Keywords
Tumor ablation; Hyperthermia; RFA; MWA; Cryoablation; HIFU; Laser ablation
Introduction
For thousands of years, man used temperature for therapeutic applications. The effect and influence of temperature had been early observed and used even though the understanding of the bioeffect of heat was not clear, so in different civilizations all over the world we can find many uses the heat and cold to treat some diseases including tumors. The principle of the thermal therapy is the application of the heat or cold to change the cutaneous, intra-articular or core temperature of the soft tissue. Oncology remains one of the fruitful application domain of the thermal therapy. Due to the enormous number of a cancerous people over the world, the World Health Organization (WHO) classifies cancer as one of the deadest diseases of the last decades. In 2010, the total worldwide cost of the cancer was estimated to USD 1.16 billion, and it is on rising. Many statistics show astronomical numbers, all over the world, of the cancer deaths and the enormous number of the new cancer cases detected each year. The WHO provides some shocking statistics by 8.8 million dead in 2015 and it is considered as the second death cause in the USA in 2016. For this reason, research on cancer treatment remains a hot and dynamic scientific issue to improve the existing therapies.
Nowadays, thermal therapy has considerably improved. It has been used in many medical applications and many techniques have been developed. Divided by range of the temperature attended and the time duration, we can classify the thermal therapy into Diathermia, Hyperthermia, and Thermal Ablation. The first one elevates the temperature up to 41°C. It is mostly used in physiotherapy to treat rheumatic diseases as muscles and joints. Its principle is based on the use of low temperature for approximately an hour to accelerate the cell healing and increasing the blood flow and metabolic rates. The second one overheats the targeted tissue by few degrees more, between 41°C to 45°C for several minutes. This therapy consists of increasing the temperature of the tissue to kill the malignant cells and save the healthy tissue. The last therapy can be classified into diverse types. It is based on the use of a hot or a cold source to ablate the unhealthy tissue by elevating the temperature or cooling down the targeted tissue. We can categorize these ablation techniques into Radio Frequency (RF) ablation, Ultrasound (US) ablation, Laser ablation, Microwave ablation (MW) and Cryoablation (CA).
The mathematical model describing the heat transfer in the living tissue is commonly known as Bio-Heat Transfer (BHT) model. The first model was proposed by Pennes in 1948 [1-19].
The equation is given as
 (1)
(1)
where k, c, and ρ stand for the thermal conductivity (W/m.k) of the tissue, specific heat (J/kg.K) and density (kg/m3), respectively. T denotes the local tissue temperature (K). Ta is the arterial blood temperature (K). ρb and cb are the density and specific heat of the blood. The perfusion rate is described by ω (l/s). Qm and Qr define the metabolic heat production per volume (W/m3) and the injected power, respectively. In lack of an external heat source, the Joule effect in our case, equation (1) describes the Pennes equation modeling the BHT in biological tissue without external excitation [20].
The Initial Condition (IC) for the 1D equation is expressed in equation (2). It is given as
 (2)
(2)
The Boundary Conditions (BC) associated with 1D BHT can be classified into three standard types. Equations (3-7) show various kinds of BC with Cartesian coordinates for one dimension (1D). For x=0, we define the BC1 as the outer surface. For x=L, we define the BC2 as the region adjacent to the core. Figure 1 shows a 1D Bio-heat Cartesian System.
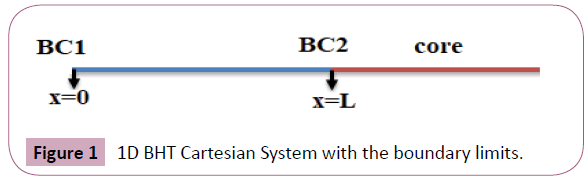
Figure 1: 1D BHT Cartesian System with the boundary limits.
Type 1 boundary condition: Specific surface temperature (Dirichlet condition)
For x=0:  (3)
(3)
For x=L: (4)
Type 2 boundary condition: Specific heat flux ‘q’ (Neuman condition)
For x=0:  (5)
(5)
For x=L: Equilibrium in flux  (6)
(6)
Type 3 boundary condition: Convection heat transfer ‘h’
For x=0:  (7)
(7)
For x=L, the tissue is considered to be in thermal equilibrium with the tissue. For this reason, we do not consider a type 3 [21].
Effects of Temperature on the Living Tissue
The heat injuries can be classified into three degrees depending on the depth of the burn. The first degree is a superficial burn on the epidermis. The second degree is deeper than the first-degree burn. It involves injuries to the dermis. It is divided into two categories: superficial partial-thickness second-degree dermal burns and deep partial-thickness second-degree dermal burns. The third-degree causes irreversible damage. It is known as full thickness burns [22]. Contrary to the first degree and the partial-thickness second degree, which can heal spontaneously, the third degree and fully partial-thickness second degree requires a specific treatment. The biological tissue reacts to heating excitation as well as a cooling excitation. For this reason, low temperatures have been used to treat some injuries or stop hemorrhages. Even in Oncology, some researchers investigated the cryotherapy technique to ablate different kind of tumors, especially some case of cervical cancer or hepatic cancer [23-25].
Pavel et al. reviewed the thermal threshold for tissue damage. They showed, according to different heating source the thresholds available in the literature. They reported the various effects of the temperature on the cells, the DNA and the different part of the body according to the Cumulative Equivalent Minute at 43°C (CEM43). Many techniques are cited and discussed [26].
Death Process of Cells with Temperature
The volume of the damaged tissue depends directly on the heating source (power injected, time of exposure, wavelength) and the tissue parameters (thermal conductivity, density, electric conductivity, specific heat). The thermal ablative therapy produces three distinct zones. The central zone, which is the principal targeted area. It holds the malignant cells to destroy. The necrosis level of the cells is reached immediately after injecting the power (especially in RF ablation). The damage is irreversible. The second zone is the peripheral zone which surrounds the central targeted area. In this zone, the necrosis is not reached. However, an overheating due to the conduction effect can provoke reversible injuries. If the time of exposure and the power injected are controlled, we can avoid the irreversible injuries. The third zone is the unaffected healthy tissue [27]. Figure 2 shows the different zones of an RF ablation.
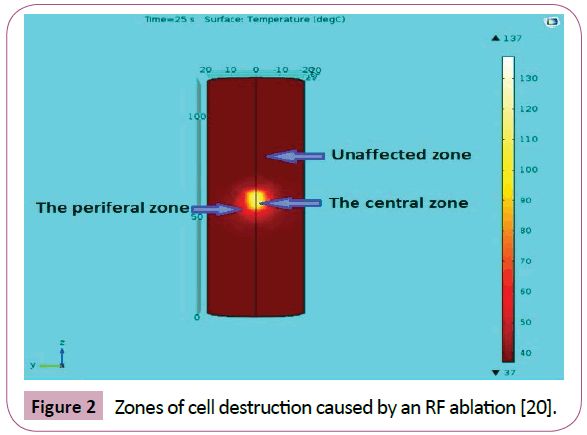
Figure 2: Zones of cell destruction caused by an RF ablation [20].
The death cells mechanism leads to the destruction of the tumor. This process occurs in several ways in cryotherapy and hyperthermal therapies. The cell death mechanism in cryotherapy is caused by an extreme low-temperature exposure. The cooling source produces a frozen necrosis area, which leads to irreversible damage. In the peripheral zone, a reversible damage can be watched due to conduction effect. In the hyperthermal therapy, other phenomena occur. This technique consists on elevating the temperature of the tumor to kill the malignant cells.
The mechanism of death is complex and took place at a different level within the tissue. At 50°C, the enzymatic activity of the cells disappears, which leads to the death of the cells. At 60°C – 70°C, the protein denaturation initiated and the cellular membranes are disorganized. The viscosity of the blood increases. At 100°C, the evaporation of the interstitial liquids conducts to the destruction of the architecture of the tissue, which needs a high amount of energy. Finally, the carbonization and the pyrolyze phenomena appear. Figure 3 explains the various phenomena depending on the temperature amplitude and the time exposure [17].
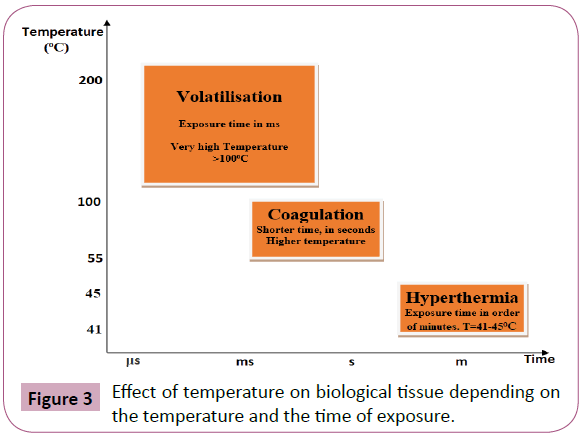
Figure 3: Effect of temperature on biological tissue depending on the temperature and the time of exposure.
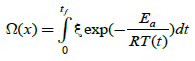
To study the tissue damage, Henriques et al. formulated a model describing damage on a porcine skin. Since that day, many researchers have investigated the tissue damage during thermal therapy [28-30]. Equation 8 gives the thermal damage.
 (8)
(8)
where ξ is the pre-exponential factor (s-1), R is the universal gas constant, 8.314 (J/(mol·K)), Ea is the activation energy to start cells kill (J/mol), and T stands for temperature (k).
Figure 4 explains the different types of energy and their interpretations in equation 1. There are three terms with positive energy, which are the conductive term, the metabolic heat, and the heating source, and one negative term due to blood convection effect. On the other side, the storage of energy is a consequence of the addition of all terms. The stored energy leads to increase the tissue temperature, which destroys the cells (Figure 4).
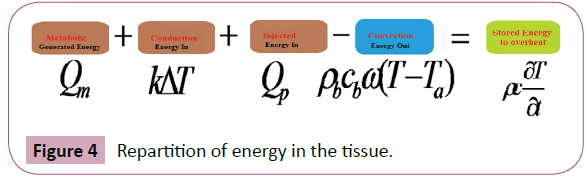
Figure 4: Repartition of energy in the tissue.
Thermal Therapy Options Applied on Oncology
Many therapeutic modalities using heat to treat cancer can be found in literature. Each modality uses different kind of clinical systems. Each modality presents advantages and limitations. We can classify these methods into invasive, non-invasive, and minimally invasive methods. The non-invasive method consists of applying an external heat source then the temperature will diffuse within the tissue to overheat the targeted area. The minimally invasive utilizes a small tip probe to inject power to kill the tumor.
This method is widely used nowadays with various modalities as RF, Laser, US, and MW. It might use intraluminal heating source or interstitial source. Other classifications are available in literature according to the nature of the heat source and other parameters.
Hyperthermia Option
Thousand years ago, man used hyperthermia to cure tumors and destroy the malignant cells [2]. It consists of raising the temperature of the whole body or a part of the body by few degrees above the normal temperature for a period that varies from few minutes to hours. The range of the temperature applied in this therapy fluctuates from 41°C to 45°C. It can be applied alone or combined with other treatment like chemotherapy, radiotherapy, surgical treatment or immunotherapy. Many clinical studies demonstrated the effectiveness of simultaneous treatment with hyperthermia and radiation [14,31-35]. The treatment process requires a heating source, thermometry system to measure the temperature evolution and a control console for adjusting the injected dose. The treatment planning guarantees the efficiency of the treatment. The heating source position differs depending on the nature of the targeted tumor. The external hyperthermia is recommended for surface tumors near to the skin, not deeper than 3-4 cm. Intraluminal hyperthermia is used for tumors near or within the body cavities as well rectum and esophagus. For the deepest tumor in the body, as well brain and liver, the interstitial hyperthermia may be efficient. This minimally invasive method uses several materials such as an RF Probe, MW antenna or LASER fiber [2,14,36].
Hyperthermia can be categorized as:
1. Local hyperthermia: Heat is applied in the small area, the purpose is to increase the temperature inside the tumor and spare the surrounding tissue. The heating source can be either external or internal. There are several approaches to overheat the tumor as well as RF, MW, and US [37]. The treatment process is accompanied with temperature measurement that can vary from invasive methods using thermometry devices to non-invasive techniques using Magnetic Resonance Imaging ( MRI) or Computed Tomography (CT). The key to the success of the treatment is the control of the injected power and an excellent location and setting of the heating source following the Hyperthermia Treatment Planning (HTP) [32,38].
2. Regional hyperthermia: The targeted region is much wider than local hyperthermia. It can be an organ or a region of the body. It is mostly used to treat deep tumors like pelvis or abdomen. This method is more complex than the first one, because of the complexity and nonhomogeneity of the targeted region [39].
3. Whole body hyperthermia: The whole body is exposed to an overheating by few degrees above the normal around 42-43°C. This kind of therapy is more complex than the local and regional hyperthermia. It is used to treat advanced metastatic cancer and some diseases like HIV. It exists many methods to heat the body among them the thermal chamber or hot water blankets [40].
Technologies for Hyperthermia
Many clinical systems are in place to hyperthermia treatment. We can find software tools and hardware tools. For the software tools, COMSOL Multiphysics and SEMCAD X are used to develop for each patient a specific planning for the treatment. They offer the possibility to combine many modules and use many geometries. With a proper set-up, we can simulate the treatment process and use the predicted model to define the injected dose [41]. The equipment used in hyperthermia occupies a significant interest for scientists and clinicians. Since the first years of raising of hyperthermia as a cancer therapy, so much commercialized equipments have been developed [3,11,14]. BDS Medical Corporation offers many versions of material for hyperthermia. The BDS-2000 3D/MR System combines the sophisticated treatment delivery and control capabilities of the Sigma Eye Applicator with the non-invasive patient and treatment monitoring capabilities of the independently operated MR imaging System [42]. In 2018, Alba Hyperthermia Systems will launch its new version of equipment for hyperthermia called ALBA 4D Deep Hyperthermia System. This system combines many approaches by using different applicators. Moreover, it includes a new system for the control of the dosimetry in real time. Also, it is equipped with an HTP software for treatment simulation [43].
Challenges of Hyperthermia
The most commonly used systems for hyperthermia are based on the EM systems. The efficiency of the treatment is evaluated by knowing if the whole targeted tumor is destroyed with a small margin of the destroyed healthy tissue surrounding the tumor. Indeed, a temperature monitoring system should be accompanied with the treatment to ensure that we reach the desired temperature without exceeding the safe threshold. Heating deeper tumors with less collateral damage is still a hot issue. Combining hyperthermai with other options is also a promising way to increase the efficiency of the treatment. For example, an hybrid method was proposed by Nizam et al. [44]. It consists of combining for the same hyperthermia treatment an EM and US system. He demonstrates, on the fantom human head, the feasibility of such approach. The biggest challenge of hyperthermia is how to monitor the temperature inside the tumor. Researchers are investigating many methods for measuring in real time the temperature while executing the treatment [41]. Thermography method based on MRI, US and CT offers the opportunity of non-surgery, but lack from true realtime and accurate feedback. In fact, after few seconds needed to take an image and do the necessary image processing than making a decision, the temperature diffuses within the tissue and changes its distribution. Another method exists based on the use of embedded thermal sensors to measure the temperature. The probe or the invasive heating source is equipped with sensors to measure the temperature locally [2,32,36,39].
Thermal Ablation Options
The ablative treatment modality means the destruction and the eradication of the tumor using temperature as an external excitation. It can be achieved in two ways: chemical or thermal. The chemical ablation uses chemical agents to coagulate and to kill the tumorous cells. The thermal ablation refers to the use of temperature to overheat the targeted tissue until its destruction. The temperature range in ablative therapies starts from 55°C and can reach 100°C. In fact, by overheating the tissue to high levels various physiological and biological phenomenon led to the destruction of this later. The ablative modality for treating cancer is used to cure many kinds of cancer like liver, kidney, rectum, lung, breast and prostate [1,20,45]. Several energy sources have been used to overheat the tissue with different approaches, invasive, minimally invasive and superficial. It includes RF, MW, LASER, US and gas for cooling in Cryotherapy [1,16,17].
To realize a successful ablation, the physicians should prepare and study the treatment. Motamedi et al. studied a cutaneous RF ablation of osteoid osteoma. They overviewed the literature and showed different steps for a successful ablation. Figure 5 shows various steps of a thermal ablation [46,47].
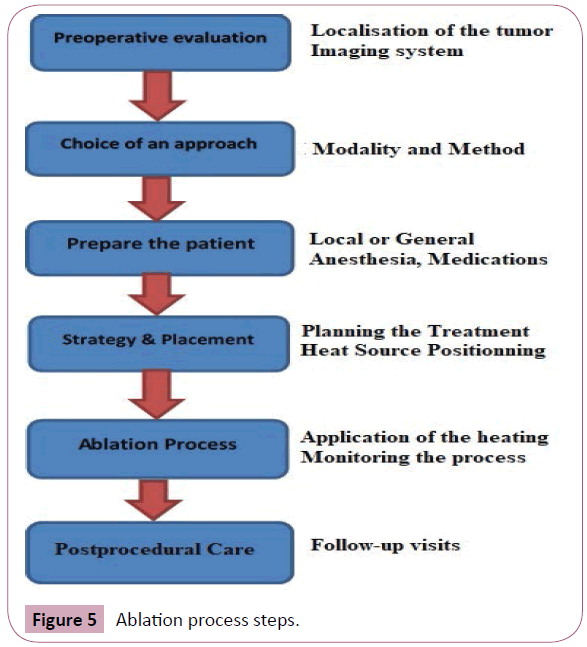
Figure 5: Ablation process steps.
An imaging system is used to check the various steps of the treatment. It can be a CT Imaging system or MR imaging system. Multiple studies proved that multiple applicators use can be more efficient where it is applicable. It can increase the effectiveness of the treatment in some cases [17,48-50].
Radio Frequency Ablation (RFA)
RFA is an ablative modality using a high-frequency heating source to kill the targeted cells. The common frequencies used in RFA vary in the range of 375-500 KHz. This modality has been widely deployed and practiced to treat cancer in many cases: liver, breast, brain [8,15,17,18,49,50]. It consists of transforming the body on a simple electrical circuit that produces a resistive heating in the surrounding tissue of the used probe [17]. In consequence, the temperature of the tissue increases due to the resistive effect and the cell death occurred. The first RF electrode was proposed in 1990 by McGahan et al. [51]. It was a monopolar electrode for hepatic ablation. Since this landmark paper, many RF Probes have been developed. We can find RFA systems with one monopolar probe, bipolar probes, or multipolar probes. The shape of the probes differs also. It can have straight needle-like, incurved or elliptical shape [20,49,50,52-55]. Different physicians use RFA to treat several diseases. The RFA has been successfully employed in many cases and still exploring new applications especially in tumor ablation. However, it also shows the effectiveness and high performance in some other circumstances as the treatment of Barrett's esophagus syndrome, varicose veins, and uterine fibroids [54,56-58]. Figure 6 shows 3 models of probes found in the literature.
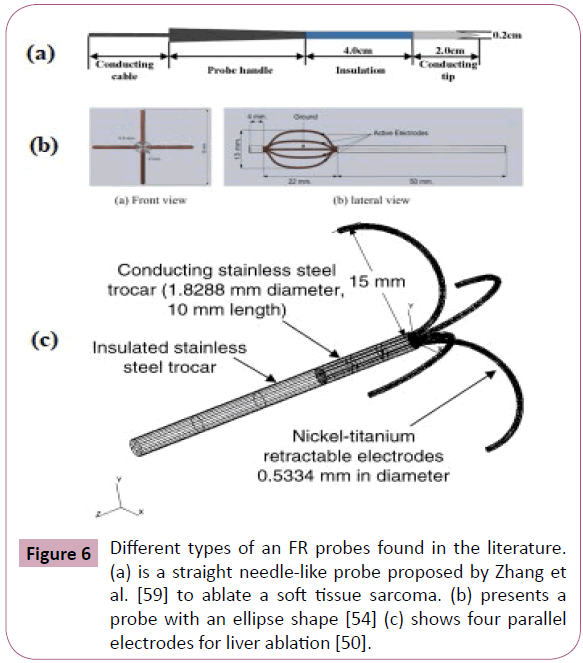
Figure 6: Different types of an FR probes found in the literature. (a) is a straight needle-like probe proposed by Zhang et al. [59] to ablate a soft tissue sarcoma. (b) presents a probe with an ellipse shape [54] (c) shows four parallel electrodes for liver ablation [50].
The research to improve the RFA is still a hot issue because it suffers from lack of precision and accuracy. For this reason, some researchers investigated the tolerated margin of the healthy tissue damaged during an RFA and the different kinds of probes [59-62]. In 2016, Idir et al. proposed a new method for more successful RFA and reduced the collateral damage of an RFA [20]. They proposed a directional probe to control the temperature diffusion direction. They simulated the ablation process of a liver tumor. They used the probe to produce a directional heat in a way to ablate just the targeted area. This probe can refine the operation with a small margin of damaged tissue. The RFA is used to eradicate tumors of various kinds. However, it is recommended for small tumors and for people who cannot support surgery [55,63]. It has received big interest as a minimally invasive technique to eradicate many types of tumor or cure some health issues in different body organs like liver, lung, bone, brain, kidney, prostate gland, pancreas, breast and so on [60,64,65].
Micro Wave Ablation (MWA)
The Micro Wave Ablation (MWA) is a thermal ablative modality, which uses Electro-Magnetic (EM) signal emitted by an antenna (or applicator) to heat the tissue and provoke a direct hyperthermic injury. The range of frequencies used in MWA begins from 915 MHz to 2.45 GHz [17,63]. It can be applied in a different way including percutaneous, laparoscopic, and open surgical access [66]. Unlike the RFA, the MWA is not an electrical current method. For this reason, the MWA is very valuable for the tissues with poor electrical conductivity like bone, kidney, and lung. Due to the nature of the used energy which is an EM radiation, the MWA can generate more uniform and larger ablation zones. It resolves some of the RFA limitations especially the increasing impedance that reduces the efficacy of the RFA [55,67]. Indeed, the heat generated by the MWA is a result of the kinetic energy of the tissue molecules after an EM excitation. The molecules, especially the water molecules, try to align with the rapid oscillating EM field. Consequently, absorption of energy is observed, which leads to tissue heating [16]. The MW heating is a deep heating, it heats tissue so efficiently. For this reason, it should be practiced with great precaution to avoid major damage [68]. MWA offers also the possibility to use multiple antennas to increase the size of the ablative zone and go deeper into the tissue [17,66]. This shortens the treatment time and gives more satisfying results what is not possible in the RFA.
High Intensity Focused Ultra Sound (HIFU)
HIFU is a hyperthermic ablation therapy that uses the principle of an Ultra Sound (US) waves. HIFU technology was proposed in 1942 by Lynn et al. [69]. The therapeutic use of the HIFU consists of sending an US beam focused on a selected area to overheat the tissue in purpose to cause a coagulation necrosis [16,70-72]. It is a highly precise treatment to kill tumors and cure some other health issues [73]. The beam is extremely oriented to a specific region of interest without causing significant collateral damage. Even when it goes through the tissue toward the targeted region, the HIFU beam does not destroy the healthy tissue [74,75]. HIFU modality knows a significant interest and growing emergence as a non-invasive treatment for solid tumors. It has been applied in the past 15 years over thousand times for several kinds of tumors [76]. HIFU treatment uses low intensity 0.125 – 3 W/cm2 to treat some physiological problem and to stimulate some functions. Intensities over 5 W/cm2 are considered as high and that can lead to the destruction of the tissue. HIFU treatment is performed under real-time monitoring with MRI or US imaging system [77]. HIFU application method can be categorized into four categories. Extracorporeal HIFU, it uses an external device. It is mostly used to treat superficial tumors. Illing e al. used an extracorporeal HIFU device to eradicate a liver and kidney tumors. They proved the safety and the feasibility of such an approach [75]. Transrectal HIFU is generally used to treat prostate cancer. Poissonnier et al. have treated 227 patients suffering from localized prostate cancer. The reported results showed an optimistic and efficient treatment with a low morbidity and fewer complications [77-79]. Interstitial HIFU treatment is recommended for deep tumors that cannot be reached with another method. This modality offers the possibility to be closer to the region of interest in a way that the injected beam will not be attenuated along the pathway [80]. It is used mostly for biliary and esophageal tumors [17]. Percutaneous HIFU treatment can be employed for deeper tumors especially in liver and kidney tumors.
The researchers make a significant focus on the HIFU modality to improve the quality of the treatment. Many scientists investigate several approaches and many application domains for the HIFU. The therapeutic applications of the US vary from sports injuries treatment and arthritis to tumor ablation therapy with HIFU technique [81]. The HIFU technique presents some unique characteristics that attract physicians and clinicians. In fact, with HIFU beam, we can elevate the temperature to 80-100°C in brief period (1-10s) without causing great damage and selectively target the tissue. Also, it offers the ability to deliver deeper to treat the deepest tumors. Moreover, it can repeatedly be applied.
LASER Ablation
A LASER (Light Amplification by Stimulated Emission of Radiation) is a monochromatic focused and directed beam of light. It is used in many applications in different fields [82]. LASER Ablation (LA) is the process of using a LASER source to deliver energy to a specific region to destroy this area. The destroyed zone depends on the beam used and other parameters related to the targeted tissue. In Oncology, LA has been used to kill tumors of different nature [63]. It has been applied to treat many kinds of cancer especially brain tumors. Because of the high compatibility with the MRI, the LA ablation is mostly monitored by an MRI imaging system. In 2017, Silva et al. used a real-time Magnetic Resonance (MR) thermometry for real-time monitoring of a Laser Interstitial Thermal Therapy (LITT) of brain tumors [83,84]. They proved the safety and effectiveness of this approach. The LA has also been applied to coagulate other cancerous tumors such as malignant hepatic, renal, pulmonary [63,85]. The destruction mechanism in LA consists of converting light into heat, which leads to the destruction of the region of interest. The conversion of the LASER beam to heat is occurred with three distinct phenomenon reflection, scattering, and absorption. Once the heat is generated, other phenomena happen to overheat the targeted volume. Conduction and Convection ensure the spread of the temperature. It is important to remind that the heat transfer by convection is negligible compared to the heat produced by the conduction [86,87].
The laser beam is characterized by its wavelength, pulse duration, pulse repetition rate and beam quality. For safer ablation, the physician should handle with all these parameters. There are so many types of laser sources, depending on the state of the used material to generate the beam: gas, liquids, solids and Light Emitting Diodes (LED). The neodymium yttrium-aluminum-garnet (Nd: YAG, the wavelength of 1064 nm) and CO2 lasers are one of the safest LASERs used in medicine [63,87,88]. The LASER beam can be delivered in continuous mode or pulsed mode. The choice of the wavelength depends on the wanted depth of the ablation. Many studies have compared different LA with various wavelengths and reported that the selection of the wavelength is directly linked the required depth of the incision [89-91]. The wavelengths used for LA starts from 560 nm to 2100 nm. The most common way to deliver a LASER beam is the use of an optical fiber. This approach has been widely used during the last decade. Adding to this, the efficacy of using optical sensors for monitoring the temperature diffusion during a LA was recently demonstrated by many studies [92-95]. In 2017, Gassino et al. developed a fully optical system for Tumor LA with an optical probe equipped with temperature real-time measurement using sensors based on Fiber Bragg Gratings (FBGs) [96]. The results obtained showed that the thermal pattern corresponds to the desired shape. Furthermore, the temperature measurement was not an estimated value, as it is with the US and MRI imaging, but a real-time measurement.
Low-Level Laser Therapy (LLLT) is also another therapeutic method used to treat a different kind on health issues. It uses a low-intensity Laser to provide a potential treatment. This approach has been used to treat hair loss, rheumatic problems, pain relief, and enhance muscle strength [97,98]. Like other modalities, the LA has advantages and limitations in some applications. Table 1 gives the high and low points of this modality.
| Advantages |
Inconvenient |
Minimally invasive. Recommended for people do not support surgery.
Safe modality
Less time
Repeatability of |
Not efficient for larger tumors
The excessive cost
Not requested for complex tumors |
Table 1: Advantages and inconvenient of the LA.
Cryoablation
Contrary to the four precedent therapies (RFA, MWA, HIFU, and LA), the cryotherapy uses a low temperature below zero to create a freezing zone and generate the destruction of the selected region [99]. It uses extremely low lethal temperature < -20°C. The mechanism of destruction of the tissue is complex and occurs at different temperature levels. The time of treatment in Cryoablation varies from seconds to tens of minutes. Baust et al. reviewed the Cryoablation therapy [100]. They investigated the cell destruction mechanism. They reported different definition proposed to define the “Cryosurgical ablative dose.” They showed the various applications of the Cryoablation in cancer treatment and other diseases. According to some studies, if the targeted cells are exposed to a low temperature of −30 to −40°C for approximately ≥1 min, we can notice almost total cell destruction. The Cryoablation is performed with a probe that delivers a low temperature to the region of interest. The probe tip is alimented by a source of nitrogen or argon for cooling the tissue to a low temperature -100°C produced by different kinds of cooling probes.
The Cryoablation has shown many benefits in several medical applications. For cancer treatment, it has been widely exploited to ablate many types of tumor. This modality offers highly efficient in the treatment of some cases of cancer where the patient is not a candidate for surgical treatment. However, it suffers from the complication of the freezing tissue. Improving this modality is a present research issue.
Discussion and Comparison
The RFA is the most used ablative modality. The MWA is gaining interest because it overpasses the limitations of the RFA. In fact, the impedance effect and the resection effect represent a practical problem for the RFA. In MWA, those limitations are resolved. Adding to this, the MWA is suitable to treat the large tumors >5 cm what is not recommended for the RFA [63]. One of the best advantages of the MWA is the size of the active zone, which is up to 2 cm surrounding the antenna. Furthermore, the possibility to use simultaneous multiple antennas to enlarge the ablative zone. On the other side, LA continues to expand and improve. It offers some advantages, but it suffers mainly from practical limitations especially the excessive cost of treatment. For the HIFU ablation, its main advantages are the ability to focus the beam to a limited area and the high level of safety for the patient.
The use of an imaging system is recommended for the placement of the needle or probe and the monitoring of the ablation process, which consists of taking consecutive images to follow up the temperature diffusion. This is a crucial factor for a successful treatment. These systems can be of different nature, CT, MRI or US. Hegg et al. performed 19 renal tumors RFA guided with an US imaging system. They reported no major complication after the treatment. They exploited the major advantages of the US-guided approach to achieve a safe and efficient ablation. The US-guided approach intervenes in important moments to place the probes accurately in the right position and evaluate the proximity to the adjacent critical structure. Moreover, it allows a real-time monitoring of the ablation process, which is crucial step to avoid a significant collateral damage. The choice of the optimal modality to get the best treatment results is done after considering many parameters. Hinshaw et al. overviewed the percutaneous tumor ablation modalities. They investigated the RFA, MWA, and CA. They focused on the methodology used to choose the appropriate modality for a tumor ablation to have an optimizing clinical result. According to their findings, there are many parameters for optimal ablation. Some of them are relating to the operator ability, others concern the material and the modality used. The choice of the ablation modality, hot (RFA, MWA, LA, HIFU) or cold (CA), is made considering many factors. First, the previous similar ablations should be studied and compared to see which modality is safer and riskless to the patient. Further, the morbidity of the patient, the type, and size of the tumor, as well as its proximity to vulnerable organs should be examined. They reported the most used method for few organs and compared these methods. One of the important parameter to compare the thermal modalities is the number and nature of the post-procedural complications. In fact, following many studies, the complication noticed, major or minor, are the lowest rate in the FRA modality comparing to the other modalities with many similarities with MWA. A recent study in 2017 by Luo et al. compared the therapeutic effects of the RFA with other ablative modalities on Hepatocellular Carcinoma (HCC). Many parameters including a Complete Tumor Ablation (CTA), Local Tumor Recurrence (LTR), Overall Survival (OS) and complications of the treatment were defined and compared. The authors selected the most 30 original and high-quality studies among the 2675 initial published studies found in the literature. They concluded that RFA has less complication comparing to the MWA, CA. The most commonly mentioned complication is the fever, which is more important in MWA (because of the deep heating) and less in RFA and LA. The CTA is achieved similarly in RFA and MWA with lower rates in CA and LA. Many other studies have compared the RFA with other modalities for treating the HCC or other tumors. They have compared the clinical results and reported evidence of efficacy and effectiveness. Sharma et al. compared the non-invasive HIFU with RFA of Osteoid Osteoma and showed the similarity of the clinical results and the advantage of the HIFU by offering a non-invasive procedure. Nou- Eldin et al. retrospectively compared the local tumor response and the survival rates of three ablation modalities (LITT, RFA, and MWA) of a non-colorectal lung tumor ablation. They followed up 109 patients in 175 CT-guided ablation sessions. The authors proved that the three modalities present an efficient therapy with approximately similar clinical results with some advantages for the MWA [101-105]. Table 2 summarizes the most used and typical characteristics, benefits, and some limitations of the discussed thermal ablative modalities.
| Description \ Modality |
RFA |
MWA |
LA |
HIFU |
CA |
| Heating Principles |
Resistive by RF alternating current |
Propagating high frequency EM waves |
Convert Laser beam to heat |
Focused US beams to heat the tissue |
Freeze selected region to destroy the tissue |
| Frequency/Wavelength |
375-550 KHz |
915MHz-2.45GHz |
560nm to 2100nm. |
200KHz-3.5MHz |
Uses gas to freeze |
| Temperature Range |
55-100°C |
55-100°C |
50-100°C |
70-100°C |
<-30°C |
| Exposure Time |
Few to tens min |
1 to 5 min |
Few min (3min) |
1 to 10 s |
7 to 30 min |
| Thermometry Method |
MRI, US or CT |
MRI, US or CT |
MRI, US or CT |
US |
CT, US or MRI |
| Electrodes |
Single or multiple probe |
One or more antennas |
Directed (or not) fiber probe |
US Array |
Nitrogen or argon based Cryoprobe |
| Advantages |
Minimal invasive
Simple and Easy
Effective
Worldwide availability
Less complications
Many robust systems |
Minimal invasive
Local target
Overpass the RF limits
Large ablative zone
Elevated temperature in small time |
Minimal invasive
Easy configuration of the LASER
High Precision |
Non-invasive
Focused lesion
Repeatability
Compatibility with other therapies
Depth of penetration |
Minimal invasive
No carbonization
Large lesion |
| Limitations |
Impedance problem
Small ablation zone
Low precision |
More complications
Coaxial cable heating
Lack of directionality |
Small ablative zone
Expensive price
More Complications
Low survival rate |
Quality of the small transducers
Long ablation time
Need acoustic coupling |
High complications rates
Difficulty in placing the probes
High risk of bleeding |
Table 2: Description and characteristics of the thermal ablative modalities.
Future Perspectives
The thermal therapy has proved its effectiveness and efficacy in many medical applications. Oncology is the most popular field where the thermal therapy has been widely exploited. Despite all the technological improvement, the thermal therapy still has problems and limitations in clinical applications.
The hyperthermia treatment suffers from lack of precision by causing considerable margin damage, which is not suitable and not tolerable especially in some organs such as brain. This therapy is usually combined with other types of treatment, which is another way for researchers to improve the quality of the treatment. In addition to hyperthermia, the thermal ablative modalities which are RFA, MWA, LA, HIFU and CA also present several inconveniences and many clinical limitations. So, all these limitations and disadvantages present significant challenges for physicians, engineers, and designers. The factors to improve the thermal therapy can be divided according to their nature to hardware systems, software tools, mathematical modeling, and imaging systems for thermography and placement. We can categorize these particular challenges of the thermal therapy into the following:
Software Tools
1. Development of powerful planning tools to prepare and optimize the treatment.
2. Invest in new modeling and simulation tools with a more realistic model based on the real architectures and real parameters.
3. Combination of different therapies with distinct modalities to improve the performances of the treatment.
4. The non-uniform shape of the tumors should be investigated and explored to reduce the margin damage in the healthy encircling tissue.
Considering the non-homogenous of the tumor.
Hardware Systems
1. Improve hardware systems by improving the devices and including more facilities and options to achieve safer and comfortable treatment.
2. Design a better electrodes and heating source with more flexibility in use and simplicity to configure. The parameters which define the heating activity should be programmable to adjust the heating source easily.
3. Invest and explore the use of multi-electrodes to increase the volume of the ablative zone and to ensure a total ablation of the tumors, particularly with the MWA, which presents promising opportunities.
4. Local parametrisation of the tumor parameters using a special probe to define the needed parameters. The collected data will be utilized in modeling and simulation of the treatment process instead of using approximated data.
Mathematical Modeling
1. Modification of the Pennes’ model for a better description of the temperature distribution in living tissue.
2. Explore new BHT models other than Pennes’ model.
Imaging and Thermometry
1. Employ the imaging systems like CT, US or MRI to place the electrodes in the right position, inject the power and follow-up the temperature distribution.
2. Improve the existing imaging systems.
3. Explore and improve the use of sensors (optical or MEMS) to measure the real temperature locally in true real time instead of estimating the value using image processing tools.
References
- Bai JF, Liu P, Xu LX (2014) Recent advances in thermal treatment techniques and thermally induced immune responses against cancer. IEEE Transactions on Biomedical Engineering 61: 1497-1505.
- Glazer ES, Curley SA (2011) The ongoing history of thermal therapy for cancer. Surgical Oncology Clinics of North America 20: 229-235.
- Roussakow S (2013) The history of hyperthermia rise and decline. Conference Papers in Science, Hindawi Publishing Corporation, Egypt.
- Habash RW, Bansal R, Krewski D, Alhafid HT (2006) Thermal therapy, part 1: An introduction to thermal therapy. Crit Rev Biomed Eng 34: 491-542.
- World Health Organization (2017) Cancer: Fact Sheet – February 2017. [https://www.who.int/mediacentre/factsheets/fs297/en/]
- Siegel RL, Miller KD, Jemal A (2016) Cancer statistics, 2016. CA Cancer J Clin 66: 7-30.
- Ahmed M (2013) Introduction to special issue on tumor ablation. Tech Vasc Interv Radiol 16: 191.
- Deschamps F, Farouil G, Ternes N, Gaudin A, Hakime A (2014) Thermal ablation techniques: a curative treatment of bone metastases in selected patients? European Radiology 24: 1971-1980.
- Huang HW, Liauh CT (2012) Review: Therapeutical applications of heat in cancer therapy. J Med Biol Eng 32: 1-10.
- Miller DL, Smith NB, Bailey MR, Czarnota GJ, Hynynen K, et al. (2012) Overview of therapeutic ultrasound applications and safety considerations. J Ultrasound Med 31: 623-634.
- Stauffer PR (2005) Evolving technology for thermal therapy of cancer. Int J Hyperthermia 21: 731-744.
- Baltzer AWA, Stosch D, Seidel F, Ostapczuk MS (2017) Low level laser therapy: A narrative literature review on the efficacy in the treatment of rheumatic orthopaedic conditions. Z Rheumatol 76(9): 806-812.
- Roemer RB (1999) Engineering aspects of hyperthermia therapy. Annual Review of Biomedical Engineering 1: 347-376.
- Habash RW, Bansal R, Krewski D, Alhafid HT (2006) Thermal therapy, part 2: hyperthermia techniques. Crit Rev Biomed Eng 34: 491-542.
- Stauffer PR, Goldberg SN (2004) Introduction: Thermal ablation therapy. Int J Hyperthermia 20: 671-677.
- Chu KF, Dupuy DE (2014) Thermal ablation of tumours: biological mechanisms and advances in therapy. Nat Rev Cancer 14: 199-208.
- Knavel EM, Brace CL (2013) Tumor ablation: Common modalities and general practices. Tech Vasc Interv Radiol 16: 192-200.
- Ryan MJ, Willatt J, Majdalany BS, Kielar AZ, Chong S, et al. (2016) Ablation techniques for primary and metastatic liver tumors. World J Hepatol 8: 191-199.
- Pennes HH (1948) Analysis of tissue and arterial blood temperatures in the resting human forearm. J Appl Physiol 1: 93-122.
- Mellal I, Kengne E, El Guemhioui KE, Lakhssassi A (2016) 3D modeling using the finite element method for directional removal of a cancerous tumor. J Biomedical Sci 5: 4.
- Becker S, Kuznetsov A (2014) Heat transfer and fluid flow in biological processes. 2014. 1st Edition, Elsevier.
- Beriat GK, Akmansu SH, Ezerarslan H, Dogan C, Han U, et al. (2012) The comparison of thermal tissue injuries caused by ultrasonic scalpel and electrocautery use in rabbit tongue tissue. Bosn J Basic Med Sci 12: 151-157.
- Atiyeh BS, Gunn SW, Hayek SN (2005) State of the art in burn treatment. World J Surgery 29: 131-148.
- Martimbianco AL, Gomes da Silva BN, de Carvalho AP, Silva V, Torloni MR, et al. (2014) Effectiveness and safety of cryotherapy after arthroscopic anterior cruciate ligament reconstruction. A systematic review of the literature. Phys Ther Sport 15: 261-268.
- Wu S, Hou J, Ding Y, Wu F, Hu Y, et al. (2015) Cryoablation versus radiofrequency ablation for hepatic malignancies: a systematic review and literature-based analysis. Medicine (Baltimore) 94: e2252.
- Yarmolenko PS, Moon EJ, Landon C, Manzoor A, Hochman DW, et al. (2011) Thresholds for thermal damage to normal tissues: An update. Int J Hyperthermia 27: 320-343.
- Chu KF, Dupuy DE (2014) Thermal ablation of tumours: biological mechanisms and advances in therapy. Nat Rev Cancer 14: 199.
- Henriques Jr F, Moritz A (1947) Studies of thermal injury: I. The conduction of heat to and through skin and the temperatures attained therein. A theoretical and an experimental investigation. Am J Pathol 23: 530-549.
- Dewey WC (2009) Arrhenius relationships from the molecule and cell to the clinic. Int J Hyperthermia 25: 3-20.
- Garcia PA, Davalos RV, Miklavcic D (2014) A numerical investigation of the electric and thermal cell kill distributions in electroporation-based therapies in tissue. PloS One 9: e103083.
- Seifert G, Budach V, Keilholz U, Ghadjar P (2016) Regional hyperthermia combined with chemotherapy in paediatric, adolescent and young adult patients: current and future perspectives. Radiation Oncology 11: 65.
- Datta NR, Ordóñez SG, Gaipl US, Paulides MM, Crezee H, et al. (2015) Local hyperthermia combined with radiotherapy and-/or chemotherapy: Recent advances and promises for the future. Cancer Treat Rev 41: 742-753.
- Trefná HD, Martinsson B, Petersson T, Renstrom N, Torstensson M, et al. (2017) Multifrequency approach in hyperthermia treatment planning: Impact of frequency on SAR distribution in head and neck. 11th European Conference on Antennas and Propagation (EUCAP) 2017: 3710-3712.
- Wust P, Hildebrandt B, Sreenivasa G, Rau B, Gellermann J, et al. (2002) Hyperthermia in combined treatment of cancer. Lancet Oncol 3: 487-497.
- van der Zee J, González González D, van Rhoon GC, van Dijk JD, van Putten WL, et al. (2000) Comparison of radiotherapy alone with radiotherapy plus hyperthermia in locally advanced pelvic tumours: a prospective, randomised, multicentre trial. Lancet 355: 1119-1125.
- Kok HP, Wust P, Stauffer PR, Bardati F, van Rhoon GC, et al. (2015) Current state of the art of regional hyperthermia treatment planning: a review. Radiat Oncol 10: 196.
- Aziz MNC, Salim MIM, Wahab AA, Manaf NA (2015) A feasibility study of ultrasound as a monitoring method for hyperthermia therapy. 2015 IEEE Student Conference on Research and Development (SCOReD).
- Gao S, Zheng M, Ren X, Tang Y, Liang X (2016) Local hyperthermia in head and neck cancer: mechanism, application and advance. Oncotarget 7: 57367-57378.
- Paulides MM, Bakker JF, Linthorst M, van der Zee J, Rijnen Z, et al. (2010) The clinical feasibility of deep hyperthermia treatment in the head and neck: new challenges for positioning and temperature measurement. Phys Med Biol 55: 2465-2480.
- Suvernev AV, Ivanov GV, Efremov AV, Tchervov R (2006) Whole body hypothermia at 43.5–44 C: Dreams or Reality? In: Baronzio G and Hager ED (eds) Hyperthermia in Cancer Treatment: A Primer. Springer, Dordrecht, 227-236.
- Sardari D, Verga N (2011) Cancer treatment with hyperthermia. Current Cancer Treatment-Novel Beyond Conventional Approaches, InTech, Croatia.
- Wilkens D (2017) BSD-2000 Microwave Hyperthermia System [https://www.pyrexar.com/hyperthermia/bsd-2000].
- Solutions SI (2017) ALBA Hyperthermia System products, ALBA 4D, Double ON4000, ON4000, ALBA HPA 434 MHz amplifiers/generator [https://www.albahyperthermia.com/hyperthermia-products.html].
- Nizam-Uddin N, Elshafiey I (2017) Enhanced Energy Localization in Hyperthermia Treatment Based on Hybrid Electromagnetic and Ultrasonic System: Proof of Concept with Numerical Simulations. BioMed Research International 2017: 5787484.
- Kang TW, Rhim H (2015) Recent advances in tumor ablation for hepatocellular carcinoma. Liver Cancer 4: 176-187.
- Motamedi D, Learch TJ, Ishimitsu DN, Motamedi K, Katz MD, et al. (2009) Thermal ablation of osteoid osteoma: overview and step-by-step guide. Radiographics 29: 2127-2141.
- Brace CL, Hinshaw JL, Lubner MG (2011) Thermal ablation for the treatment of abdominal tumors. J Visualized Experiments: JoVE.
- Littrup PJ, Jallad B, Vorugu V, Littrup G, Currier B, et al. (2009) Lethal isotherms of cryoablation in a phantom study: effects of heat load, probe size, and number. J Vasc Interv Radiol 20: 1343-1351.
- Lee J, Lee JM, Yoon JH, Lee JY, Kim SH, et al. Percutaneous radiofrequency ablation with multiple electrodes for medium-sized hepatocellular carcinomas. Korean J Radiol 13: 34-43.
- Mulier S, Jiang Y, Wang C, Jamart J, Marchal G, et al. (2012) Bipolar radiofrequency ablation with four electrodes: Ex vivo liver experiments and finite element method analysis. Influence of inter-electrode distance on coagulation size and geometry. Int J Hyperthermia 28: 686-697.
- McGahan JP, Browning PD, Brock JM, Tesluk H (1990) Hepatic ablation using radiofrequency electrocautery. Invest Radiol 25: 267-270.
- Mulier S, Jiang Y, Jamart J, Wang C, Feng Y, et al. (2015) Bipolar radiofrequency ablation with 2 × 2 electrodes as a building block for matrix radiofrequency ablation: Ex vivo liver experiments and finite element method modelling. Int J Hyperthermia 31: 649-665.
- Tungjitkusolmun S, Staelin ST, Haemmerich D (2002) Three-dimensional finite-element analyses for radio-frequency hepatic tumor ablation. IEEE transactions on Biomedical Engineering 49: 3-9.
- Ruxsapong P, Phasukkit P, Tungjitkusolmun S (2013) Airflow analysis of radiofrequency ablation for asthma therapy by using 3D finite element method. 6th Biomedical Engineering International Conference (BMEiCON).
- Ni Y, Mulier S, Miao Y, Michel L, Marchal G (2005) A review of the general aspects of radiofrequency ablation. Abdom Imaging 30: 381-400.
- Almeida JI, Raines JK (2006) Radiofrequency ablation and laser ablation in the treatment of varicose veins. Ann Vasc Surg 20: 547-552.
- Shaheen NJ, Sharma P, Overholt BF, Wolfsen HC, Sampliner RE, et al. (2009) Radiofrequency ablation in Barrett's esophagus with dysplasia. N Engl J Med 360: 2277-2288.
- Lee BB (2002) Radiofrequency Ablation of Uterine Leiomyomata: A New Minimally Invasive Hysterectomy Alternative. Obstet Gynecol 99: 9S.
- Zhang R, Liu H, Li H (2014) Finite element analysis of radiofrequency ablation process in soft tissue sarcomas. 4th IEEE International Conference on Information Science and Technology.
- Singh S, Bhowmik A, Repaka R (2016) Thermal analysis of induced damage to the healthy cell during RFA of breast tumor. J Therm Biol 58: 80-90.
- Kim YS, Lee WJ, Rhim H, Lim HK, Choi D, et al. (2010) The minimal ablative margin of radiofrequency ablation of hepatocellular carcinoma (> 2 and < 5 cm) needed to prevent local tumor progression: 3D quantitative assessment using CT image fusion. AJR Am J Roentgenol 195: 758-765.
- Wang XL, Li K, Su ZZ, Huang ZP, Wang P, et al. (2015) Assessment of radiofrequency ablation margin by MRI-MRI image fusion in hepatocellular carcinoma. World J Gastroenterol 21: 5345-5351.
- Habash RW, Bansal R, Krewski D. Thermal therapy, Part III: ablation techniques. Crit Rev Biomed Eng 2007;35(1-2).
- Mirza AN, Fornage BD, Sneige N, Kuerer HM, Newman LA (2000) Radiofrequency ablation of solid tumors. Cancer J 7: 95-102.
- Zhao W, Chen JZ, Hu JH, Huang JQ, Jiang YN, et al. (2017) In vivo effects of radiofrequency ablation on long bones and the repair process in swine models. Jpn J Radiol 35: 31-39.
- Lubner MG, Brace CL, Hinshaw JL, Lee FT Jr. (2010) Microwave tumor ablation: mechanism of action, clinical results, and devices. J Vasc Interv Radiol 21: S192-S203.
- Salati U, Barry A, Chou FY, Ma R, Liu DM (2017) State of the ablation nation: a review of ablative therapies for cure in the treatment of hepatocellular carcinoma. Future Oncol 13: 1437-1448.
- Martin RC, Scoggins CR, McMasters KM (2010) Safety and efficacy of microwave ablation of hepatic tumors: A prospective review of a 5-year experience. Ann Surg Oncol 17: 171-178.
- Lynn JG, Zwemer RL, Chick AJ, Miller AE (1942) A new method for the generation and use of focused ultrasound in experimental biology. J Gen Physiol 26: 179-193.
- Köhler MO, Mougenot C, Quesson B, Enholm J, Le Bail B, et al. (2009) Volumetric HIFU ablation under 3D guidance of rapid MRI thermometry. Med Phys 36: 3521-3535.
- Zhang L, Wang ZB (2010) High-intensity focused ultrasound tumor ablation: Review of ten years of clinical experience. Front Med China 4: 294-302.
- Dubinsky TJ, Cuevas C, Dighe MK, Kolokythas O, Hwang JH (2008) High-intensity focused ultrasound: current potential and oncologic applications. AJR Am J Roentgenol 190: 191-199.
- Lang BHH, Wu ALH (2017) High Intensity Focused Ultrasound (HIFU) ablation of benign thyroid nodules – a systematic review. J Ther Ultrasound 5: 11.
- Karaboce B (2016) Investigation of thermal effect by focused ultrasound in cancer treatment. IEEE Instrumentation & Measurement Magazine 19: 20-64.
- Illing RO, Kennedy JE, Wu F, ter Haar GR, Protheroe AS, et al. (2005) The safety and feasibility of extracorporeal High-Intensity Focused Ultrasound (HIFU) for the treatment of liver and kidney tumours in a Western population. Br J Cancer 93: 890-895.
- Zhou Y (2014) High-intensity focused ultrasound treatment for advanced pancreatic cancer. Gastroenterology Research and Practice 2014: 205325.
- Gelet A, Crouzet S, Rouviere O, Chapelon JY (2017) High-Intensity Focused Ultrasound (HIFU) for Prostate Cancer. In: Bolla M and van Poppel H (eds) Management of Prostate Cancer: A Multidisciplinary Approach. Springer International Publishing, 251-272.
- Crouzet S, Rouviere O, Martin X, Gelet A (2014) High-intensity focused ultrasound as focal therapy of prostate cancer. Curr Opin Urol 24: 225-230.
- Poissonnier L, Chapelon JY, Rouviere O, Curiel L, Bouvier R, et al. (2007) Control of prostate cancer by transrectal HIFU in 227 patients. Eur Urol 51: 381-387.
- Lafon C, Melodelima D, Salomir R, Chapelon JY (2007) Interstitial devices for minimally invasive thermal ablation by high-intensity ultrasound. Int J Hyperthermia 23: 153-163.
- Izadifar Z, Babyn P, Chapman D (2016) Applications and safety of therapeutic ultrasound: Current trends and future potential. Clin Res Open Access.
- Jakubczak K (2011) Lasers-Applications in science and industry. InTech.
- Schwartz JA, Shetty AM, Price RE, Stafford RJ, Wang JC, et al. (2009) Feasibility study of particle-assisted laser ablation of brain tumors in orthotopic canine model. Cancer Res 69: 1659-1667.
- Carpentier A, McNichols RJ, Stafford RJ, Itzcovitz J, Guichard JP, et al. (2008) Real-time magnetic resonance-guided laser thermal therapy for focal metastatic brain tumors. Neurosurgery 63: ONS21-28.
- Shi Y, Mao Y (2017) Magnetic resonance thermometry–guided laser interstitial thermal therapy in neurosurgery, a promising tool for dural-based lesions? World Neurosurgery 98: 836-838.
- Ansari MA, Erfanzadeh M, Mohajerani E (2013) Mechanisms of Laser-Tissue Interaction: II. Tissue Thermal Properties. J Lasers Med Sci 4: 99-106.
- Steiner R (2011) Laser-tissue interactions. Laser and IPL Technology in Dermatology and Aesthetic Medicine, Springer.
- Sierra H, Cordova M, Nehal K (2016) Laser ablation of basal cell carcinomas guided by confocal microscopy. Proc. of SPIE.
- Fornaini C, Merigo E, Sozzi M, Rocca JP, Poli F, et al. (2016) Four different diode lasers comparison on soft tissues surgery: a preliminary ex vivo study. Laser Ther 25: 105-114.
- Schena E, Saccomandi P, Fong Y (2017) Laser ablation for cancer: Past, present and future. J Funct Biomater 8: 19.
- Kim B, Kim DY (2016) Enhanced tissue ablation efficiency with a mid-infrared nonlinear frequency conversion laser system and tissue interaction monitoring using optical coherence tomography. Sensors 16: 598.
- Pacella CM, Papini E (2017) Ultrasound-Guided Laser Ablation. Advanced Thyroid and Parathyroid Ultrasound, 391-401.
- Tosi D, Macchi EG, Braschi G, Cigada A, Gallati M, et al. (2014) Fiber-optic combined FPI/FBG sensors for monitoring of radiofrequency thermal ablation of liver tumors: ex vivo experiments. Applied Optics 53: 2136-2144.
- Palumbo G, Tosi D, Schena E, Massaroni C, Ippolito J, et al. (2017) Real-time temperature monitoring during radiofrequency treatments on ex-vivo animal model by Fiber Bragg grating sensors. SPIE Optics + Optoelectronics, Prague, Czech Republic.
- Schena E, Tosi D, Saccomandi P, Lewis E, Kim T (2016) Fiber Optic Sensors for Temperature Monitoring during Thermal Treatments: An Overview. Sensors 16: E1144.
- Gassino R, Liu Y, Konstantaki M (2017) A fiber optic probe for tumor laser ablation with integrated temperature measurement capability. Journal of Lightwave Technology 35(16): 3447-3454.
- Zarei M, Wikramanayake TC, Falto-Aizpurua L, Schachner LA, Jimenez JJ (2016) Low level laser therapy and hair regrowth: an evidence-based review. Lasers Med Sci 31: 363-371.
- Landucci A, Wosny AC, Uetanabaro LC, Moro A, Araujo MR (2016) Efficacy of a single dose of low-level laser therapy in reducing pain, swelling, and trismus following third molar extraction surgery. Int J Oral Maxillofac Surg 45: 392-398.
- Maccini M, Sehrt D, Pompeo A, Chicoli FA, Molina WR, et al. (2011) Biophysiologic considerations in cryoablation: a practical mechanistic molecular review. Int Braz J Urol 37: 693-696.
- Baust JG, Gage AA, Bjerklund Johansen TE, Baust JM (2014) Mechanisms of cryoablation: clinical consequences on malignant tumors. Cryobiology 68: 1-11.
- Hegg RM, Schmit GD, Kurup AN, Weisbrod AJ, Boorjian SA, et al. (2014) Ultrasound-Guided Transhepatic Radiofrequency Ablation of Renal Tumors: A Safe and Effective Approach. Cardiovasc Intervent Radio 37: 508-512.
- Hinshaw JL, Lubner MG, Ziemlewicz TJ, Lee FT Jr, Brace CL (2014) Percutaneous Tumor Ablation Tools: Microwave, Radiofrequency, or Cryoablation—What Should You Use and Why? RadioGraphics 34: 1344-1362.
- Luo W, Zhang Y, He G, Yu M, Zheng M, et al. (2017) Effects of radiofrequency ablation versus other ablating techniques on hepatocellular carcinomas: a systematic review and meta-analysis. World J Surg Oncol 15: 126.
- Sharma KV, Yarmolenko PS, Celik H, Eranki A, Partanen A, et al. (2017) Comparison of Noninvasive High-Intensity Focused Ultrasound with Radiofrequency Ablation of Osteoid Osteoma. J Pediatr 190: 222-228.
- Nour-Eldin NEA, Exner S, Al-Subhi M, N. Naguib NN, Kaltenbach B (2017) Ablation therapy of non-colorectal cancer lung metastases: retrospective analysis of tumour response post-laser-induced interstitial thermotherapy (LITT), radiofrequency ablation (RFA) and microwave ablation (MWA). Int J Hyperthermia 33: 820-829.