INTRODUCTION
Rationale
Percussive therapy (PT) was developed in the 1950’s by Robert Fulford through the introduction of the percussion vibrator which was applied to local areas of the body for deep tissue osteopathic treatment for musculoskeletal pain.1 The first commercial massage gun was invented in 2008 and in recent years, there has been an increase in popularity of handheld devices for personal and professional therapeutic use, as well as by strength and conditioning coaches and athletes to elicit potential performance gains.2 The use of massage gun technology, often referred to as PT, involves “floating” the device over the surface of the skin, applying vibration and rapid pulses in short bursts of pressure to the muscle belly or tendon.3,4 The application is comprised of a triad of characteristics; frequency (Hz), amplitude (mm) and torque (lbs),4 and mimics the therapeutic effects of tapotement massage therapy, where rhythmic percussive strokes are applied to the body with a cupped hand.5
The impact of vibration on physical performance parameters and experiences of pain has been extensively researched, using an array of devices. Vibration is delivered by mechanical vibration, where the energy is transferred from the device directly to the tendon or muscle6 or indirectly through the feet while standing on a platform or the hands by holding a device.7 These forms of delivery can include cycloidal vibration,8 oscillation vibration,9 local vibration therapy,10 whole body vibration therapy (WBV)11 and handheld vibrating equipment.12 Reviews to date have adopted an umbrella term of “vibration therapy” to encompass a range of devices and treatments.13 Vibration treatment has been found effective in promoting acute adaptations in pain reduction,14 increasing strength15 and improving flexibility16 after single and multiple treatments.
Despite this extensive literature there is a lack of specific research on PT delivered by massage guns and the effect on physiological adaptations. A systematic literature review was deemed appropriate to investigate research conducted on PT and the effects of PT interventions on performance in strength and conditioning settings and on experiences of musculoskeletal pain. Identifying the most effective PT protocols would allow researchers to develop targeted interventions to support physiological adaptations and reduce experiences of musculoskeletal pain.
For the purpose of this review the following definitions were applied:
-
Muscle strength – ability of a muscle or muscle group to exert force on an external resistance.17
-
Explosive muscle strength – ability of a muscle or muscle group to rapidly produce speed or large forces.18
-
Flexibility – ability of muscles and tendons to elongate around a joint.19
-
Musculoskeletal pain – unpleasant sensory experience associated with the bones, joints or tissues of the body.20
The purpose of this review was to determine the effect of PT delivered by massage guns on physiological adaptations: muscle strength, explosive muscle strength and flexibility, and experiences of musculoskeletal pain.
METHODS
Protocol and registration
The systematic literature review protocol21 was registered with Prospero. Registration number: CRD42021253767.
Eligibility Criteria
Databases were searched from January 2006 to capture any preliminary research prior to the introduction of PT massage guns in 2008, with a final search before completion of the study to include any recent articles. Table 1 details the full eligibility criteria.
The PICO criteria were used to frame the research questions and define the eligibility criteria:
-
Participants - adult populations aged 18 years and older.
-
Interventions - PT applied by massage guns directly to the muscle belly or tendon of the intended muscle for treatment in any location on the body.
-
Comparators – alternative, placebo or no treatment.
-
Outcomes - physiological adaptations: muscle strength, explosive muscle strength, flexibility or experiences of musculoskeletal pain. Measures of these outcomes included self-reported scores and units of measurement, such as degrees, distance and time.
Information sources
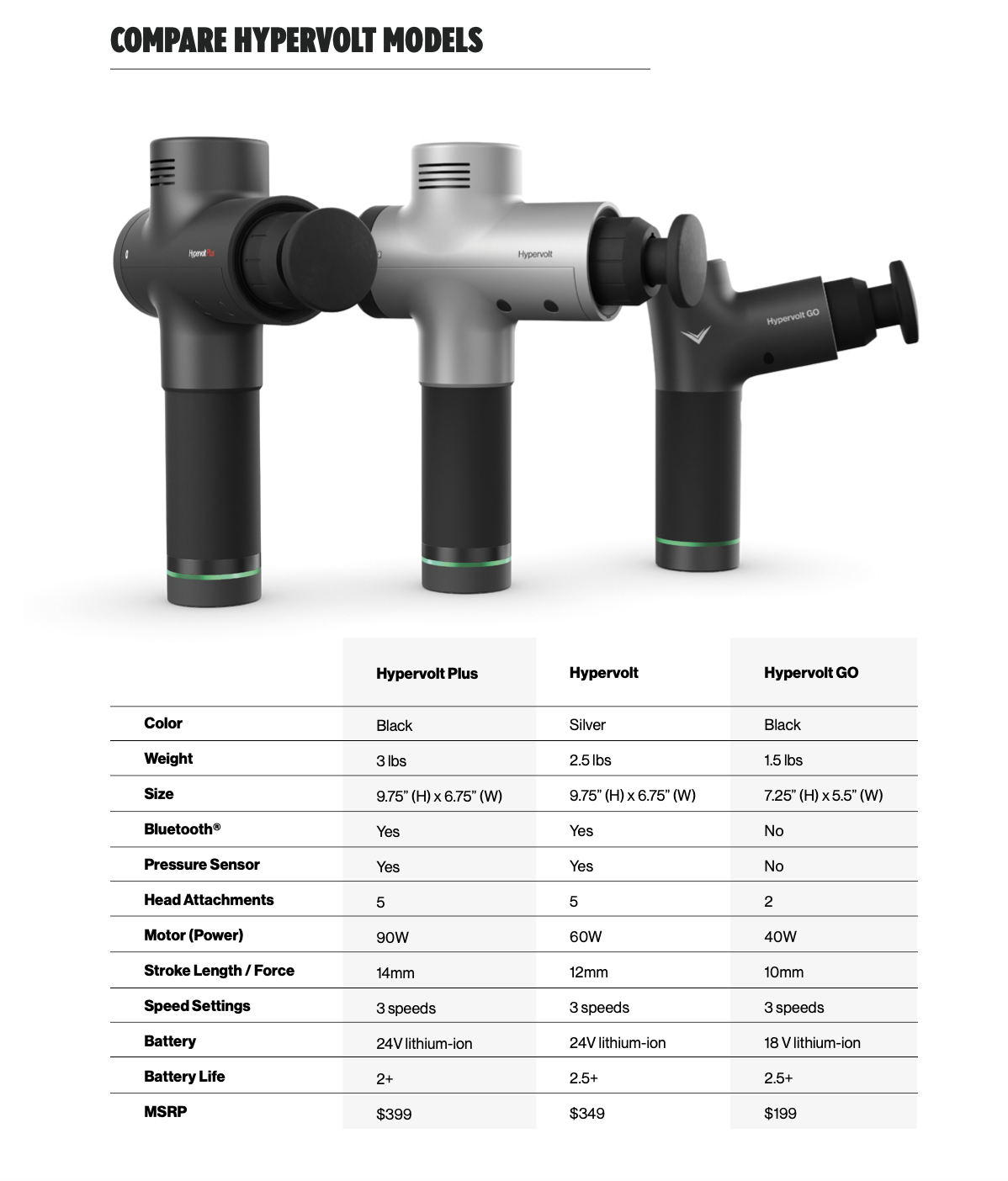
To provide a comprehensive overview, all existing literature was included, for example primary research studies, systematic reviews and conference papers, providing the full-text version of the articles were available. The search strategy was created in collaboration with all authors (Supplementary file 1). The following electronic databases were searched: PubMed, SportDISCUS, CINAHL, Cochrane Library and Psychinfo. Grey literature was searched for in Google, Google Scholar and OpenGrey using a combination of key words, massage gun, percussion therapy, percussive massage and percussive therapy. In addition, all sources were searched using the following brand names; Addsfit, Exogun, Fluxmassage, Hydragun, Hyperice, Hypervolt, Muscle Gun, Myopro, Physion®, Powerplate®, Recovapro, Therabody, Theragun and Timtam. Finally, reference lists of all relevant studies, reviews and reports were searched.
Study selection
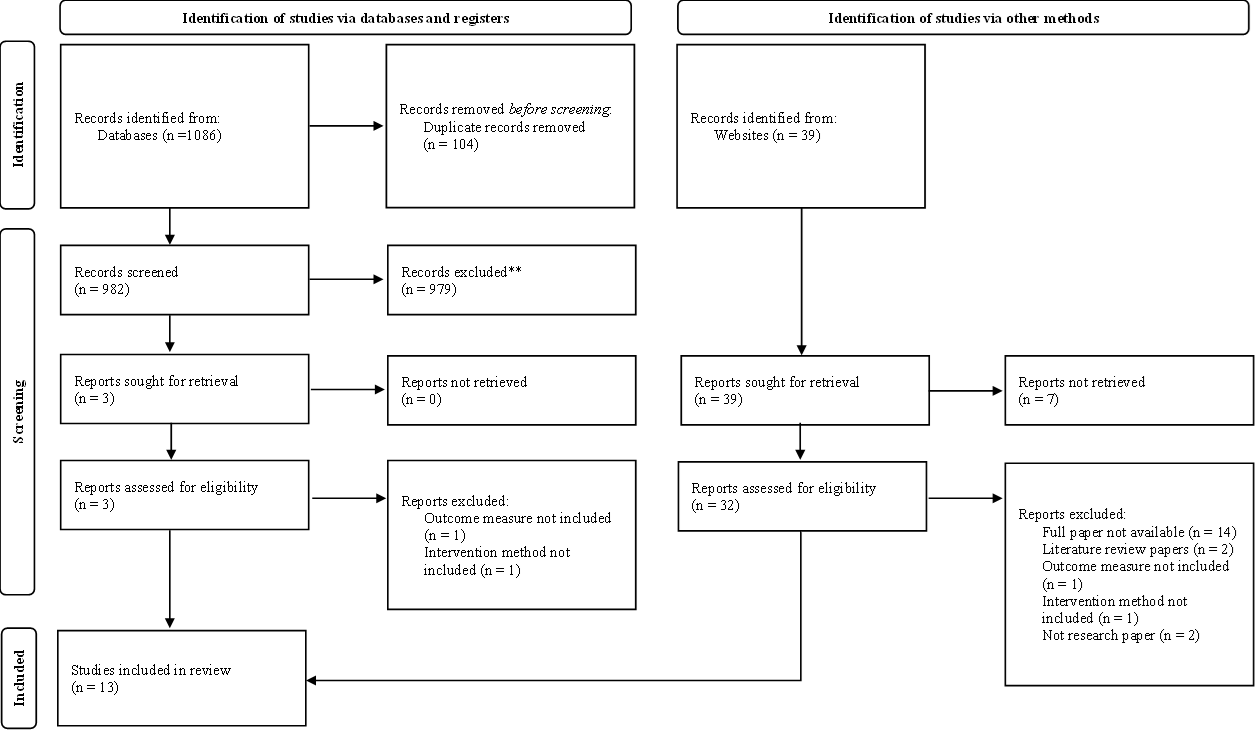
Study selection at title, abstract and full text screening was performed by one reviewer and checked for consistency and completeness by all reviewers. Any disagreements were resolved using Table 1 as a basis for discussion. After eliminating any duplicates, an initial screening of titles and abstracts excluded records that did not meet the inclusion criteria. Each record was classified as ‘include’, ‘exclude’ or ‘maybe’ to identify relevant and exclude irrelevant literature. The researcher was inclusive at this stage and, if uncertain about the relevance of a publication, it remained in. For records that potentially met the inclusion criteria, the full text was obtained and screened. Studies written in a foreign language were professionally translated into English and screened for eligibility. Seven papers required translation from Portuguese, Turkish, Korean, Indonesian, Czech and Spanish. Studies that did not meet the inclusion criteria were listed with the exclusion reason(s) (Supplementary file 2). Two attempts in one month were made to contact original authors to locate publicly unavailable full texts or obtain missing data. Any missing data was not inferred. A flowchart that documents the process outlined above can be found in Supplementary file 3.
Data extraction
Data for analysis was extracted from the included studies to assess that all relevant data was captured and that it could be reliably interpreted. Extracted data included participants, study design, interventions, comparators, outcomes, authors, year of study, aim/purpose, type of paper, geographical area, sample size, intervention length, treatment methods, measures of acute or chronic adaptations and key findings that related to the review questions. One reviewer extracted data which was checked for consistency and completeness by all other reviewers, with disagreements resolved by discussion.
Critical appraisal of individual sources of evidence
The included studies were evaluated using quality appraisal tools. The Mixed Methods Appraisal Tool (MMAT) Version 201822 and Critical Appraisal Skills Programme (CASP) tool23 were tested on two full papers. Both tools have been standardized and validated24,25 and are widely used for systematic review purposes. The CASP tool was selected due to its criteria providing the best cover of the methodologies used in the included studies.
Risk of bias in individual studies
One reviewer assessed the risk of bias and methodological quality using the Physiotherapy Evidence Database (PEDro) scale26 which was checked for consistency and completeness by all other reviewers. The PEDro scale awards points ranging from 0-10 and studies were deemed high risk of bias and low quality with a score of <3.27
Synthesis of results
Findings from the included studies were synthesised narratively with reference to the narrative synthesis guidance, in order to draw conclusions based on the body of evidence. This guidance focusses on synthesising findings from multiple studies which rely on the use of text to summarise and explain findings, and details specific tools and techniques that can be used in the synthesis,28 the purpose of which is to gain insight into the body of knowledge derived from the review.
RESULTS
Study selection
A preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow-chart of the study selection is shown in Figure 1.29

Study characteristics
Study characteristics are summarised in Table 2. A total of 255 adult participants were involved in the studies (n = 13), with at least 18.8% of these being female. There were five studies which involved mixed genders, one female case study, four studies focussing only on males and three studies not reporting participant genders.
Eleven studies considered the effect of PT delivered by massage guns on the lower body (n = 7) and the back (n = 4), with the remaining two focussing on the shoulders. Ten studies examined the effect of PT on flexibility, with five of these combining outcomes of pain, muscle strength and/or explosive muscle strength. The remaining three papers focussed solely on either explosive muscle strength or pain. Eleven studies included a control group using a range of comparators, such as no treatment, static stretching and foam rolling, and the final two were case studies. Nine of the studies involved one application of PT with treatment ranging from 30 s to 30 min, and four studies administered multiple treatments over a period of one to four weeks. Only one study reported on the effect of PT 24 h and 48 h post treatment, with the remaining studies assessing the acute effects. A variety of outcome measures and application protocols were used across the studies (Table 3), with twelve (92%) studies using a Theragun or Hypervolt massage gun.
Critical appraisal within sources of evidence
CASP tool quality data for the included studies is presented in Supplementary file 4. All studies had limitations in methodological quality or reporting of findings but still included contextually-rich details that contributed to the overall narrative synthesis and the research questions. Caution was therefore taken when drawing on these details. It was deemed in all studies that the benefits of the intervention outweighed any harms and financial costs, and results could be applied to local populations.
Risk of bias
The PEDro scale risk of bias analysis is presented in Supplementary file 5. PEDro scale scores of 0-3 are considered ‘poor’, 4-5 ‘fair’, 6-8 ‘good’, and 9-10 ‘excellent’.27 Total scores of included studies ranged between two and nine, with an average score of 5.92±2.1. It was not possible to distinguish between the methodological quality of the trials and the quality of reporting. No studies reported blinding of participants to the intervention they were receiving, or of the therapists to the intervention they were administering. Although blinding of participants and therapists can minimise bias, it is challenging to achieve as physical therapy cannot be masked in a way as, for example, pharmacological substances can.46 It is unclear in ten of the included papers if assessors were blinded when analyzing outcomes, risking potential bias to findings.47
SYNTHESIS OF RESULTS
This systematic review identified 13 studies addressing the effects of PT delivered by massage guns on the physiological adaptations of muscle strength, explosive muscle strength and flexibility, and on experiences of pain. Results of the individual studies are detailed in Table 2.
Effect on muscle strength
Two studies considered the effect of PT on muscle strength; lower body30 and shoulder,37 representing a minor proportion of the population, with a large variance in age, suggesting results may vary with a broader intervention and limiting a wider application of findings into practice.
Lower body
The application of PT had no influence on planter flexor strength immediately after a single treatment as tested using a dynamometer, but the effects of multiple treatments or other strength measures were not considered.30
Upper body
The case study focussing on shoulder strength following rotator cuff surgery indicated an increase in muscle strength for the participant who was eight months post-surgery.37 While case study designs are important, they limit the application of results to the wider population. However, results from this case study must be viewed with caution due to the limitation of strength being assessed by Manual Muscle Testing (MMT) which lacks inter and intra tester reproducibility owing to the subjective nature of the test.48
Effect on explosive muscle strength
Four studies considered the effect of PT on lower body explosive muscle strength.4,31,39,40
Outcome measures
According to studies which measured outcome data with tensiomyography (TMG)4,39 and jumping longitudinally40 there was evidence of improvements in explosive muscle strength. This is in contrast to Hernandez (2020) where PT, when added to a warm-up, had no impact on explosive muscle strength when assessed by counter-jump testing.31 However, this was the only study to report that participants were instructed to wear compressions shorts and no instructions were provided on jumping techniques or squat depth for the counter-jump, which may have impacted the results.
Combination of treatments
Piñero (2019) conducted the only study to involve combined treatments.40 Myofascial induction (i.e., mechanical stimuli such as pressure or stretching) was paired with PT and administered 15 days after the first treatment of massage and manual vibration. The results did not consider any long-term effect of the first treatment, and it was impossible to establish whether PT alone was responsible for the significant improvement in explosive muscle strength or the proportion attributable to the other treatments.40
Long term effect
In one study the largest increases in muscle contraction were measured in regular users of massage guns suggesting potential benefits of long-term use of PT, however, these results are limited by the omission of statistical data analysis.39 García-Sillero et al. (2021) re-examined the effect of PT both 24 h and 48 h after treatment, with the greatest changes reported in time of contraction (Tc) (i.e., the time between 10% and 90% of muscle contraction32) immediately following PT and after 24 h for radial displacement.4
Gender
Of the few studies including male and female participants, only Michal (2021) reported results separately.39 These results showed that PT had a greater effect on explosive muscle strength in women compared to men, with an average increase in the rate of change of contraction as measured by TMG of 4.47±11.67% and 3.64±4.53% respectively.
Effect on flexibility
Ten studies focussed on the effect of PT on flexibility, including the back,35,38,41 lower body3,30,31,33,40 and shoulder.36,37 Overall, results indicated an improvement in flexibility in all anatomical locations after PT.
Multiple treatments
There were three studies which considered multiple treatments of PT.33,35,37 Kayoda (2019) highlighted the potential positive effect of long-term use of PT on shoulder flexibility over four weeks, but did not report statistical analysis.37 The remaining studies investigated the impact of PT on flexibility of the trapezius after two weeks of treatment35 and hamstrings after one week.33 All protocols applied a consistent frequency, with the exception of Seju and Rajput (2021), where the frequency set on the massage gun was gradually increased over the period of the intervention35 (Table 2).
Single treatment
There were two other studies which reported on back flexibility; thoracolumbar41 and lumbar,38 and one focusing on the shoulder,36 with all three reporting significant improvements after one application of PT. However, one study used Vaseline when applying PT which may have influenced the positive results observed on thoracolumbar flexibility.41 Vaseline is a lubricant which would have enabled the PT gun to glide more easily over the skin but could have impacted body mechanics by applying too much pressure to the targeted muscle.49 Further analysis of the study by Godemeche (2020) suggested that PT promoted greater results in lumbar flexibility only in the very active participants, after increasing the intensity on the massage gun over 16 min of treatment.38 The effect of PT on the calf muscle was considered by three studies3,30,44 with a further study focusing on hamstrings.40 Significant acute improvements in flexibility were reported in all studies after one application of PT, despite the variation in measures used to assess outcome data, brand of massage gun, frequency protocol, amplitude and head attachment. Despite these positive findings, there was also evidence to suggest that the alternative method of static stretching was as effective as a single treatment of PT for increasing flexibility.3
Effect on experiences of pain
Considerations of the effect of PT on experiences of pain were made by four studies, which involved the back,34,35 shoulder37 and lower body.40 All the included studies used validated measures of pain; numeric pain rating scale (NPRS), visual analogue scale (VAS)50 and Oswestry Low Back Pain Disability Questionnaire.51
Single treatment
Piñero (2019) examined the effect of PT on pain experienced hamstrings after one application and reported a reduction in experiences of pain.40 However, the study did not report on the cause of pain and results did not consider any long-term effect of the first treatment administered 15 days prior to PT, making it impossible to establish whether PT alone was responsible for the reduction in pain, or the proportion attributable to the other treatments.
Multiple treatments
Two studies investigated experiences of back pain and involved PT five times per week for three weeks34 or three times per week for two weeks35 with a gradual increase in frequency set on the massage gun (Table 2). The significant positive results of these studies suggest benefits of long-term PT use, with the potential to explore increasing the intensity of treatment. Mansuri and Patel (2021) also included a further intervention of ergonomic advice, making it difficult to determine the extent of the positive effect of PT alone.34 This study focussed on bus drivers so there is no evidence to suggest the results would be transferable to other populations. Koyada (2019) investigated the effects on shoulder pain by applying PT twice per week for four weeks, reporting an increase in flexibility.37 However, the participant also took cannabidiol (CBD) oil for the first week of the trial which may have influenced the results, as CBD oil has been used to manage pain.52
Comparison to alternative, placebo or no treatment
Overall, there were greater positive results from PT interventions when compared to placebo protocols, no treatment, or alternative treatments, suggesting a superior effectiveness of PT against treatments such as sports massage, WBV and foam rolling.
No treatment
Six studies reported statistically significant increases in muscle strength, explosive muscle strength, and flexibility after PT when compared with no treatment.4,30,31,34–36 A further two studies did not report statistics, but PT demonstrated an increase in the outcomes of muscle strength, perceptions of pain and flexibility.33,37
Alternative treatment
A further five studies compared PT against an alternative treatment (see Table 2) and demonstrated statistically significant increases in explosive muscle strength, flexibility and perceptions of pain after PT.4,35,38,40,41 One study reported a statistically significant increase in flexibility from pre to post PT intervention, with the result being comparable with the alternative treatment of static stretching.3 Michal (2021) did not report statistical results, but the PT intervention demonstrated a greater increase in pre to post explosive muscle strength compared to the alternative treatment of sports massage.39
Placebo
Finally, one study reported no improvement in flexibility after the placebo treatment of ultrasound, compared to a statistically significant improvement after PT.38 However, it was not evident if the de-activated ultrasound device touched the skin or hovered over, and whether this may have promoted a physiological response.46
Methodological characteristics
An issue found throughout the literature was the variety of methods used to record the outcome measures. These included dynamometer and manual muscle test for muscle strength, counter jump and TMG for explosive muscle strength, dynamometer and lunge test for flexibility, and NPRS and VAS for experiences of musculoskeletal pain (Table 2). Further heterogeneity was evident in the specification set on the PT massage guns and Table 3 summarises the comparison between protocols used across the 13 included studies. This variety of methods makes it difficult to draw overall conclusions on the studies included and future research should consider developing a standardised protocol.
DISCUSSION
Summary of evidence
Muscle strength
Although only represented by limited number of studies, this review found there was a positive effect of PT on upper body muscle strength,37 with no changes observed in the lower body.30 It should be recognised that this evidence for the positive impact on muscle strength is limited as it is based on a single case-study that utilized a subjective method of strength assessment (MMT), thus questioning the reliability and validity of the results. However, comparisons can be made to a systematic review by Alghadir et al. (2018) which considered the effect of localized vibration on muscle strength. The types of vibration included in the review varied and included, for example, a percussion hammer, electric-powered dumbbell and vibrating cable. While 82% of the included studies found a significant improvement in upper and lower body strength, it was noted there was a lack of robustness and consistency in methodology, thus hindering the recommendation for an effective protocol.15 This is consistent with findings in this current review. It should be considered that a review of the application of vibration in sport suggested that a duration of 6 - 30 minutes could lead to a decrease in muscle strength.53 Furthermore, a study that considered the effect of vibration on peak torque of the quadriceps 300 days after anterior cruciate ligament (ACL) reconstruction surgery supported the positive results of vibration treatment. There was a statistically significant difference in peak torque between the treated group and the control group, with results indicating an almost complete recovery following vibration treatment.54
Explosive muscle strength
The results of the current review concluded that PT can promote an increase in explosive muscle strength4,31,39,40 supporting the narrative review by Germann et al. (2018) on the effect of local vibration on various outcomes, such as muscle strength, power and flexibility.13 Overall, the 21 studies reported that local vibration elicits beneficial changes in the outcomes being measured. The term “local vibration” encompassed a wide range of devices such as WBV, vibrating cables and devices strapped over the muscle, resulting in an array of vibration protocols and adding to the uncertainty about the most effective treatment.13
In contrast, the results of this current review on the positive effect of PT on explosive muscle strength contradicts research which investigated the effect of tapotement on ankle flexibility and explosive power.55 It is deemed that PT delivered by massage guns mimics the therapeutic effects of tapotement massage therapy5 and Mckechnie et al. (2007) reported results which indicated an increase in flexibility, but no change in explosive power.55 This is further supported by recent studies investigating the impact of PT on vertical jump height which concluded there was no acute effect on explosive muscle strength after two minutes56 or five minutes57 of treatment.
Flexibility
Multiple studies included in this review reported an increase in flexibility after PT.3,30,31,33,35–38,40,41 However, there was no significant difference in improvements in flexibility observed after PT, when compared to traditional static stretching.3 This indicates that the impact of PT may not be particularly novel in this outcome. There is conflicting evidence of the effect of PT on flexibility of the lower body, with some studies reporting positive effects58,59 and other investigations observing no significant adaptation.60,61 The positive results are supported the meta-analysis by Osawa and Oguma (2013) which investigated the acute and chronic effects of vibration on flexibility. Conclusions were similar to this current review, in that positive associations were recorded following vibration treatment. The review included 19 articles involving a combination of WBV, cycloid vibration and specifically made equipment. Again, there was diversity in the vibration device settings which prevents identification of the most effective protocol for promoting flexibility adaptations.16 A review of the application of vibration in sport suggested a duration of four minutes could elicit increases in flexibility53 and the results of the meta-analysis by Osawa and Oguma (2013) are further supported by a recent study which suggested that vibration foam rolling, with the intensity of vibration set at a frequency of 48 Hz, significantly increased flexibility without compromising muscle strength or performance.62
Experiences of pain
This current review indicates that multiple treatments of PT could reduce experiences of musculoskeletal pain.34,35,37,40 This was also evident from a recent meta-analysis and systematic review which focussed on the benefits of vibration on delayed-onset of muscle soreness (DOMS).14 Ten studies were included in the review which measured changes using the VAS after a variety of vibration interventions, such as WBV, cycloid vibration and sonic vibration. Results indicated that vibration reduced DOMS at 24 h, 48 h and 72 h, with the suggestion that the greatest effect was evident after 48 h. A number of exercises were used to elicit DOMS, such as downhill walking and strength training which contributed to the heterogeneity between studies, along with the variety in application protocols. This result is further supported by research which concluded that PT was effective in acutely reducing lower body pain resulting from DOMS.61,63
Pain vs flexibility
Studies in this review reported that reductions in experiences of musculoskeletal pain also demonstrated improvements in flexibility.35,37,40 It is worth considering if improvements in flexibility in response to PT play a significant role in pain reduction. Data from previous studies have indicated a relationship between stretching-based programmes and reduced hamstring,64 low back,65 quadriceps and anterior knee pain.66 Interestingly, the Patel and Patel (2020) hamstring flexibility study, also considered changes in experiences of lumbar pain following the same treatment applied to hamstrings. Pain, measured using the NPRS, indicated a reduction in pre (score = 8) to post treatment (score = 2) suggesting that PT had a positive effect on experiences of back pain, and highlighting possible advantages of indirect treatment.
Gate control theory of pain
When PT is applied to the muscle belly or tendon it activates the muscle fibres67 and induces a tonic vibration reflex, which involves the sustained contraction of the vibrated muscle and relaxation of its antagonist.68,69 This stimulation further promotes excitability in the muscle spindles afferent nerve fibres70 and these impulses are transmitted to the spinal cord and are believed to trigger an analgesic effect, as suggested by the gate control theory of pain. This theory suggests vibration causes a more closed position of the ‘gate’, thereby reducing the sensation of pain.71
Metabolic changes from percussive therapy
Research suggests that exposure to vibration or PT promotes an increased metabolic activity occurring within the muscles, including increased blood flow,72 oxygen saturation73 and temperature.74 These acute physiological responses may be contributing to the positive muscle strength and explosive muscle strength results seen in this review.
LIMITATIONS
The methodological characteristics of included studies were heterogenetic in the variety of methods used to record the outcome measures and the specific vibration parameters. This makes it inappropriate to compare the results of the included studies and draw conclusions concerning the most reliable and effective protocol. As 62.4% of participants across the studies were healthy active young adults, with another 30.2% experiencing pain, the effect of PT on the specified outcomes appears to be most advantageous for these populations and may not be generalisable to other groups. There were a number of studies identified by the search criteria which were published only as conference papers, which did not have full papers available, and these were excluded.
There are also number of strengths we would like to highlight:
-
PRISMA guidelines were followed, and stringent inclusion and exclusion criteria were adhered to in the selection of the review articles ensuring transparency and robustness throughout.
-
The review used broad inclusion criteria for the paper type (e.g. primary studies, conference presentations, Doctoral theses) resulting in an extensive literature search, enabling literature to be included that would otherwise be missed.
-
Some articles were professionally translated from different languages (Portuguese, Turkish, Korean, Indonesian, Czech and Spanish) as it was deemed important to include these studies as they provided information in line with the research questions of this paper.
CONCLUSION
The results of this systematic literature review infer that PT, delivered by massage guns, can promote an acute response in muscle strength, explosive muscle strength, flexibility, and experiences of pain, when compared to alternative, placebo or no treatment. The evidence suggests that PT has an acute effect on improving musculoskeletal performance with a single application, whereas multiple treatments are required to reduce experiences of back and shoulder pain. In addition, there is an under representation of females in sports science and sports therapy research75,76 and future studies should look to establish any differences between genders or just the impact of PT on females as a cohort, to achieve an equal knowledge about female participants. Further research should establish a standard, validated treatment protocol to allow analysis across populations and those with specific performance needs or pain, as well as considering the chronic effects of PT and the impact of multiple treatments.
Conflicts of interest
The authors have no conflicts of interest.
{kind=link}