Case Report: Giant left atrial cystic tumor: myxoma or intracardiac blood cyst?
 Weizhang Xiao
Weizhang Xiao Jing Qin2
Jing Qin2 - 1Department of Cardiothoracic Surgery, Affiliated Hospital and Medical School of Nantong University, Nantong, China
- 2Department of Echocardiography, Affiliated Hospital and Medical School of Nantong University, Nantong, China
- 3Department of Pathology, Affiliated Hospital and Medical School of Nantong University, Nantong, China
Background: Primary cardiac tumors are uncommon, with the majority being benign myxomas. Cystic myxoma, a particularly rare type of benign cardiac tumor, demands cautious differential diagnosis from other cardiac tumors.
Case summary: A 43-year-old male patient presenting with intermittent dyspnea was referred to our department for surgical evaluation. Transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE) unveiled an intra-left atrial cyst, which was subsequently found to be blood-filled during a video-assisted microinvasive heart surgery. Pathological examination depicted a cyst wall filled with small stellate and fat spindle cells, along with a mucoid matrix, indicating a diagnosis of cystic myxoma.
Conclusions: We herein presented a rare case of an adult patient with cystic myxoma, initially misdiagnosed as an intracardiac blood cyst (CBC) prior to surgery, and ultimately verified via pathological findings.
Introduction
Primary cardiac tumors are rare, with an incidence of 0.002% to 0.3% and a prevalence of 0.001% to 0.03%. Over half of these tumors are myxomas (1). Most myxomas occur in the left atrium (75% to 80%), with fewer cases found in the right atrium (10% to 20%) (2). Typically, these tumors are solid, round, or polypoid in shape and attached to the interatrial septum, lacking a cystic structure. However, cystic myxomas are exceedingly rare (3–8). Intracardiac blood cysts are another unusual cardiac tumor, mainly seen in fetuses or infants under six months of age and rarely reported in adults. Here, we present an uncommon case of a left atrial cystic myxoma that was initially suspected as a CBC before surgery and ultimately diagnosed as a cystic myxoma.
Patient information
A 43-year-old male patient presented with intermittent dyspnea during sleep for 20 days and underwent TTE at a local hospital, which revealed a left atrial myxoma. He was referred to our hospital for surgical evaluation and was further directed to the cardiothoracic surgery department. The patient denied any history of hypertension, diabetes mellitus, and tobacco use. Upon physical examination, a moderate diastolic murmur was auscultated at the cardiac apex area. Electrocardiography showed a sinus rhythm with a heart rate of 63 beats per minute. All initial laboratory tests were within normal limits, except for a mild elevation in B-type natriuretic peptide (108 pg/L). Additionally, hemoglobin was 143 g/L, albumin was 38.5 g/L, aspartate aminotransferase was 13 U/L, alanine aminotransferase was 12 U/L, erythrocyte sedimentation rate was 2 mm/hour, and Troponin was 0.011 μg/L. TTE demonstrated an almost echoless mass measuring 4.6 × 4.4 cm with well-defined margins in the left atrium, which was attached to the atrial septum with a narrow base (Figures 1A,B). TEE showed a large cystic mass in the left atrium that protruding into the mitral valve during diastole, causing mild mitral stenosis (Supplementary Video S1). A cardiac CT scan displayed a giant tumor located in the left atrium with heterogeneous density following enhancement, suggesting the possibility of a myxoma (Figures 1C,D).
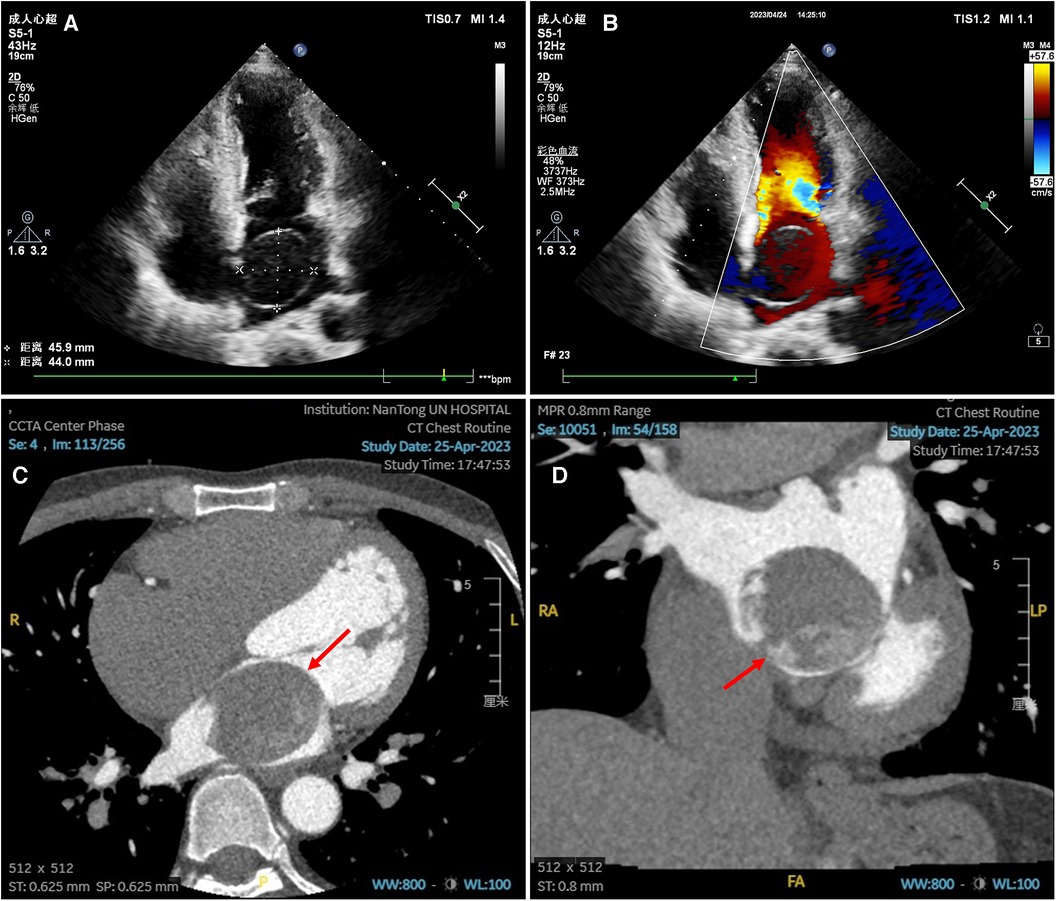
Figure 1. Preoperative echocardiography and enhanced cardiac CT scan images. (A–B) Transthoracic echocardiography showed an echoless tumor measuring 4.6 × 4.4 cm in the left atrium, with clear boundary, a small base attached to the atrial septum, and no blood signal in the tumor. (C–D) Enhanced cardiac CT scan in transverse plane (C) and coronal plane (D) showed a giant tumor in the left atrium with heterogeneous density after enhancement.
The patient underwent a video-assisted thoracic surgery using the Da Vinci surgical system (Intuitive Surgical Inc., Sunnyvale, CA, USA). After double-lumen intubation, cardiopulmonary bypass (CPB) was established by femoral artery and vein cannulation, and a right-sided incision was made to access the chest cavity. During the surgery, a giant parenchymal cyst was found in the left atrium with a pedicle attached to the atrial septum, which was intact (Figure 2A). We attempted to completely remove this lesion. Unfortunately, the cyst accidentally ruptured during resection, causing blood to flow out and resulting in its collapse. Nevertheless, the tumor was completely removed without causing any damage to the adjacent tissue. The total operation time was 2 h and 14 min, the CPB time was 1 h and 18 min, and the cross-clamp time was 35 min. Pathological examination revealed a smooth cyst wall with a thickness of 0.1–0.2 cm. The cyst wall consisted of small stellate and fat spindle cells with round, oval, or elongated nuclei and eosinophilic cytoplasm, surrounded by a mucoid matrix. The tumor cells were arranged in a linear pattern and oriented towards the blood vessels, with no cytological atypia present (Figure 2B). The postoperative recovery process was uneventful, and the patient was transferred from the intensive care unit to the general ward on the second day after surgery, and discharged nine days later, with normal mitral valve and left ventricular functions confirmed through echocardiography before discharge. During the follow-up period, there was no recurrence of myxoma.
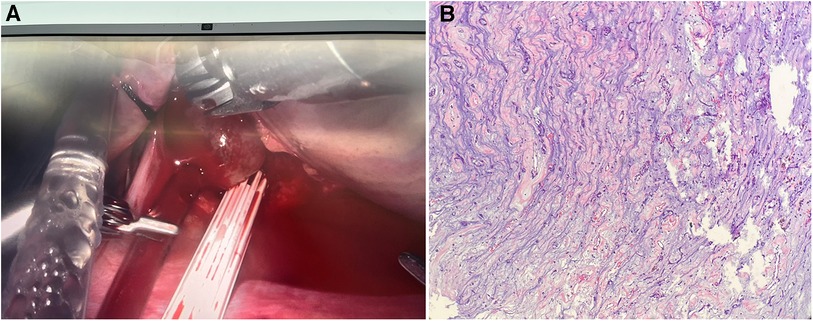
Figure 2. Intraoperative and pathological images. (A) Intraoperative view revealed a parenchymal blood-filled cyst with smooth surface attached to the atrial septum with a pedicle. (B) Pathological examination of the cyst (hematoxylin and eosin stain, ×4) showed spindle cells with eosinophilic cytoplasm surrounded by mucoid matrix.
Discussion
As a very rare tumor, the pathological type of cardiac mass is closely related to its location. For instance, myxoma can always be seen in the left atrium, lipoma is more common in the right atrium or left ventricle, and fibroma and rhabdomyoma are more common in the ventricles (9). While most diagnoses of cardiac tumors are rendered through imaging techniques, some of them may not exhibit characteristic imaging features that suggest their pathological type, making the diagnosis challenging. Therefore, myocardial biopsy plays an important role in the diagnosis of cardiac tumors. Currently, computerized tomography (CT), TEE, or intracardiac echocardiography are commonly used to guide myocardial biopsy (10). Among them, CT-guided biopsy has been proven to be safe for pericardial or superficial intermural tumors (11). For intracardiac masses, myocardial biopsy is most performed via the venous route, including internal jugular or femoral vein, and for left ventricular lesions, biopsy can also be performed by transseptal puncture or directly through peripheral arteries (12). Considering the high risk of myocardial biopsy including vasovagal reaction, pericardial tamponade, arrhythmias, ventricular perforation, and vascular injury (13), it is generally utilized for tumors in the right cardiac system (14). Additionally, myocardial biopsy is considered contraindicated in the following situations: (1) cardiac tumors without a safe puncture path; (2) the surface of mass is surrounded by large tortuous blood vessels; (3) preoperative imaging showing significant necrosis within the lesion or severe coagulation dysfunction; (4) severe dyspnea or agitation; and (5) friable masses with a high embolic potential, such as left ventricular tumors or typical cardiac myxomas (11).
As the most common cardiac tumor, the clinical features of cardiac myxoma depend on the location and size of tumor. Dyspnea is the most frequent symptom of left atrial myxoma, which is a characteristic manifestation of mitral valve dysfunction leading to left-sided heart failure. Conversely, myxoma in the right atrium may result in symptoms related to right-sided heart failure. Given that the majority of cardiac myxomas exhibit a non-cystic structure, embolism should be of particular concern, with approximately half of all cases presenting embolism-related events, including strokes, retinal artery emboli, and limb embolism (15).
Cystic myxoma is a relatively rare condition that is typically identified incidentally via TTE. Through searching PubMed, only a few literatures were found to report the existence of cystic myxoma as shown in Table 1. Reports have indicated the presence of feeding arteries into the tumor, originating from either the left or right coronary artery, potentially leading to coronary steal phenomenon such as angina (5, 8). We hypothesize that hemorrhage within the tumor contributes to the formation of a cystic mass filled with blood. Moreover, the stability of this blood-filled cyst requires a sufficient drainage hole for outlet flow. Diagnosing cystic myxoma requires caution, as the differential diagnosis includes several other conditions, such as CBC, hemangioma, angiosarcoma, hydatid cyst, thrombus, and metastatic tumors (8, 21).
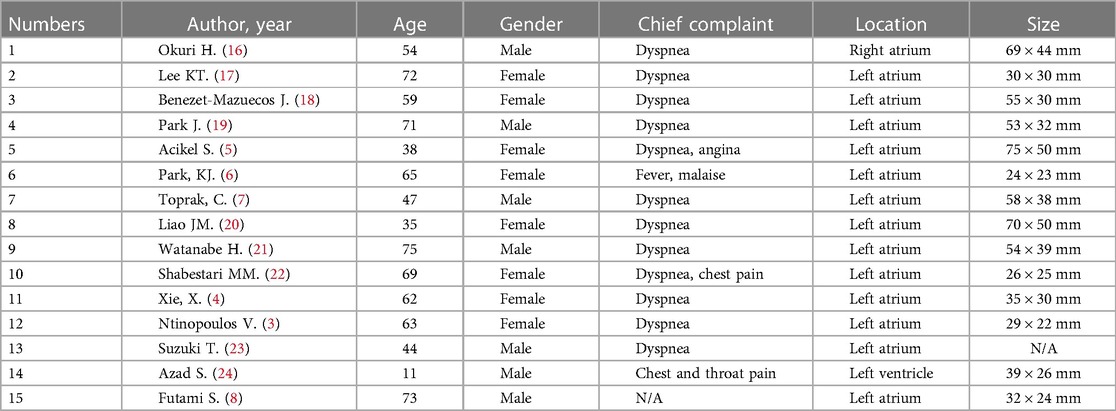
Table 1. Reported cases of cystic cardiac myxoma in the literature till January 2024.
CBC, first documented in 1,844, remains a relatively uncommon benign cardiac tumor, primarily discovered during autopsy and rarely reported in adults (25). Many patients with CBC exhibit no symptoms and are often diagnosed incidentally during routine echocardiography. Nevertheless, CBCs positioned in the semilunar or atrioventricular valves, as is most commonly the case, may induce valve dysfunction.
In the present case, given the smooth and thin morphology of the cyst wall, a CBC was strongly suspected prior to surgery. This suspicion was further reinforced by the intraoperative observations, which revealed a blood-filled, balloon-like cyst. Although an enhanced cardiac CT scan failed to demonstrate any feeding arteries within the tumor, histopathological examination was crucial for arriving at a definitive diagnosis. The result revealed a cyst wall exhibiting myxoma manifestations and lacking endothelial structure, confirmatively indicating a cystic myxoma.
Conclusion
In this case report, we present an extremely rare case of a cystic left atrial myxoma. Preoperative echocardiography of the patient revealed a thin-walled cyst, which was further confirmed during surgery. Additionally, the cystic fluid was found to be bloody, leading us to initially suspect it as a CBC. However, upon the histopathological examination of the tissue, it was conclusively diagnosed as a cystic myxoma rather than CBC due to the absence of endothelial structure in the cyst wall and the presence of distinctive histological features of myxoma.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by The Institutional Review Board (IRB) and ethics committee of the Affiliated Hospital of Nantong University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
WX: Conceptualization, Methodology, Writing – original draft. JQ: Data curation, Software, Writing – original draft. JF: Data curation, Software, Writing – review & editing. FJ: Data curation, Software, Writing – review & editing. XCh: Data curation, Methodology, Writing – review & editing. XCa: Methodology, Writing – review & editing. QX: Conceptualization, Supervision, Writing – review & editing. JS: Conceptualization, Funding acquisition, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This work was supported by the National Natural Science Foundation of China (82370253), Jiangsu Provincial Research Hospital (YJXYY202204), Innovation Team Project of Affiliated Hospital of Nantong University (XNBHCX31773).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2024.1323890/full#supplementary-material
References
1. Rahouma M, Arisha MJ, Elmously A, El-Sayed Ahmed MM, Spadaccio C, Mehta K, et al. Cardiac tumors prevalence and mortality: a systematic review and meta-analysis. Int J Surg. (2020) 76:178–89. doi: 10.1016/j.ijsu.2020.02.039
2. Layton S, Ripley DP, Bellenger NG. Left atrial myxoma. Br Med J. (2013) 347:f4430. doi: 10.1136/bmj.f4430
3. Ntinopoulos V, Dushaj S, Brugnetti D, Rings L, Loeblein H, Dzemali O. Left atrial myxoma: unusual presentation as a cystic tumor. J Card Surg. (2020) 35:511–3. doi: 10.1111/jocs.14401
4. Xie X, Bai J. Left atrial myxoma presenting as a cystic mass. J Card Surg. (2017) 32:694–5. doi: 10.1111/jocs.13224
5. Acikel S, Aksoy MM, Kilic H, Karapinar K, Oguz AS, Aydin H, et al. Cystic and hemorrhagic giant left atrial myxoma in a patient presenting with exertional angina and dyspnea. Cardiovasc Pathol. (2012) 21:e15–8. doi: 10.1016/j.carpath.2011.01.006
6. Park KJ, Woo JS, Park JY. Left atrial myxoma presenting with unusual cystic form. Korean J Thorac Cardiovasc Surg. (2013) 46:362–4. doi: 10.5090/kjtcs.2013.46.5.362
7. Toprak C, Kahveci G, Tabakci MM, Acar G, Emiroglu MY. Unusual image of a cystic atrial myxoma: mass in mass appearance in the left atrium. Herz. (2015) 40:259–60. doi: 10.1007/s00059-013-3923-y
8. Futami S, Hieda M, Fukata M, Shiose A. A rare case of cardiac myxoma with light bulb-like cystic morphology: a case report. Eur Heart J Case Rep. (2023) 7:ytad331. doi: 10.1093/ehjcr/ytad331
9. Seferović PM, Tsutsui H, McNamara DM, Ristić AD, Basso C, Bozkurt B, et al. Heart failure association of the ESC, heart failure society of America and Japanese heart failure society position statement on endomyocardial biopsy. Eur J Heart Fail. (2021) 23:854–71. doi: 10.1002/ejhf.2190
10. Naruse G, Kawasaki M, Yanase K, Tanaka T. Primary angiosarcoma in the right atrium diagnosed by a cardiac tumor biopsy using intracardiac echocardiography. J Med Ultrasound. (2020) 28:120–2. doi: 10.4103/JMU.JMU_93_19
11. Xie Y, Hong ZL, Zhao YC, Chen S, Lin YC, Wu SS. Percutaneous ultrasound-guided core needle biopsy for the diagnosis of cardiac tumors: optimizing the treatment strategy for patients with intermural and pericardial cardiac tumors. Front Oncol. (2022) 12:931081. doi: 10.3389/fonc.2022.931081
12. Veinot JP. Diagnostic endomyocardial biopsy pathology–general biopsy considerations, and its use for myocarditis and cardiomyopathy: a review. Can J Cardiol. (2002) 18:55–65. PMID: 1182632911826329
13. Oliveira GH, Al-Kindi SG, Hoimes C, Park SJ. Characteristics and survival of malignant cardiac tumors: a 40-year analysis of >500 patients. Circulation. (2015) 132:2395–402. doi: 10.1161/CIRCULATIONAHA.115.016418
14. Veinot JP. Endomyocardial biopsy–when and how. Cardiovasc Pathol. (2011) 20:291–6. doi: 10.1016/j.carpath.2010.08.005
15. Butany J, Nair V, Naseemuddin A, Nair GM, Catton C, Yau T. Cardiac tumours: diagnosis and management. Lancet Oncol. (2005) 6:219–28. doi: 10.1016/S1470-2045(05)70093-0
16. Okuri H, Shimizu M, Yokoyama K, Kawada H, Irisawa A, Kikawada R. A case of right atrial myxoma: M-mode and pulsed-doppler echocardiographic findings before and after operation. Kokyu to Junkan. (1993) 41:397–401. PMID: 85165808516580
17. Lee KT, Lai WT, Yen HW, Voon WC, Hwang CH, Lu YH, et al. Cystic left atrium myxoma–a rare case report. Kaohsiung J Med Sci. (2001) 17:579–81. PMID: 1185246611852466
18. Benezet-Mazuecos J, Marcos-Alberca P, Farre J, Manzarbeitia F, Rabago R, Rey M. Multicystic/cavitated giant left atrial myxomas: a matter of technology. Eur J Echocardiogr. (2008) 9:101–2. doi: 10.1016/j.euje.2007.03.040
19. Park J, Song JM, Shin E, Jung SH, Kim DH, Kang DH, et al. Cystic cardiac mass in the left atrium: hemorrhage in myxoma. Circulation. (2011) 123:e368–9. doi: 10.1161/CIRCULATIONAHA.110.004655
20. Liao JM, Nasseri F, Nachiappan AC, Kuban J, Cheong BY. Left atrial myxoma presenting as a cystic mass. Tex Heart Inst J. (2013) 40:358–9. PMID: 2391404023914040
21. Watanabe H, Nara I, Yamaura G, Iino K, Iino T, Shimbo M, et al. Blood balloon induced by an atrial myxoma in the heart. Circulation. (2014) 130:2351–3. doi: 10.1161/CIRCULATIONAHA.114.010732
22. Shabestari MM, Fazlinezhad A, Moravvej Z, Tashnizi MA, Azari A, Bigdelu L. A case of left atrial myxoma with unusual tumor vascularity. Asian Cardiovasc Thorac Ann. (2015) 23:458–60. doi: 10.1177/0218492313513776
23. Suzuki T, Hata M, Yamaya K, Saitou T, Haba F, Matsuno M, et al. Cystic myxoma which obstructed the mitral valve orifice;report of a case. Kyobu Geka. (2020) 73:380–3. PMID: 3239839732398397
24. Azad S, Dutta N, Roy Chowdhuri K, Ramman TR, Chandra N, Radhakrishnan S, et al. Atypical left ventricular myxoma: unusual echocardiographic and histopathological features. World J Pediatr Congenit Heart Surg. (2020) 11:NP129–129NP131. doi: 10.1177/2150135117742626
Keywords: case report, cardiac tumor, myxoma, intracardiac blood cyst, cardiac surgery
Citation: Xiao W, Qin J, Feng J, Jiang F, Chen X, Cao X, Xue Q and Shi J (2024) Case Report: Giant left atrial cystic tumor: myxoma or intracardiac blood cyst? Front. Cardiovasc. Med. 11:1323890. doi: 10.3389/fcvm.2024.1323890
Received: 18 October 2023; Accepted: 5 February 2024;
Published: 14 February 2024.
Edited by:
Enyi Shi, China Medical University, ChinaReviewed by:
Karthik Seetharam, West Virginia State University, United StatesMassimo Baudo, Lankenau Institute for Medical Research, United States
Mohamed Rahouma, Weill Cornell Medical Center, United States
© 2024 Xiao, Qin, Feng, Jiang, Chen, Cao, Xue and Shi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jiahai Shi happysjh167@163.com