AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2643-6612/019
1 Clarós Clinic. Barcelona. Spain.
2 Scholarship Clarós Clinic, Clarós Foundation, Barcelona. Spain.
*Corresponding Author: Clarós P, Clarós Clinic. Barcelona. Spain.
Citation: Clarós P., Cygan A., Clarós A, (2021) Key Points on Short Term Medical Mission International organization on Orofacial cleft J, Dentistry and Oral Maxillofacial Surgery. 4(1); DOI: 10.31579/2643-6612/019
Copyright: © 2021, Claros P, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 April 2021 | Accepted: 01 May 2021 | Published: 17 July 2021
Keywords: orofacial cleft, STMMI organization, short term medical mission (STMMs), non-governmental organisation, international law
Background: Children suffering from congenital facial malformations in underdeveloped countries are the main objective of the STMMIs with the aim of easing their lives. Clarós Foundation (CF) has carried out 115 missions worldwide with the aim, among others, of treating patients with this type of orofacial cleft malformation. We think that the experience we have acquired in this field can be transmitted to new NGOs institutions that want or wish to continue in this line. The optimization of the use of means and human resources, both from the NGO and the local health workers, will make it possible to achieve greater outcomes and results when applied in the development of Short Term Medical Mission International (STMMIs) missions.
Material and Methods: We present the experience CF has acquired throughout the various STMMIs it has accomplished, during a period of 7 days each, specifying the details of its organization, patient selection, preparation of the surgery and its performance, in a well- organized manner to be fast, effective and safe in its results. During each of the 115 missions, the medical team has treated patients with this congenital pathology, in different proportions that go from 90% of the total cases to only 10% of the patients attended. The surgical techniques applied are those used in our medical center in Barcelona, which we may say, are the state-of-the-art surgical techniques used by the most advancedcenters.
Results: A total of 1725 patientsunderwent surgery throughout 115 STMMIs, averageduration of 7 days each,115 STMMIs by 15 cases average. During this time 925 patients were operated for cleft lip and 800 patients for cleft palate. Male patients accounted for 58% and female for 42%. According to the age of the patients we found that the majority of cases were operated on babies 68.35% (1.179 neonatal period); 20.2% on children (300 cases) and (19.76%) adolescents (233 cases); and 1.10% adults in the 20-67 age range (13 cases).
Of the total number of operated patients(1.725), there have been few immediate and late postoperative complications, but we estimate them at 11%.
Conclusion: International cooperation between experienced NGOs and local medical teams turn out to be much more effective, less expensive and with better clinical results than those obtained without this collaboration. This organizational model can be very useful in order to know the details that these missions entail and apply them in your own activities.
Clarós Foundation (CF) is very active in organizing humanitarian medical missions around the world. Since the program started in 1992 in India, until today, all the missions have been carried out in countries of Latin America (Cuba), Eastern Europe (Moldova, Romania, Armenia), Africa (Liberia, Ethiopia, Senegal, Cameroon, Gabon, Sudan, Kenya, Democratic Republic of Congo, Cape Verde, Gambia, Burundi), Asia (Jordan and Uzbekistan). Missions are done upon the invitations of local hospitals and Governments. In many of these countries, medical missions have been repeated regularly every year, such is the case in Senegal - 10 missions, in India 14 missions, Romania 15, Cameroon 5, Gambia 3, Burundi 2, Gabon 5, Ethiopia 5, Cape Verde 10, etc...
CF has a network of over 50 volunteer health professionals, which includes ear, nose and throat surgeons, maxillofacial surgeons, specialists in facial plastic surgery, nurses, audiologists, anaesthetists and other professionals from other surgical specialties, such as vascular surgery or ophthalmology. Most of them come from different cities in Spain, Portugal, Poland, Romania, France, United States, as well as local native volunteers.
Surgical missions are made up of 8-10 members’ unpaid volunteers with basic foreign language skills. These missions last 7-10 days, this is why they are called STMMIs. The local operating rooms (OR) are adapted so that two operations can be carried out simultaneously, which means that in each mission 80-100 surgeries may be conducted. To finance these missions, donations are received from private individuals, private companies and bodies corporate that collaborate and support the Foundation, both through financial contributions and through the donation of medical equipment.
For over 25 years, Clarós Foundation has been committed to tackling the greatest inequities in this world and at the same time has observed many faults done by other NGOs regarding compliance with International Law. This is the purpose for preparing articles on the prevalence of international law by medical responses to domestic or external disasters, full-time relief practice such as Médecins Sans Frontières NGOs.
Medical missions are classified into short and long-term missions. In the last years there has been a shift in focus from long-term overseas assignments to short-term medical missions (STMMs), but both of them address unmet health care needs [1]. STMMs refer to an activity where health care professionals travelto a country with the purpose of providing medical help to the developing countries without compensation for a period from days to a few weeks. They differentiate themselves from other missions who provide medical assistance to people affected by conflict, pandemia, disasters or exclusion from healthcare services, such as Médecins Sans Frontières (MSF), military or other governmental expeditions or residency training programs [2].
We can divide STMMIs in three types: emergency, surgical, and mobile services. Emergency services provide early post disaster medical care anywhere in the world. Surgical services provide any surgical assistance which might be generally unavailable. Mobile services provide medical consultations and surgeries to support primary care in different sites [3].
Facial malformations have undergone a major evolution in their treatment and the final results achieved today are very good in developed countries unlike what occurs in emerging countries, where either they do not have access to being treated by local doctors or they do it with poor or bad results. In advanced and higher income countries there are strict protocols for action, time schedules and the participation of different multidisciplinary teams that coordinate to achieve the best result [4]. However, others with low resources, lack the most basic systems of diagnosis, prevention and treatment [5]. Specialized NGOs, like CF, have provided important help to fill in this gap.
It is estimated that each year more than 160.000 new patients with cleft lip and palate are born in the world.India, China and Indonesia, followed by Pakistan, accumulate the highest incidence. Other countries such as Democratic Republic of Congo, Ethiopia, Cameroon and Africa in general, although in smaller numbers, it is also frequent to find these malformative disorders. This is the reason why CF wanted to contribute to treating this type of pathology which receives a very positive social response. In most of the countries visited by CF, affected children are hidden from villagers to avoid bullying. It is, therefore, thanks to the efforts made by international aid workers, that this punished population has had support to improve its appearance and reduce its incidence [4].
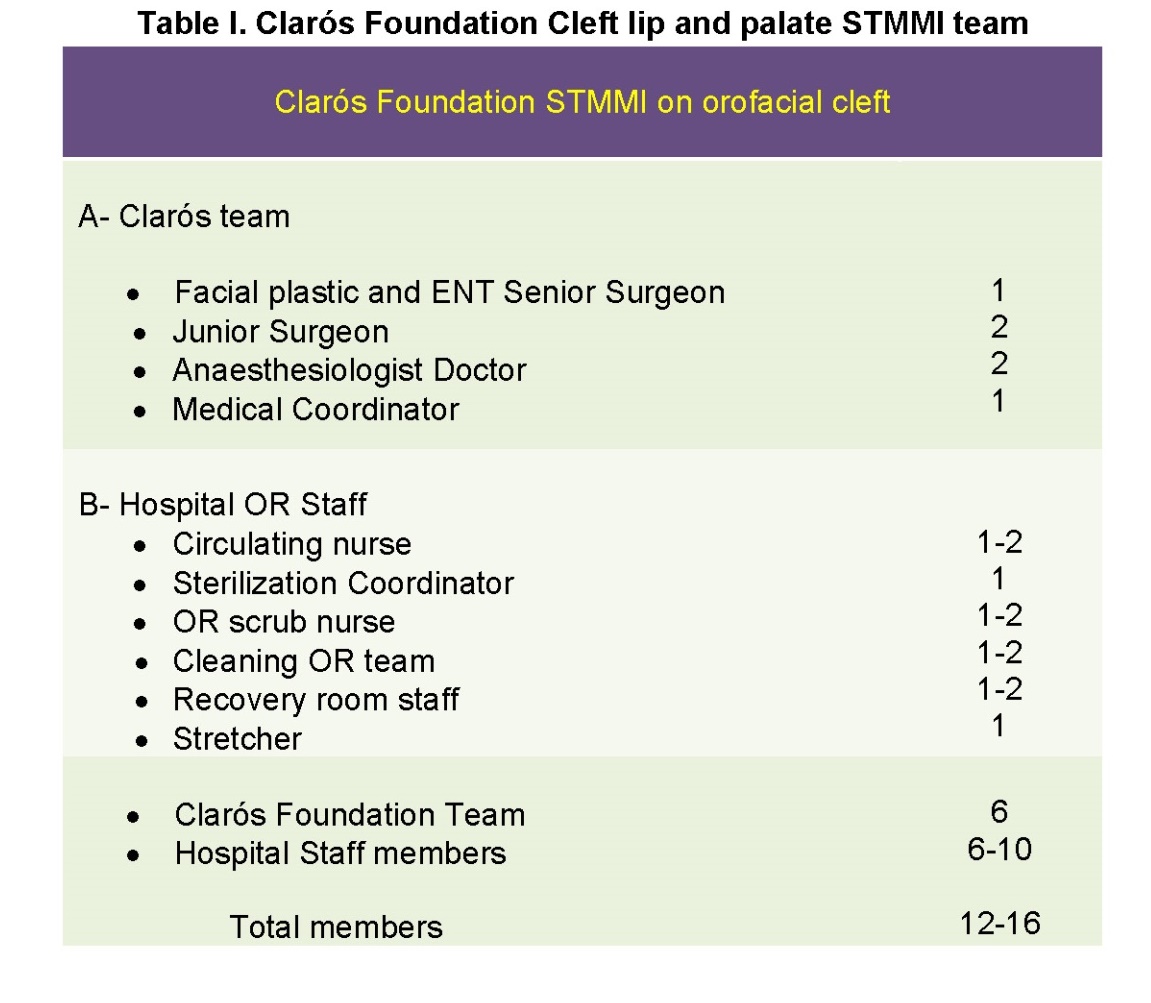
Since 1996, CF has conducted 115 missions, partially focused on Orofacial cleft (OFCs), having treated a large number of patients, in different proportions, for cleft lip and palate, among other types of head and neck pathologies. These missions are composed of an experienced senior surgeon in maxillofacial surgery, assisted by two or three young surgeons who help, prepare and collaborate in the surgical acts, and consequently allowing the chief surgeon to be able to have much more activity and efficiency. In the same team there are two anesthetists who coordinate, allowing anesthesia and resuscitation maneuvers are fast (Table I). We also have an operating room coordinator and the person in charge of care surgical instruments. We operate either in two operating rooms (OR) simultaneously or in a single surgical OR with two independent tables and anesthesia trolleys to be able to alternate a surgery and a wake-up phase at the same time. This way, we can perform about 50 surgeries in a week-long STMMI. It is true that in certain places such as DR of Congo (Kinshasa), some 70-90 surgical procedures by mission have been performed, due at large to the number of cases existing. In other places visited with a low incidence of cases, only 10-15 cases were carried out.
It is important to mention that with years of experience our organization has been able to achieve double results with half the time used since all its components of nursing, OR circulating nurses, anesthesia doctors and young surgeons have improved training. We have to say that the circumstances have been used to teach, but we have never allowed young doctors to experiment alone with their skills. In the same way, the applications of the most current and new procedures and protocols have resulted in better surgical procedures and greater use of time. We believe that this system that we consider to be of good organization should be adapted to apply in a surgical activity as specific as the OFC patient.
A retrospective study was carried out examining all Cleft lip and Cleft palate including orofacial cleft on adult and paediatric over the past 25 years during 115 STMMs performed in India, Senegal,Cameroon, Sudan, Ethiopia, Ghana, Kenya, Gabon, Democratic Republic of Congo, Republic of Cabo Verde, Gambia and Burundi.
Patients
Our study included all the patients with cleft lip and cleft palate, associated or not referred to our team, during 115 STMMs from 1996 to 2021. All the patients were treated by the same senior surgeon specialized in head and neck surgery as well as facial plastic and ENT surgery.
Upon the invitation of different “First Ladies” of countries such as DR of Congo, Senegal, Gabon,Gambia or other countries, or by the members of Government as India, Ethiopia, Kenya, Burundi, etc., we organized the medical missions. We accepted the request and our first mission took place in India in 1992. In 1996, a Hospital in New Delhi proposed to settle collaboration with us. Since then, we continue to repeat these activities over the years. We started the STMMIs in 1992, one per year and from 2000 on we incorporated more activities until reaching 5-6 per year. A good campaign carried out in the local and state media and the participation of local pediatric teams, nurses, family doctors, specialists and pediatric surgery,hospitals, religious institutions and others is the key to recruiting patients. Curiously, in the first days of the STMMI mission, it is common for patients to attend timidly, but in the middle of the week many more appear, as if they wanted to first see the results in their peers before accepting the surgery of their own children.
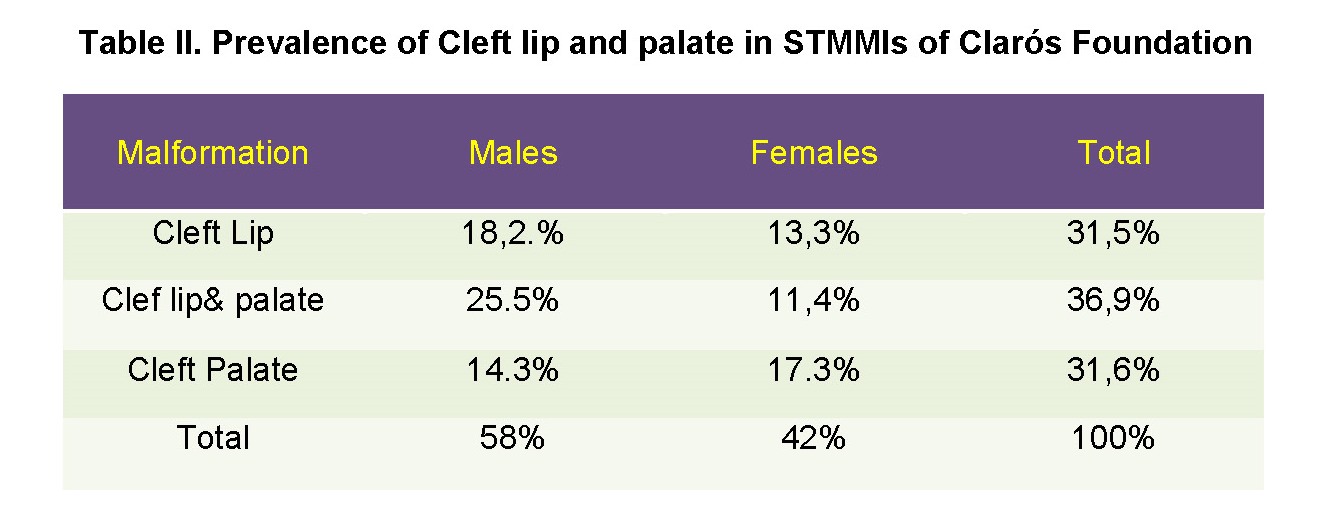
The first patient selection is made by the Chief surgeon, assisted by 2 Junior Surgeons, to assess the degree of facial deformation conveniently selected according to the rules of CF (Table II). From this moment on, they are conveniently labeled with a badge containing the patient's personal data. Once accepted for surgery, the anesthetist performs the pre- anesthesia evaluation and takes into consideration possible surgical risks. Special interest in ruling out other associated anomalies (Figure 1).

Prevalence of the orofacial cleft during STMMI of CF
The location of the Oro Facial Cleft pathology can be divided into six groups: right or left unilateral Cleft lip and palate (CLP1), cleft palate (CP), bilateral cleft lip and palate (CLP2), isolated cleft palate (CP), isolated cleft lip (CL) and medial cleft (MC).
We have calculated the prevalence according to the type of cleft,side, sex, age and the place where it has been most frequent in Clarós Foundation STMMIs. The most common type found was unilateral CLP (40.1%), which was observed more on the left side (23.9%), followed by CP (29.8%). MC had a minimal relationship (0.5%) between facial cleft types.
The average incidence that we have observed during the Clarós Foundation STMMIs shows that in men it is more common to have unilateral CLP (right side, 63.9%) and bilateral CLP (59.1%), while women are more prone to have a CP (61.8%). The highest numbers of cases treated were in 2013, 2014 and 2015 during the CF STMMI carried out in DR of Congo.
Although patients of many ages (adolescents 20.2% and adults 11.5%) have been treated and operated on, it is true that most of the patients did so in the babies’ special in neonatal period (68.3%).
Unilateral left CLP was the most common type. According to gender, men presented a greater number of CLP. In women, the incidence of isolated PC is higher than in men.
As stated in different statistics consulted, we could say that it is estimated that in the world there is an average of 1.4 cases of orofacial cleft in 1.000 live births with extremes of 2.39 Latin America South and 0.38 Sub- Saharan East Africa, [4].
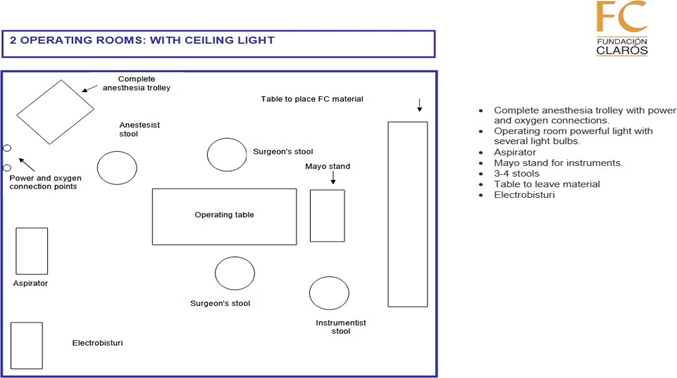
The infrastructure of the operating room (OR) was organized with two operating tables, anesthesia trolleys and electro cautery machine, ECG heart monitors, oxygen-pulsimeter, sets of operating instruments, emergency equipment and all other necessary medications and surgical supplies. We assured that the oxygen equipment for anesthesia was always available and with a sufficient reserve of extra cylinder and pharmaceutical medical material for all interventions (Figure 2).

The mechanism of action of the surgical team is important as to coordination with the aim of not wasting time. With the established system of having permanently two simultaneous operating tables we allow that while a patient is being intervened, the next one is in the phase of being anesthetized and preparing the surgical field with the help of a Junior Surgeon assistant and a surgeon. The senior surgeon together with a junior surgeon proceeds to perform the intervention of one of the patients. The transport systemic carried out by the stretcher who transfers the patient to the recovery room, where the nursing team is responsible for monitoring together with one of the family members. In case the patient is a child, the warmth of the family is important.
The sutures used for the cleft lip were Vicryl 4/0 absorbable on a cutting needle size 17, 5 mm and were left until completely resorbed and reinforced by steri-strape strips on the lip. To avoid removal of stitches, that produces distress to the patient and family, we recommend absorbable stitches, as well as in Cleft Palate. "After lip surgery, use ‘No- Nos' ® or handmade equivalent with the aim of avoiding the baby to touch his mouth and delicate points with fingers and hands (Fig 3).The diet the OFC patient should follow must be very well explained in order to avoid the results of the surgical activity. Smooth foods are typically recommended and bottles should be avoided, as they can rub against the stitches and break them. We recommend the use of teaspoons during the postoperative process as the best option to avoid suture breaks. Breastfeeding was recommended to be done in a few days to prevent sucking with the lips from tearing the sutures. Some foods can be irritating such as citrus fruits and tomatoes due to their acidic properties but once the child has more control, it will be easier to ingest them.
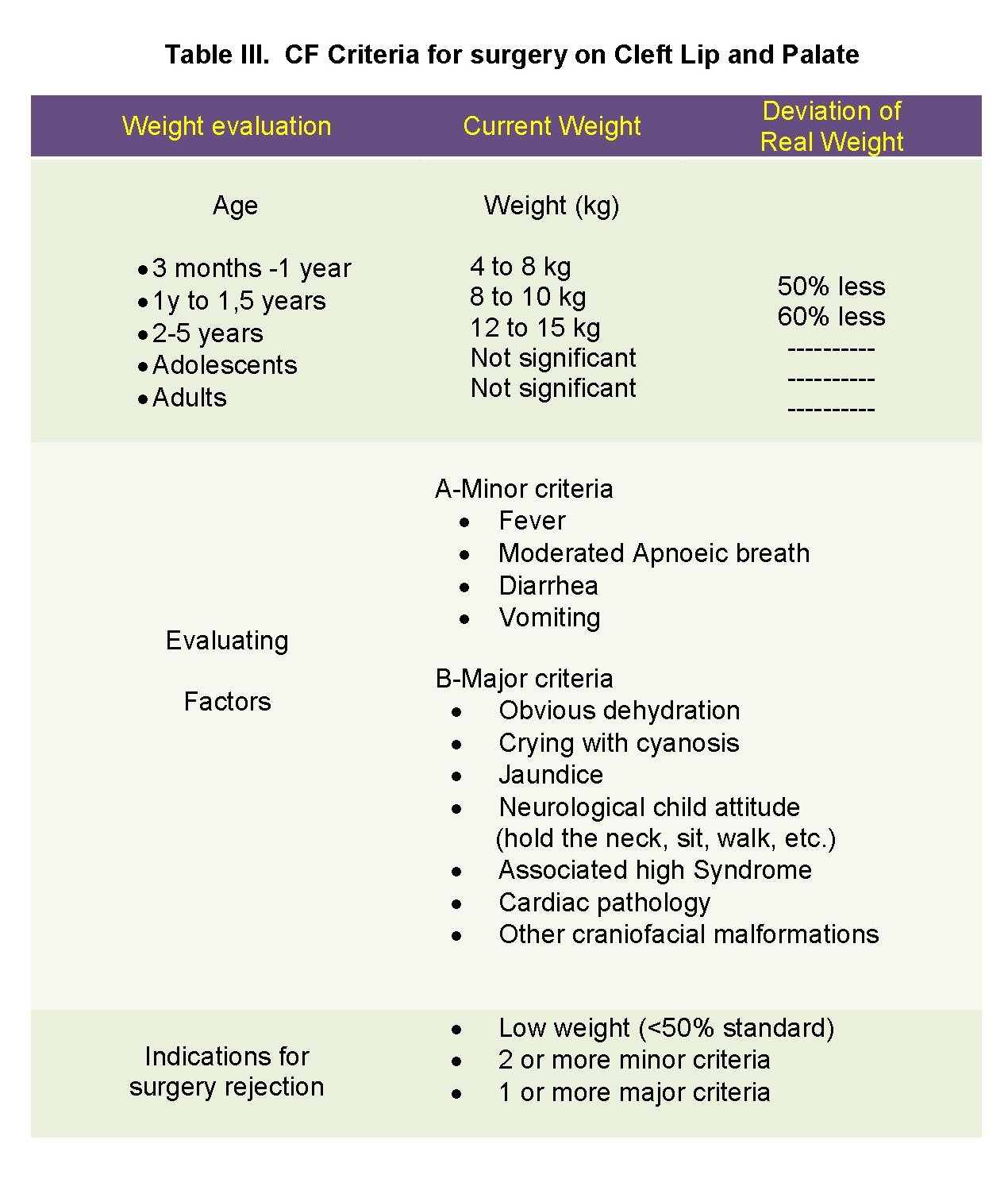
Treatment of patients with cleft lip and palate is complex. The objective of Cleft lip repair is to restore the anatomy of the malformed lip by suturing the upper lip, joining the orbicularis muscle of the lips and the skin and labial mucosa, leaving minimal scars. The procedure is done at the age of three months and with a minimum weight of the baby. This surgery is recommended to be performed before one year of age. Additional surgeries are often required to achieve the best functional results (Table III).

It’s clear that the Cleft Palate Repair, consisting of closing the open palate to restore normal eatingand drinking functionand enhance normalspeech development. The palate forms the floor of the nose and the roof of the oral cavity; therefore, a slit at this level causes free communication between these two cavities [5].
The first information we give the family is about the surgical steps that must be followed and the moment of the surgical intervention that we detail as follows: lip, palate, dent alveolar, scar revision, orthognathic surgery and rhinoplasty, to avoid late management that they resultin nasal speech even in good palatal repair. A multidisciplinary team including: surgeon, anaesthetists, paediatrician, periodontics, orthodontist, speech therapist and psychiatrist), the surgeon will also help to facilitate the management of each case and reduce its complications (Table IV).

Surgical Procedures
For cleft lip procedures, our team uses rotational surgicalprocedures with several minor modifications or Tennison's modality. For cleft palate, we use the von Langenbeck, Veau / Wardill / Kilner or Furlow technique.
Unilateral cleft lips (complete or incomplete) were repaired by Millard rotational advancement [6] or Tennison [7,8] (Triangular repair) techniques. Primary closed rhinoplasty was performed at the same time as all primary unilateral labial repairs. Bilateral cleft lips were repaired using the Millard bifurcated flap technique [9, 10]. Unilateral or bilateral complete / incomplete cleft palate was repaired with von Langenbeck palatorrhaphy technique [11] modified with intravelar veloplasty [12] both for children from 10 to 18 months and adults.
We have been able to appreciate that with the passage of time we have had more and more patients who have benefited from our OFC STMMI as we demonstrate in Table V. The better the missions are organized the better results and efficiency are obtained (Table V).


From our experience, a total of 1725 patients underwent surgery throughout 115 STMMIs, average duration of 7 days each (115 STMMIs by 15 cases average). 53.62% of patientswere operated for cleft lip (925) and for cleft palate, 46.38% (800) patients. Male patients accounted for 58% and female for 42%. According to the age of the patients we found that the majority of 1179 cases on babies neonatal period (68.35%); 300 children 2-7y (25.44%); 233 Adolescents 8-20y (19.76%); and, 13 adults in the 20-67 age range (1.10%).









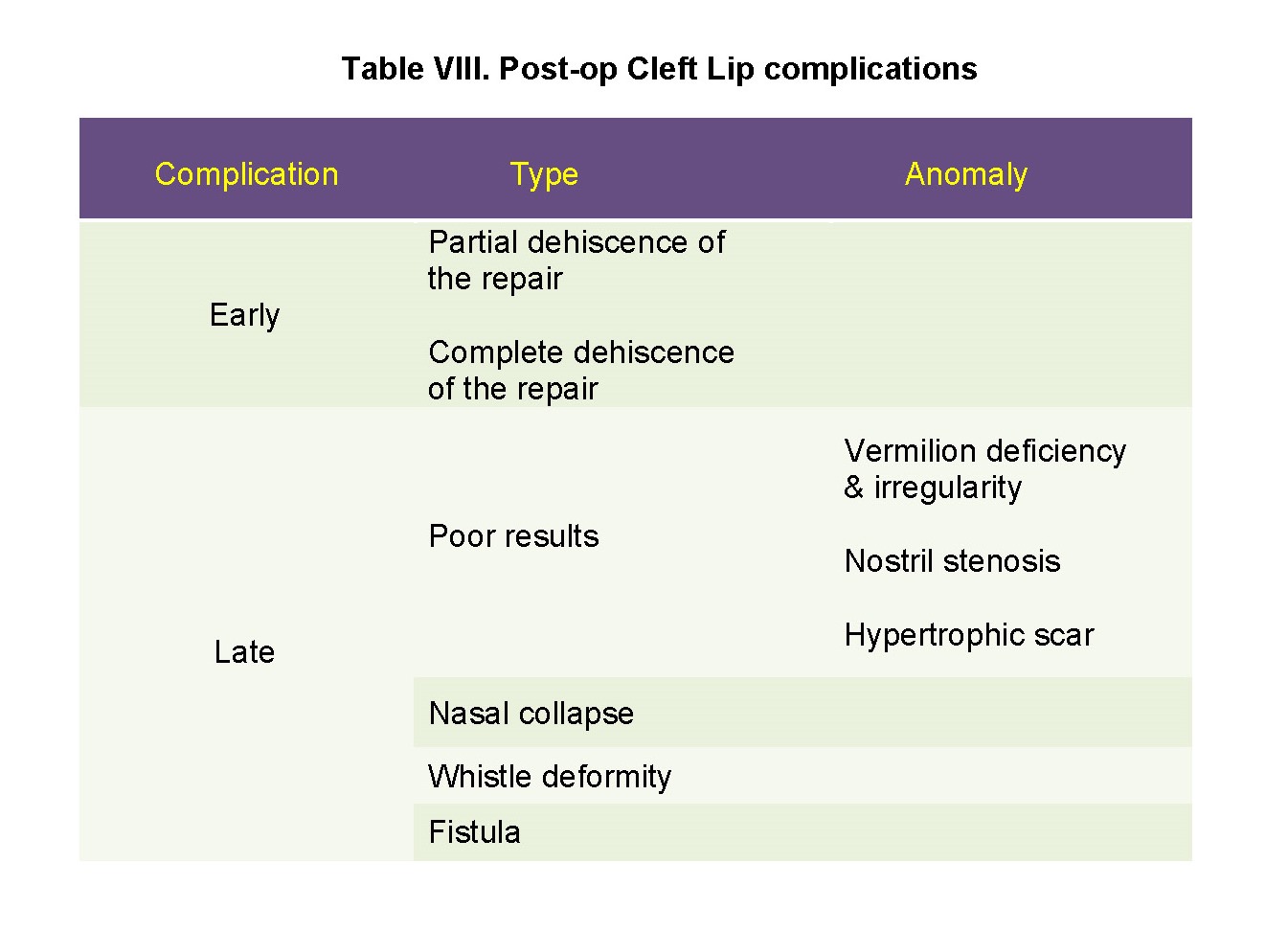
Complications after cleft surgery are clinically unavoidable. Death can occur in patients with OFCs, because they are very fragile children and during anesthesia induction or during the same, it is feasible. During our missions we have reported two deaths, during anesthesia induction and a few days later, due to cardiac arrest. Special attention should be placed to airway problems, bleeding and malnutrition.
Haemorrhage, tissue reactivity, wound dehiscence, and local wound infection were the wound healing complications recorded after cheilorrhaphy for Cleft lip. Tissue reactivity was defined as an erythema and/or crust at the suture site that extended more than 3 mm from the surgical wound. This was defined as spontaneous suture disruptions that are not the result of trauma such as scratching. Local wound infection was diagnosed when the wound contained purulent material and/or showed other clinicalsigns of infection(warmth, erythema, and local tenderness).
Some authors consider that a longer hospital stay contributes to the occurrence of these complications [13]. The exact calculation of the complications of ORC surgery in an STMMI is very difficult to calculate since many, most of the patients disappear and are no longer controlled until, in case of complications, they return to the hospital where the NGO goes again or is another that arrives. Therefore, we only have evidence of those that occurred during the first days or those that the people in charge of reviewing them do communicate it to us.



Orofacial Clefts (OFCs) are anomalies that occur in many human populations. They are isolated or in combination with widespread development disease which has a deep impact on their lifetime. The incidence of patients with OFCs in the world varies greatly according to the countries to which we refer. It is not always possible to find out the incidence rate of many of them, especially the underdeveloped ones, since there are no reliable statistics available. These large differences are due to different ethnic origins, genetics, and various situations environmental and methods of ascertainment. For example, in Asia represent a 1.57 (1.54-1.60), North America 1.56 (1.53-1.59), Europe 1.55 (1.52-1.58), Oceania 1.33 (1.30-1.36), South America 0.99 (0.96-1.02), and Africa
0.57 (0.54-0.60) per 1,000 live births, respectively. The Blacks had the lowest rate of 0.58 per 1,000 live births. Birth defects, especially facial ones, represent a significant problem both at a family and social level and for the individual himself [15].
Countries with high incomes have access to very advanced treatments for their repair and the results obtained are good, even though there can always be more or less important sequelae that will require various treatments. Comparatively, it means that populations with limited financial means will hardly have access to treatment with the guarantees and results they would like [5].
Both cleft lip and cleft palate are malformations that most frequently affect the face of full-term children. They are one of the most common congenital alterations that affect the structures of the face [16]. About 10,000 children are born each year with a cleft lip and palate in East Africa. "It is not known exactly whether these problems are caused by genes that may be responsible for the fissures or by other factors, such as lifestyle or environmental factors"
According to Hlongwa the incidence of CLP in South Africa is 0.3 per 1000 live births, with a provincial variation of 0.1 / 1000 to 1.2 / 1000. The proportion affected by the different anomalies is 35, 3% cleft palate; 34.6% cleft lip and palate; 19.0% cleft lip and other cleft anomaliesat 2%. The distribution by sex of CLP, 47.5%were men and 52.5% women, and this difference was statistically significant (p <0>
The overall prevalence of OFC is estimated to be approximately 1 in 700 live births, accounting for nearly one half of all craniofacial anomalies - are born with either a cleft lip and / or palate and approximately 15% of all congenital abnormalities [18]. As reported by the World Health Organization (WHO), the prevalence at birth of OFC varies worldwide, ranging 3.4–22.9 per 10,000 births for CL/P, and 1.3–25.3 per 10,000 births for CPO [19].
The overall prevalence of CLP was 9.92 per 10,000. The prevalence of CL was 3.28 per 10,000 and that of CLP and 6.64 per 10,000 CLP prevalence at Birth of Cleft Lip with or without Cleft Palate [20].
Approximately 10,000 babies are born each year with a cleft lip and palate in East Africa, congenital deformities that can hinder the development of children, according to the African Foundation for Medicine and Research (AMREF) [21].
It can involve both soft and bony tissues,from the lip area to fissures that connect the oral cavity with the nasal cavity and can cause ear and eye damage. In the case of palatal fissures, the patient has difficulty feeding and breathing, speech problems, lack of development of the alveolar processes, problems of shape, number and tooth eruption that affect not only children's teeth, but also that of adults.
Finding fissured adults in our developed countries is really a total rarity; however, in the countries where we perform STMMIs isn’t rare to be able to treat them, even at unusual ages. For us there is no upper age limit, but it is lower, establishing three months as the lower limit.
Newborns with an Orofacial Cleft have feeding problems due to lack of suction. Children who only have a cleft lip usually do not have difficulty feeding, but when the palate is affected, feeding can be difficult and represents a serious problem for their development. You have to think that the palate acts as a barrier to prevent food and liquids from entering through the nose. Children with a cleft palate swallow a lot of air and regurgitate food through their nose. These children must be fed with special bottles or placement of a naso gastric tube to be able to drink the milk. Its weight gain is very slow and requires pediatric care that in emerging countries does not have access.
CF has been fighting this pathology for years in a way that we could say "on a small scale" although we are aware that large institutions such as the NGO Smile created in 1982 [22]. Other smaller NGOs and Foundations from different countries collaborate in isolation to solve the incidence of these cases.
Our experience is based on the cases operated in India, Gambia, Gabon, Senegal, Cameroon, Cape Verde, Burundi, Ethiopia, Sudan, Kenya, DR Congo, among others but all with the same African profile. Estimates are that they could represent 25% of the entire population affected by this pathology.
Thanks to the STMMIs carried out by specialized NGOs that deal with this type of pathology, solutions can be provided to a population lacking a well-organized public medical system in emerging countries. To guarantee that this is effective, we always try to involve all the local- regional hospital and extra-hospital staff to achieve the best benefits for the affected population. Analysing the complications of dehiscence we have to make the observation that depends on the experience of the surgeon and the care given to the patients. For this reason, postoperative recommendations are important to be followed. In Africa and other emerging countries, the concept that the child cannot go hungry is truly a deeply rooted culture of social status.
Only the close collaboration between the NGOs that carry out STMMIs specialized in Cleft Lip and Palate repair can improve the quality of life of these patients with craniofacial malformations. Teaching these surgical techniques to young teams of surgeons from countries in need is the key for them to have self-sufficiency in solving this pathology. Good organizations carried out by the institutions that are dedicated to it allow operating more and bettering in places where there are large numbers of them.
Patients or their parents or guardians provided written consent for the use of the patients’ image.
To the entire FC team that for many years has accompanied its members to carry out these humanitarian activities.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
