

Introduction
Concussions are diffuse injuries to the brain,1 affecting various brain functions, including neurocognition and motor control.2 Gait research has advanced the understanding of the effect of concussions on motor control; altered gait patterns have been observed as a result of sports-related concussions.3–6 Dual-task walking involves locomotion while performing a concurrent cognitive task. Concussions usually affect motor and cognitive functions, so the divided attention required in dual-tasks may be more sensitive to post-concussion impairments than single-tasks.7 The addition of a cognitive load while walking also allows the evaluation of more subtle motor impairments due to the increase in processing demands required and decrease in available attention.8,9 Dual-task cost quantifies the change in a specific variable with the addition of the load (the difference in the variable from single-task to dual-task).10 Assessing the effects of dual-task is also advantageous as most sport and daily living activities require both a motor and cognitive component. Understanding their interaction in concussion may provide helpful information in injury recovery.
Researchers have observed that a full recovery in gait performance post-concussion required months to years, especially when the participant’s attention is divided.3,4,11,12 More traditional markers of recovery, like symptom surveys or neurocognitive test performance, typically analyze recovery on a shorter timeline.13,14 Assessing gait is advantageous because it is a non-novel task and can be objectively measured,3,4,12,15 unlike more obsolete methods of measuring balance16,17 or less mobile methods.18 Gait can be measured in-lab, but also on-field, using portable inertial measurement units.19,20
Accelerometry can be used to quantify gait and the incorporation of accelerometers into these body-worn portable sensors allow for an assessment of gait that allows for widespread use.19 Including a gait assessment in post-concussion protocols may provide an objective and sensitive measurement that can be assessed throughout return-to-play to monitor progress and management. Because limited sex-specific normative data exist for single and dual-task gait characteristics,7,21 baseline measurements are recommended22 as gait is unique to individuals and varies based on body size,23 concussion history,6,24 and sex.25 Females generally report more symptoms post-concussion26 and take a longer time to fully recover27 than males. Due to the differences in the presentation of concussions, it is interesting to understand any sex-specific gait changes. Understanding the effect of sex on the presentation and recovery of concussion will hopefully provide helpful information to drive sex-specific interventions.
Athletes with a history of concussion have been shown to have a more conservative pattern in their gait,6 including decreased walking speed, decreased cadence, decreased stride length, and increased double-leg support time compared with control subjects during dual-task walking.12 It is unknown how a season worth of cumulative head impacts in a contact sport affects gait. The aims of this study were to explore the differences between sexes in 1) dual-task gait metrics, 2) gait metric changes from pre-season to post-concussion and post-season, and 3) the dual-task costs associated with gait metrics.
Methods
Study Participants
In Spring 2019, Fall 2019, and Spring 2020, athletes from women’s and men’s collegiate club rugby teams were recruited for this study. Written informed consent was obtained from each participant after explaining the purpose, associated benefits, and risks of the study according to the ethical guidelines of Virginia Tech’s Institutional Review Board (IRB). Seventy-seven female athlete-seasons (age: 20.7 ± 1.2 years, height: 1.7 ± 0.1 m, weight: 75.1 ± 17.6 kg) and 64 male athlete-seasons (age: 21.0 ± 1.2 years, height: 1.8 ± 0.1 m, weight: 89.5 ± 17.5 kg) participated in the study. If an athlete participated for two seasons, their data are treated as two unique athlete-seasons, and they completed the full dual-task gait protocol each season. Athletes reported suspected concussions to the research team. Not all concussions were clinically diagnosed.
Dual-Task Gait Protocol
The gait protocol was completed pre-season (baseline), post-season, and post-concussion (if applicable). Athletes were not tested if they had a lower extremity injury. Those who sustained concussions were evaluated an average of 2.7 days after injury (range = 1 - 4 days). There were no post-season data collected for Spring 2020, as the season was interrupted due to COVID-19.
The gait protocol included two conditions: walking without a cognitive task (single-task) and walking while completing a cognitive task (dual-task). Five trials were conducted for each condition.21 The subject walked at a self-selected, comfortable pace, barefoot or in socks. They were instructed to walk towards an object 8 m in front of them, walk around it, and return to the starting point.21 For the dual-task trials, the test administrator explained the task before the start of the walk and the athlete began walking when cued by an auditory beep. The test administrator did not instruct the athlete to prioritize the motor or cognitive task, only to continue walking while responding to the task as best as possible.21 The dual-task consisted of a Mini-Mental Status Examination (MMSE), which has been shown to detect differences in dual-task walking after concussion.28 The MMSE contained three tasks: spelling a 5-letter word backward,15,29 subtracting by 6s or 7s from a randomly presented 2-digit number,30 and reciting the months in reverse order starting from a randomly chosen month.31 This cognitive test is similar to the Standardized Concussion Assessment Tool, Version 3, which is used for on-field concussion diagnosis.22,32 The tasks were randomly ordered to reduce learning effects from one trial to the next.
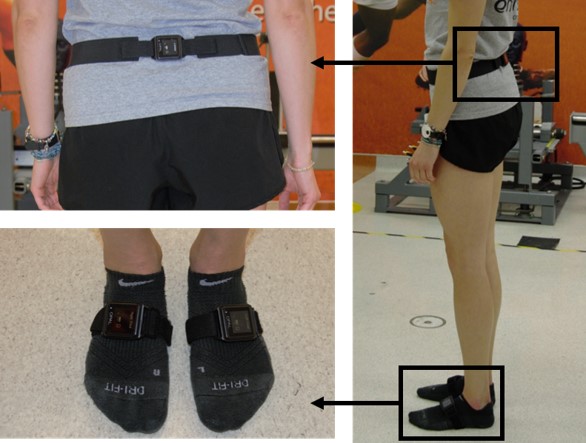
During the walking protocols, athletes wore inertial measurement units (Opal Sensor, APDM Inc. Portland, OR) attached with an elastic strap on the lumbar spine, at the lumbosacral junction, and on the dorsal surfaces of the left and right feet (Figure 1). This system has been validated33 and utilized in clinical evaluations of gait through the completion of motor tasks.20 Data were collected at a sampling frequency of 128 Hz and wirelessly synced to a computer during each trial. Temporal-distance measurements were calculated using Mobility Lab software20 and variables of interest included gait speed, cadence, double support time, and stride length, previously shown to differentiate healthy from concussed subjects.21,28,34

Outcome Variables
Gait speed, cadence, double support time, and stride length were measured for each athlete under both task conditions at each time point. Gait speed was calculated as the average velocity for the left and right foot across all gait cycles in each trial (m/s). Cadence was defined as the rate of steps per minute (steps/min). Double support time is the percentage of time that both feet were on the ground in each gait cycle, reported as percent of gait cycle time (%GCT). Stride length is the average distance for each foot between consecutive steps in each trial (m). The changes in each metric were computed from baseline to post-season and baseline to post-concussion (if applicable). Dual-task cost, the percent change between single and dual-task conditions, was calculated for each athlete to normalize their dual-task performance to their single-task performance.34,35 Dual-task cost was calculated as (dual-task value – single-task value)/(single-task value) and reported as a percentage. Dual-task cost was measured for each gait characteristic of interest.
Statistical Analysis
Shapiro-Wilk tests were used to confirm the normality of the gait metrics. Paired Welch two-sample t-tests were used to compare the magnitudes and estimate the effect size and precision of cadence, double support time, gait speed, and stride length from baseline to post-season within each task condition. The same paired comparisons were completed for athletes with baseline and post-concussion time point data. These comparisons were paired per athlete and compared within sex. Welch two-sample t-tests were completed to compare the differences in metrics between sexes from baseline to post-season for each task condition. Because there was only one concussion for the males, only females’ data were compared from baseline to post-concussion time points.
Dual-task costs were not normally distributed, so paired Wilcoxon rank-sum tests were used to compare dual-task costs from baseline to post-season within sex for each gait characteristic. Welch two-sample t-tests were used to estimate effect size and precision. Unpaired Wilcoxon rank-sum tests compared dual-task cost for each metric at each time. Again, only the females’ data were compared for the differences in baseline to post-concussion change, and between sex differences were not. Welch two-sample t-tests were used to estimate the effect size and precision of the comparisons. An α = 0.05 was used as a level of significance for all statistics.
Results
Gait metrics are presented from both task conditions at each time point (where applicable) for all athletes (Table 1). All comparisons within sex were paired, i.e., only athletes with both time points were included in this particular analysis.
Females walked with faster cadences at both task conditions at baseline and post-season than males (p < 0.032). Males walked with longer stride length in dual-task conditions at baseline and post-season (p < 0.023) and greater double support time in single-task conditions at baseline (p = 0.020). All other conditions were similar between sexes. The addition of the dual-task negatively impacted all gait metrics for both sexes at each time point (p < 0.001). Mean percent differences and 95th percentile confidence intervals between sex are shown in Figure 2. The females walked with greater cadence and a shorter stride length for the males in both task conditions. For each, mean differences were normalized to the males’ mean so each gait metric could be scaled for the sake of visualization. All baseline and post-season data that were collected were included in this comparison.

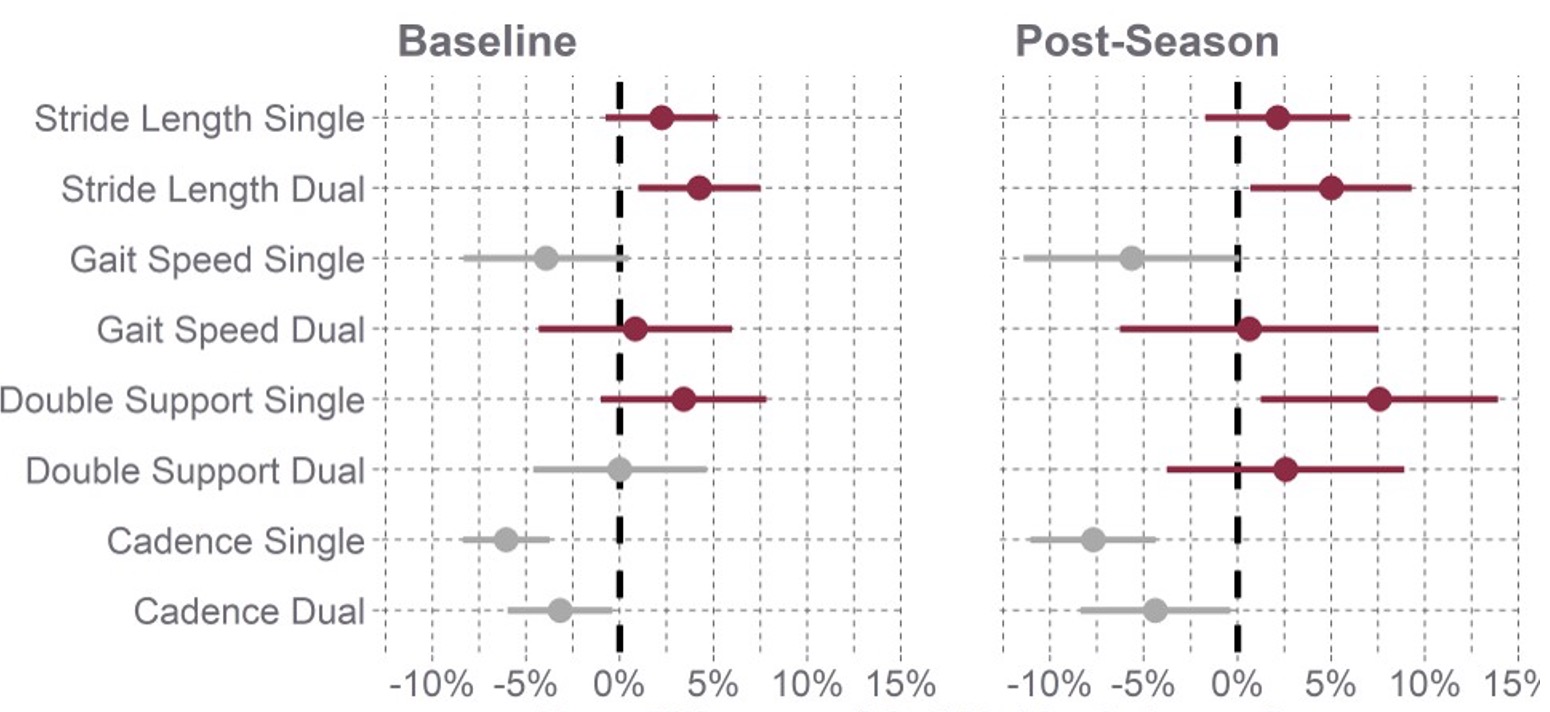
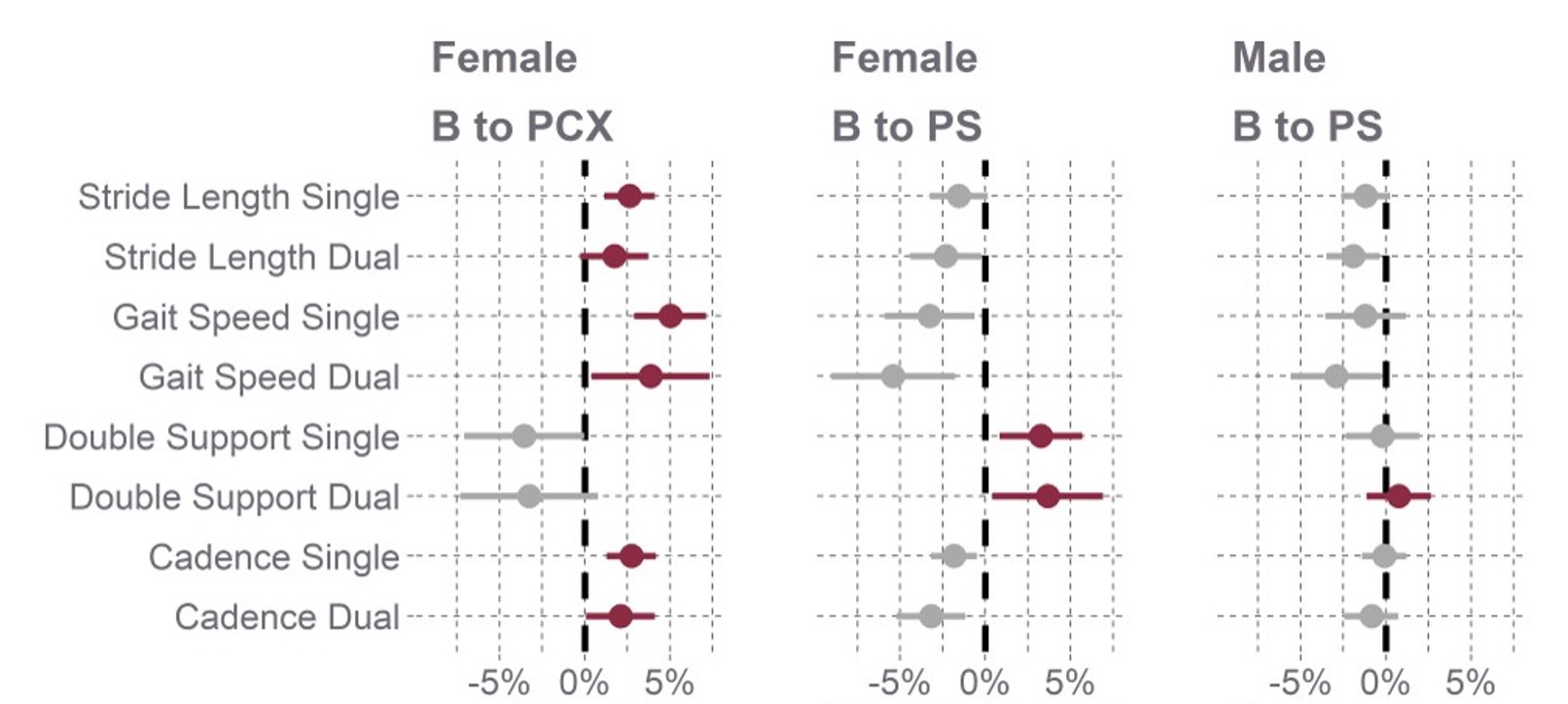
Paired t-tests showed improvement in cadence (increase), double support time (decrease), gait speed (increase), and stride length (increase) in both task conditions among the female athletes over the course of the season (Table 2) (p < 0.030). There was no change in stride length from baseline to post-season in dual-task (p = 0.071). The same tests for the males showed no differences in the metrics over the course of the season, except for faster gait speeds and longer stride lengths in the dual-task condition by the end of the season (p < 0.034). In general, cadence, gait speed, and stride length increased while double support time decreased by the end of the season, improving all characteristics. Females showed greater improvement in all gait metrics over the course of the season compared to males. The females performed worse at post-concussion compared to their baseline in each metric. Mean percent differences and 95th percentile confidence intervals between time points are shown in Figure 3. For each, mean differences are normalized to the baseline mean so each gait metric could be scaled for the sake of visualization. Only athlete-paired data were included in this comparison (Appendix Table A1).

The metrics from baseline to post-concussion were similarly compared to provide context to the changes over the course of the season (Figure 3). Post-concussion changes (Table 3) are opposite in magnitude to those seen in post-season (Table 2), with cadence, gait speed, and stride length increasing, and most double support times decreasing. Consistent with prior literature, cadence, gait speed, and stride length decrease while double support time increases after concussion. All characteristics showed deficits in the females in both task conditions (p < 0.042) with the exceptions of double support time and stride length during the dual-task condition (p > 0.083). It is impossible to generalize the males’ responses because post-concussion gait data were only collected from one male athlete.
The costs for cadence, gait speed, and stride length are all negative and double support time is positive because gait becomes more conservative with the addition of the cognitive load in the dual-task condition (Table 4). In all four gait characteristics, at baseline and post-season, females had higher dual-task costs (p < 0.003) than males (Figure 4). Females had a greater cost for each gait metric both at baseline and post-season. All baseline and post-season data that were collected were included in this comparison (Table 4).

Paired Wilcox test showed cadence and gait speed had higher dual-task costs at baseline compared to post-season for both males and females (p < 0.049) (Figure 5). Across all conditions, gait speed had the highest cost. Dual-task cost for double support time and stride length were not different at baseline or post-season for males or females (p > 0.059) (Figure 5). When comparing the post-concussion data to the paired baseline data for the females, there were no differences in cost between the two time points (p > 0.384) (Figure 5). Dual-task cost did not change much from baseline to post-season or post-concussion for either sex. Only athlete-paired data were included in this comparison (Appendix Table A2).

Discussion
The goal of including a dual-task condition in gait tests is to identify deficits that may not be as prevalent when the attention is focused on gait. In this study, the addition of the mental load at each time point decreased cadence, gait speed, and stride length and increased double support time for both sexes, in line with other studies.21 Compared to the males, females walked with faster cadences and shorter stride lengths, similar to previous research.7,34 It has been suggested that females’ dual-task gait velocity is higher because females may be better than males at executing two tasks at once.36 This also may explain the females’ improvement in all four gait variables (except for stride length in dual-task) over the course of the season. Males improved their gait speed and stride length in dual-tasks only; the rest of their metrics were not different from their baseline values. In this study, collegiate rugby players did not exhibit similar deficits in gait post-season to those they, or other studies have shown, post-concussion.12,37–40 Compared to a similar study by Howell, the athletes in this study spent much less time in double support (mean range 34.0 – 38.2 for concussed and control males and females),34 but there lacks a body of sex-specific normative value for comparison.
The changes the females showed post-concussion are consistent with post-concussion gait tests in the literature.7,34 Their cadence, gait speed, and stride length increased, and most double support times decreased. Previous work has shown a decrease in these metrics post-concussion,34,35 indicating a more conservative gait pattern, with the athletes walking slower with smaller steps post-concussion.
At baseline and post-season, females had higher dual-task costs than the males in all four variables. In general, gait speed had the largest dual-task cost. Dual-task costs for gait speed have been used as a predictor of prolonged recovery time in concussed athletes.41 Previous literature has shown a more significant cadence cost in females compared to males post-concussion.34 In the same study, they did not notice any dual-task cost difference between male and female controls,34 which is inconsistent with these results at baseline. They did not see a difference in dual-task cost from control males to concussed males either,34 which follows the same trend as the male athletes at baseline and post-season in this study.
It was expected that females would have a higher cost than males and that cost would be higher at post-concussion compared to baseline.4,35,42 The additional cognitive load was expected to reflect functional changes post-concussion and decreased interhemispheric brain connectivity,43 forcing the brain to reorganize to perform the challenging task while simultaneously providing resources for walking. In concussed athletes, this resource allocation is expected to be hindered,44,45 and appropriately reflected in dual-task costs. However, in this study, there were no differences in cost between the paired baseline and post-concussion data. Previous work has shown dual-task deficits at days 5-6,46 or in the year following,40 which is after all of the athletes in this study were tested. Additionally, as gait metrics in athletes in the current study improved over the season, cadence and gait speed had higher dual-task costs at baseline compared to post-season for both sexes. No study has quantified cost after a season of impacts for comparison.
The overall improvement in gait and decrease in dual-task cost could result from a learning effect of the tests. Still, there does not appear to be a deficit in gait or more conservative gait pattern that accumulated over the season. A study examining acute postural control effects after a simulated match load of rugby impacts also suggested no changes following subconcussive impacts.47 The learning effect is likely noticeable in this study as athletes completed the protocol multiple times in a season, and many participated in multiple seasons. Other studies compared concussed athletes to controls,34,35,48 which reduces the overall number of times an athlete would complete the dual-task protocol. Additionally, a season’s worth of exercise and training in their sport may have contributed to gait metrics improving.
There were several limitations to this study. Only one male post-concussion time point was collected, making it impossible to generalize about males’ responses post-concussion, compare them to the females at post-concussion, or compare them to males at baseline and post-season. Additionally, age, height, weight, or prior concussion history were not included in the comparisons in this analysis. Although likely the differences in sizes between males and females may contribute to the four gait variables, BMIs from the two groups are similar, and the dual-task cost normalizes performance individually. The environment in which the tests were conducted was not always consistent. They were conducted in the lab or the hallway, but sometimes the lab was busier than others, and the other distractions may have confounded the subject’s attention. However, the accuracy of these dual-task tests was not checked because the divided attention should be enough to elucidate differences; their performance on the MMSE should not matter. It has been shown that females prioritize the accuracy of their answers over their gait compared to their male counterparts.49
Conclusion
The results of this study indicate that collegiate rugby players do not exhibit post-season gait deficits, but show post-concussion gait deficits, similar to previous work.12,37–40 This suggests that although gait is affected by a concussive impact, it may not be affected by a season’s worth of head impacts. Contrary to other studies,40,46 the female athletes in this cohort did not exhibit differences in dual-task cost from baseline to post-concussion. Although the results of this study are mixed, dual-task gait can be used to uncover functional deficits in athletes who may be asymptomatic and do not exhibit neuropsychological dysfunction.45 Still, it is important to use dual-task gait in the context of other diagnostic tools. The sex-specific differences in gait metrics and dual-task cost at each time point suggest a need to consider the sex of the athlete in concussion diagnostics and therapies. Including dual-task gait assessments is also relevant given the implication of concussion on musculoskeletal injuries,50 and therefore should be incorporated into future clinical assessments and sex-specific concussion interventions.
Conflicts of Interest
The authors have no conflicts to disclose.