Sensory Snack Time: A School-Based Intervention Addressing Food Selectivity in Autistic Children
 James Galpin
James Galpin Laura Osman1
Laura Osman1 - 1The Bridge London Trust, London, United Kingdom
- 2Nutrition and Dietetics Department, The Whittington Hospital, NHS Trust, London, United Kingdom
Difficulties with diet and mealtimes, often exacerbated by food selectivity have been highlighted as priority areas of support by parents of autistic children. There is a large body of evidence noting the significant relationship between sensory differences and greater food selectivity in individuals on the autism spectrum. In order to address the needs expressed by parents the present study examined the effect of a whole class, sensory based feeding intervention carried out in a special school setting that was integrated into part of the daily school routine. The intervention sought to become self-sustaining with minimal financial and time costs. In total 23 autistic pupils aged 4–10 took part in the Sensory Snack Time intervention. Results indicated that pupils ate a wider variety of foods and displayed significantly reduced food selectivity, distressed mealtime behaviors, and food refusal following the 12-week intervention. Furthermore, the intervention was successfully integrated into everyday practice and was successfully implemented by existing school staff. Further research is necessary to qualify the precise impact the intervention had on supporting pupils to manage sensory based aversions to foods and to examine the potential for the intervention to be generalized to main meals and different settings, such as pupils' homes.
Introduction
Feeding problems in childhood are relatively common, with feeding or eating difficulties identified in at least 25% of neurotypically developing children (Lindberg et al., 1991; Manikam, 2000; Silverman et al., 2009), however, these problems are at least twice as prevalent in children on the autism spectrum.1. Feeding or eating difficulties are widely recognized as problematic for autistic children (Schreck et al., 2004; Schreck and Williams, 2006; Provost et al., 2010; Nadon et al., 2011a,b; Kral et al., 2013; Sharp et al., 2013; Hubbard et al., 2014; Marí-Bauset et al., 2014; Suarez et al., 2014b) and are often compounded by co-occurring difficulties such as highly idiosyncratic food preferences, the need for food to be presented in specific ways, a narrow diet, aversion to a range of textures, and pica (Kerwin et al., 2005; Schreck and Williams, 2006; Martins et al., 2008; Cermak et al., 2010; Seiverling et al., 2010; Hendy et al., 2013).
Commonly identified early childhood eating and feeding problems (such as picky eating) in the neurotypical population are often seen as mild or transient (Bernard-Bonnin, 2006; Mascola et al., 2010) whereas for autistic children these difficulties have been found to persist past childhood remaining a significant difficulty into adolescence and adulthood (Cornish, 2002; Suarez et al., 2014b; Kuschner et al., 2015) and can lead to inadequate nutrition and a range of negative outcomes including weight loss, impaired cognitive development, malnutrition and poor overall health, and growth (Keen, 2008; Schmitt et al., 2008; Herndon et al., 2009; Bandini et al., 2010). As Johnson et al. (2014) noted, across the existing literature three categories of feeding difficulties in autistic children are highlighted: food selectivity, food refusal, and disruptive mealtime behaviors (see Johnson et al., 2014). Of these, food selectivity (that might present as a preference for, or avoidance of, foods based on smell, texture, or color), is identified as being the most common difficulty (Fodstad and Matson, 2008; Twachtman-Reilly et al., 2008; Laud et al., 2009; Matson and Fodstad, 2009; Bandini et al., 2010; Cermak et al., 2010; Sharp et al., 2013; Marí-Bauset et al., 2014; Rastam and Wentz, 2014) and has a significant association with disruptive mealtime behavior (Curtin et al., 2015).
The prevalence rate of food selectivity in children on the autism spectrum has shown a large variability, Postorino et al. (2015) report that differing definitions of food selectivity, along with a lack of consistent methodology, may account for the range in the prevalence rate of 13 to 87% in the existing literature (Postorino et al., 2015). Bandini et al. (2010) looked to operationalise the term “food selectivity,” suggesting that it was comprised of three domains: food refusal, limited food repertoire, and high frequency single food intake (HFSFI). Whilst the HFSFI domain was not found to be a significant problem for autistic individuals, their study supported previous findings regarding the negative impact that limited food repertoire has upon nutritional intake (Herndon et al., 2009; Bandini et al., 2010; Bicer and Alsaffar, 2013). As a result of the potential health impact of a limited food repertoire this is often the primary focus of examination of food selectivity in children on the autism spectrum (Cermak et al., 2010; Rastam and Wentz, 2014). Research has, therefore, sought to explore why there is such a high level of food selectivity in autistic compared to both neurotypical children and children with other developmental differences (Field et al., 2003; Schreck et al., 2004; Twachtman-Reilly et al., 2008; Sharp et al., 2010), especially as parent reports suggests that it is not a result of lack of appetite (Williams et al., 2000). The core diagnostic feature of restricted interests and repetitive behaviors has been suggested as an underlying cause of some of the behaviors associated with food selectivity, such as rigidity in the way in which food is presented and rigid mealtime rules (Twachtman-Reilly et al., 2008). There is, however, an increasing amount of evidence to support the causal relationship between sensory differences (such as hypo- or hyperreactivity to sensory input) and food selectivity in children on the autism spectrum (Cermak et al., 2010). The focus on mealtime behavior or sensory differences has informed current feeding interventions for autistic children.
Behavioural Interventions
The effectiveness of behavioral interventions have received empirical support in the treatment of children's feeding problems (Ahearn, 2002; Ledford and Gast, 2006; Greer et al., 2008; Bachmeyer, 2009; Sharp et al., 2010; Gale et al., 2011; Silbaugh et al., 2016). The majority of existing behavioral research depicting effective specific feeding treatment protocols consist of single case studies or small sample sizes (Najdowski et al., 2003; Tarbox et al., 2010; Peterson et al., 2016). These describe a variety of approaches that were found to be effective in these cases (see Silbaugh et al., 2016 for a recent review). However, the high professional to child ratio of these interventions could limit their effectiveness in school settings. Indeed, we were unable to find any studies that had examined a whole class approach delivered in a school setting and there is a need for studies to take into account the ecology of the school setting (Ledford et al., 2018). There are also wider concerns regarding the replicability of the positive effects of some specific behavioral interventions (Silbaugh and Swinnea, 2018) and the generalisability of behavioral treatments to foods that have not been specifically targeted in the intervention (Peterson et al., 2016), highlighting the need for more research in this area. Whilst behavioral interventions for food selectivity have shown promise, and the growth of evidence from single-case designs is promising, behavioral interventions have not been found to meet Council for Exceptional Children criteria for evidence-based practice (Silbaugh et al., 2016). Furthermore, behavioral based interventions can often fail to take into account sensory challenges children face in feeding and the extent to which they impact upon food selectivity (Overland, 2011). By focussing specifically on behavior an intervention may fail to recognize that the sensory experience of certain foods may well be a negative one for autistic children. As such food selectivity, perpetuated by refusal of new foods, and potentially negative behaviors around the acceptance of new foods, should be seen as an adaptive and communicative response to a physiologically motivated difficulty. The current study seeks to address the need for further research that examines interventions that address food selectivity and sensory differences with larger samples of children in a naturalistic setting (Ledford et al., 2018).
Sensory Approach
Sensory differences in autism have been increasingly recognized as a result of first-hand accounts (Grandin, 1992, 2000; Williams, 1994; Jones et al., 2003) as well as wider research highlighting the prevalence of hyper- or hyporeactivity to sensory input in autistic individuals (Leekam et al., 2007; Tomchek and Dunn, 2007; Ben-Sasson et al., 2009; Baum et al., 2015). Clinical recognition of these differences came with the revised diagnostic criteria for autism that included, for the first time, differences in sensory processing (DSM 5; American Psychiatric Association, 2013). Specifically sensory differences in processing in the proximal domains of touch and smell/taste have been shown to distinguish autism and non-autism groups (Schreck et al., 2004; Schreck and Williams, 2006; Leekam et al., 2007; Tomchek and Dunn, 2007), thereby potentially implicating sensory differences as a cause of food selectivity (Williams et al., 2000; Rastam, 2008; Twachtman-Reilly et al., 2008; Cermak et al., 2010). Indeed, specific contextual factors such as texture, taste, temperature, smell, and consistency of foods, have been reported to be associated with food selectivity (Whiteley et al., 2000; Williams et al., 2000; Schreck et al., 2004; Seiverling et al., 2010, 2011; Kuschner et al., 2015; Luisier et al., 2015; Postorino et al., 2015). The growing body of evidence supporting the significant relationship between sensory differences and greater food selectivity not only in autistic individuals (Matson and Fodstad, 2009; Cermak et al., 2010; Nadon et al., 2011b; Suarez et al., 2012, 2014b; Beighley et al., 2013; Mazurek et al., 2013; Johnson et al., 2014; Zobel-Lachiusa et al., 2015; Chistol et al., 2018) but also in typically developing children (Farrow and Coulthard, 2012; Johnson et al., 2015; Coulthard et al., 2016) and those with an intellectual disability (Engel-Yeger et al., 2016) should not therefore be surprising. These findings, therefore, highlight the need for food selectivity interventions to focus on the sensory components of eating (Nadon et al., 2011b; Chistol et al., 2018; Nederkoorn et al., 2018). An understanding of the potential sensory basis for food selectivity informed the approach developed for the current study.
A sensory based approach will often focus on encouraging tactile and oral exploration, looking to normalize sensation, as the first steps to addressing food selectivity (Twachtman-Reilly et al., 2008) rather than addressing the behavior being displayed as the primary concern. Indeed, sensory-based activities have been shown to facilitate the behavioral readiness needed for improved performance of functional skills that would be required for eating (Field et al., 1997; Fertel-Daly et al., 2001; Smith et al., 2005; Schaaf and Nightlinger, 2007). One sensory based approach that is growing in popularity, particularly in clinical settings in the US, is the sequential oral sensory (SOS) approach (Toomey and Ross, 2011; Benson et al., 2013; Peterson et al., 2016). The SOS approach is typically a 12-week, therapist delivered program that is based on the typical developmental steps involved with feeding (Benson et al., 2013). Play is also central to the approach which aims to “increase the range and volume of foods the child will eat through a play-based intervention” (Toomey and Ross, 2011, pg. 86). The approach has developed a six step eating hierarchy (visual tolerance, interaction, smell, touch, taste, and eating) as the protocol to advance the child forwards with exposure and experiences of a variety of foods and textures based on the child's response to each step (Toomey and Ross, 2011). The rationale behind the intervention is that a process of systematic desensitization, in the context of the six step hierarchy children begin to interact with and eat a wider variety of foods (Mattingly et al., 2015). Whilst not initially developed specifically for autistic individuals, it is increasingly being used to address feeding difficulties, such as restricted diet, experienced by children on the autism spectrum (Benson et al., 2013; Peterson et al., 2016). As with behavioral interventions reviewed by Silbaugh et al. (2016), sensory-based approaches cannot yet be seen to meet the criteria for evidence-based practice. Whilst there has been some empirical support for sensory approaches (Benson et al., 2013; Aswathy et al., 2016; Reinoso et al., 2018), a randomized control trial, of a modified SOS approach (M-SOS) was not found to be effective in addressing food selectivity in four of the six children who took part (Peterson et al., 2016). One potential reason for this may have been that the “play-based” element may not have been as child-led as originally proposed in the SOS approach, the M-SOS being “not the true and comprehensive SOS method” (Peterson et al., 2016, p.3). Despite this limitation and the research literature highlighting the relationship between sensory differences and food selectivity in autism (Zobel-Lachiusa et al., 2015) further research is still needed to examine sensory based approaches to addressing food selectivity in autistic children. We found no studies that have examined this type of approach within a UK school setting. As with behavioral interventions, one potential barrier to implementation of sensory based interventions are the resources required to implement them. The SOS program, for example, whilst recommended to be delivered in a group setting, is often delivered by a multi-disciplinary team that may consist of a speech and language therapist, occupational therapist and dietician (Boyd, 2007) at least one of whom is required to be trained in the SOS method. Whilst the involvement of such a wide range of professionals will be beneficial, the reality in many schools is that they do not have such resources available to them. The current study is therefore not only unique in terms of examining an intervention that can be integrated into everyday school practice using existing staff and resources but also in that it sought to respond to calls to address the research to practice gap in autism research (Dingfelder and Mandell, 2011; Carrington et al., 2016; Guldberg, 2017).
Aim
The current study sought to address food selectivity across a sample of children attending a primary school for pupils with autism and/or profound and multiple learning difficulties in inner-city London. A brief survey of staff in the setting highlighted the prevalence of pupils for whom mealtimes were an area of struggle. Previous research has highlighted the negative impact that eating difficulties can have on pupils within the educational setting (Koenig and Rudney, 2010). In line with previous studies that have shown a strong correlation between mealtime behavior and parental stress and a negative impact on family life (Kerwin et al., 2005; Bagby et al., 2012; Suarez et al., 2014a; Postorino et al., 2015; Thullen and Bonsall, 2017), parents have themselves identified their child's diet as a priority area for support (Galpin et al., 2017). The aim of the current study was, therefore, to examine the impact of a sensory based intervention to address food selectivity in autistic pupils that could be delivered in a school setting by teaching staff. A secondary aim of the study was to also address the research to practice gap in autism (Dingfelder and Mandell, 2011; Carrington et al., 2016).
Methods
The study had a repeated-measures within-subject design. Each child served as his or her own control, with pre- and post- measures for mealtime behavior and variety of food eaten providing the outcome measures. Although the intervention became embedded in practice and was therefore ongoing, outcome measures were taken after 12 weeks.
Participants
Whilst the intervention was offered to all pupils, three whole classes (a total of 23 children) from the same government funded, special school in inner-city London were initially selected for inclusion in the study following teacher, parent, and therapist assessment of need for a selective eating intervention. Four children were not included in the final analysis as they had been absent for more than 25% (n = 15) of the sessions. A total 19 children (3 girls and 16 boys) who ranged in age from 4 years 10 months to 10 years 7 months (M = 6 years; 5 months; SD = 1;7) took part in the sessions during the 12-week intervention period.
All children had received an independent clinical diagnosis of an autism spectrum condition according to ICD-10 (World Health Organization, 1992) or DSM-IV-TR (Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision) (American Psychiatric Association, 2000). All children met Kasari et al. (2013) definition of minimally verbal, i.e., they may use no language, or may have a very small repertoire of single words and fixed phrases that are used at low rates and in limited contexts. Additionally, all of the children had communication difficulties, and a high proportion presented with behavior that challenges and complex needs including additional learning difficulties. To attend the school, pupils need to have a Statement of Special Educational Need (SEN) or, more recently, an Education, Health and Care Plan (UK Department for Education, 2014) which is a legal document that details the child's needs and services that the local educational authority has a duty to provide. All children had been identified by the school speech and language therapist as having the requisite oral-motor skills to eat table food and had no physical complications, such as dysphagia.
The study was conducted with approval from The Bridge London Trust Research Ethics Committee and conformed to the British Psychological Society's (BPS) Code of Human Research Ethics (British Psychological Society, 2010) and the British Educational Research Association's (BERA) Ethical Guidelines for Educational Research (British Educational Research Association, 2011). All pupils taking part in Sensory Snack Time were informed that they would be having a new type of snack time. All pupils were free to withdraw from snack time by removing themselves to the “quiet space” in their classroom or leaving the classroom altogether (in line with everyday practice in which pupils may withdraw from activities that cause them distress). Parents and/or carers provided informed, written consent for their child to take part and were further informed of the fact that they were able to withdraw their children and/or their data from the snack time sessions and/or analysis at any time. All pupils' data was coded upon entry to remove any information that could link it back to an individual.
Procedure
A sensory based selective eating intervention “Sensory Snack Time” was designed to be used as a whole class approach in a school for children with autism and/or severe learning difficulty. In order to ensure high fidelity of implementation of the sessions participating staff attended a short training session to explain the programme and the principles of a sensory based approach to feeding (Greenberg et al., 2004). Additionally, the school dietitian (CP) attended the first session and either led that session or supported the class teacher to lead the session. The dietitian then attended at least 30% of subsequent class sessions to provide feedback and ensure the approach was being used correctly.
Staff Training
The school dietitian (CP) alongside a class teacher who was also a trained speech and language therapist (LO) developed a 1 h training session based on a sensory approach to addressing restrictive eating with the aim of enabling class teams to introduce Sensory Snack Time as a whole class approach. Relevant class teams of Teachers and Special Needs Professionals (support staff - SNPs) attended the training prior to beginning the 12-week block of intervention in their classes.
During the training, the complexity of feeding was described to demonstrate how feeding competency is influenced by the successful involvement of all organ systems, muscles, and sensory systems, an individual's capacity to learn (including the impact of different ways of thinking associated with autism), their developmental age, nutritional status, and environmental influences. This was explained to provide a platform to discuss and challenge common myths about feeding. Operant conditioning and physiological responses to stress were also explained within a feeding context.
The Sensory Snack Time approach was briefly discussed in relation to its basis in child-led systematic desensitization through the sequential presentation of foods. The steps to eating were discussed in order to reinforce the complexity of feeding and the number of steps required for an individual to eat a specific food. The hierarchy of six steps to eating (visual tolerance, interaction—without touching, smell, touch, taste, and eating), used in SOS feeding interventions (Toomey and Ross, 2011) further broken down into 32 sub-steps, as described in the M-SOS intervention (Peterson et al., 2016), was also used to guide teachers and SNPs in grading the children's interactions with foods during intervention meal times. This was based on the child's individual responses and needs. The subsequent creation of individualized food hierarchies by considering the sensory qualities of each food were discussed and examples were given. The importance of considering food allergies, dietary requirements and dysphagia was highlighted and staff were advised to discuss any concerns with the relevant school health professionals to ensure the safe delivery of the approach.
Clips of a sensory feeding approach previously implemented by the dietitian were shared with staff, showing the different stages of group and 1:1 feeding therapy with neurotypically developing children and children with autism and/or severe learning difficulties. The videos showed examples of table based sensory preparation such as hand washing, cleaning tables, and bubble blowing. They also showed the process of presenting and interacting with each food according to children's individual level of comfort with that food. It further highlighted strategies such as having a “spit out” bowl to encourage interaction with food without the demand of eating it. The clips showed food aversive behaviors in autistic children which were discussed in relation to the hierarchy of steps to eating.
Finally, a lesson plan provided an outline of how the approach would be used in the classroom (see Appendix A) and individual teachers met with the dietitian and speech and language therapist to construct food hierarchies specific to the children in their classes. The number of foods in the hierarchy varied between 4–8 depending on the needs and tolerance of the children in the class.
Class Based Intervention
Prior to the start of the intervention a consistent snack time routine was established and embedded into the class routine. Prior to the Sensory Snack Time sessions children took part in sensory preparation games and activities that supported sensory integration and readiness to learn. The types of games and activities put in place were based on professional judgement to ensure they met the needs of the specific pupils (Twachtman-Reilly et al., 2008). Children were motivated to sit at the table independently with bubble play and hand held paper windmills which led into hand washing and oro-motor awareness activities to provide further sensory preparation. Interactions throughout the session were child-led.
A range of 52 different foods, three liquids and five sauces categorized based upon their texture and food group was made available to pupils during the 12 weeks of Sensory Snack Time sessions (see Appendix B for examples of foods offered), with 4–8 foods available during each session. Systematic desensitization through sequential food hierarchies determined what food was presented and in which order. The food hierarchies maintained the nutritional requirements and sensory qualities of each food and always started and finished with preferred foods. Food was presented one-by-one in clear plastic bags to reduce branding bias (Whiteley et al., 2000). Distractions were managed by minimizing the use of packaging and equipment such as plates. The session leader (Teacher or SNP) determined when to introduce the next food through observations of children's responses. On average, the same food hierarchy was used for 2 consecutive weeks before changes were made to move children up the hierarchy.
The child-led, therapeutic approach ensured that there was no expectation on the child to interact with the food. Supporting adults modeled playful and exploratory interactions with the food based on individual children's needs in order to create a comfortable and relaxed environment (Ernsperger and Stegen-Hanson, 2004). Knowledge of appropriate interactions was based on the six steps to eating hierarchy described in the SOS approach (Toomey and Ross, 2011). For example, passing the bag along without opening it (interaction), opening the bag, taking foods out of the bag or playing with foods at table-top level (touch). Adults also modeled strategies of managing non-preferred food items, for example by having a tissue to wipe it up and a tray to place food on when it was finished. A drink completed the snack time routine providing a clear cue to finish the activity.
Measures
Brief Autism Mealtime Behavior Inventory (BAMBI)
The BAMBI is a standardized assessment tool designed to measure mealtime behavior problems of autistic children. It consists of an 18-item caregiver-report questionnaire using a 5-point Likert scale (ranging from 1 = never/rarely to 5 = at almost every meal) (Lukens and Linscheid, 2008). Items include “My child cries or screams during mealtimes,” “My child is willing to try new foods,” and “My child is flexible about mealtime routines.” Test–retest reliability is reported at 78 and interrater reliability at 78 (Lukens and Linscheid, 2008). A total frequency score is calculated with higher scores reflecting more problematic mealtime behaviors. Those completing the BAMBI are also asked to rate each item as a “Yes” if they think the item is a specific problem for their child or “No” if they think it is not a problem. More severe mealtime behavior difficulties are indicated by a greater number of “Yes” responses. Initial factor analysis by Lukens and Linscheid supported three sub-scale scores: eight items related to limited variety; five items related to food refusal; and five items related to features of autism, such as short attention span, aggressive and self-injurious behavior, rigid and repetitive behavior, and abnormal response to sensory input (Lukens and Linscheid, 2008). However, in a larger, more recent study, confirmatory factor analysis carried out by DeMand and colleagues failed to support the three factor structure (DeMand et al., 2015). Furthermore, three items were recommended for removal from the questionnaire. The resultant exploratory factor analysis supported a four factor structure: Food Selectivity (4 items, α = 0.87; e.g., “Is willing to try new foods”), Disruptive Mealtime Behaviors (5 items, α = 0.70; e.g., “Is disruptive during mealtimes”), Food Refusal (3 items, α = 0.54; e.g., “Turns his/her face or body away from food”), and Mealtime Rigidity (3 items α = 0.60; e.g., “Prefers to have food served in a particular way”) (DeMand et al., 2015). The revised scale's overall internal consistency was good for the full scale (i.e., all 15 items) with Cronbach's alpha of 835. The 15 item BAMBI supported by DeMand et al. (2015) was used in the current study and means across items for each subscale were calculated. To improve the clinical value of the BAMBI DeMand et al. (2015) also identified a cut-off score of 34 for the qualification of problematic feeders based on the Total Score in the 15 item BAMBI.
Although the BAMBI was originally developed as a parent-report questionnaire, the items were all applicable to teacher-report of school mealtime behavior. The brevity of the measure, good reliability, the Food Selectivity subscale, and the ability for it to be completed by non-clinical professionals made it particularly relevant for the current study.
Food Variety
Few studies that have sought to address food selectivity have reported on the implicit primary goal of increased food variety, instead volume of food intake has been reported (Marshall et al., 2014). This may be due to a lack of standardized instruments for capturing increased food variety, with a lack of “gold standard” measures (Cermak et al., 2010). One of the desired outcomes of the current study was for pupils to become intrinsically motivated to try new foods, food variety was, therefore, quantified through the difference between the number of food items (from those made available during the intervention) that pupils independently selected and ate before and after the intervention. A total of 52 different foods, three liquids and five sauces were made available over the course of the intervention (henceforth simply referred to as foods). Table 1 shows the breakdown of the foods by food group and texture. Prior to the start of the intervention the foods were made available during snack time over the course of 1 week. The number of foods that each child selected and ate, without prompting, was recorded by the class staff. As well as individual totals the overall mean for the group was calculated so as to provide a baseline measure of number of foods selected.
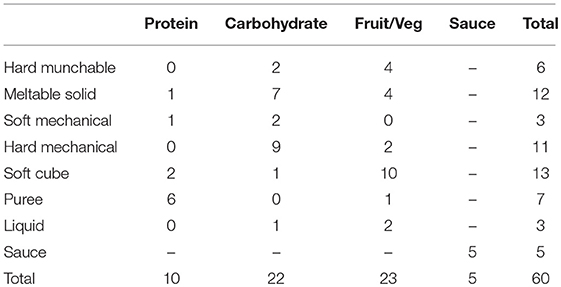
Table 1. Foods available during the intervention by food group and texture.
Results
BAMBI
The baseline and post intervention overall scores and sub-scale scores for the BAMBI were calculated and are displayed in Table 2. In addition, the severity score of problem behaviors was also calculated, “Yes” responses were coded as 1 and “No” responses coded as 0 so as to provide a quantitative value for severity (severity score).

Table 2. BAMBI scores for baseline and post intervention*.
Comparisons of the baseline and post intervention scores on the BAMBI were made. For the Total, Food Selectivity and Food Refusal scores paired samples t-test were conducted. These comparisons indicated that the Total BAMBI scores of the participants were significantly lower post-intervention (M = 31.00, SD = 9.37) than at baseline (M = 38.53, SD = 12.49), t(18) = 4.66, p < 0.001, d = 1.07. Similarly, the Food Selectivity score was significantly lower post-intervention (M = 11.37, SD = 4.31) than at baseline (M = 14.00, SD = 4.67), t(18) = 5.06, p < 0.001, d = 1.16. Food Refusal scores were also significantly lower on average post-intervention (M = 5.53, SD = 2.04) than at baseline (M = 7.26, SD = 2.85), t(18) = 3.18, p = 0.005, d = 0.73.
As the data for the Severity Score, Disruptive Mealtime Behaviour and Mealtime Rigidity scores were not normally distributed (Shapiro-Wilk = p < 0.05) Wilcoxon Signed-rank tests were conducted. The tests indicated that Severity scores were significantly lower post-intervention (Mdn = 1, range: 0–6) than at baseline (Mdn = 5, range: 0–15), Z = −3.00, p < 0.001, r = -0.49. Disruptive Mealtime Behaviour scores were also significantly lower post-intervention (Mdn = 7, range: 5–14) than at baseline (Mdn = 10, range: 5–21), Z = -2.46, p < 0.05, r = −0.4. The difference between the baseline and post-intervention scores for Mealtime Rigidity were not shown to be significant (Z = −1.51, p = 0.13).
DeMand et al. (2015) identified a cut-score of 34 to identify problematic feeders. The mean score of the pupils was above this threshold at baseline (M = 38.53, SD = 12.49) and under it post-intervention (M = 31.00, SD = 9.37). Of the 19 participants, 14 had scores of 34 or above at baseline compared to 7 post-intervention.
Food Selectivity
The mean number of foods eaten across all participants at baseline and post-intervention across all 17 categories (by food group and texture) are displayed below in Table 3. The mean number of items eaten increased across all food categories, except for Carbohydrate Soft Cube which remained the same, following the intervention. A mixed design repeated measures ANOVA with food category (17 items) as the with-in subjects variable and time (baseline or post-intervention) as the between subjects factor was carried out to examine the significance of the difference between the baseline and post-intervention mean number of items eaten. Mauchly's test indicated that the assumption of sphericity had been violated ( = 1521.78, p < 0.001), therefore degrees of freedom were corrected using Greenhouse-Geisser estimates of sphericity (ε = 0.07). The results show that there was a significant interaction effect between food category and time F(1.24, 44.67) = 10.42, p < 0.001, = 0.22, observed power = 0.93. Post-hoc tests using the Bonferroni correction indicated that the baseline and post-intervention mean number of foods eaten were significantly different (p < 0.05) in seven specific categories (see Table 3) as well as the overall mean across all the categories.
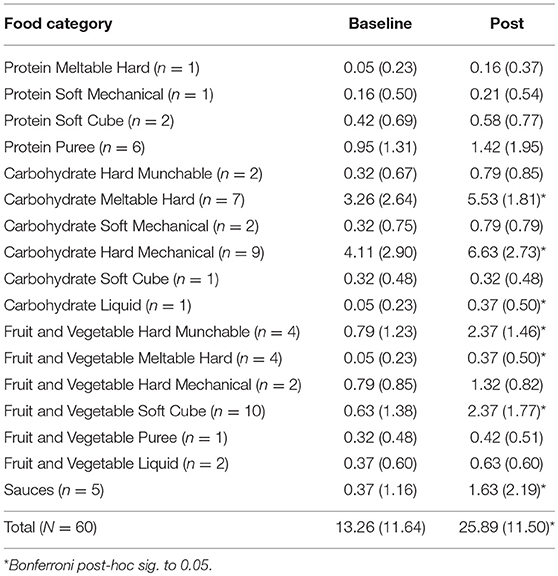
Table 3. Mean (SD) number of foods tried by pupils at Baseline and Post intervention across food categories.
The range of food categories that were tried was also examined. 17 of the 19 participants tried at least one new category of food with the other two participants having tried each category at Baseline and Post-test. There was a statistically significant difference between the mean number of categories of food tried at Baseline (M = 5.53, SD = 3.64) and Post intervention (M = 9.26, SD = 3.48) as determined by one-way ANOVA [F(1, 36) = 10.46, p = 0.003, η2 = 0.23). Participants' data was then coded as either having eaten or not eaten at least one item from a category in order to then examine the specific relationship between baseline and post-intervention amount of categories tried, these results are displayed in Table 4. Chi-square test was then performed on the baseline and post-intervention data for each category. A significant relationship was found for eight of the categories (indicated with an asterisk in Table 4), participants were significantly more likely, following the intervention, to eat an item from: Carbohydrate Hard Munchable [ = 4.07, p = 0.04, ϕ = 0.38]; Carbohydrate Hard Meltable [ = 4.77, p = 0.03, ϕ = 0.34]; Carbohydrate Soft Mechanical [ = 7.24, p = 0.007, ϕ = 0.44]; Carbohydrate Liquid [ = 5.7, p = 0.02, ϕ = 0.39]; Fruit and Vegetable Hard Munchable [ = 8.92, p = 0.003, ϕ = 0.49]; Fruit and Vegetable Hard Meltable [ = 5.7, p = 0.02, ϕ = 0.39]; Fruit and Vegetable Soft Cube [ = 8.92, p = 0.003, ϕ = 0.49]; and Sauces [ = 4.39, p = 0.04, ϕ = 0.34].
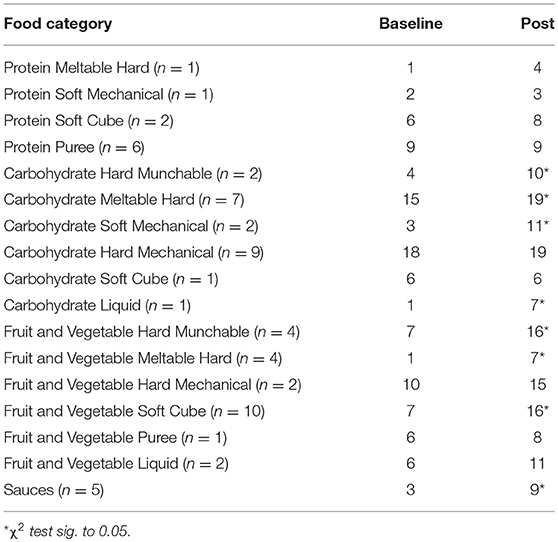
Table 4. Number of participants (N = 19) who ate at least one item in a category of food at baseline and post intervention.
Discussion
This study sought to address food selectivity in autistic children through a sensory based intervention delivered in school by existing school staff. The study is unique in that it sought to translate previously clinically based types of sensory feeding interventions into a viable part of the daily school routine (examining the effectiveness of the intervention) that would address a difficulty that had been identified as a priority area for support by parents (Galpin et al., 2017). A further contribution to the wider literature is, therefore, to respond to the call for autism research to address issues identified as priorities by the autism community (Pellicano et al., 2014). The Sensory Snack Time intervention aimed to increase the range of foods that children voluntarily chose to eat during snack time at school as well as decrease any stress experienced by children at this time. The results indicate that, on average, the sensory snack time intervention led to pupils eating a wider variety of foods during snack times. There was also a significant decrease across five of the six scores produced by the BAMBI with mealtime rigidity the only area in which there was not a significant improvement.
Following the sensory snack time intervention fewer children reached the cut-off score indicating problematic feeding (DeMand et al., 2015). Disruptive Mealtime Behaviours and Food Refusal scores had also significantly reduced. In light of the impact that difficulties in these areas can have upon family life, notably parenting stress (Kerwin et al., 2005; Bagby et al., 2012; Suarez et al., 2014a; Postorino et al., 2015; Thullen and Bonsall, 2017) these results are particularly encouraging. Parents of autistic children have identified diet and eating as a priority area for support for them and their children (Galpin et al., 2017). Whilst selective eating interventions that are carried out in clinical settings or small groups may result in improvements for certain individuals, a school-based intervention that can be carried out by existing staff members has the benefit of being available to all pupils who attend the school. There is no additional cost for parents and the costs for the school are minimal, with a larger variety of food at snack time and time for staff training and for staff to be able to plan sessions being the primary resource costs.
The increase in the variety of foods eaten, reflected not only in the selective eating subscale scores of the BAMBI, but more explicitly in the lists of foods tried further demonstrates the promise of the Sensory Snack Time intervention for addressing food selectivity. The increase in items tried from the Fruit and Vegetable food group, in light of health concerns around children with autism eating only a limited repertoire of foods (Herndon et al., 2009; Bandini et al., 2010; Bicer and Alsaffar, 2013) with calls for interventions to specifically examine this food group (Bandini et al., 2017), is also encouraging. Anecdotal feedback from school staff as well as informal observations of Sensory Snack Time also suggested that the pupils enjoyed the sessions. The decrease in the Disruptive Mealtime Behaviour scores on the BAMBI may further reflect this. Staff feedback also highlighted that the sessions were easy to implement. It should be noted that, being a special school setting snack times were highly structured prior to the intervention and, therefore, carrying out the Sensory Snack Time sessions would have required little additional work. The need for a high level of consistency and structure in the use of the approach could potentially be an obstacle to implementation in less specialist school settings. Similarly, further research is need to examine whether the level of structure and consistency required may make Sensory Snack Time difficult for parents to implement at home. Pupil enjoyment and the ease of implementation for staff indicate that a daily snack time group (whole class) intervention is feasible within a special school setting. Practitioners and parents may therefore wish to consider using a child-led sensory-based approach to help address food selectivity.
Limitations
Whilst the results of the study add to the nascent literature on sensory based interventions for selective eating (Benson et al., 2013; Aswathy et al., 2016), this research is not without its limitations. Whilst there was an increase in the variety of foods eaten, the extent to which this was as a result of the intervention and the systematic desensitization specifically offered by the intervention is unclear. With regards the intervention in general the study lacked a baseline control period that would have allowed for the evaluation of how food selectivity and mealtime behavior may change naturally (without the Sensory Snack Time intervention) across the 12-week intervention period. In terms of the systematic desensitization pupils may have been averse to certain foods at baseline simply because they were unfamiliar as opposed to any specific sensory quality of the food. Indeed, there was no significant reduction in Mealtime Rigidity (as measured on the BAMBI) suggesting pupils had a rigid understanding of snack times and what foods were offered and the presentation of novel food items may have violated this and were, therefore, initially avoided. The fact that there was not a significant increase across all of the novel food items presented does, nevertheless, suggest that qualities other than novelty were motivating resistance to try certain foods. In order to better understand the increase in variety of foods eaten a more specific sensory profile of each pupil should be carried out. Cross checking an individual sensory profile with foods eaten would provide a clearer indication of specific sensory differences that may be underlying limited food variety and further clarify the extent to which the systematic desensitization of the sensory snack time intervention had an impact on increasing food variety. Recent research examining mealtime behaviors has found a significant relationship between sensory profiles and behavior difficulties (Shmaya et al., 2017), future studies should consider an explicit measure of sensory differences in relation to selective eating so as to provide further support for the efficacy of the intervention.
School staff were involved in the collection of all of the data. This was partly due to the need to integrate the intervention into everyday school practice whereby staff collect data on pupils throughout the day. However, this resulted in some of the raters (school staff) completing both the BAMBI measure and coding the foods eaten. This reflects a wider limitation regarding testing effects and potential experimenter bias. Limited staff capacity rendered it difficult to take a measure of inter-observer agreement that future research, with greater staff resources, could look to include.
The sample size was relatively small and addressed a heterogeneous group of pupils that makes generalizing the results to a wider population difficult. The heterogeneity of the sample and indeed the population for whom the intervention may benefit contributes to the methodological limitation of a lack of control group. There are significant difficulties in being able to match sample groups in this population due to the wide range of needs pupils can have as such an imbalance between groups in baseline variables. A lack of meaningful standardized assessment measures that may allow for intervention and control groups to be matched on baseline variables further impacts the potential validity of comparable control groups. However, the results do suggest that the intervention can have a positive impact on a wide range of autistic pupils with a large degree of variability in terms of their intellectual and linguistic strengths and needs and therefore applicable and potentially beneficial to whole class groups within a special school setting.
Future Directions
The measure used to assess mealtime difficulties, the BAMBI, was chosen do to the ease of administration and for the specific sub scores that it gave which were pertinent to the current study, notably, Selective Eating scores. Whilst confirmatory factor analysis failed to support the original three factor structure of the BAMBI (DeMand et al., 2015) it has nevertheless continued to be used in its original 18 item form (Thullen and Bonsall, 2017). It has also been adapted to be used with a wider population of children (Hendy et al., 2013). The lack of consistency in the literature over the use of the measure may add to the difficulties in building up a robust body of work around support for mealtime difficulties for autistic children. Furthermore, the measure validated by DeMand and colleagues (DeMand et al., 2015) removed two questions that explicitly examined sensory aspects of foods (textures and tastes). In their analysis they note that perhaps there were insufficient items in the measure that related to sensory issues related to feeding and that should more be included it may result in another factor in the BAMBI (DeMand et al., 2015). Further development of the BAMBI may therefore be required in order for it to become a more effective measure for research in this area. It is important to note that caveats regarding the BAMBI reflects a wider problem with measures used in research with autistic individuals, particularly those with higher needs (Tager-Flusberg et al., 2017).
Whilst the Sensory Snack Time intervention demonstrated a significant increase in the range of foods eaten at snack times, the generalizing of this increase in variety of foods to main meals and other settings, particularly home, was not examined in the current study. Future research should look to examine the impact a sensory based feeding intervention has upon main meals and how any improvement in range of foods eaten generalizes to multiple settings. The Sensory Snack Time protocol reported here is currently being adapted and individualized in order to be delivered by parents in their home settings.
Conclusion
The current study demonstrated that a sensory based feeding intervention can be successfully implemented within a special school setting by existing school staff for relatively minimal costs. The Sensory Snack Time intervention was associated with a significant improvement in terms of food selectivity, with pupils choosing to eat a wider variety of foods. A more explicit examination of the specific sensory needs of each pupil taking part should be undertaken in all future applications of the intervention in order to better understand the impact the intervention is having on sensory based food refusal. Taking this into account the approach is now being extended to examine its ability to impact in home settings and main mealtimes at school, specifically lunchtimes.
Author Contributions
JG, LO, and CP designed the study. JG reviewed literature, analyzed the data, and drafted the majority of the paper. LO and CP collected the data and drafted the Methods section of the paper and provided discussion, and reviews/edits. All authors have reviewed and approved the complete manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/feduc.2018.00077/full#supplementary-material
Footnotes
1. ^In this article, we use identity-first as well as person-first language to respect the wishes of all individuals on the spectrum (Kenny et al., 2016).
References
Ahearn, W. H. (2002). Effect of two methods of introducing foods during feeding treatment on acceptance of previously rejected items. Behav. Interv. 17, 111–127. doi: 10.1002/bin.112
American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental Disorders, 4th Edn. Washington, DC: American Psychiatric.
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edn. Arlington, VA: American Psychiatric Publishing.
Aswathy, A. K., Manoharan, A., and Manoharan, A. (2016). Addressing oral sensory issues and possible remediation in children with autism spectrum disorders: illustrated with a case study. World Acad. Sci. Eng. Technol. Int. J. Med. HealthBiomed. Bioeng. Pharm. Eng. 10, 374–377.
Bachmeyer, M. H. (2009). Treatment of selective and inadequate food intake in children. Behav. Anal. Pract. 2, 43–50. doi: 10.1007/BF03391736
Bagby, M. S., Dickie, V. A., and Baranek, G. T. (2012). How sensory experiences of children with and without autism affect family occupations. Am. J. Occup. Ther. 66, 78–86. doi: 10.5014/ajot.2012.000604
Bandini, L. G., Anderson, S. E., Curtin, C., Cermak, S., Evans, E. W., Scampini, R., et al. (2010). Food selectivity in children with autism spectrum disorders and typically developing children. J. Pediatr. 157, 259–264. doi: 10.1016/j.jpeds.2010.02.013
Bandini, L. G., Curtin, C., Phillips, S., Anderson, S. E., Maslin, M., and Must, A. (2017). Changes in food selectivity in children with autism spectrum disorder. J. Autism Dev. Disord. 47, 439–446. doi: 10.1007/s10803-016-2963-6
Baum, S. H., Stevenson, R. A., and Wallace, M. T. (2015). Behavioral, perceptual, and neural alterations in sensory and multisensory function in autism spectrum disorder. Prog. Neurobiol. 134, 140–160. doi: 10.1016/j.pneurobio.2015.09.007
Beighley, J. S., Matson, J. L., Rieske, R. D., and Adams, H. L. (2013). Food selectivity in children with and without an autism spectrum disorder: investigation of diagnosis and age. Res. Dev. Disabil. 34, 3497–3503. doi: 10.1016/j.ridd.2013.07.026
Ben-Sasson, A., Hen, L., Fluss, R., Cermak, S. A., Engel-Yeger, B., and Gal, E. (2009). A meta-analysis of sensory modulation symptoms in individuals with autism spectrum disorders. J. Autism Dev. Disord. 39, 1–11. doi: 10.1007/s10803-008-0593-3
Benson, J. D., Parke, C. S., Gannon, C., and Mu-oz, D. (2013). A retrospective analysis of the sequential oral sensory feeding approach in children with feeding difficulties. J. Occup. Ther. Sch. Early Interv. 6, 289–300. doi: 10.1080/19411243.2013.860758
Bernard-Bonnin, A. C. (2006). Feeding problems of infants and toddlers. Can. Fam. Phys. 52, 1247–1251.
Bicer, A. H., and Alsaffar, A. A. (2013). Body mass index, dietary intake and feeding problems of Turkish children with autism spectrum disorder (ASD). Res. Dev. Disabil. 34, 3978–3987. doi: 10.1016/j.ridd.2013.08.024
Boyd, K. L. (2007). The Effectiveness of the Sequential Oral Sensory Approach Group Feeding Program (Doctoral dissertation). Proquest Dissertations and Theses database.
British Educational Research Association (2011). Ethical Guidelines for Educational Research. London. Available online at: https://www.bera.ac.uk/wp-content/uploads/2014/02/BERA-Ethical-Guidelines-2011.pdf.
British Psychological Society (2010). Code of Human Research Ethics. Leicester. Available online at: http://www.bps.org.uk/sites/default/files/documents/code_of_human_research_ethics.pdf.
Carrington, S. J., Uljarevi, M., Roberts, A., White, L. J., Morgan, L., Wimpory, D., et al. (2016). Knowledge acquisition and research evidence in autism: researcher and practitioner perspectives and engagement. Res. Dev. Disabil. 51, 126–134. doi: 10.1016/j.ridd.2016.01.011
Cermak, S., Curtin, C., and Bandini, L. (2010). “Sensory sensitivity and food selectivity in children with autism spectrum disorders,” in Comprehensive Guide to Autism, eds V. B. Patel, V. R. Preedy and C. R. Martin (New York, NY: Springer), 2061–2076.
Chistol, L. T., Bandini, L. G., Must, A., Phillips, S., Cermak, S. A., and Curtin, C. (2018). Sensory sensitivity and food selectivity in children with autism spectrum disorder. J. Autism Dev. Disord. 48, 583–591. doi: 10.1007/s10803-017-3340-9
Cornish, E. (2002). Gluten and casein free diets in autism: a study of the effects on food choice and nutrition. J. Hum. Nutr. Diet. 15, 261–269. doi: 10.1046/j.1365-277X.2002.00372.x
Coulthard, H., Harris, G., and Fogel, A. (2016). Association between tactile over-responsivity and vegetable consumption early in the introduction of solid foods and its variation with age. Matern. Child Nutr. 12, 848–859. doi: 10.1111/mcn.12228
Curtin, C., Hubbard, K., Anderson, S. E., Mick, E., Must, A., and Bandini, L. G. (2015). Food selectivity, mealtime behavior problems, spousal stress, and family food choices in children with and without autism spectrum disorder. J. Autism Dev. Disord. 45:3308–3315. doi: 10.1007/s10803-015-2490-x
DeMand, A., Johnson, C., and Foldes, E. (2015). Psychometric properties of the brief autism mealtime behaviors inventory. J. Autism Dev. Disord. 45, 2667–2673. doi: 10.1007/s10803-015-2435-4
Dingfelder, H. E., and Mandell, D. S. (2011). Bridging the research-to-practice gap in autism intervention: an application of diffusion of innovation theory. J. Autism Dev. Disord. 41, 597–609. doi: 10.1007/s10803-010-1081-0
Engel-Yeger, B., Hardal-Nasser, R., and Gal, E. (2016). The relationship between sensory processing disorders and eating problems among children with intellectual developmental deficits. Br. J. Occup. Ther. 79, 17–25. doi: 10.1177/0308022615586418
Ernsperger, L., and Stegen-Hanson, T. (2004). Just Take a Bite: Easy, Effective Answers to Food Aversions and Eating Challenges. Arlington, TX: Future Horizons.
Farrow, C. V., and Coulthard, H. (2012). Relationships between sensory sensitivity, anxiety and selective eating in children. Appetite 58, 842–846. doi: 10.1016/j.appet.2012.01.017
Fertel-Daly, D., Bedell, G., and Hinojosa, J. (2001). Effects of a weighted vest on attention to task and self-stimulatory behaviors in preschoolers with pervasive developmental disorders. Am. J. Occup. Ther. 55, 629–640. doi: 10.5014/ajot.55.6.629
Field, D., Garland, M., and Williams, K. (2003). Correlates of specific childhood feeding problems. J. Paediatr. Child Health 39, 299–304. doi: 10.1046/j.1440-1754.2003.00151.x
Field, T., Lasko, D., Mundy, P., Henteleff, T., Kabat, S., Talpins, S., et al. (1997). Brief report: autistic children's attentiveness and responsivity improve after touch therapy. J. Autism Dev. Disord. 27, 333–338. doi: 10.1023/A:1025858600220
Fodstad, J. C., and Matson, J. L. (2008). A comparison of feeding and mealtime problems in adults with intellectual disabilities with and without autism. J. Dev. Phys. Disabil. 20, 541–550. doi: 10.1007/s10882-008-9116-6
Gale, C. M., Eikeseth, S., and Rudrud, E. (2011). Functional assessment and behavioural intervention for eating difficulties in children with autism: a study conducted in the natural environment using parents and ABA tutors as therapists. J. Autism Dev. Disord. 41, 1383–1396. doi: 10.1007/s10803-010-1167-8
Galpin, J., Barratt, P., Ashcroft, E., Greathead, S., Kenny, L., and Pellicano, E. (2017). 'The dots just don't join up': understanding the support needs of families of children on the autism spectrum. Autism 22, 571–584. doi: 10.1177/1362361316687989
Grandin, T (1992). “An inside out view of autism,” in High Functioning Individuals With Autism, eds E. Schopler and G. B. Mesibov (New York, NY: Plenum Press), 105–126.
Greenberg, M. T., Domitrovich, C. E., Graczyk, P. A., and Zins, J. E. (2004). The Study of Implementation in School-Based Preventative Interventions: Theory, Research, and Practice. Final Project Report. Washington, DC: Department of Human Health and Services, Substance Abuse and Mental Health Services Administration, Centre for Mental Health Services.
Greer, A. J., Gulotta, C. S., Masler, E. A., and Laud, R. B. (2008). Caregiver stress and outcomes of children with pediatric feeding disorders treated in an intensive interdisciplinary program. J. Pediatr. Psychol. 33, 612–620. doi: 10.1093/jpepsy/jsm116
Guldberg, K. (2017). Evidence-based practice in autism educational research: can we bridge the research and practice gap? Oxford Rev. Educ. 43, 149–161. doi: 10.1080/03054985.2016.1248818
Hendy, H. M., Seiverling, L., Lukens, C. T., and Williams, K. E. (2013). Brief assessment of mealtime behavior in children: psychometrics and association with child characteristics and parent responses. Child. Health Care 42, 1–14. doi: 10.1080/02739615.2013.753799
Herndon, A. C., DiGuiseppi, C., Johnson, S. L., Leiferman, J., and Reynolds, A. (2009). Does nutritional intake differ between children with autism spectrum disorders and children with typical development? J. Autism Dev. Disord. 39, 212–222. doi: 10.1007/s10803-008-0606-2
Hubbard, K. L., Anderson, S. E., Curtin, C., Must, A., and Bandini, L. G. (2014). A comparison of food refusal related to characteristics of food in children with autism spectrum disorder and typically developing children. J. Acad. Nutr. Diet. 114, 1981–1987. doi: 10.1016/j.jand.2014.04.017
Johnson, C. R., Turner, K., Stewart, P. A., Schmidt, B., Shui, A., Macklin, E., et al. (2014). Relationships between feeding problems, behavioral characteristics and nutritional quality in children with ASD. J. Autism Dev. Disord. 44, 2175–2184. doi: 10.1007/s10803-014-2095-9
Johnson, S. L., Davies, P. L., Boles, R. E., Gavin, W. J., and Bellows, L. L. (2015). Young children's food neophobia characteristics and sensory behaviors are related to their food intake. J. Nutr. 145, 2610–2616. doi: 10.3945/jn.115.217299
Jones, R. S., Quigney, C., and Huws, J. C. (2003). First-hand accounts of sensory perceptual experiences in autism: a qualitative analysis. J. Intellect. Dev. Disabil. 28, 112–121. doi: 10.1080/1366825031000147058
Kasari, C., Brady, N., Lord, C., and Tager-Flusberg, H. (2013). Assessing the minimally verbal school-aged child with autism spectrum disorder. Autism Res. 6, 479–493. doi: 10.1002/aur.1334
Keen, D. V. (2008). Childhood autism, feeding problems and failure to thrive in early infancy: seven case studies. Eur. Child Adolesc. Psychiatry 17, 209–216. doi: 10.1007/s00787-007-0655-7
Kenny, L., Hattersley, C., Molins, B., Buckley, C., Povey, C., and Pellicano, E. (2016). Which terms should be used to describe autism? Perspectives from the UK autism community. Autism 20, 442–462. doi: 10.1177/1362361315588200
Kerwin, M. E., Eicher, P. S., and Gelsinger, J. (2005). Parental report of eating problems and gastrointestinal symptoms in children with pervasive developmental disorders. Child. Health Care 34, 217–234. doi: 10.1207/s15326888chc3403_4
Koenig, K. P., and Rudney, S. G. (2010). Performance challenges for children and adolescents with difficulty processing and integrating sensory information: a systematic review. Am. J. Occup. Ther. 64, 430–442. doi: 10.5014/ajot.2010.09073
Kral, T. V., Eriksen, W. T., Souders, M. C., and Pinto-Martin, J. A. (2013). Eating behaviors, diet quality, and gastrointestinal symptoms in children with autism spectrum disorders: a brief review. J. Pediatr. Nurs. 28, 548–556. doi: 10.1016/j.pedn.2013.01.008
Kuschner, E. S., Eisenberg, I. W., Orionzi, B., Simmons, W. K., Kenworthy, L., Martin, A., et al. (2015). A preliminary study of self-reported food selectivity in adolescents and young adults with autism spectrum disorder. Res. Autism Spectr. Disord. 15, 53–59. doi: 10.1016/j.rasd.2015.04.005
Laud, R. B., Girolami, P. A., Boscoe, J. H., and Gulotta, C. S. (2009). Treatment outcomes for severe feeding problems in children with autism spectrum disorder. Behav. Modif. 33, 520–536. doi: 10.1177/0145445509346729
Ledford, J. R., and Gast, D. L. (2006). Feeding problems in children with autism spectrum disorders: a review. Focus Autism Other Dev. Disabl. 21, 153–166. doi: 10.1177/10883576060210030401
Ledford, J. R., Whiteside, E., and Severini, K. E. (2018). A systematic review of interventions for feeding-related behaviors for individuals with autism spectrum disorders. Res. Autism Spectr. Disord. 52, 69–80. doi: 10.1016/j.rasd.2018.04.008
Leekam, S. R., Nieto, C., Libby, S. J., Wing, L., and Gould, J. (2007). Describing the sensory abnormalities of children and adults with autism. J. Autism Dev. Disord. 37, 894–910. doi: 10.1007/s10803-006-0218-7
Lindberg, L., Bohlin, G., and Hagekull, B. (1991). Early feeding problems in a normal population. Int. J. Eat. Disord. 10, 395–405. doi: 10.1002/1098-108X(199107)10:4<395::AID-EAT2260100404>3.0.CO;2-A
Luisier, A. C., Petitpierre, G., Ferdenzi, C., Clerc Bérod, A., Giboreau, A., Rouby, C., et al. (2015). Odor perception in children with autism spectrum disorder and its relationship to food neophobia. Front. Psychol. 6:1830. doi: 10.3389/fpsyg.2015.01830
Lukens, C. T., and Linscheid, T. R. (2008). Development and validation of an inventory to assess mealtime behavior problems in children with autism. J. Autism Dev. Disord. 38, 342–352. doi: 10.1007/s10803-007-0401-5
Manikam, R. (2000). Current literature: pediatric feeding disorders. Nutr. Clin. Pract. 15, 312–314. doi: 10.1177/088453360001500608
Marí-Bauset, S., Zazpe, I., Mari-Sanchis, A., Llopis-González, A., and Morales-Suárez-Varela, M. (2014). Evidence of the gluten-free and casein-free diet in autism spectrum disorders a systematic review. J. Child Neurol. 29, 1718–1727. doi: 10.1177/0883073814531330
Marshall, J., Hill, R. J., Ziviani, J., and Dodrill, P. (2014). Features of feeding difficulty in children with Autism Spectrum Disorder. Int. J. Speech Lang. Pathol. 16, 151–158. doi: 10.3109/17549507.2013.808700
Martins, Y., Young, R. L., and Robson, D. C. (2008). Feeding and eating behaviors in children with autism and typically developing children. J. Autism Dev. Disord. 38, 1878–1887. doi: 10.1007/s10803-008-0583-5
Mascola, A. J., Bryson, S. W., and Agras, W. S. (2010). Picky eating during childhood: a longitudinal study to age 11 years. Eat. Behav. 11, 253–257. doi: 10.1016/j.eatbeh.2010.05.006
Matson, J. L., and Fodstad, J. C. (2009). The treatment of food selectivity and other feeding problems in children with autism spectrum disorders. Res. Autism Spectr. Disord. 3, 455–461. doi: 10.1016/j.rasd.2008.09.005
Mattingly, R., Mukkada, V., Smith, A., and Pitts, T. (2015). Optimizing an aversion feeding therapy protocol for a child with food protein-induced enterocolitis syndrome (FPIES). J. Pulm. Respir. Med. 5:287. doi: 10.4172/2161-105X.1000287
Mazurek, M. O., Vasa, R. A., Kalb, L. G., Kanne, S. M., Rosenberg, D., Keefer, A., et al. (2013). Anxiety, sensory over-responsivity, and gastrointestinal problems in children with autism spectrum disorders. J. Abnor. Child Psychol. 41, 165–176. doi: 10.1007/s10802-012-9668-x
Nadon, G., Feldman, D. E., Dunn, W., and Gisel, E. (2011a). Mealtime problems in children with autism spectrum disorder and their typically developing siblings: a comparison study. Autism 15, 98–113. doi: 10.1177/1362361309348943
Nadon, G., Feldman, D. E., Dunn, W., and Gisel, E. (2011b). Association of sensory processing and eating problems in children with autism spectrum disorders. Autism Res. Treat. 2011:541926. doi: 10.1155/2011/541926
Najdowski, A. C., Wallace, M. D., Doney, J. K., and Ghezzi, P. M. (2003). Parental assessment and treatment of food selectivity in natural settings. J. Appl. Behav. Anal. 36, 383–386. doi: 10.1901/jaba.2003.36-383
Nederkoorn, C., Theiβen, J., Tummers, M., and Roefs, A. (2018). Taste the feeling or feel the tasting: tactile exposure to food texture promotes food acceptance. Appetite 120, 297–301. doi: 10.1016/j.appet.2017.09.010
Overland, L. (2011). A sensory-motor approach to feeding. SIG 13 Perspect. Swallowing Swallowing Disord. 20, 60–64. doi: 10.1044/sasd20.3.60
Pellicano, E., Dinsmore, A., and Charman, T. (2014). What should autism research focus upon? Community views and priorities from the United Kingdom. Autism 18, 756–770. doi: 10.1177/1362361314529627
Peterson, K. M., Piazza, C. C., and Volkert, V. M. (2016). A comparison of a modified sequential oral sensory approach to an applied behavior-analytic approach in the treatment of food selectivity in children with autism spectrum disorder. J. Appl. Behav. Anal. 49, 485–511. doi: 10.1002/jaba.332
Postorino, V., Sanges, V., Giovagnoli, G., Fatta, L. M., De Peppo, L., Armando, M., et al. (2015). Clinical differences in children with autism spectrum disorder with and without food selectivity. Appetite 92, 126–132. doi: 10.1016/j.appet.2015.05.016
Provost, B., Crowe, T. K., Osbourn, P. L., McClain, C., and Skipper, B. J. (2010). Mealtime behaviors of preschool children: comparison of children with autism spectrum disorder and children with typical development. Phys. Occup. Ther. Pediatr. 30, 220–233. doi: 10.3109/01942631003757669
Rastam, M. (2008). Eating disturbances in autism spectrum disorders with focus on adolescent and adult years. Clin. Neuropsychiatry 5, 31–42
Rastam, M., and Wentz, E. (2014). “ASD, eating problems, and overlap with anorexia and bulimia nervosa,” in Comprehensive Guide to Autism, eds V. B. Patel, V. R. Preedy, and C. R. Martin (New York, NY: Springer), 2015–2034.
Reinoso, G., Carsone, B., Weldon, S., Powers, J., and Bellare, N. (2018). Food selectivity and sensitivity in children with autism spectrum disorder: a systematic review defining the issue and evaluating interventions. N. Z. J. Occup. Ther. 65, 36–42.
Schaaf, R. C., and Nightlinger, K. M. (2007). Occupational therapy using a sensory integrative approach: a case study of effectiveness. Am. J. Occup. Ther. 61, 239–246. doi: 10.5014/ajot.61.2.239
Schmitt, L., Heiss, C. J., and Campbell, E. E. (2008). A comparison of nutrient intake and eating behaviors of boys with and without autism. Top. Clin. Nutr. 23, 23–31. doi: 10.1097/01.TIN.0000312077.45953.6c
Schreck, K. A., and Williams, K. (2006). Food preferences and factors influencing food selectivity for children with autism spectrum disorders. Res. Dev. Disabil. 27, 353–363. doi: 10.1016/j.ridd.2005.03.005
Schreck, K. A., Williams, K., and Smith, A. F. (2004). A comparison of eating behaviors between children with and without autism. J. Autism Dev. Disord. 34, 433–438. doi: 10.1023/B:JADD.0000037419.78531.86
Seiverling, L., Williams, K., and Sturmey, P. (2010). Assessment of feeding problems in children with autism spectrum disorders. J. Autism Dev. Disord. 22, 401–413. doi: 10.1007/s10882-010-9206-0
Seiverling, L. J., Hendy, H. M., and Williams, K. E. (2011). Child and parent variables associated with texture problems in children's feeding. J. Dev. Phys. Disabil. 23, 303–311. doi: 10.1007/s10882-011-9229-1
Sharp, W. G., Berry, R. C., McCracken, C., Nuhu, N. N., Marvel, E., Saulnier, C. A., et al. (2013). Feeding problems and nutrient intake in children with autism spectrum disorders: a meta-analysis and comprehensive review of the literature. J. Autism Dev. Disord. 43, 2159–2173. doi: 10.1007/s10803-013-1771-5
Sharp, W. G., Jaquess, D. L., Morton, J. F., and Herzinger, C. V. (2010). Pediatric feeding disorders: a quantitative synthesis of treatment outcomes. Clin. Child Fam. Psychol. Rev. 13, 348–365. doi: 10.1007/s10567-010-0079-7
Shmaya, Y., Eilat-Adar, S., Leitner, Y., Reif, S., and Gabis, L. V. (2017). Meal time behavior difficulties but not nutritional deficiencies correlate with sensory processing in children with autism spectrum disorder. Res. Dev. Disabil. 66, 27–33. doi: 10.1016/j.ridd.2017.05.004
Silbaugh, B. C., Penrod, B., Whelan, C. M., Hernandez, D. A., Wingate, H. V., Falcomata, T. S., et al. (2016). A systematic synthesis of behavioral interventions for food selectivity of children with autism spectrum disorders. Rev. J. Autism Dev. Disord. 3, 345–357. doi: 10.1007/s40489-016-0087-8
Silbaugh, B. C., and Swinnea, S. (2018). Failure to replicate the effects of the high-probability instructional sequence on feeding in children with autism and food selectivity. Behav. Modif. doi: 10.1177/0145445518785111. [Epub ahead of print].
Silverman, A. H., Tarbell, S., Roberts, M. C., and Steele, R. G. (2009). Feeding and Vomiting Problems in Pediatric Populations. Handbook of Pediatric Psychology. New York, NY: Guilford Press, 429–445.
Smith, A. M., Roux, S., Naidoo, N. T., and Venter, D. J. (2005). Food choices of tactile defensive children. Nutrition 21, 14–19. doi: 10.1016/j.nut.2004.09.004
Suarez, M. A., Atchison, B. J., and Lagerwey, M. (2014a). Phenomenological examination of the mealtime experience for mothers of children with autism and food selectivity. Am. J. Occup. Ther. 68, 102–107. doi: 10.5014/ajot.2014.008748
Suarez, M. A., Nelson, N. W., and Curtis, A. B. (2012). Associations of physiological factors, age, and sensory over-responsivity with food selectivity in children with autism spectrum disorders. Open J. Occup. Ther. 1:22.
Suarez, M. A., Nelson, N. W., and Curtis, A. B. (2014b). Longitudinal follow-up of factors associated with food selectivity in children with autism spectrum disorders. Autism 18, 924–932. doi: 10.1177/1362361313499457
Tager-Flusberg, H., Plesa Skwerer, D., Joseph, R. M., Brukilacchio, B., Decker, J., Eggleston, B., et al. (2017). Conducting research with minimally verbal participants with autism spectrum disorder. Autism 21, 852–861. doi: 10.1177/1362361316654605
Tarbox, J., Schiff, A., and Najdowski, A. C. (2010). Parent-implemented procedural modification of escape extinction in the treatment of food selectivity in a young child with autism. Educ. Treat. Child. 33, 223–234. doi: 10.1353/etc.0.0089
Thullen, M., and Bonsall, A. (2017). Co-parenting quality, parenting stress, and feeding challenges in families with a child diagnosed with autism spectrum disorder. J. Autism Dev. Disord. 47, 878–886. doi: 10.1007/s10803-016-2988-x
Tomchek, S. D., and Dunn, W. (2007). Sensory processing in children with and without autism: a comparative study using the short sensory profile. Am. J. Occup. Ther. 61, 190–200. doi: 10.5014/ajot.61.2.190
Toomey, K. A., and Ross, E. S. (2011). SOS approach to feeding. SIG 13 Perspect. Swallowing Swallowing Disord. 20, 82–87. doi: 10.1044/sasd20.3.82
Twachtman-Reilly, J., Amaral, S. C., and Zebrowski, P. P. (2008). Addressing feeding disorders in children on the autism spectrum in school-based settings: physiological and behavioral issues. Lang. Speech Hear. Serv. Sch. 39, 261–272. doi: 10.1044/0161-1461(2008/025)
UK Department for Education (2014). Special Educational Needs and Disability Code of Practice: 0 to 25 Years. London: HMSO.
Whiteley, P., Rodgers, J., and Shattock, P. (2000). Feeding patterns in autism. Autism 4, 207–211. doi: 10.1177/1362361300004002008
Williams, P. G., Dalrymple, N., and Neal, J. (2000). Eating habits of children with autism. Pediatr. Nurs. 26, 259–264.
World Health Organization (1992). ICD-IO Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva: World Health Organisation.
Keywords: autism, food selectivity, education, participatory action research, intervention, sensory differences
Citation: Galpin J, Osman L and Paramore C (2018) Sensory Snack Time: A School-Based Intervention Addressing Food Selectivity in Autistic Children. Front. Educ. 3:77. doi: 10.3389/feduc.2018.00077
Received: 27 April 2018; Accepted: 20 August 2018;
Published: 07 September 2018.
Edited by:
Vasiliki Totsika, University of Warwick, United KingdomReviewed by:
Emily S. Kuschner, Children's Hospital of Philadelphia, United StatesKonstantinos M. Ntinas, Ministry of Education, Research and Religious Affairs, Greece
Copyright © 2018 Galpin, Osman and Paramore. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: James Galpin, james.galpin@thebridgelondon.co.uk