INTRODUCTION
The deadlift is a strength training exercise targeting hip, thigh, grip, and lower back strength. It is also one of three competitive lifts in the sport of powerlifting. In addition to being a fundamental exercise among powerlifters,1,2 the deadlift, and variations thereof, is also practised by weightlifters,3 strongman competitors,4 CrossFit athletes,5 and bodybuilders6 to increase strength and stimulate hypertrophy. In addition, the deadlift has been used as a rehabilitation exercise for patients with low back pain.7 However, it was recently shown that onset of injuries in the low back region among Swedish sub-elite powerlifters was significantly associated with performing the deadlift in training.8 Further, although male and female powerlifters reported similar injury frequencies, there were significant differences of their anatomic locations, whereas males had a higher frequency of low back pain and females thoracic and neck pain.8
Deadlift technique is considered to be associated with both performance and risk of injury.9 Regarding the spine, it has been suggested that a lifting technique that enables the lifter to maintain a neutral position of the spine ensures optimal loading on both passive and active structures.10,11 For most people, a neutral position of the spine is when the lumbar spine has a slight concave curve (lordotic), the thoracic spine a slight convex (kyphotic) curve and the cervical spine a slight concave curve.12 In the scientific literature, neutral position has been defined as the region in the joint motion where there is little or no resistance to motion, i.e. a mid-range position (neutral position).13,14 It has also been described that in this region, spinal muscles operate with a complex strategy to control motions15 and that forces exerted on body structures vary depending on the ability to maintain a neutral position of the lumbar spine.16–18 This could be of clinical importance since for example when the lumbar spine is fully flexed, the longissimus/iliocostalis muscle complex have been proposed to have a reduced ability to produce posterior shear, which results in higher loads on the posterior passive tissues and high shearing forces.19,20
It has been shown that lifting technique, and thereby lifting mechanics when performing the deadlift, may differ between individuals.21 For example, it has been shown that high-skilled lifters are better able to keep the bar closer to the body than low-skilled lifters.21 The purpose of this study was to quantify the spinal alignment in the upper (thoracolumbar, T11-L2) and lower (lumbopelvic, L2-S2) lumbar spine during the deadlift exercise in male and female lifters. Secondary aims were to compare lumbar spine alignment during the deadlift to standing habitual posture, and determine whether male and female lifters differ in these aspects. The authors hypothesised that the lumbar spinal alignment during standing habitual posture would differ from the alignment during the deadlift exercise and that there would be a difference in lumbar spinal alignment between men and women during the the deadlift. The latter hypothesis was based on the results from a study by McKean et al.,22 which showed that men had a significantly larger range of lumbar flexion during the descent phase of the back squat exercise compared to women. Possibly due to differences in pelvic dimensions,23 lumbar vertebrae sizes,24 and trunk geometry,25 that together may influence lifting mechanics.
METHODS
Experimental Approach to the Problem
Using an observational, comparative study design, this study sought to describe and compare lumbar spine alignment in men and women competitive lifters during standing habitual posture, and whether the spinal alignment changed during execution of the deadlift. Spinal alignment was measured in all three planes of movement using inertial measurement units (IMUs), for the upper lumbar spine (i.e. thoracolumbar) and lower lumbar spine (i.e. lumbopelvic). After a warm-up, spinal alignment was measured in standing habitual posture and during the execution of one set of three deadlift repetitions when lifting 70% of self-estimated 1RM. The reasons for choosing IMUs for monitoring of the spinal movements during the execution of deadlifts were that they can easily be used outside of a movement lab and also show adequate validity of measures of spinal movement compared to 3D motion capture systems.26–28
Participants
Fourteen men and 10 women power- and weightlifters were recruited from local power- and weightlifting clubs. Only lifters with the intent of competing in power- or weightlifting and with at least two years of strength training experience were included. These criteria aimed to minimize variability in movement patterns between repetitions and to ensure that all lifters were familiar with performing heavy deadlifts. Lifters reporting a current injury which may have affected their lifting ability were excluded. Additionally, lifters less than 150 cm in height were excluded because of the risk that the IMUs would contact each other during movements. All lifters completed a questionnaire detailing training and medical history to ensure eligibility criteria was complied with. None of the invited lifters had any recent or previous medical issues which prevented them from participating in the study. Written informed consent was obtained from all lifters prior to participation and the study was approved by the Regional Ethical Review Board of Umeå, Sweden (Dnr 2014-285-3M).
Procedures
Warm-up: Lifters completed a self-administred warm-up with the intention to be prepared for heavy deadlifts. The warm-up typically consisted of sub-maximal deadlifts with increasing loads. Thereafter, three calibrated IMUs were affixed to the lifter’s back. They were placed at the spinous processes of T11 and L2, and on the sacrum (S2). Finally, the lifter completed one further set of bodyweight squats and deadlifts while it was ensured that the IMUs were set firmly and did not hinder the deadlift execution.
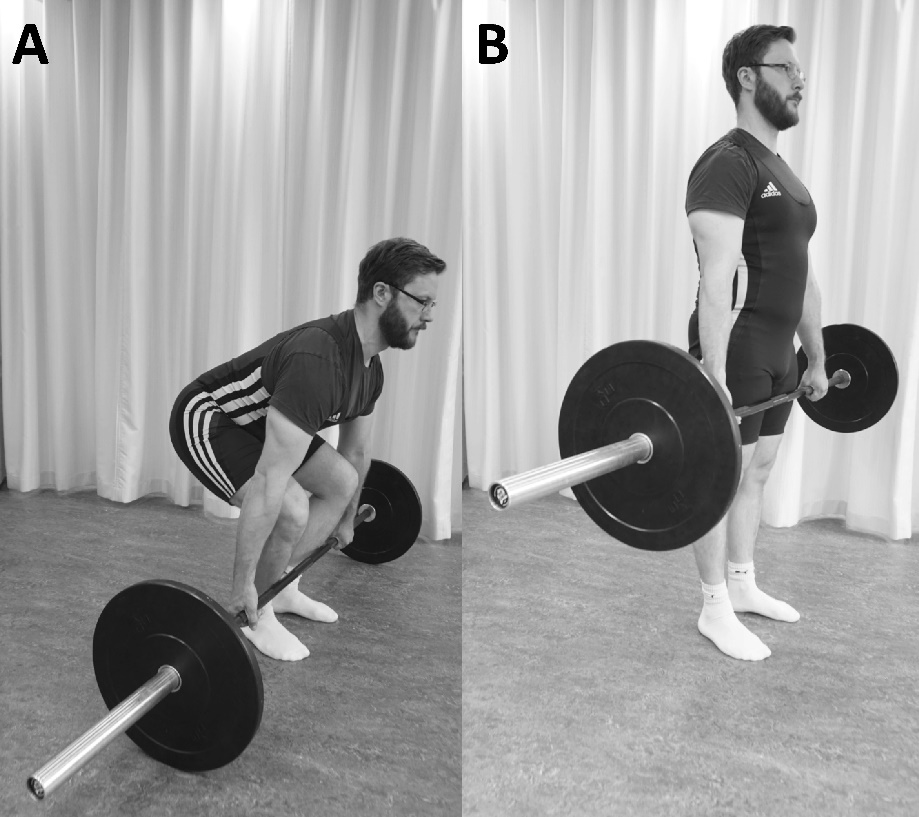
Data collection: First, the lifters were instructed to assume their habitual posture in standing with their arms at their sides while looking straight ahead (habitual posture). The IMUs then recorded their respective position to provide a measure of spinal alignment. The lifters were asked to perform one set of three deadlift repetitions at 70% of their self-estimated 1RM. In the start position of the deadlift, lifters stood with flexed knees and hips, straight arms, and held the barbell with an optional grip, i.e. a double pronated or mixed grip with one hand pronated and the other supinated (start position). In accordance with the rules of the International Powerlifting Federation,29 the barbell was then lifted by extension of the knees and hips until the lifter was standing erect (stop position) (Figure 1).

When the barbell was held motionless and standing erect with the hip and knees extended and the shoulders back the lifter was given a down signal and the barbell was lowered to the ground before the lifter released the grip. The lifter was instructed to stand erect momentarily before beginning with the next repetition. In the present study, only conventional style deadlifts were allowed so that the measurements would be uniform. No additional equipment (e.g., liftings straps, knee wraps, lifting belts) was allowed.
Instruments and Measurements
For the purpose of this study, the measurement of spinal movements were divided in to two movement segments, hereby refered to as upper lumbar spine (i.e. thoracolumbar spine) and lower lumbar spine (i.e. lumbopelvic spine). The IMUs placed on T11 and L2 measured their respective position (angle) relative to each other in all planes of movement for the upper lumbar spine. For the lower lumbar spine, the IMUs placed on L2 and S2 measured their respective position (angle) relative to each other in all planes of movement. A positive angle in the sagittal plane indicated a lordotic spinal alignment and negative sagittal plane value indicated a kyphotic spinal alignment. A positive value in the frontal and transverse plane indicated a right lateral flexion or rotation, respectively.
The spinal alignment [degrees] was measured during habitual posture in standing and during execution of the deadlift exercise. The following measurements were selected to quantify the spinal alignment in the upper lumbar spine (thoracolumbar, T11-L2) and lower lumbar spine (lumbopelvic, L2-S2), respectively: 1) habitual posture in standing, 2) start position, 3) stop position, 4) Min angle (the minimum angle in degrees captured during the deadlift exercise in each respective movement plane), 5) Max angle (the maximum angle in degrees captured during the deadlift exercise in each respective movement plane), and 6) range of motion (ROM) between the minimum and maximum angles during the deadlift exercise.
The IMUs (MPU-9150, InvenSense, San Jose, USA) each have a size of Length 60 x Width 45 x Height 10 mm and weigh 14 g, and communicate with a laptop via WiFi.30 The sampling frequency was 100 Hz with a 16-bit resolution and an anti-aliasing low pass filter set at 50 Hz. The full-scale range was ±1000 °/s for the gyroscopes, ±8 g for the accelerometers and ±4800 µT for the magnetometers. Using three axis gyros and three axis accelerometer, the IMUs detected the spinal alignment in all three planes of movement and real-time orientation was calculated using a customised system MoLab™ POSE (AnyMo AB, Umeå, Sweden). The placements of the IMUs made it possible to measure movement patterns previously stated important to the performance and risk of injury when squatting, i.e. flexion of the thoracolumbar and lumbopelvic spine.9 The anatomical location sites of the units were palpated by the same experienced person at each time with the lifters standing erect. IMUs were mounted with double-sided tape and elastic self-adhesive bandage wraps. Further, the deadlift execution was recorded with a web camera to facilitate the determination of start and stop of the squat repetitions when processing the data. Weight plates of official measures were attached to each end of a powerlifting barbell and the weight was adjusted to the nearest 2.5 kg.
Orientation data (i.e. segment angles) from the IMUs were processed in Matlab (version 7.10.0 (R2010a), The MathWorks, Inc., USA). The Euler sequence used for the segment angles were X (rotations in the sagittal plane), Y (rotations in the frontal plane), and Z (rotations in the transverse plane). All orientation data was low-pass filtered with a second order Butterworth filter at a cut-off frequency of 10 Hz. A more detailed description of the used algorithms can be found in Öhberg et al.30
Statistical analyses
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) version 23 (IBM Corp., Armonk, NY, USA). A factorial repeated measures analysis of variance (mixed ANOVA) was conducted to compare the influence of the independent variables (group: 1=men and 2=women) and the effect of the dependent variable (segment angle at five different positions: 1=habitual posture, 2=start position, 3=stop position, 4=minimum angle at any timepoint, and 5=maximum angle at any timepoint) using the mean values for the three repetitions. Sphericity was calculated using Mauchly’s test of Sphericity. If sphericity was was not assumed, a correction was made using the Greenhouse-Geisser estimation. If significant position x group effects were found, the results were also presented separately for men and women. If significant within-subjects effects were found, post-hoc pairwise comparisons were calculated. Effect size was calculated with partial eta squared (η2p) using 0.01, 0.06 and 0.14 to denote small, medium and large effects respectively.31 Significance level was set at 0.05 and Bonferroni corrections were performed for multiple comparisons.
RESULTS
Background characteristics for the participants are summarized in table 1, including their Wilks score in deadlift, i.e. a body mass adjusted measure of strength.32
The spinal alignment of the upper lumbar spine during standing habitual posture, and during the deadlifts for the start position, stop position, minimum and maximum angle, and range of motion are presented in Table 2. For the upper lumbar spine, there were no statistically significant differences between men and women in spinal alignment (group x position interaction in the sagittal plane (F(2.0, 43.3) = 1.9, p = 0.156), frontal plane (F(1.6, 34.9) = 0.9, p = 0.386), or transverse plane (F(2.7, 59.9) = 0.9, p = 0.451)). In all participants their alignment in standing habitual posture differed from the alignment at the start position and further spinal adjustments were made during the deadlift (significant main effect for position in the sagittal plane (F(2.0, 43.3) = 45.8, p < 0.001, η2p = 0.676), frontal plane (F(1.6, 34.9) = 15.6, p < 0.001, η2p = 0.414), and transverse plane (F(2.7, 59.9) = 23.9, p < 0.001, η2p = 0.521).
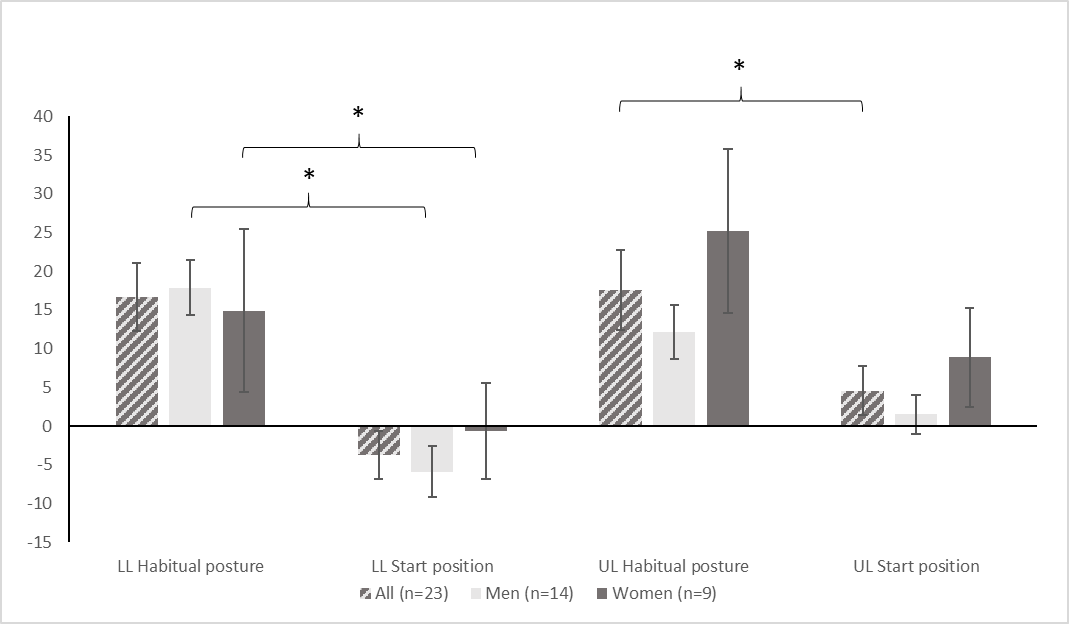
For the lower lumbar spine (Table 3), the decreased lumbar lordosis during the start position compared to during standing habitual posture was significantly greater among men than women (group x position interaction in sagittal plane spinal alignment (F(1.9, 41.9) = 4.0, p = 0.028, η2p = 0.154). There were no statistically significant differences between men and women in spinal alignment in the frontal plane (group x position interaction) (F(1.8, 39.9) = 0.3, p = 0.757) or in the transverse plane (F(2.1, 45.5) = 1.0, p = 0.156). In all participants their alignment in standing habitual posture differed from the alignment at the start position and further spinal adjustments were made during the deadlift (significant main effect for position in the frontal plane) (F(1.8, 39.9) = 9.2, p = 0.001, η2p = 0.294) and transverse plane (F(2.1, 45.5) = 15.2, p < 0.001, η2p = 0.676).
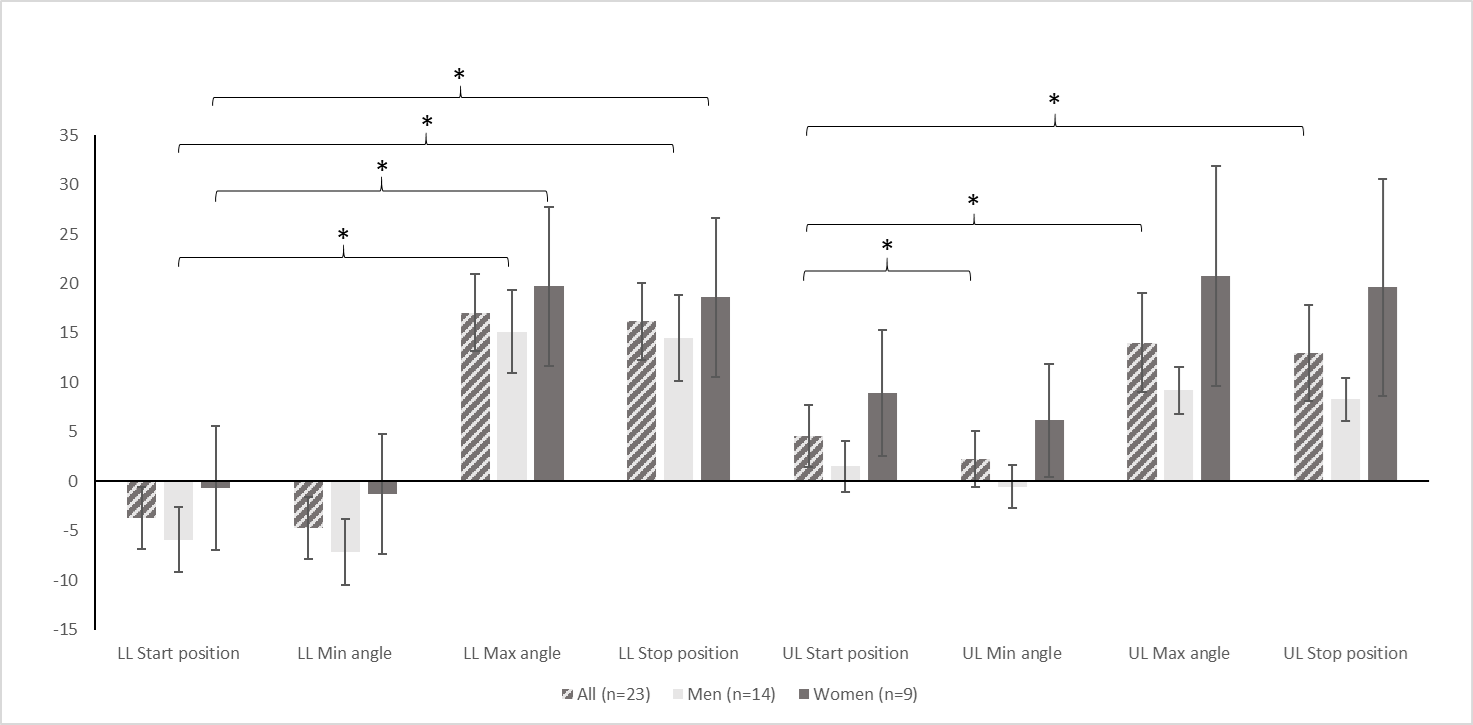
The factorial repeated measures ANOVA simple effects for position in the upper and lower lumbar sagittal plane spinal alignment are presented in Figures 2 and 3.


DISCUSSION AND IMPLICATIONS
This is the first study to describe and compare spinal alignment, in all planes of movement, during the deadlift exercise in both men and women. The results show that the lifters’ lumbar spinal alignment in standing habitual posture differed from the alignment at the start position of the deadlift, and that further spinal adjustments were made during the deadlift. As shown by the measures of range of motion, neither men nor women kept their spine in a fixed position when performing a heavy deadlift. Specifically, spinal adjustments were made mainly in the sagittal plane, a phenomenon that has also been reported for the squat exercise.22
The results showed no differences between men and women although this was initially hypothesized. In regard to the potential impact of differences in anthropometric factors it is not possible to draw any firm conclusions since these were not measured specifically. However, the results could indicate that potential anthropometric differences between men and women do not affect range of motion of the spine during deadlifts, as opposed to the findings by McKean et al.22 in regards to back squats. Also, regarding the previously observed difference in pain locations,8 thoracic and neck regions for women and low back region for men, the results do not present any evidence that movement pattern of the spine could explain those findings.
An inability to maintain the spinal curvature in its neutral position has been proposed to increase the strain on passive structures of the back.17,21,33,34 This belief is based on the fact that the spine is better at managing compressive rather than shearing forces, meaning that an upright posture with all vertebrae aligned in a neutral posture is preferable.16 Performing the deadlift with the lumbar spine in its fully flexed position, in conjunction with a heavy load, is believed to be injurious to both active and passive structures.33 Previous epidemiological research has found that training of the deadlift exercise might be associated with low back pain in powerlifters,8 although there is only a limited amount of research reporting the occurrence of specific injuries.35 Still, experts in the field of powerlifting have agreed that flexing (rounding), twisting, side bending or hyperextending the low back during deadlifting is a risk factor for low back pain.9 Whether lifters adopting any of these adjustments in spinal alignment are in fact more injury-prone remains to be studied. Specifically, there is no in vivo evidence of a causative correlation between spinal alignment and low back pain/injuries.35 When it comes to deadlifting with heavy loads, some have argued that it is extremely difficult or almost impossible to maintain a neutral spinal curvature.11 This might be explained by an increase in strength in the deadlift while lifting with a flexed back due to an increase of the effectiveness of the back extensors36 and shortening of the external moment arm. Also, it is very likely that the back could flex due to several other factors, e.g. the back or hip extensors inability to produce enough torque to withstand the external torque imposed on them, the coordination between back and hip extensors or insufficient range of motion in the hip, knee or ankle joints leading to compensatory movements in the low back. It has also been suggested that the adjustment of the spinal curve during lifting tasks is the human body’s way of managing the additional load by trying to keep the combined body and barbell center of mass vertically in line with the center of gravity.22,37 In addition, previous authors have shown that the deadlift exercise entails lumbopelvic movement in all planes38 and that visual observation of these movements are very difficult to accurately observe.39 These results are be supported by the results of the present study, especially with the small movements detected in the frontal and transverse planes in mind. Therefore, there may be a need to study movement patterns in the deadlift with a range of loads and with more attention to the magnitude of movement in relation to individuals maximum range of motion and less attention to exclusively noting presence of lumbopelvic movement.
For the standing habitual posture, the mean lordosis was 18° in the upper and 17° in the lower lumbar spine. In an earlier study using an inclinometer, the lumbar lordosis of an unloaded lumbar spine of a standing person was shown to be about 25° and the normal ROM for flexion from this point is about 50°.40 Beforehand it was hypothesized that lumbar spinal alignment during standing habitual posture would differ from lumbar alignment during the deadlift exercise. This was confirmed. In the start position, the lumbar lordosis decreased to five degrees in the upper and into slight flexion (-4°) in the lower lumbar spine. However, during the lift the lifters returned to a more lordotic alignment although it was still significantly less lordotic in the stop position compared to the standing habitual posture in the upper lumbar spine. Regarding the lower lumbar spine, all lifters flexed this area especially during the first part of the lift. After the first part of the lift, the lifters returned to an alignment that was similar to the standing Habitual posture. However, in relation to previously described41 average maximal ranges of motion, no participant achieved such ranges. The movement pattern of a flexed lumbar spine during execution of heavy deadlifts has also been shown in an earlier study examining the lumbar spine using fluoroscopy.18 In that study, one of the lifters reported lower back discomfort when the L4/L5 joint exceeded the passive full flexion and the posterior ligaments were fully stretched. However, the authors stated that the extensor moment supported by the ligaments was unlikely to threat the ligamentous tissue in a healthy intervertebral joint, even though it produced momentary discomfort.18 The finding that men flexed their back more than women in the start position has not been presented earlier. However, differences in movement patterns between men and women have been reported in the squat exercise22 and for lifting tasks.42 While the reason for the differences in spinal movement pattern between sexes during the execution of heavy deadlifts is unknown, the influence of sex on movement pattern has been attributed to anatomical differences.22 However, a study by Keogh et al.43 revealed that for powerlifters in New Zealand both men and women seem to have similar anthropometric characteristics in regard to skeletal features like bone lengths and breadths. Another inherent difference could be the structure of the hip joint, whereby men tend to have lesser hip ROM than females and therefore may need to flex their lumbar spine more in order to reach the bar.
Regarding the frontal and transverse spinal alignment, significant differences were found in both the upper and lower lumbar spine during the deadlift when compared to the standing habitual posture. Even though these differences were significant, it could be questioned whether they are clinically relevant since the absolute change was less than 5 degrees. The reason for the adjustments in spinal alignment could be how the lifters gripped the barbell. While some of the lifters gripped the barbell with a double pronated grip, others used a mixed grip with one hand pronated and the other supinated. The alternated grip is thought to induce a hip rotation44 and hence could explain the transverse plane movements. Movements in the frontal plane during deadlifts have not been reported earlier but it is possible that asymmetries with alternating grip or in grip width could result in movements in frontal plane of this small magnitude.
Methodological considerations of the present study should be noted. Firstly, to increase the internal validity of the study, the lifters were asked to perform conventional deadlifts regardless of whether they competed with the conventional or sumo style deadlifts. As proposed in a recent article,11 some individuals might be more suited to one of these styles than the other depending on anthropometrics, mobility and strength capacity in individual muscle groups. It is, however, possible that movement patterns would have been different if the choice of deadlift style had been optional. Since the sumo deadlift stance generally enables a more upright torso, and since it has been argued that lumbar lordosis is easier to maintain using the sumo stance,11 it is reasonable to assume that a different movement pattern in the upper and lower lumbar spine could be reported using sumo style deadlifts. Secondly, all lifts were performed without a lifting belt due to practical reasons concerning the fitting of the IMUs. This could, however, have had an impact on the results, where a lifting belt might have resulted in smaller range of motion in the spine since a belt improves lumbar spine stability.45
Thirdly, it is important to consider that the lifters in this study were lifters who, during training and competition, most often attempt to lift the maximum amount of weight possible. Therefore, the lifters might have used a technique enabling them to lift heavy weights in their respective sports but not necessarily to reduce the risk of injury. However, little is known about how the deadlift technique impacts injury risk and whether there is a difference between the optimal technique for performance and injury reduction.
Fourthly, all lifters were instructed to complete three repetitions with a load equivalent to 70% of their self-estimated 1RM. The load and repetition range are commonly used in powerlifting2 and weightlifting training46 and were chosen to represent a “minimum” training load. However, previous studies have used loads ranging from no additional load26 to 1RM.16,18 It is important to remember that spinal adjustments might differ depending on load and strength level. The level of strength and training experience among the men and women differed, i.e. the men were more experienced, lifted more weight relative to body mass and had a higher Wilks coefficient than the women. Top ranked lifters on national level have a Wilks coefficient between ~175-215, suggesting that both the men and women performed at an intermediate level.
Lastly, the findings rely on inertial motion sensors and the validity of this measurement approach has to be discussed. It has to be noted that the IMUs were mounted on the skin surface and that the angles might differ from actual skeletal alignment due the possibility that the IMUs could glide on the skin. There is no earlier study to measure the validity of the angles in comparison with a “gold standard” such as radiographs, videofluoroscopy, etc, but the IMUs have been validated to electromagnetic based system for measuring 3D spinal ranges of movement and coupled motion measurement.26 Finally, it could be argued that the measurement accuracy could be greater in the sagittal plane where the lumbar spine also have more range of motion and vice versa for the frontal and transverse planes.
CONCLUSION
This is the first study to describe spinal alignment; in all planes of movement, during the deadlift among men and women lifters, and to compare this between sexes. The results indicate that both sexes decreased lumbar lordosis from standing habitual posture to the start position of the deadlift and that spinal adjustmenst were made during execution of the deadlift. The decreased lumbar lordosis from standing habitual posture to the start position of the deadlift was significantly greater among men. As indicated by the measures of lumbar spine ROM, both men and women adjust their spinal alignment in all three planes of movement when performing a deadlift at approximately 70% of 1RM. Despite guidelines that a lumbar lordosis and/or neutral position should be preserved when lifting heavy weights, it seems that men and women lifters partially flex the lower back when performing deadlift at a sub-maximal load. Whether spinal alignment adjustments of this magnitude have an impact on injury risk should be investigated.
Conflicts of interest
The authors report no conflicts of interest.
Acknowledgments
The authors wish to thank Jimmy Falk for his help with the data collection.