Introduction
Trail-running is defined as a pedestrian race in a natural environment (e.g. mountain) with minimal possible paved or asphalt road (which should not exceed 20% of the total course) (Association, 2018). As a consequence, trail-running involves long stretches of up- and downhill running not encountered on classical road races and including technical sections on rocky and root-covered paths (Ehrström et al., 2018). Even though off-road races are not a new invention, trail-running as a sport with its own International Trail-Running Association has become increasingly popular (Giandolini et al., 2016; Vernillo et al., 2017). More information about the special demands of trail-running on the athlete is therefore essential to develop better training methods and to determine the major differences between trail- and level road runners.
One of the biggest differences between trail and road running is the large amount of uphill running involved. There are several aspects to this difference.
Level running (LR) can be described by the stretch-shortening cycle of the muscle-tendon unit of the lower limb in which part of the mechanical energy of the center of mass (COM) is absorbed during the negative work phase to be restored during the next positive work phase (Nicol et al., 2006). This change in kinetic and potential energy contributes to one of the energy-saving mechanisms during running (Cavagna, 1977;
Cavagna et al., 1977; Cavagna and Kaneko, 1977) and the storage and release of elastic energy contribute to the acceleration of the body upwards during the propulsive phase and to the reduction of the energy production needed during the concentric phase (Snyder and Farley, 2011; Snyder et al., 2012). In uphill running (UR), the COM needs to be propelled vertically and does not oscillate around an equilibrium but gains potential energy by losing elastic energy (Dewolf et al., 2016). This changes running into a mainly concentric muscle work (Giandolini et al., 2016). These biomechanical considerations should lead to changes in running economy and therefore, physiology of UR and LR. The question therefore arises, whether these biomechanical observations are reflected in physiological variables that can be measured during UR and LR?
The key physiological variables used for evaluating performance in running are peak oxygen uptake
Lauenstein et al. (2013) were even able to show a strong correlation between maximal running velocity uphill and
Blood lactate also seems to reach higher levels when examined with supramaximal uphill tests compared to level running tests (Vernillo et al., 2017). Some studies were even able to show an increase in blood lactate concentration in response to the increasing slope (Itoh et al., 1996; Padulo et al., 2013). Incline has a significant effect on the metabolism of rats running on a motor-driven treadmill (Armstrong et al., 1983) and uphill training in rats has proven to increase glycogen content in the gastrocnemius muscle (Morais et al., 2018) as well as enhance mitochondrial function in soleus and vastus intermedius muscles (Schlagowski et al., 2016). Considering these findings, it could be hypothesized that trail runners have a lower lactate difference between a maximal uphill running test and a maximal level running test than runners used to level road races.
The energy cost of running represents the amount of energy spent to transport the subject’s body a given distance (di Prampero et al., 1986)
The other factor that differentiates trail running from road running is the uneven and difficult terrain. It has been pointed out before that Cr measured during running does not reflect the reality in the field (Minetti et al., 2002a; Vernillo et al., 2017). It was shown that the correlation between laboratory-based values and a 2-km time
trial performance was lower when the field test was performed in a forest path compared to the road condition (Hébert-Losier et al., 2014). Thus, investigating cardiopulmonary exercise variables on a treadmill even in an uphill setting may not reflect the true cardiopulmonary capacity of trail runners. In order to determine the cardiopulmonary capacity and training thresholds (VT1 and VT2) of athletes, sports-specific cardiopulmonary testing is necessary. We have been able to show that ski mountaineers need to be tested on skis (Schöffl et al., 2018). As trail running involves uphill running as well as running on uneven terrain, testing on a treadmill with positive inclination would not suffice to determine the correct thresholds as well as the cardiopulmonary capacity of a trail runner. We therefore hypothesized that a field test would be better suited for establishing the ventilatory thresholds in trail runners allowing for the differentiation between trail runners and road runners with respect to the unique characteristics of running on trails as well as uphill.
In this study we compared data from two different maximal incremental running tests in a group of competitive road runners versus a group of competitive trail runners. The purpose was to evaluate the difference between these two groups regarding cardiopulmonary exercise variables such as
Methods
Participants
Ten male competitive trail runners and ten competitive level road runners from local clubs participated in our study. Trail runners participated in at least two trail races between 23 and 50 km lengths per year, while level road runners were half marathon and marathon runners on a regular basis (more than ten races per year). Participants were fully notified about the possible risks associated with the study and gave written informed consent to take part in the study. Before each test participants were examined clinically to rule out infections or other contraindications to CPET. This study was approved by the Ethics Committee of the University of Erlangen-Nürnberg, Erlangen, Germany (Study Number 13_19 B).
The study was conducted in the preseason training period. Between the two tests there was a rest period of two weeks. Each participant was asked to refrain from maximal effort the day preceding the test day and to abstain from eating solid foods or carbohydrate-rich drinks in the three hours leading up to the test. The standards of general performance diagnosis and stress tests were fulfilled (temperature 18 – 24 °C, relative humidity 30 – 60%), and all participants had a minimum rest period of 48 hours prior to the first test from athletic or any other energy demanding activity.
Measures
Athletes performed one test on a treadmill (Callis Ortho ®, Kleines Wiesental, Germany) as a speed-incremented treadmill test to exhaustion with an inclination of 1%, as this inclination most accurately reflects energetic costs of level outdoor running (Jones et al., 2000). The indoor test was conducted first as we were thus able to perform an ECG during the test for monitoring the athlete’s cardiac health. At the beginning, there was a ten-minute warm-up at a speed of 8 km/h to familiarize athletes with the treadmill. Then the test started at a speed of 8 km/h and increased by 1.5 km/h every three minutes until exhaustion. After each step there was a short rest interval (max. 10 s) during which athletes hopped onto the stationary part of the treadmill and blood lactate samples from the earlobe were drawn within 30 seconds. The Borg’s Scale was used to assess participants’ relative perceived exertion (RPE) (Borg, 1982). The heart rate was measured using a regular heart rate monitoring system (Polar H7 Bluetooth Smart 4.0 heart rate sensor ®, Kempele, Finnland). Oxygen uptake was measured breath-by-breath with an open-circuit mobile spirometry system (Metamax ®, Cortex, Leipzig, Germany). Lactate concentration was determined taking a 10 μl blood sample from the right ear lobe and measured with a table-top lactate analyzer (the Lactate Scout ® EKF, Cardiff, United Kingdom).
The second test was performed as a field test. We chose a hill with a constant grade of 16% corresponding to 14°. Athletes warmed up for ten minutes on the hill and the surrounding trails. After the warm-up and a ten-minute rest period, athletes were instructed to run up the hill four times for a time of three minutes: the first time with a leisurely pace, the second time with a normal pace, the third time with a submaximal pace and the fourth time at maximal speed. After completion of the tree minute uphill run, a blood lactate sample from the earlobe was drawn immediately upon completion of the uphill run, within a timeframe of 30 seconds. The heart rate and oxygen uptake were measured as in the treadmill test. The RPE was not evaluated as athletes were instructed to run at a certain exertion comparable to 8 on the Borg scale for the first run, 11 - 12 for the second run, 15 - 16 for the third run, and 19 - 20 for the fourth run. Athletes then ran back down to the bottom of the hill in a leisurely pace.
EF, defined as the ratio between horizontal and uphill running performance was calculated according to the following formula:
where α = angular degree of the hill, which corresponds to 9°.
Cr was calculated using the following formula:
Ventilatory thresholds VT1 and VT2 were determined using the Wasserman approach (Beaver et al., 1986) during the treadmill test. In the field test we used the recording of the second uphill run for determining VT1, again using the Wasserman approach. The second ventilatory threshold (VT2) (Westhoff et al., 2013) was determined by visual analysis of the breakpoints of ventilator equivalents for oxygen and carbon dioxide, and minute ventilation changes over time with an increase in both
Furthermore, we investigated the remaining variables determined during cardiopulmonary exercise testing, namely O2pulse, tidal volume (VT), breath rate reserve (BRR), heart rate reserve (HRR) and
After comparing the two groups we combined the test results of both groups and compared the field test with the treadmill test to achieve a clearer understanding of the differences of uphill running on uneven terrain with level running on a treadmill.
Statistical Analyses
Statistical analysis was performed using Microsoft Excel 2000® for data collection and SPSS 12.0® (SPSS Inc., Chicago, IL). All measured values are reported as means and standard deviations. The Kologomorov-Smirnov test was used to check for normal distribution. Homogeneity of variance was investigated using the Levene’s test. For normally distributed variables differences between the two test protocols were assessed with paired t-tests, otherwise the Wilcoxon or the Whitney-Mann-U-tests were used. All tests were 2-tailed, a 5% probability level was considered significant (*), a 1% probability level was considered highly significant (**). For linear regression analysis the nonparametric Spearman correlation coefficient (rs) was used for normally distributed variables.
Results
The trail runners were 42.8 (± 14.6), the road runners 34.3 (± 5.9) years of age. Even though trail runners were older by ten years, this difference did not reach significance. The mean body mass was 75.8 (± 10.2) kg, the mean body height 179.9 (± 6.6) cm for trail runners and 77.6 (± 9.6) kg and 181.7 (± 7.5) cm for road runners. No significant differences were observed in body mass and height between the groups.
When comparing the two groups regarding the cardiopulmonary exercise variables at maximum exertion as well as at VT1 and VT2 during the trail test and the treadmill test, there were no significant differences between trail and road runners. The main cardiopulmonary exercise variables from the two tests are presented in Table 1. Road runners were faster on average during the treadmill test (16.5 vs. 15.8 km/h), but also during the trail test (8.1 vs. 7.6 km/h). However, when expressed in terms of relative speed, trail runners reached 48.2% of the speed of their treadmill test during the trail test and road runners reached 46.6% of the relative speed. None of these results reached the level of significance.
Table 1
Mean and standard deviation for the cardiopulmonary exercise parameters during the trail and treadmill test in both groups (* indicates significant differences between the Trail and the Treadmill test)
As there was no difference between the two groups, we were able to compare the trail test with the treadmill test. Most variables showed significant differences (Table 1). However,
Figure 1
Energy cost of running (Cr, ml O2/kg/m) during the trail and the treadmill test for road runners and trail runners (*indicates a significant difference between the trail test and the treadmill test).
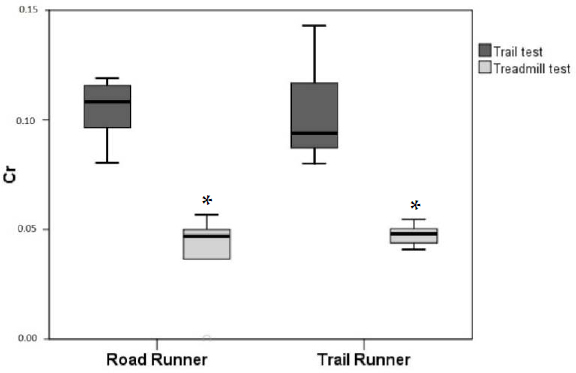
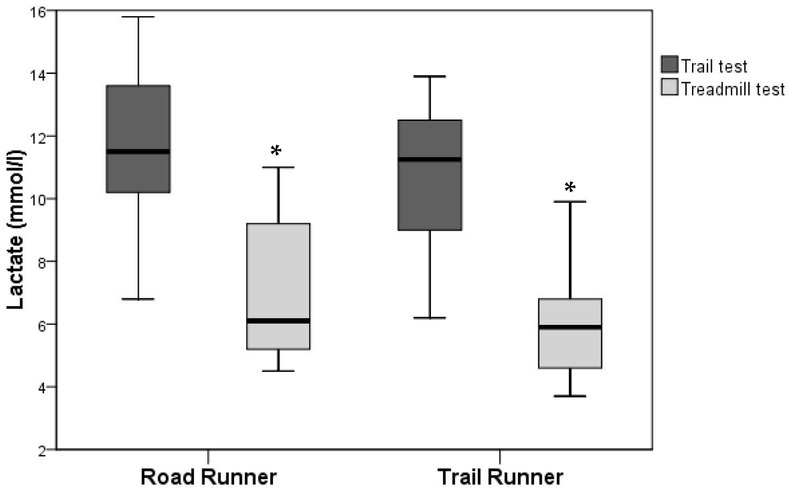
Figure 2
Lactate concentration (mmol/l) during the trail and the treadmill test for road runners and trail runners (* indicates a significant difference between the trail test and the treadmill test).
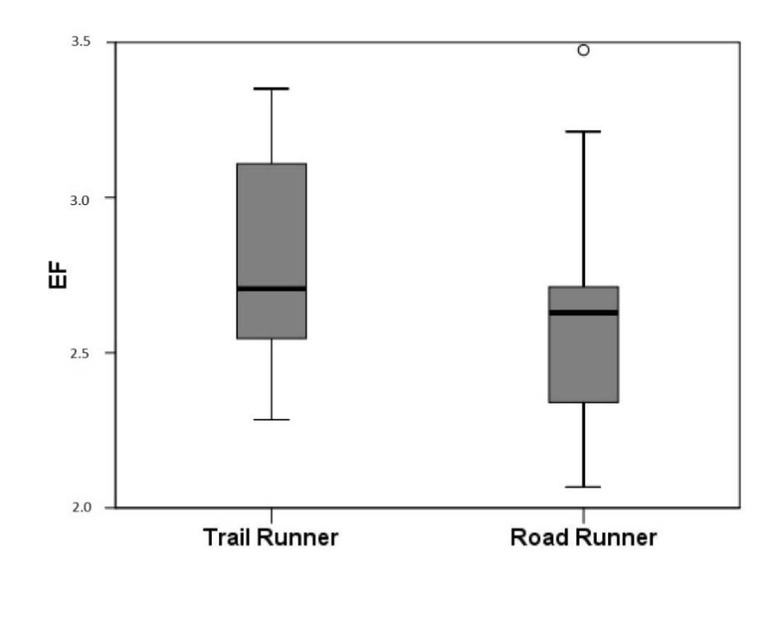
The EF reached a mean value of 2.8 (± 0.4) in the group of trail runners and a mean value of 2.6 (± 0.5) in the group of road runners. Again, there was no significant difference between the two groups (Figure 3).
Discussion
As trail running is a sport which involves covering large amounts of incremental running over uneven terrain, uphill running ability as well as the ability to run efficiently on uneven trails is a determining factor of performance. This study was undertaken to determine if there was a difference between a group of trail runners when compared to a group of road runners with respect to cardiopulmonary exercise variables collected during an incremental uphill field test versus a standard incremental treadmill test without inclination. The goal was to establish a better testing method for determining ventilatory thresholds for trail runners during uphill training, and to establish a better understanding of the physiologic demands of trail running
So far most studies comparing uphill versus level running elicited higher
significantly
The maximum speed achieved during the trail test was about half as high as the speed achieved during the treadmill test, with higher speeds achieved by road runners in both tests. This suggests that road runners were the fitter group. Trail running tends to involve longer distances and be less competitive than road running. We observed a wider age range in our trail running group with more runners in the age group of fifty years and older. Thus, we hypothesized that our road running group would be fitter with higher speeds achieved during both tests as a consequence of the trail runners being older. This was also reflected in higher heart rates achieved by road runners. There was a strong correlation between the maximum speed during both tests and
There was no difference between O2pulse between the groups nor between the test protocols, thus the proposal of higher cardiac output during uphill locomotion (Kamon and Pandolf, 1972b) is unlikely in a group of well-trained athletes. However, peak O2pulsee of the trail test correlated significantly with
Blood lactate concentration seems to reach higher levels in UR compared to LR (Itoh et al., 1996; Padulo et al., 2013; Vernillo et al., 2017). Glycogen depletion (assessed by muscle biopsy) has been shown to be higher in the vastus lateralis, gastrocnemius and soleus muscle in rats and in humans during UR (Armstrong et al., 1983; Costill et al., 1974), suggesting a higher percentage of muscle mass being recruited during UR in these muscles. This could explain the higher blood lactate values observed in our study as well.
As previously described, energy cost of running was significantly higher during UR than during LR (Balducci et al., 2016; Minetti et al., 1994) and comparable to previous studies with the same amount of increment (Balducci et al., 2016). It has been observed that subjects vary widely in uphill Cr (Balducci et al., 2016). Bearing in mind that Cr can be improved by appropriate training (Barnes et al., 2013) the difference between Cr in UR and Cr in LR should be reduced after training of UR. Thus, it was surprising that trail runners showed a wider variety of Cr during the trail test and a lower variety during the treadmill test compared to road runners, exactly opposite to what we would have expected. This reflects a possible bias of our study sample, having older runners in the trail running group than in the road running group. Also, the difference in Cr during the trail test and the treadmill test was not lower in the trail running group, although it could have been expected that regular uphill training would lead to a lower Cr during the field test in trail runners. As discussed previously, even though each group raced in their respective categories their training probably involved both types of running (trail and road running) so that the differences may have been suppressed.
To determine how many meters of horizontal distance equate to 1 m of climb, a standardized method has been proposed, i.e., the equivalence factor (EF). It equates one unit of climb to a horizontal distance. The recorded values for the EF in runners have shown to be prone to high inter-individual variability and have been proposed in orienteering athletes for aiding route choice during competition (Lauenstein et al., 2013). An EF greater than 7 represents a weak uphill running ability, whereas an EF smaller than 5.6 represents a strong uphill running ability (Lauenstein et al., 2013). Similar values have been proposed after evaluating the EF in fell running races (Scarf, 2007). In treadmill running experiments or mountain road-relays, however, much lower values have been recorded (3.3 to 4.4) (Scarf, 2007). It was therefore surprising to note that the EF values in our athletes were all below those reported by Lauenstein et al. (2013) and collectively below 3.5. It has been hypothesized that rough outdoor terrain may limit the runner’s ability to physically exert themselves and therefore, raise the EF. Although the field test was conducted on an outdoor trail, the surface of the trail was rather smooth and not as rough as often encountered in real trail events. Therefore, the reason for the rather low EF across our study sample may well be due to the smooth surface and thus comparable with lower technical demand of the trail. However, even considering that our trail was not rough enough to force a higher EF, our runners achieved astoundingly low values. This reflects that both our groups were probably accustomed to the kind of the slope and length of the hill we used during the field test as it represents a typical hill in the area our study participants trained in. The hill was not as steep as previously described (Lauenstein et al., 2013) and may also have contributed to a better efficacy in running uphill. A steeper hill with more trail-like terrain may well have yielded similar results to previous studies (Lauenstein et al., 2013; Scarf, 2007) and may have had the advantage to lead to a better differentiation between our two groups.
Therefore, the limitations of this study lie mainly in the choice of the two groups. Even though trail runners only participated in trail running events and road runners only in running road races, both groups regularly trained in the forest and on hills, leading to comparable test results in both groups. A further limitation was the choice of the hill for the field test. A steeper hill with more rough terrain would probably have led to a higher EF and may very well have helped for a better differentiation between the two groups.
Conclusions
The comparable