

- Department of Neurosurgery, Brain Research Institute, Niigata University, Niigata, Japan.
Correspondence Address:
Kohei Shibuya, Department of Neurosurgery, Brain Research Institute, Niigata University, Niigata, Japan.
DOI:10.25259/SNI_449_2023
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Kohei Shibuya, Hitoshi Hasegawa, Tomoaki Suzuki, Hidemoto Fujiwara, Satoshi Shibuma, Kazuki Shida, Makoto Oishi. Usefulness of Y-shaped PulseRider-assisted coil embolization for basilar artery tip aneurysm with a misaligned axis: A case report. 25-Aug-2023;14:300
How to cite this URL: Kohei Shibuya, Hitoshi Hasegawa, Tomoaki Suzuki, Hidemoto Fujiwara, Satoshi Shibuma, Kazuki Shida, Makoto Oishi. Usefulness of Y-shaped PulseRider-assisted coil embolization for basilar artery tip aneurysm with a misaligned axis: A case report. 25-Aug-2023;14:300. Available from: https://surgicalneurologyint.com/surgicalint-articles/12513/
Date of Submission
27-May-2023
Date of Acceptance
09-Aug-2023
Date of Web Publication
25-Aug-2023
Abstract
Background: Endovascular treatment of wide-necked bifurcation aneurysms remains challenging. Although the advent of PulseRider and Web has expanded treatment options, aneurysms with a large deviation from the parent artery axis remains difficult to treat. We present the case of a wide-necked bifurcation aneurysm that was misaligned with the angle between the long axis of the parent artery and the aneurysm and was successfully treated with Y-shaped PulseRider-assisted coil embolization.
Case Description: A 64-year-old woman presented with an unruptured basilar tip aneurysm. Cerebral angiography showed a wide-necked aneurysm measuring 8.1 mm × 6.1 mm, neck 5.7 mm. The aneurysm was strongly tilted to the right and posterior relative to the basilar artery, and the bilateral posterior cerebral artery (PCA) and superior cerebellar artery (SCA) diverged from the aneurysm body. PulseRider-assisted coil embolization was performed. A Y-shaped PulseRider was selected to be placed in a hybrid fashion with the right arch in the aneurysm and the left arch in the branch. Adequate coil embolization with preservation of the bilateral PCA and SCA was possible, and cerebral angiography immediately after the treatment showed slight dome filling. Cerebral angiography 6 months after the procedure showed that the embolic status had improved to complete occlusion.
Conclusion: For wide-neck bifurcation aneurysms with a misaligned axis, a Y-shaped PulseRider used in a hybrid fashion, in which the leaflet on the side with the tilted axis is placed in the aneurysm, allows the PulseRider to be deployed more closely to the aneurysm, thereby enabling good coil embolization.
Keywords: Coil embolization, PulseRider, Wide-neck bifurcation aneurysm
INTRODUCTION
Endovascular treatment of intracranial wide-neck aneurysms is widely performed due to advances in devices.[
CASE PRESENTATION
A 64-year-old woman with a head injury incidentally showed an unruptured basilar tip aneurysm on magnetic resonance angiography. Cerebral angiography showed a wide-necked aneurysm measuring 8.1 mm × 6.1 mm; neck, 5.7 mm, at the basilar artery (BA) tip. The aneurysm was strongly tilted to the right and posterior relative to the BA, and the bilateral posterior cerebral artery (PCA) and superior cerebellar artery (SCA) diverged from the aneurysm body [
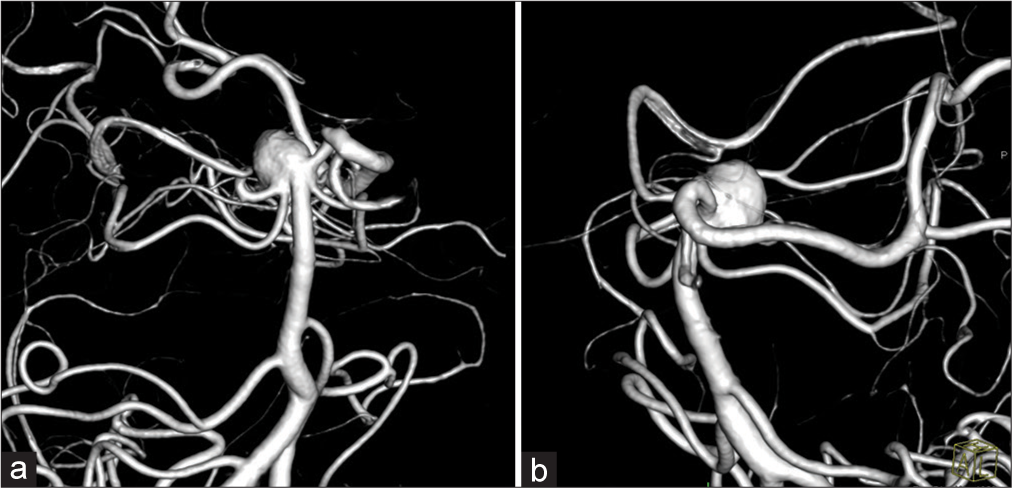
Figure 1:
Cerebral angiography showing a wide-necked aneurysm measuring 8.1 mm × 6.1 mm; neck, 5.7 mm, at the BA tip. (a and b) The aneurysm is strongly tilted to the right and posterior relative to the BA, and the bilateral PCA and SCA diverge from the aneurysm body. BA: Basilar artery, PCA: Posterior cerebral artery, and SCA: Superior cerebellar artery.
Because branch preservation with conventional stent-assisted coil embolization is difficult, we decided to perform PulseRider-assisted coil embolization. A Y-shaped PulseRider was selected to be placed in a hybrid fashion with the right arch in the aneurysm and the left arch in the branch. The patient received dual antiplatelet therapy with 100 mg aspirin and 75 mg clopidogrel 2 weeks before treatment. Under general anesthesia, an 8 Fr-long sheath was inserted into the right femoral artery. After inserting an 8 Fr Roadmaster (Goodman, Aichi, Japan) into the left subclavian artery, a 6-Fr Navien (Medtronic, Minneapolis, MN, USA) was inserted into the left distal vertebral artery as an intermediate catheter. A Headway27 (Terumo Corporation, Tokyo, Japan) was selected as the microcatheter in anticipation of torque transfer and support to the PulseRider, and the Headway was guided proximal to the BA tip aneurysm. Although somewhat difficult, a PulseRider (10Y/2.7-3.5, Cerenovus, New Brunswick, NJ, USA) was deployed in a hybrid fashion as planned [
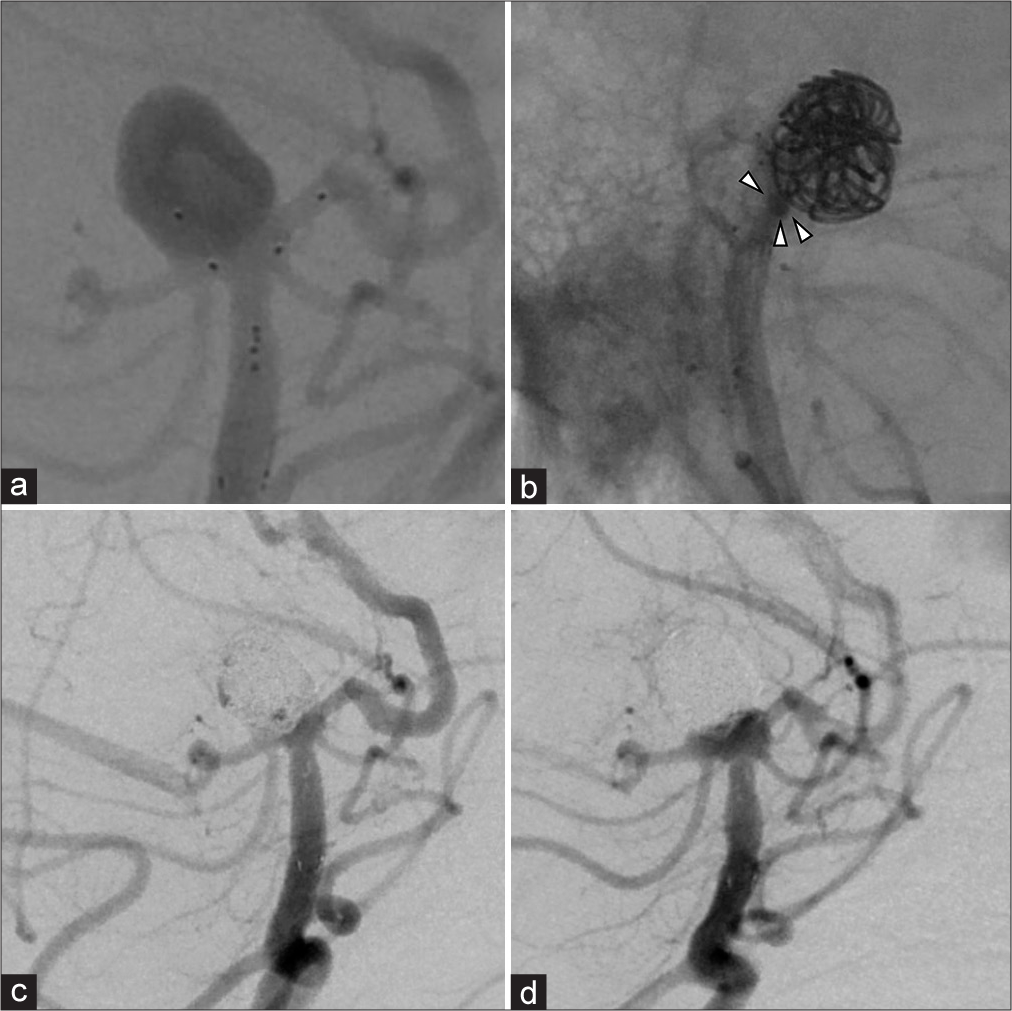
Figure 2:
(a) A PulseRider (10Y/2.7–3.5) is deployed in a hybrid fashion with the right arch in the aneurysm and the left arch in the PCA as planned. (b) The aneurysm neck is covered by PulseRider, and the barrel view shows no deviation of the coil into the parent artery (arrowhead). (c) A cerebral angiography immediately after treatment showing slight dome filling, and bilateral PCA and SCA blood flow is normal. (d) A cerebral angiography 6 months after the treatment showing that the embolic status had improved to complete occlusion. PCA: Posterior cerebral artery and SCA: Superior cerebellar artery.
DISCUSSION
Despite advances in endovascular treatment, coil embolization of wide-neck bifurcation aneurysms remains challenging.[
The efficacy and safety of the PulseRider in intracranial wide-neck aneurysms have been demonstrated in a meta-analysis.[
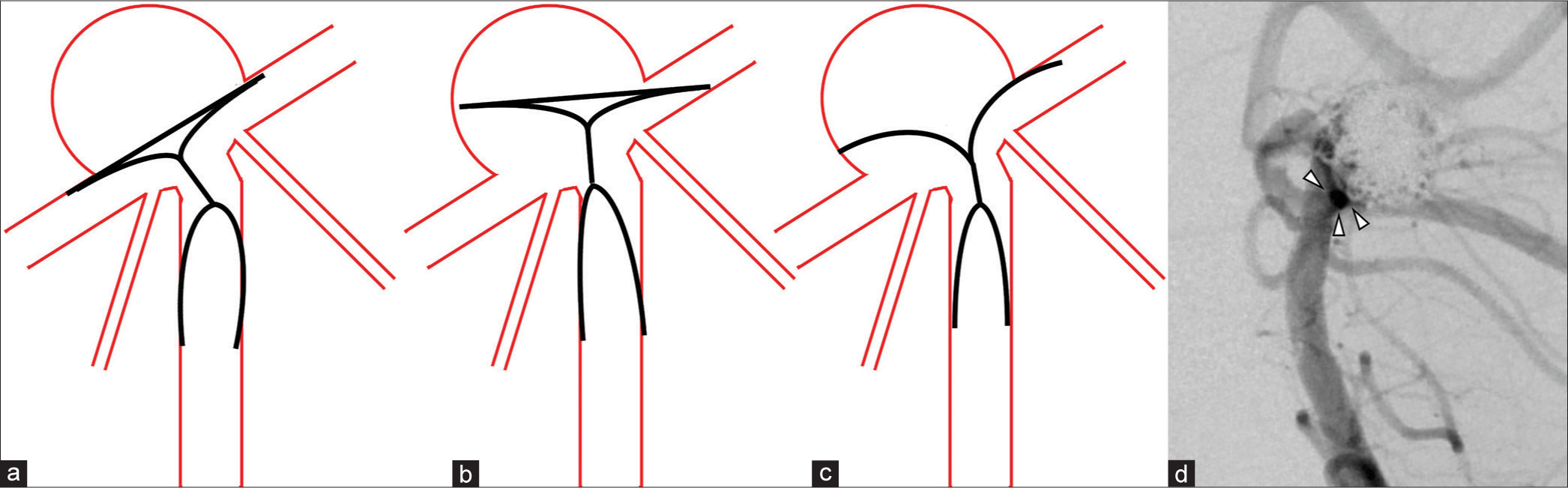
Figure 3:
(a) When the aneurysm is displaced to the left or right in relation to the axis of the parent artery, it is ideal to place the PulseRider in the extra-aneurysm position. (b) However, this is often difficult, and hybrid placement should also be considered. (c) The Y-shaped PulseRider can adhere more closely to the neck than the T-shaped PulseRider. (d) Cerebral angiography immediately after treatment shows no coil deviation in the parent artery in the barrel view (arrowhead).
There are few reports on the long-term efficacy of PulseRider-assisted coil embolization. In a report comparing the results of a Y-stent technique and PulseRider-assisted coil embolization, there was no difference in adequate occlusions immediately after treatment, but cerebral angiography 6 months later reported significantly less complete occlusion with PulseRider and significantly more worsening of the embolic conditions with PulseRider.[
CONCLUSION
Here, we described a case of coil embolization using a Y-shaped PulseRider with good results for a BA tip aneurysm misaligned along the axis with the parent artery. By placing the leaflet with a tilted axis into the aneurysm, the PulseRider can be placed closer to the aneurysm, which is expected to provide effective embolization and reduce the risk of recurrence.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author(s) confirms that there was no use of Artificial Intelligence (AI)-Assisted Technology for assisting in the writing or editing of the manuscript and no images were manipulated using the AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Blackburn SL, Kadkhodayan Y, Shekhtman E, Derdeyn CP, Cross DT, Moran CJ. Treatment of basilar tip aneurysms with horizontal PCA to PCA stent-assisted coiling: Case series. J Neurointerv Surg. 2013. 5: 212-6
2. Fiorella D, Albuquerque FC, Han P, McDougall CG. Preliminary experience using the Neuroform stent for the treatment of cerebral aneurysms. Neurosurgery. 2004. 54: 6-16
3. Fiorella D, Arthur AS, Chiacchierini R, Emery E, Molyneux A, Pierot L. How safe and effective are existing treatments for wide-necked bifurcation aneurysms? Literature-based objective performance criteria for safety and effectiveness. J Neurointerv Surg. 2017. 9: 1197-201
4. Goyal N, Hoit D, DiNitto J, Elijovich L, Fiorella D, Pierot L. How to WEB: A practical review of methodology for the use of the Woven EndoBridge. J Neurointerv Surg. 2020. 12: 512-20
5. Lee CY, Kim CH. Very late stent thrombosis following the placement of a crossing Y-stent with dual closed-cell stents for the coiling of a wide-necked aneurysm. BMJ Case Rep. 2014. 2014: e38
6. Limbucci N, Cirelli C, Valente I, Nappini S, Renieri L, Laiso A. Y-stenting versus pulserider-assisted coiling in the treatment of wide-neck bifurcation aneurysms: Role of anatomical features on midterm results. Neurosurgery. 2020. 87: 329-37
7. Malek AM, Halbach VV, Phatouros CC, Lempert TE, Meyers PM, Dowd CF. Balloon-assist technique for endovascular coil embolization of geometrically difficult intracranial aneurysms. Neurosurgery. 2000. 46: 1397-406
8. Pranata R, Yonas E, Vania R, Sidipratomo P, July J. Efficacy and safety of PulseRider for treatment of wide-necked intracranial aneurysm-a systematic review and meta-analysis. Interv Neuroradiol. 2021. 27: 60-7
9. Sakai N, Imamura H, Arimura K, Funatsu T, Beppu M, Suzuki K. PulseRider-assisted coil embolization for treatment of intracranial bifurcation aneurysms: A single-center case series with 24-month follow-up. World Neurosurg. 2019. 128: e461-7
10. Spiotta AM, Chaudry MI, Turner RD, Turk AS, Derdeyn CP, Mocco J. An update on the adjunctive neurovascular support of wide-neck aneurysm embolization and reconstruction trial: 1-year safety and angiographic results. AJNR Am J Neuroradiol. 2018. 39: 848-51
11. Spiotta AM, Sattur MG, Kan P, Crowley RW. Bifurcation aneurysm treatment with PulseRider: Technical nuances, device selection, positioning strategies, and overcoming geometric challenges. World Neurosurg. 2020. 142: 339-51
12. Zhao B, Yin R, Lanzino G, Kallmes DF, Cloft HJ, Brinjikji W. Endovascular coiling of Wide-Neck and Wide-Neck bifurcation aneurysms: A systematic review and meta-analysis. AJNR Am J Neuroradiol. 2016. 37: 1700-5

