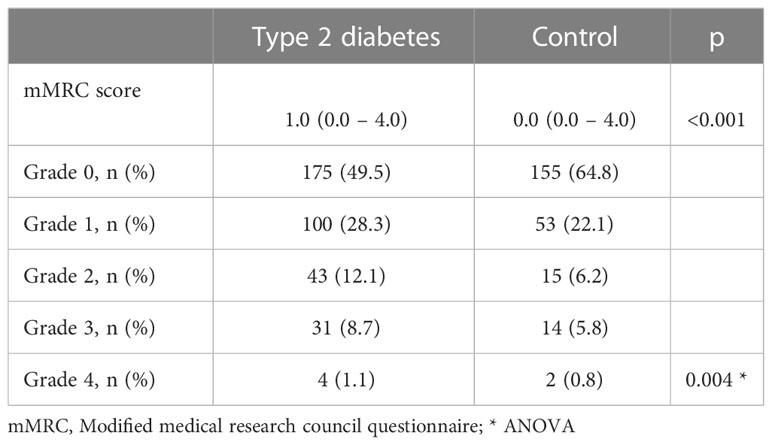
Table 2 Results of Modified medical research council questionnaire according to the presence of type 2 diabetes.
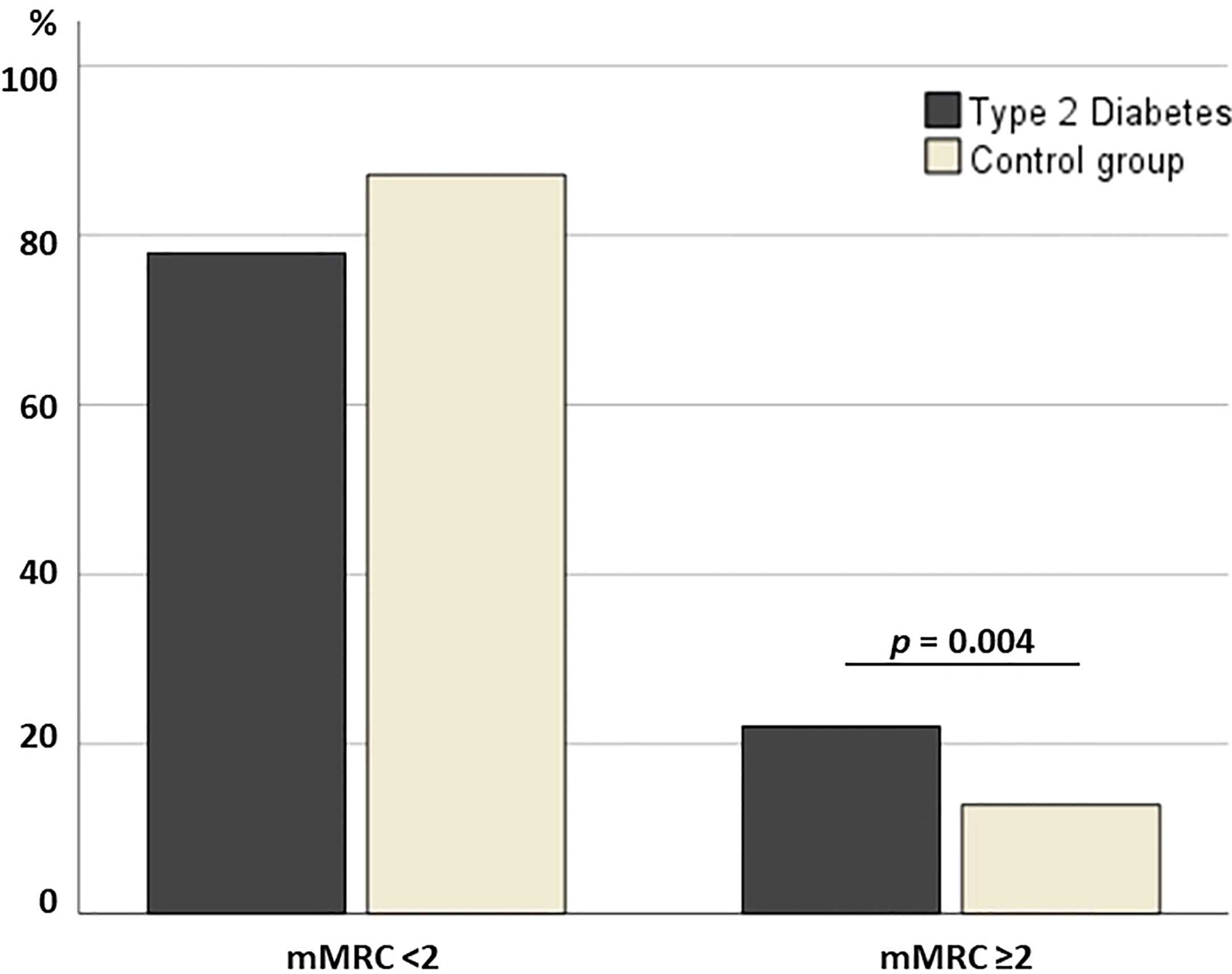
Figure 2 Bar plot displaying the prevalence of subjects with dyspneic sensation.
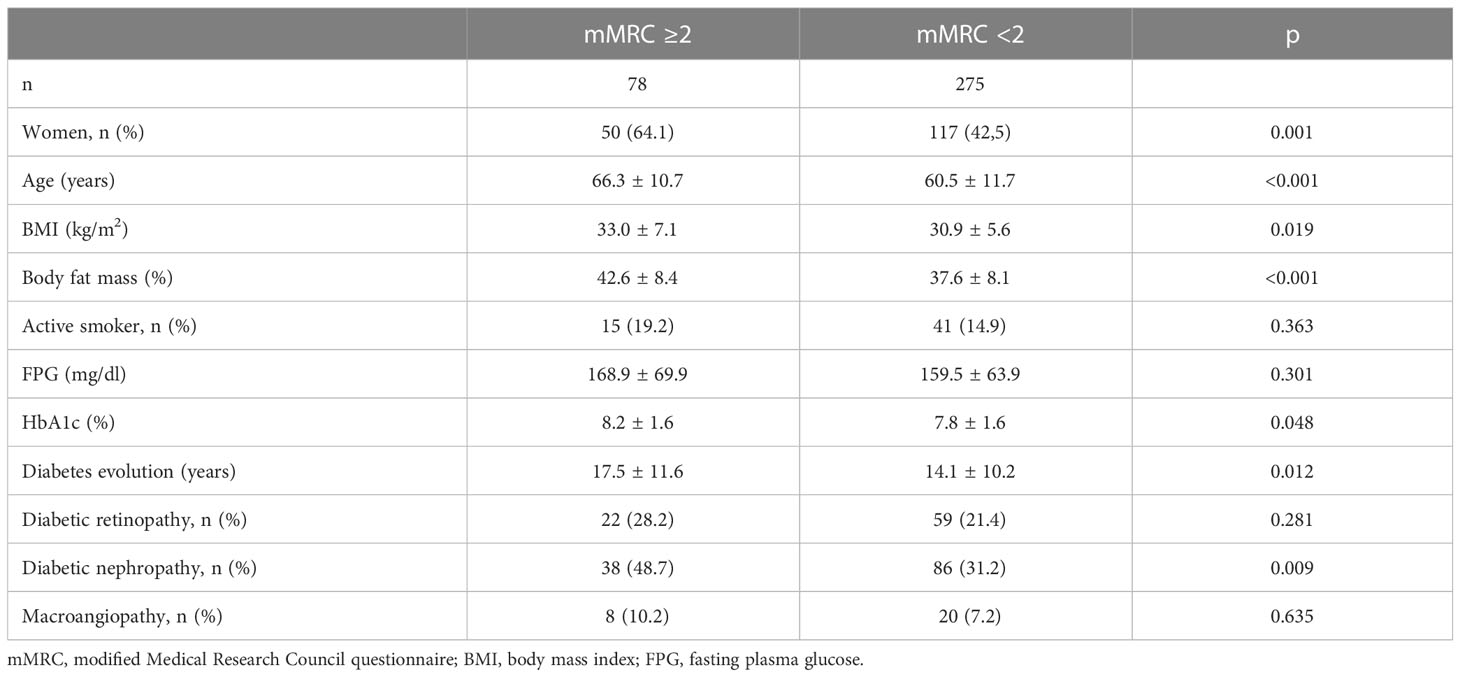
Table 3 Clinical characteristics of patients with type 2 diabetes according to the presence of a positive dyspneic sensation defined by a modified Medical Research Council questionnaire ≥2.
When the known evolution of T2D was less than 10 years, the prevalence of mMRC ≥2 was 14.1%, increasing to 25.5% when the evolution was ≥10 years (p=0.018) (Figure 3). In addition, the mMRC score was significantly higher in those patients with T2D and more than 10 years of evolution than in those with less time of disease [1.0 (0.0 – 4.0) vs. 0.0 (0.0 – 3.0), p=0.043]. Likewise, the prevalence of mMRC ≥2 increased from 18.3% in patients without kidney disease to 30.6% in those with diabetic nephropathy (p=0.009). Similarly, in patients with T2D the mMRC score raised from 0.0 (0.0 – 4.0) in those without to 1.0 (0.0 – 4.0) in those with nephropathy (p=0.047) (Figure 3). However, no differences were observed between patients with or without retinopathy (p=0.081) or macrovascular disease (0.467) in the mMRC score. In the multivariate analysis, when all the participants in the study were included, age, sex, BMI, active smoking habit and the presence of T2D [OR=1.95 (1.19 to 3.22), p=0.008] predicted the presence of a mMRC ≥2 (Table 4). When the analysis was restricted to patients with T2D, HbA1c [OR=1.19 (1.01 to 1.41), p=0.034] and the presence of diabetic nephropathy [OR=2.00 (1.14 to 3.52), p=0.015], but not years of evolution of the disease, appeared to be independently related with a mMRC ≥2 (Table 4).
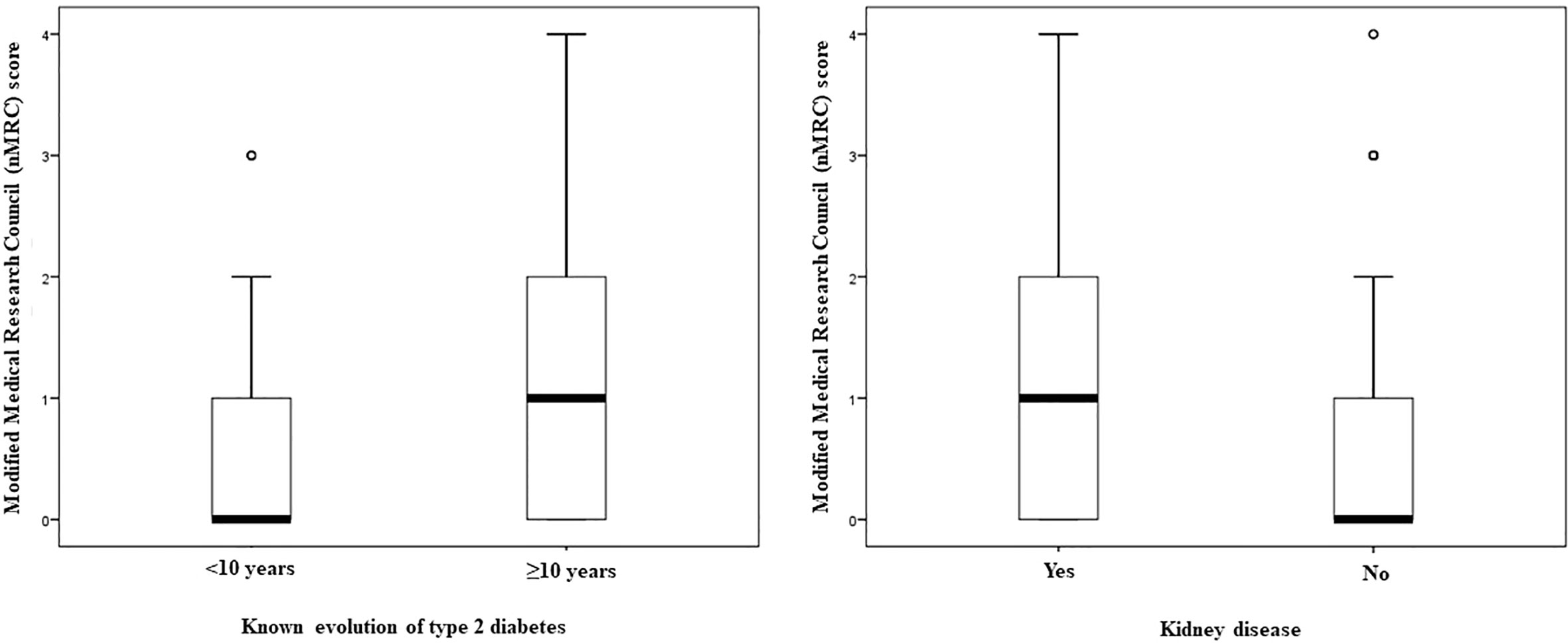
Figure 3 Box plots displaying the modified Medical Research Council score of subjects with type 2 diabetes according to years after diabetes diagnosis and the presence of kidney disease.
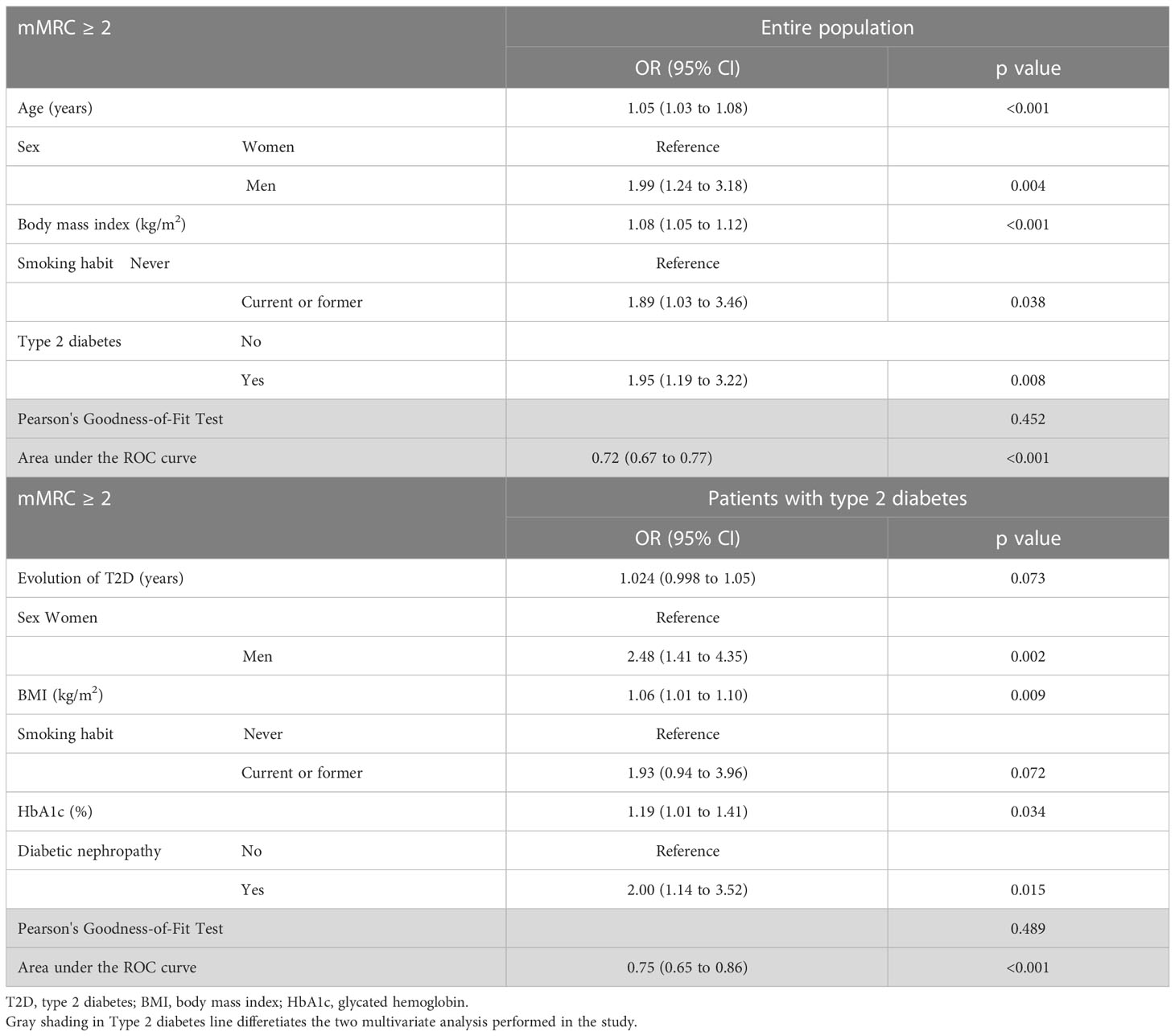
Table 4 A multinomial logistic regression model for presence of a modified Medical Research Council ≥2 in both the entire population and restricted to patients with type 2 diabetes.
Regarding the SGRQ, no differences were observed in the total score among groups [14.3 (0.0 - 75.3) in T2D vs. 12.2 (0.0 - 65.6) in controls, p=0.923] nor in the symptoms [8.8 (0.0 - 61.7) vs. 8.8 (0.0 - 75.7), p=0.698], activity [23.8 (0.0 - 100.0) vs. 18.4 (0.0 - 100.0), p=0.690] and impact [4.6 (0.0 - 69.5) vs. 4.8 (0.0 to 57.2), p=0.827] domains of the questionnaire. In the univariate analysis, the total score of the SGRQ showed a significant correlation with BMI (r=0.212, p<0.001) and total body fat (r=0.214, p<0.001), but not with age (r=0.054, p=0.327), FPG (r=0.056, p=0.396) or HbA1c (r=0.021, p=0.794).
Discussion
This is a cross-sectional study that provides evidence in favor of the idea that T2D has a negative impact on lung function that is associated with an increased selfperceived sense of dyspnea. This sensation would appear during activities of daily living and can be assessed with simple questionnaires.
Even though previous studies have shown that patients with T2D have decreased lung capacity compared to the general population, few have so far evaluated the clinical impact that diabetes may have on the sensation of dyspnea (21). It has been suggested that since the pulmonary microvascular bed is the largest in humans, great involvement is required for any type of symptom and disability to appear (4). Thus, the involvement of other organs and systems with a smaller microvasculature, such as the retina or the kidney, would appear more quickly in patients with T2D, despite a similar severity of anatomic involvement (20). Therefore, the deleterious impact of diabetes on the lungs would result in dysfunctions that would remain undiagnosed for a long period of time if screening is not proposed in routine clinical practice (4).
Dyspnea is a heterogeneous symptom that can only be known through a patient’s report and can be present quantitatively and qualitatively different among patients (22). However, knowledge of its evolution is important for the diagnosis and monitoring of patients with T2D who will require a complementary study of their pulmonary function. In this way, the mMRC scale is a simple and quick self-assessment tool that measure the degree of disability that dyspnea poses to daily activities with a simple question (14). Kopf et al. showed a progressive increase in the mMRC score from controls (n=48) to patients with prediabetes (n=68), patients with newly diagnosed T2D (n=29) and patients with long term diabetes (n=110) (23). This result is in line with the fact than in the entire population of our study the presence of T2D appeared to be an independent factor to score ≥2 in the mMRC. In parallel, the 14.1% to 25.5% increase that we have described when the known duration of T2D exceeds 10 years support that the symptomatic dyspnea appears progressively in patients with T2D, in whom disease evolution must be added to other factors such as sex and BMI.
In Italy, in the framework of the GEIRD (Gene Environment Interactions in Respiratory Diseases) study, De Santi et al. showed how a group of 259 patients with T2D reported more frequently than the general population a dyspnea that limited walking on level ground (grade 2 mMRC dyspnea) (12). In fact, the odds ratio of grade 2 mMRC dyspnea among patients with T2D was almost four [3.92 (3.28 - 4.68), p <0.001] in the 4554 age group and decreased to 1.79 (1.68 - 1.91; p <0.001) in the 75 - 84 age group. More recently, the Canadian Longitudinal Study on Aging evaluated the potential risk factors for dyspnea (measured by mMRC) in 28,854 adults aged 45 to 85 years old (21). Even the population also comprised subjects with lung disease, depression and heart disease, the study described how the adjusted odds ratio for dyspnea “walking on flat surfaces” was highest in patients with T2D (21). It is important to note that both studies included participants with asthma and chronic obstructive pulmonary disease, so the origin of dyspnea cannot be attributed exclusively to the presence of diabetes. To avoid this bias, we were careful to exclude other causes that could favor the presence of dyspnea, such as pulmonary disease or clinically significant heart failure. However, we could not rule out the presence of heart failure with preserved ejection fraction that could also favor respiratory symptomatology (24).
The Hispanic Community Health Study/Study of Latinos (HCHS/SOL) is a large, multicenter observational study that included 2,300 T2D patients without lung disease and assessed symptomatic lung impairment using the Baseline Dyspnea Index (BDI) questionnaire, which provides measures significantly related to the mMRC (25, 26). Key results showed a significantly higher breathlessness score in people with T2D compared to the population without diabetes [0.60 (0.49–0.71) vs. 0.41 (0.34–0.49), p<0.001]. This study was the first to show that the impairment in the dyspnea score correlated with the ratio, rising by 0.02 ± 0.006 per 100 mg/g increase in those patients without previous disease (25). In this way, Vracko et al. described in the year 1979 how the thickness of the epithelial and capillary basal laminae of alveoli correlated significantly with thickness of basal laminae in renal tubules (27). In our study, the prevalence of mMRC ≥2 doubled from 18.3% to 30.6% in patients with T2D with and without diabetic kidney disease. These data were corroborated by multivariate analysis, in which the presence of diabetic nephropathy significantly increased the risk of obtaining a mMRC score equal or higher than 2.
None of the studies cited above have established a correlation between metabolic control and dyspnea symptoms in patients with T2D (12, 21). However, in our cohort of patients with T2D, not only did those with an mMRC score ≥2 have significantly higher HbA1c values than those with a lower mMRC score, but HbA1c was also an independent factor related to the presence of positive dyspnea sensation in the multivariate analysis. Taken together, our results reinforce the negative impact of T2D on lung function and the importance of achieving good metabolic control in the treatment of this complex disease.
Finally, when the Saint George’s respiratory questionnaire was administered to participants with and without T2D, no differences were found between groups not only in the total score, but also in the dimensions of symptoms, activity and impact. These contradictory results could be partly explained by the fact that this questionnaire is a specific instrument designed to be applied to patients with obstructive airway disease, capable of measuring the impact on patients’ general health, daily life and perceived wellbeing. Therefore, when administered to patients without known lung disease, this instrument may not be sensitive and specific enough to detect small differences between patients with and without T2D.
This study has some limitations that need to be considered. The first is that dyspnea is a subjective sensation that changes according to each patient’s perception of their state of health. However, it is important to know how patients with diabetes perceive and self-report this sensation, as it can help us to identify those who need a more extensive evaluation of their lung function. In addition, the lack of information on the presence of established neuropathy in our cohort of patients with type 2 diabetes prevents us from ruling out that low-grade neuropathy translates into a feeling of increased dyspnea. Secondly, we have not correlated the sensation of dyspnea with lung function, so we cannot state that patients with the highest score on the mMRC are those who also have the most affected spirometric values. However, previous studies have well established that the mMRC scale is recommended for assessing dyspnea and an mMRC scale grade equal to or greater than 3 can be used to predict hospitalization and exacerbation in patients with chronic obstructive pulmonary disease (14, 19). Third, the treatment of T2D has not been evaluated. In this regard, there is evidence that glucagon-like peptide 1 receptor agonists, such as liraglutide, have a positive effect on lung function, independent of the weight reduction associated with their use (28). Finally, it should be remembered that our population of patients with diabetes was recruited from the outpatient clinics of two university hospitals, being heterogeneous in terms of factors such as sex and age, so it is possible that the results obtained cannot be generalized to other groups of patients.
Conclusions
Patients with T2D showed a greater sensation of dyspnea than subjects with normal carbohydrate metabolism. Risk factors included male sex and higher BMI, but also poor metabolic control and the presence of renal disease. These data support the fact that the lungs should be considered a target organ for late complications of T2D and that, consequently, the symptomatology that may result from pulmonary dysfunction should be investigated.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by The human ethics committee from the Arnau de Vilanova Hospital University and the Sant Joan de Reus University Hospital (CEIC2173 and CEIM173/2019, respectively). The patients/participants provided their written informed consent to participate in this study.
Author contributions
CM and ES contributed equally to this work. All authors contributed to the article and approved the submitted version.
Funding
This research was supported by grants from Instituto de Salud Carlos III (PI15/00260), Fondos FEDER “Una manera de hacer Europa”), and Sociedad Española de Endocrinología y Nutrición. CIBER de Diabetes y Enfermedades Metabólicas Asociadas (CIBERDEM) is an initiative of the Instituto Carlos III.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Zhang RH, Cai YH, Shu LP, Yang J, Qi L, Han M, et al. Bidirectional relationship between diabetes and pulmonary function: a systematic review and metaanalysis. Diabetes Metab (2021) 47:101186. doi: 10.1016/j.diabet.2020.08.003
2. van den Borst B, Gosker HR, Zeegers MP, Schols AMWJ. Pulmonary function in diabetes: a metaanalysis. Chest. (2010) 138:393–406. doi: 10.1378/chest.09-2622
3. Klein OL, Krishnan JA, Glick S, Smith LJ. Systematic review of the association between lung function and type 2 diabetes mellitus. Diabetes Med (2010) 27:977987. doi: 10.1111/j.1464-5491.2010.03073.x
4. Lecube A, Simó R, Pallayova M, Punjabi NM, López-Cano C, Turino C, et al. Pulmonary function and sleep breathing: two new targets for type 2 diabetes care. Endocr Rev (2017) 38:550573. doi: 10.1210/er.2017-00173
5. Sánchez E, Gutiérrez-Carrasquilla L, Barbé F, Betriu À, López-Cano C, Gaeta AM, et al. ILERVAS project. lung function measurements in the prediabetes stage: data from the ILERVAS project. Acta Diabetol (2019) 56:10051012. doi: 10.1007/s00592-019-01333-6
6. Yeh HC, Punjabi NM, Wang NY, Pankow JS, Duncan BB, Cox CE, et al. Crosssectional and prospective study of lung function in adults with type 2 diabetes: the atherosclerosis risk in communities (ARIC) study. Diabetes Care (2008) 31:741–6. doi: 10.2337/dc07-1464
7. Gutiérrez-Carrasquilla L, Sánchez E, Barbé F, Dalmases M, López-Cano C, Hernández M, et al. Effect of glucose improvement on spirometric maneuvers in patients with type 2 diabetes: the sweet breath study. Diabetes Care (2019) 42:617624. doi: 10.2337/dc18-1948
8. Davis TM, Knuiman M, Kendall P, Vu H, Davis WA. Reduced pulmonary function and its associations in type 2 diabetes: the fremantle diabetes study. Diabetes Res Clin Pract (2000) 50:153–9. doi: 10.1016/S0168-8227(00)00166-2
9. Lecube A, Sampol G, Lloberes P, Romero O, Mesa J, Hernández C, et al. Diabetes is an independent risk factor for severe nocturnal hypoxemia in obese patients. A case-control study. PloS One (2009) 4:e4692. doi: 10.1371/journal.pone.0004692
10. Sánchez E, Sapiña-Beltrán E, Gavaldà R, Barbé F, Torres G, Sauret A, et al. On behalf of the ilervas project collaborators. prediabetes is associated with increased prevalence of SleepDisordered breathing. J Clin Med (2022) 11:1413. doi: 10.3390/jcm11051413
11. Lecube A, Sánchez E, Gómez-Peralta F, Abreu C, Valls J, Mestre O, et al. Global assessment of the impact of type 2 diabetes on sleep through specific questionnaires. A Case-Control Study. PloS One (2016) 11:e0157579. doi: 10.1371/journal.pone.0157579
12. De Santi F, Zoppini G, Locatelli F, Finocchio E, Cappa V, Dauriz M, et al. Type 2 diabetes is associated with an increased prevalence of respiratory symptoms as compared to the general population. BMC Pulm Med (2017) 17:101. doi: 10.1186/s12890-017-0443-1
13. Guazzi M, Arena R. Type 2 diabetes and exercise unexplained dyspnoea: a new focus under the lens with a long way to go yet. Eur J Prev Cardiol (2023) 30:123124. doi: 10.1093/eurjpc/zwac177
14. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the medical research council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. (1999) 54:581586. doi: 10.1136/thx.54.7.581
15. Jones PW, Quirk FH, Baveystock CM. The St george’s respiratory questionnaire. Respir Med (1991) 85:25–31. doi: 10.1016/S0954-6111(06)80166-6
16. American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care (2021) 44:S15S33. doi: 10.2337/dc21-S002
17. Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. Kidney disease: improving global outcomes (KDIGO) glomerular diseases work group. KDIGO 2021 clinical practice guideline for the management of glomerular diseases. Kidney Int (2021) 100:S1S276. doi: 10.1016/j.kint.2021.05.021
18. Gómez-Ambrosi J, Silva C, Catalán V, Rodríguez A, Galofré JC, Escalada J, et al. Clinical usefulness of a new equation for estimating body fat. Diabetes Care (2012) 35:383388. doi: 10.2169/internalmedicine.55.4490
19. Natori H, Kawayama T, Suetomo M, Kinoshita T, Matsuoka M, Matsunaga K, et al. Evaluation of the modified medical research council dyspnea scale for predicting hospitalization and exacerbation in Japanese patients with chronic obstructive pulmonary disease. Intern Med (2016) 55:1524. doi: 10.2169/internalmedicine.55.4490
20. Richards JB. Calculated decisions: mMRC (Modified medical research council). Dyspnea Scale. Emerg Med Pract (2017) 19:12.
21. Verschoor CP, Cakmak S, Lukina AO, Dales RE. Activityrelated dyspnea in older adults participating in the Canadian longitudinal study on aging. J Gen Intern Med (2022) 37:33023309. doi: 10.1007/s11606-021-07374-4
22. Campbell ML. Dyspnea. Crit Care Nurs Clin North Am (2017) 29:461470. doi: 10.1016/j.cnc.2017.08.006
23. Kopf S, Groener JB, Kender Z, Fleming T, Brune M, Riedinger C, et al. Breathlessness and restrictive lung disease: an important DiabetesRelated feature in patients with type 2 diabetes. Respiration. (2018) 96:2940. doi: 10.1159/000488909
24. Gevaert AB, Kataria R, Zannad F, Sauer AJ, Damman K, Sharma K, et al. Heart failure with preserved ejection fraction: recent concepts in diagnosis, mechanisms and management. Heart. (2022) 108:13421350. doi: 10.1136/heartjnl-2021-319605
25. Klein OL, AvilesSanta L, Cai J, Collard HR, Kanaya AM, Kaplan RC, et al. Hispanics/Latinos with type 2 diabetes have functional and symptomatic pulmonary impairment mirroring kidney microangiopathy: findings from the Hispanic community health Study/Study of latinos (HCHS/SOL). Diabetes Care (2016) 39:20512057. doi: 10.2337/dc16-1170
26. Mahler DA, Wells CK. Evaluation of clinical methods for rating dyspnea. Chest. (1988) 93:5806. doi: 10.1378/chest.93.3.580
27. Vracko R, Thorning D, Huang TW. Basal lamina of alveolar epithelium and capillaries: quantitative changes with aging and in diabetes mellitus. Am Rev Respir Dis (1979) 120:973983. doi: 10.1164/arrd.1979.120.5.973
Keywords: diabetes complications, dyspneic sensation, type 2 diabetes, respiratory symptoms, questionnaires
Citation: Mizab C, Sánchez E, Gutiérrez-Carrasquilla L, Balsells N, Arqué A, Ruano R, Mateu M, Zorzano-Martínez M, Pomés A, García-Aguilera E, Martí R, Manzanares JM, Hernández C, Simó R and Lecube A (2023) Assessment of dyspneic sensation in patients with type 2 diabetes. Front. Endocrinol. 14:1208020. doi: 10.3389/fendo.2023.1208020
Received: 18 April 2023; Accepted: 14 June 2023;
Published: 10 August 2023.
Edited by:
Christian Göbl, Medical University of Vienna, AustriaReviewed by:
Aleksandra Klisic, Primary Health Care Center Podgorica, MontenegroKenneth Nugent, Texas Tech University Health Sciences Center, United States
Duy-Thai Nguyen, Ministry of Health, Vietnam
Copyright © 2023 Mizab, Sánchez, Gutiérrez-Carrasquilla, Balsells, Arqué, Ruano, Mateu, Zorzano-Martínez, Pomés, García-Aguilera, Martí, Manzanares, Hernández, Simó and Lecube. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rafael Simó, rafael.simo@vhir.org; Albert Lecube, alecube@gmail.com
†These authors have contributed equally to this work and share first authorship