According to the World Health Organization (WHO) and United Nations Children’s Fund (UNICEF),1 every woman and child has the right to access high-quality maternal and newborn services. Globally, in 2020 and 2021, nearly 47% of under-five deaths occurred during the neonatal period.2,3 While, also globally, 2.5 million child deaths occur in the first month of life,1,3–5 with 2 millions additional of those being stillbirths.1,6 Women and newborns also die every day from complications during pregnancy, childbirth, and postnatal.7–10 During childbirth or the first 24 hours of life, most mothers and their neonates die.11 It makes the day of birth, time around labour and childbirth, immediate postnatal care or first 28 days highly vulnerable for neonates (and mothers).2,3,7–9,12 Poor quality of care rather than an inadequate access to health system is currently the top barrier to reducing mortality,13 improving maternal newborn and child health,11,14–16 with 60% of mortality arising from preventable healthcare conditions.13 The remaining 40% of deaths result from non-utilization of the health services.13 Since skilled care around childbirth is one of the approaches to reduce maternal and early newborn morbidity and mortality,17,18 developing countries, including Namibia, have reported an increasing number of skilled birth attendants.19 Yet, as health facility deliveries are increasing, more preventable deaths are reported.19 This is the case even though most neonatal deaths, stillbirths and maternal deaths are preventable with high-quality evidence-based interventions e.g., antenatal care, early essential newborn care, and early essential care for labour and childbirth delivered before, during births, hours, and immediately postnatal period.1,12,13,20–22 Also, poor quality of care accounts for half of maternal deaths, around 60% of neonatal deaths1,13,22,23 and stillbirths.6,23 Without recognizing the fundamental role of quality healthcare, it will be challenging to achieve Sustainable Development Goals (SDG) 3 on good health and well-being and gender equality, goal 5.11 Thus to improve maternal and newborn health outcomes, the health system needs to prioritize quality healthcare.
As reported in our baseline paper from this piece of work,24 the WHO/UNICEF/UNFPA maternal and newborn eight quality standards were developed in response to the growing need to improve the quality of maternal and newborn care during childbirth.19,25 The WHO quality of care framework consists of three domains. The first two domains have three standards each, and the third has two standards, and each standard has quality statements, and each statement has several quality measures. The first domain is the provision of care and include: 1) evidence-based practice for routine care and management of complications; 2) actionable information systems; and 3) functioning referral systems. Second is the experience of care: 4) effective communication; 5) respect and preservation of dignity; and 6) emotional support. The cross-cutting domain include: 7) competent, motivated personnel, and 8) availability of essential physical resources.19,24,26 The quality statements measure within each WHO standards are concise statements of priorities for measurably improving quality of care around childbirth. "They define the markers of quality derived from evidence on the thematic areas and the resource required. While the quality measures are criteria for assessing, measuring, and monitoring the quality of care as specified in the quality statement. They include three elements: inputs- what must be in place for the desired care to be provided, e.g., physical resources, human resources, policies, guidelines. Outputs- whether the desired process of care was provided as expected; and outcome: the effect of the provision and experience of care on health and people-centred".19(pp18-19) WHO defines what quality of care is including what maternal and newborn quality of care entails. WHO defines the quality-of-care as the "extent to which healthcare services provided to individual and patient populations improve desired health outcomes.19(p14) WHO further explains that to achieve the above definition, the health care must be safe, effective, timely, efficient, equitable and people-centred".19(p14) While, the quality of care for women and newborn is the level at which maternal and newborn health services (for individuals and populations) improve the chance of delivering opportune/timely, appropriate care with the objective to attain required results that considers women and their families, and aligns with the current skills and knowledge.19
In Namibia, the first seven days is accountable for three-quarters of neonatal deaths with most happening in the first 24 hours.27 Kavango region or northeast Namibia’s neonatal mortality increased from 21 in 2007 to 27/1000 when compared to national level 20/1000 live births in 2013.28 During the same period, infant mortality rate also increased from 49 to 62/1000 live births.28 Meanwhile only 47.7% of mothers and 3% of newborns received postnatal care within two days after delivery.28 According to the district health information system data, in 2017, almost half of deliveries in Kavango region occurred in the intermediate hospital. There was also an increase in births from 8399 in 2016 to 8823 in 2019 and 11967 in 2020. Our hypothesis is improving quality of maternal and newborn care during labour, childbirth and first week of life reduces neonatal mortality. To address and support response to the increasing newborn deaths amidst increasing facility deliveries, this study report on pre-and-post implementation of WHO/UNICEF/UNFPA quality of care standard measures/interventions, northeast Namibia. The facility maternal and newborn care practices were benchmarked against the WHO definition and implementation of maternal and newborn quality standards or interventions.19
The study aims to assess and describe the quality-of-care practices around labour, childbirth, and immediate postnatal care pre- and post-implementation of interventions to improve care in northeast Namibia.
METHODS
Study setting
Kavango region (east/west) is situated 730km away from two national referral hospitals. It has the only northeast regional referral hospital covering three district hospitals and the Zambezi region, which is 500km away, far northeast of the country. It is also among the four high-volume hospitals in the country and serves as a teaching hospital. According to the Namibia national statistics agency,29 the Kavango region has a relatively young population, with 43% below 15 years old and 53% female.30 Kavango East, where the study site was located, accounts for 50.14% (124 286) of the total population.29 Most births (72.8%) are health facility deliveries, and 75% are by skilled birth attendants.28 Less than half (47.7%) of mothers and 3% of newborns received postnatal care within two days after delivery.28 There were increases in births from 8399 in 2016 to 8823 in 2019 and 11967 in 2020. In our baseline study, we found an exemplary implementation of the World Health Organization, United Nations Children’s Fund, United Nations Population Fund (WHO/UNICEF/UNFPA) quality measures for admission, labour and delivery but poor care during the immediate postnatal period.24 Quality measures on experiences of care quality domain were also poor.24 This study reports progress in quality-of-care practices around childbirth, the early postnatal period and care experience, pre-and-post-implementation of quality improvement interventions.
Study design
A before-and-after quasi-experimental study design was applied using structured quantitative interviewer-administered questionnaires adapted from the Every Mother Every Newborn (EMEN) childbirth assessment tool.31 To determine the type of interventions or level of care women and their babies receive during labour, childbirth, and early postnatal care we conducted a baseline survey,24 January 2020 for 2019. The baseline study assessed the quality of maternal and newborn care provided during labour and delivery and postnatal period. This was followed by implementation of the WHO/UNICEF/UNFPA standards/interventions, January 2020 to December 2021(intervention phase) and then an end of study evaluation from January to July 2022. Some findings from the baseline survey may reflect in this paper for reasons of comparison. Through UNICEF Namibia country office, the interventions were supported (PhD intervention phase). The earlier described eight WHO/UNICEF/UNFPA standards/interventions were then implemented for 24 months (January 2020 to December 2021). The ongoing implementation of the interventions end of this study will be reported elsewhere, including the study processes. This study, therefore, reports on and describes the quality-of-care practices pre-and-post implementation of the WHO/UNICEF/UNFPA interventions/measures around labour, childbirth, and immediate postnatal care period.
Description of materials/tools
As reported in our EMEN tool and baseline assessment papers,24,26 the EMEN quantitative survey or quality assessment tools are designed to narrate a story of care provision through inputs, outputs/process, and outcomes around time of birth. The tool consists of six structured questionnaires, 1) facility physical, structural, and functional readiness form1; 2) facility management interview form2; 3) facility staff interview with vignettes form3; 4) facility observation of provider-client interactions and care provision form4; 5) client medical records review form5, and 6) women’s exit interview and companion perceptions of care form 6.
Within the EMEN Tool, we used Form (questionnaires) 1, which assesses space, services, equipment, drugs, and supplies used to provide quality care. Form 2, Management interview to reviews overall facility policies, guidelines, and staff rotation. Form 3, for staff, to determines formal and refresher trainings received by staff providing maternal and newborn care, and performance of signal functions. Form 3 also contains vignettes to test staff knowledge and practices. Form 4, observations, follows up a woman presenting in labour as she navigates the care process via stages of childbirth. The observation questionnaires also provide real time data on care provision and highlights gaps identified including provider-client interactions. Form 5. client medical record, we captured quality of data on care provision, assessed the quality-of-care content including partograph review, and caesarean section, and collected data on outcomes. Details on outcomes data will not be part of this paper, but future manuscripts; and Form 6, women exist interviews, was used at the time of discharge to collect women’s perspectives and experiences of their care during their hospital stay. It obtains data (mother’s report) from time of admission, through labour, childbirth, and postnatal care until time of discharge home. It further gathers information on examinations, tests, providers’ attitude, hygiene, payment of legal and illegal fees. As per our baseline paper,24 the EMEN tool was developed by pulling together best interventions of WHO’s service availability readiness assessment (SARA) and those used in vigorous research settings.32 By using EMEN tool to collect data we were able to capture both strengths and gaps in quality-of-care including those reported from other large studies,.32–35 We chose the EMEN tool because it is designed to assess quality-of-care within 24 hours (30) and has the ability to capture quality measures around childbirth. (26, 31) Results from the use of EMEN tool is published in peer-reviewed studies done in Bangladesh, Ghana, Tanzania, and Namibia, (25, 31-33) and captured noteworthy strengths and gaps in quality care around childbirth.24,36 For example, Manu et al study found 61% to 80% increases in the implementation of EMEN-QI standards.36 This demonstrates the strong validity and reliability of the EMEN tool and results from this study. Since no single tool is sufficient on its own to capture all quality measures.37–39 We encourage researchers to use a mixture of the tools to derive the best benefit of the results.24 Even if it is one quality domain to be assessed, we found at least 3-4 EMEN tools to widely capture quality standards measures.24 Details of the EMEN childbirth assessment tools have been described previously.24,26,31,32
Data collection
We collected quantitative survey data from January 2019 to December 2021, whereas 2019 is the baseline (preintervention) and 2021 the end-of-study (postintervention), while 2020 and 2021 were the intervention phase. During the intervention phase, continuous monitoring and/or follow up field visits to the research site was done as part of routine programme visits. End of study data collection was completed mid-2022. Two student medical doctors were trained as data collectors in December 2019 and refreshened in January 2021. The international UNICEF consultant, a senior researcher who also led similar studies in Bangladesh, Ghana, and Tanzania jointly with the first author trained them. The student medical assistant researchers conducted pre-and post-exit interviews with women who successful delivered their babies prior to their discharge home. They also observed provider-client interactions during the care process. The data collected did not include respondents’ identifiers. While one retired senior nurse and three third year student nurse midwives were also trained and interviewed staff, and the facility manager. The first author interviewed the medical doctors (staff). The assessors read and explained the purpose of the study orally before each interview and asked the participant to indicate either “yes” or "no’'. The interviews proceeded with only those who consented.
Sampling
The intermediate hospital Rundu was purposively selected because 1) It is the only regional hospital in northeast Namibia; 2) in terms of volume of deliveries, it is among the four hospitals with high-volume of patients in the country; 3) Northeast Namibia is among the regions or districts supported by UNICEF Namibia-due to its poor child health indicators. Thus, UNICEF resources were used to support interventions to address quality-of-care around childbirth. Since the same EMEN quantitative questionnaires were used pre-and-post intervention we applied the same selection criteria as at baseline.24 For example, staff selection for interviews were purposeful (pre, 20; post, 24) and included staff working with pregnant women, in the labour and delivery ward, and in the postnatal and premature unit regardless of the age and professional level. While the facility manager was conveniently selected for the interview as the only facility manager. The women observed were conveniently sampled during the data collection days (baseline, 53; end of study, 60) at admission into the maternity ward for labour and delivery. The women who successfully delivered their babies prior to their discharge from hospital (baseline, 100; end of study, 102) were also conveniently sampled for interviews during the data collection. The sampled number of the facility manager, staff, and observed women, and exit interviews at discharge for women who successfully delivered their babies was an estimation of having good reach on saturation and obtaining sufficient voice representation. In this study, the four stages of childbirth were observed, including admission into the maternity ward, labour, delivery, and immediate care after birth/early postnatal care period. Of the 60 women observed in the post-period, 50 were observed for all four stages. The interviews at the time of discharge home with women who successfully delivered babies were with different mothers at baseline and a different group of women for the end of study. The professional and socio demographic characteristics of staff and women interviewed and observed were similar in context and/or eligibility criteria applied. Table 1 shows other characteristics for exit interviews with women prior to their discharge home.
Data analysis
Data was entered into SPSS by a private statistician who was consulted by the first author. The statistician is not part of the study team. The first author performed data cleaning before analysis using SPSS for version 28.0.1.1
Descriptive statistics were used to summarize results in tables, figures, and text. Minimum and maximum age and standard deviation for age of exit interviews was also calculated. All the questionnaires were coded for anonymity with no link to any participant. The first ten questionnaires of each tool were cross-checked and verified for correction by the first author who was available for the first week of data collection. Any errors or missing variables were returned to a particular assessor for correction. If the mother was not traced during verification window, the data was declared missing. We adopted26 the scoring analysis approach for data collected using the EMEN tool used by Brizuela and colleagues38 and expanded24 on it by benchmarking our results from the tool against each quality measure.24 We then analysed the proportion of responses from each tool against a WHO/UNICEF/UNFPA standard measure. In summary, the responses from the EMEN tool were aligned to each quality-of-care measure within the quality statement across each standard. This was crucial step in having a summarized table of results depicting clearly which indicator(s) or quality intervention(s) were poorly, moderately, or highly practiced. It then becomes easier to tell from the table (Table 2) which of WHO/UNICEF/UNFPA quality measures under each quality statement and/ or standard were poorly/low, moderately and/or highly performed. Similar details of the calculations of responses from the applied EMEN tool versus the WHO/UNICEF/UNFPA standards can be found in our other paper (S2 Table,24) This study focused on measures during admission, labour, childbirth, immediate postnatal care, and women’s experience of care. For the latter two, we also compare women’s exit interviews and observations of women in the maternity ward.
RESULTS
This is the first study to document the quality-of-care provided at admission, during labour, childbirth, and early postnatal care after implementing quality improvement interventions in Namibia. Pre-intervention, 100 women delivered in the hospital and 53 women were observed. Post-intervention, 102 women successfully delivered their babies, and 60 women were observed. We had a power of 74-80% at alpha 0.5 based on this sample size to provide a 20% difference in mortality outcome (http://powerandsamplesize.com/Calculators/Compare-2-Proportions/2-Sample-Equality). The mortality outcomes will be reported in future manuscript(s). Table 1 shows high (78.4%) unemployment for exit interviewed women, with 25.4% of them being adolescents (10-19 years) and young women, 20-24 (25.4%) and 25-29 (23.5%) years respectively. The minimum age at pre-and-post was 12 and 15 years respectively, while maximum was 42 and 41 years respectively. The mean age was 23.94 and 24.89 at baseline and end of study/follow up, with Standard Deviation (SD) of 6.897 and 6.550 respectively. Table 1 also shows that most births were by spontaneous vaginal deliveries, while deliveries by caesarean sections were 18.6%.
Table 2 shows how each quality statement measure within the WHO/UNICEF/UNFPA standards performed before and after quality improvement interventions. We refer to three levels of performance in quality-of-care practices. The levels include low or poor if responses are 0-49%, moderate if responses 50-79% and high if responses range 80-100%.24
Table 2 shows varying performances across the WHO/UNICEF/UNFPA quality standards and statement measures at the postintervention phase compared to baseline. For standard 1, 62.5% (5 of 8) moderate (range 63.8- 74.8%) performance for quality-of-care statement measures on evidence-based care practices. However, Table 2 shows high performance for quality statement measures on actionable information systems (standard 2) and functional referral systems (standard 3) (range 96.1-100%). Meanwhile, 50% (1 of 2) of the quality statement within effective communication (standard 4) and 66.7% (2 of 3) on respect and preservation of dignity (standard 5) show moderate performance. While for emotional support (standard 6) quality statements, one shows maintenance of its low/poor (35.0 versus 42.1%) and another moderate (56.0 versus 58.8%) performance level. Further analysis of emotional support measures shows that both at baseline and end-of-study providers allow no woman a companion of choice, and both at baseline and end-of-study providers allow no woman a choice of companion. Meanwhile, all quality statement measures on competent and motivated staff (standard 7) and essential physical resources (standard 8) show high (above 80%) performance at postintervention.
Healthcare for mothers at admission, during labour and childbirth
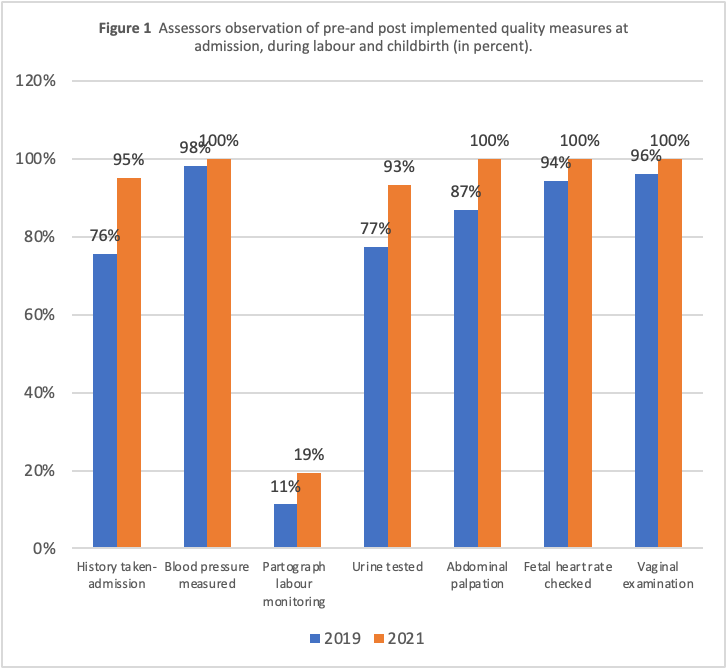
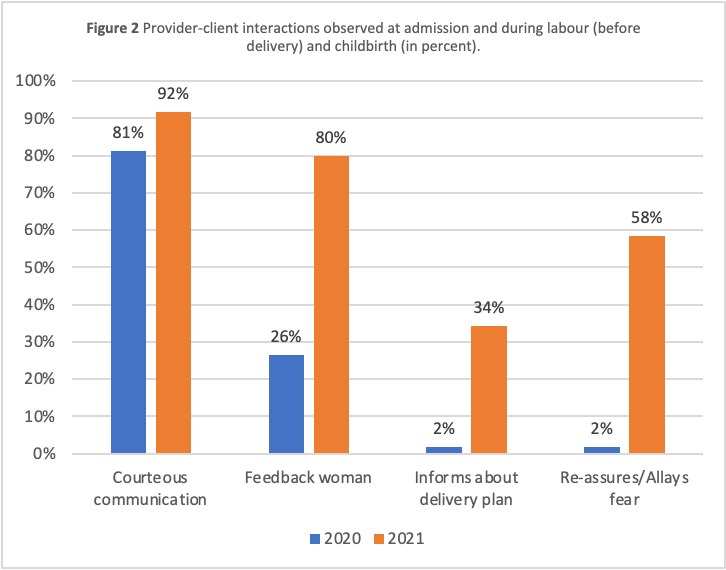
Figure 1 shows an assessment of most (range 93%-100%) women at admission and during labour for vital signs. The process of assessing their vital signs includes history taking, blood pressure checks, urine testing for protein, foetal heart rate, abdominal palpation, and vaginal examinations. On the contrary, only 19.3% of women whose labour was monitored using a partograph. This translates into an 8% increase from baseline. Figure 2 shows that most providers (81.1% versus 91.7%) communicated courteously with women. Also, compared to the baseline period, more women (26.4% versus 80.0%) received feedback after examination(s) post-study intervention. There was also a 32.4% increase in providers informing women about the delivery plan.


Healthcare for maternal and newborns immediately after birth, and during postnatal care
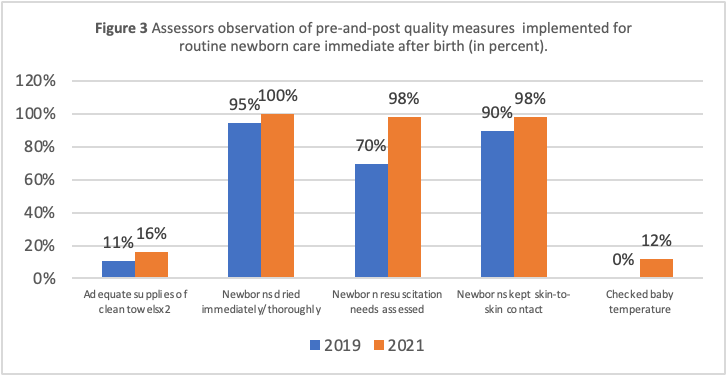
WHO recommends that newborns receive routine evidence-based care and manage their complications according to WHO guidelines.19,40 Despite inadequate (16%) availability of clean towels in the delivery packs for drying the baby immediately at birth, Figure 3 shows high performance in providers placing babies’ skin-to-skin with the mother (98%), assessing newborns for resuscitation needs (98%) and immediate, thorough drying (100%). All immediate newborn care measures improved from the pre-intervention to the post-intervention period.

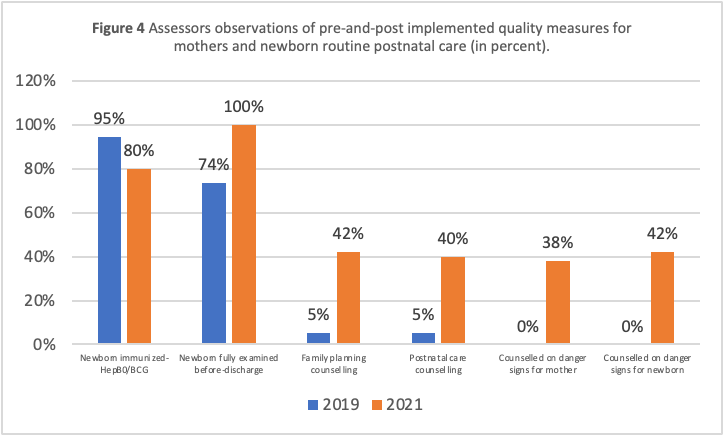
Figure 4 shows increases in providers performing routine postnatal quality-of-care measures for mothers and newborns. Most newborns were immunized for HepB0/BCG (80%), with full examinations (100%) done before discharge. Though the proportion of immunized babies was still high by postintervention, this practice recorded a decrease of 14.7% (94.7 versus 80%). While counselling the mother on danger signs and how to care for themselves and newborns, maintained low or poor performance (ranging from 38% to 42%).

Competent and motivated personnel, and Provider-client interactions
Despite high coverages or performance for competent and motivated staff quality-of-care measures; further analysis within measures reveals that fewer staff (baseline 40.0% versus end-of-study 45.9%) were trained or refreshed on essential newborn care and breastfeeding management. In contrast, the proportion of staff training or refreshers on routine postnatal care and breastfeeding within the last 12 months remains low (25.0 versus 39.6%).
Table 3 summarises the provider-client interaction on experiences of care for the four stages of labour. For example, there is an improvement in women’s satisfaction with health services from moderate (69%) to high (83.3%) performance. Women satisfaction with breastfeeding information increased from low (48.0%) to moderate (56.9%). Whereas satisfaction with the post-partum care and hygiene information remains low or poor (41.0 versus 43.1%).
Also, when comparing responses from exit interviews and assessors’ observations, more improvement was observed in provider-client interaction than women’s reports of their experiences. For example, though the improvement was reported in provider’s courteous communication with women in both pre-and-post exit interviews (73% to 83%), and pre-and-post observations of maternal women (43% to 55%); the difference in the percentage increases for exit interviews (8.4%) and observations (10.6%), respectively were small. That is 2.2% more for observed providers courteous communication acts. A high (53.6%) improvement was observed in providers providing feedback to mothers after examination (26.4 to 80%) when comparing women’s reports or exit interviews (47% to 55.9%). That is an 8.9% increase for exit interviews. On the contrary, at pre-and-post, few providers were reported (exit interviews: 17 to 19%), and 1.9 to 8.3% were observed to communicate delivery plans to women. Also, at preintervention, none of the women were observed receiving counselling from providers on maternal and newborn danger signs. By postintervention, 38% and 42% of women were observed counselled on maternal and newborn danger signs, respectively.
DISCUSSION
This is the first study in northeast Namibia to assess quality-of-care practices at admission, during labour, childbirth, and early postnatal period post-quality improvement interventions. It is also among few studies that identify noteworthy implementation gaps inconsistent with the WHO/UNICEF/UNFPA standards for improving the quality of maternal newborn care19 and for improving the quality of care for small and sick newborns.19,24,33,40
Overall, for post-implementation of quality-of-care interventions, we report both increases and decreases in providers practicing quality-of-care measures across the standards pre- and post-intervention. Communication measures within the experiences of care quality domain are interwoven across the quality-of-care standards, affecting the provider-client interactions during the intrapartum and postnatal care periods. For example, few providers communicate and involve women in their care or the care of their newborns. This result is consistent with our baseline results on the same site.24 While there were increases in providers-client interactions, the level of practices/improvement is not adequate to attain good engagement or a high overall performance level. Below, we present our discussions into themes aligned with the first three quality statements within evidence-based care (standard 1).19
Women are assessed routinely on admission, during labour and childbirth
To identify and manage complications on time, women need to be assessed on admission, during antenatal care, pregnancy, labour history, and confirmation of labour.19 The assessment includes checking foetal heart rate, vaginal and abdominal examination.24 To detect pre-eclampsia, WHO recommends urine testing for protein and blood pressure measurement.41 In this study, all women’s blood pressure measurements, urine testing, foetal heart rate and vaginal examination were performed.19 Suggestive that monitoring vital signs at admission and during labour as per WHO guidelines is done for most women.19 This result is consistent with our baseline findings from the same site.24
Also, WHO recommends monitoring labour progress using a partograph,19 as managing labour progress using a partograph assists with the timely identification and managing delays or labour obstruction as per WHO guidelines.42 However, at baseline and post-intervention, few providers monitored women’s labour using a partograph.24 This result is consistent with previous author42 and our baseline result.24 Though the result is not inspiring, the use of partograph in this study it is still higher than a Bangladesh study by Billah et al,34 where none of the facilities used a partograph.34 It is unclear if healthcare providers lack knowledge and skills in labour monitoring,42 a skill crucial for early identification of prolonged or obstructed labour and timely care and management initiation.42,43 In Namibia, during the intervention phase and last half of 2020, UNICEF Namibia supported the revision of the maternity records.24 The revision includes inserting the new WHO Labour Care Guide (LCG). Since mid-2021, maternity records or LCG orientation and training of doctors and nurse midwives working with pregnant women in labour and delivery and postnatal care is ongoing. The good news about the new WHO Labour Care Guide is that the intrapartum care recommendations promote a positive childbirth experience.43 The four recommendations address similar key quality-of-care gaps found in this study. They include 1) provision of respectful maternity care to women to ensure freedom from harm and mistreatment, that enable informed choices and continuing support during labour and childbirth, 2) Effective communication, 3) Companionship and 4) Continuum of care.43 By the time of data collection, we submit that the small increases in labour monitoring could be due to a few staff’s orientation or /training on the new LCG. It is suggested that the more staff receive orientation and training on the new LCG, the likelihood of providers monitoring labour using a partograph/LCG increases. We recommend training or refreshers on the importance of proper use and timely documentation of vital signs to accompany the regular supplies of the partographs.17,34 Regular supervision for improved childbirth and immediate postnatal care outcomes will likely improve labour monitoring.17,24
Mothers and newborns receive routine care immediately after birth and postnatal care
Routine care in immediate afterbirth supports the adaptation of the newborn to the new environment and meets the baby’s needs in the most suitable manner that reduces preventable complications.19 In this study, immediately after birth, most babies were dried immediately and thoroughly, and placed skin-to-skin contact with the mother. This practice complies with standard 1, evidence of care especially measures on routine newborn care immediately after birth.19 Keeping babies warm by practising skin-to-skin contact with the mothers immediately after birth was sustained high both at baseline and end-of-study. This is a crucial element of care, as even very preterm infants, irrespective of clinical stability, do not develop hypothermia after birth during immediate skin-to-skin contact.44 Affirming concerns that thermal regulations should not limit implementation of skin-to-skin contact immediately afterbirth even in high resource settings.44 This finding is consistent with several authors19,40,44 promoting skin-to-skin but inconsistent with one study conducted in India,33 where putting babies skin-to-skin contact with their mothers was mostly not practiced.
WHO recommends providing routine postnatal care for mothers and newborns19,40 as it has a protective effect on newborn death outcomes.45 In this study, few mothers and neonates receive post-partum and post-natal newborn care. This result is consistent with several authors.24,28,32–35,46,47 According to the NDHS 2013, postnatal newborn care within 48 hours after birth was almost non-existent (3%).28 A similar result to a Malawi study.46 According to Lazzerini at al.48 women suggest improving quality-of-care provision by increasing counselling and breastfeeding support to women. Thus, in this study, despite low postnatal newborn care, less than 50%, we report improvement compared to 3% from the NDHS 2013 and our baseline results.24,28
Another gap is that most providers do not empower and educate women on maternal and newborn danger signs and when to seek immediate care from the nearest health facility. Also, most women were not happy or satisfied with the family planning, breastfeeding, post-partum, and hygiene care information they received from the providers.
In Namibia, normal vaginal deliveries are discharged home within 48-72 hours, suggesting that most mothers go home uneducated on immediate care-seeking if a danger sign is present.24 Early discharge and counselling only a few women suggests that most women and neonates may go home with unidentified, unreported or undiagnosed danger signs or complications .24 Thus, depending on how far the mother lives from the nearest health facility and her level of education on danger signs, neonates can be at risk of preventable deaths resulting from late identification of the condition or delays in care seeking.24 Thus, if the quality of postnatal care services is not improved, it continues to increase maternal and newborn vulnerability in immediate afterbirth and early postnatal care.7–9,12,24 Training or refreshers with a strong focus on interpersonal communication skills, provider-client interactions and information sharing are likely to make a difference and result in low-cost, high-impact.24 We, therefore, submit that implementing the WHO/UNICEF/UNFPA maternal newborn care standards as a package will likely improve the quality-of-care immediate or early postnatal care. This submission is consistent with the findings from the study by Manu and co-authors,36 that a similar package is feasible in reducing mortality around childbirth.
Health system implications
The Lancet Global Health Commission asserts that “providing health services without guaranteeing a minimum level of quality is ineffective, wasteful, and unethical”.13(pe1198) In Namibia, the head of quality assurance also reiterated the wording of 'wasting resources…" if the country continues to record preventable mortalities. This statement was made during the scale-up of the maternal newborn quality improvement programme to the rest of the hospitals in December 2022. The first author’s advocacy to improve quality-of-care beyond the study site realized the design, implementation and scale-up. We thus commend the government or Ministry of Health Namibia for the bold decisions to improve maternal newborn quality of care within the maternity settings. The ministry of health, however, needs to allocate resources and improve or sustain high evidence-based care around childbirth and the immediate postnatal period when most mothers and neonates die.2,3,7–9,12 Without health system strengthening and prioritizing quality-of-care during labour, childbirth, and early postnatal period, facility births do not guarantee perinatal survival amidst suboptimal services.49
Measurement implications: Observation versus Exit Interview
According to Aujla et al50 although direct observation of patients is often considered ‘gold standard’ neither observation nor exit interviews is superior to another. During observation, the Hawthorne effect, which is behaviour change triggered by being observed, could lead to bias of the results in a positive direction than usual.50 Although improvement or positive change in provider’s behaviour is a good outcome, we submit that the observed level of change in behaviour post-intervention could be due to the Hawthorne effect. For example, post-intervention, more than half of providers gave feedback post-examination and reassured women to allay their fears. This behaviour was observed to be performed by none to very few providers at pre-intervention. While for similar measures, there was less than 10% change in behaviour reported during women’s exit interviews. During exit interviews, patients were more likely to recall what was done to them, counselling danger signs, information or advice given, and their experiences of disrespect or mistreatment.50 They would also recall the working diagnosis if shared with them.50 In this study, the reported provider’s behaviour by women and assessors on the same measures differs. Also, according to exit interviews and observations, providers communicating a delivery plan to women postintervention increased only by a small amount, 2% and 6%, respectively. The wording, which could influence these major or minor differences in exit and observation reports, is assessors’ level of probing,50 or biases. Thus, the results in Table 3 need to be interpreted with caution. We, however, submit that capturing women’s voices on their perception and experiences of care is key if the quality of care is to improve.38
Strengths and limitations: This study is not without limitations. We used the before-after study design with no control site. Implying that the results may not be due to the intervention but could also be impacted by external temporal trends. The observations of provider-client interactions may be subjected to the Hawthorne effect, resulting in providers altering their behaviour during care. To reduce observer and data collector biases, the data collectors were trained by the first author and the developer of the EMEN tool (UNICEF international consultant). Experiences from larger but similar studies conducted in Bangladesh, Ghana and Tanzania using the EMEN Tool informed the finalization of the questionnaires used and training content. During the training, the assessors demonstrated how to use the questionnaires by role-playing for quality assurance. During training, a field visit was held in a maternity ward to familiarize the assessors with the various areas of care, including identifying possible spots for the exit interviews. The data collection took three weeks. We submit that these actions could have reduced the provider’s changes in behaviours.
CONCLUSIONS
To our knowledge, this is the first study in Namibia to assess the quality-of-care implementation on admission, labour, childbirth, and immediate postnatal care. Provider’s inconsistency in implementing quality-of-care measures in four stages of childbirth resulted in most mothers and neonates receiving low or poor quality-of-care during the early postnatal period. When comparing before and after implementation of quality improvement interventions, many quality improvement interventions demonstrated the feasibility of potentially improving or increasing quality-of-care immediately after birth or during the postnatal care period. The trainings or refreshers of providers in postnatal care, interpersonal communication, and the importance of provider-client interactions are likely to have a significant and low-cost, high impact. Results from this study are being used to inform country scale-up of quality improvement interventions and can be used in similar resource settings. We have threefold recommendations. First, a further investigation to unpack the drivers for poor provider-client interactions and low quality-of-care practices for labour and postnatal care. Second, to reduce preventable newborn deaths, we recommend the health system to invest resources, including trainings on improving quality-of-care around childbirth and early postnatal period, a time when most babies and their mothers die. Third, the trainings/refreshers on the importance of educating mothers on danger signs, proper use, and timely documentation of vital signs to accompany the regular supplies of the partographs. We submit that regular supervision for improved childbirth and immediate postnatal care outcomes will likely improve labour monitoring.
Acknowledgements
The authors thank the Ministry of Health and Social Services officials at national, regional and facility levels for their input and support. The leadership of the national quality assurance/management unit and QI trainers is highly appreciated. Special gratitude to the facility management team, assistant data collectors, interviewed staff and maternal women at discharge for supporting the research. The authors also acknowledge the support from the UNICEF international consultant (AM) for inputs to the data collection tools before the final print and training of data collectors. Gratitude also goes to UNICEF HQ Health Advisor (TDH) and UNICEF ESAR Health Specialist (FG) for supporting overall the maternal and newborn Quality improvement agenda in Namibia.
Ethics statement
The Ethical Review Board of the national level Ministry of Health and Social Services (MoHSS), Namibia (Ref: 17/3/3) and the Biomedical Science Research Ethics Committee of the University of the Western Cape (Ref: BM17/10/4) approved to carry out the study in Namibia. Hospital management gave verbal consent to review records, conduct facility readiness, and interview staff and discharged women. Only participants who consented by signing consent forms after explaining the study’s purpose were interviewed.
Data availability
The original contributions presented in this study are included in the article/supplementary material; further inquiries can be directed to the corresponding author.
Funding
‘Conducted with support of Belgian Development Cooperation, through the Institute of Tropical Medicine Antwerp (Grant Ref: FA4 DGD-ITM 2017-2020)’, this PhD scholarship was awarded through UWC, School of Public Health to enable the first author to conduct a research study in the pursuit of a doctoral degree with UWC’. DJ was also supported by the London School of Hygiene and Tropical Medicine Takeda Chair in Global Child Health. The funders have no influence or involvement in this paper.
Authorship contributions
GMS was PI, and this work is part of her PhD. She performed data collection and analysis and worked closely with the Ministry of Health and local stakeholders. TM and DJ were co-investigators and supervisors for the research. All authors participated in the study’s conceptualization and approved the final manuscript.
Disclosure of interest
"The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Correspondence to:
Gloria Mutimbwa Siseho
University of the Western Cape, Faculty of Community and Health Sciences, School of Public Health, Bellville, Republic of South Africa
Email. [email protected] and/ or [email protected]