
Abstract
Background and Objective: We previously reported that risedronate improved the structural parameters of the proximal femur, as well as lumbar spine and proximal femoral bone mineral density (BMD), after 1 year of therapy by suppressing bone resorption in patients with an increased risk of fracture. Our practice-based observational study was subsequently extended to determine whether these effects were enhanced, maintained or attenuated after 3 years.
Methods: A total of 174 patients (nine men and 165 postmenopausal women) with a mean age of 67.8 years who had osteoporosis or osteopenia and clinical risk factors for fracture started risedronate therapy. The BMD of the lumbar spine and proximal femur, as well as proximal femoral structural parameters, were evaluated by dual-energy x-ray absorptiometry with advanced hip assessment (AHA) software at baseline and every year for 3 years.
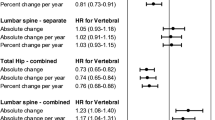
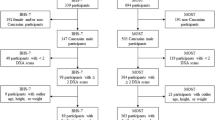
Results: Data were available for 107 patients at 1 year, 80 patients at 2 years and 74 patients at 3 years. Lumbar spine, total hip and femoral neck BMD and the cross-sectional area (CSA) of the proximal femur increased from baseline after 1 year with levels being maintained after 2–3 years. The crosssectional moment of inertia (CSMI) of the proximal femur increased from baseline after 1 year and the increase was enhanced after 2 years with levels being maintained after 3 years. The femoral strength index (FSI) increased from baseline after 1 and 2 years and the increase was enhanced after 3 years. The increases in proximal femoral CSMI and FSI were greater than those of total hip and femoral neck BMD after 3 years of therapy.
Conclusion: The present study showed the effects of risedronate therapy for 3 years on the BMD of the lumbar spine and proximal femur, as well as on proximal femoral structure, in patients with an increased risk for fracture.



Similar content being viewed by others
References
NIH Consensus Development Panel. Osteoporosis prevention, diagnosis, and therapy. JAMA 2001; 285: 785–95
Reginster J, Minne HW, Sorensen OH, et al. Randomized trial of the effects of risedronate on vertebral fractures in women with established postmenopausal osteoporosis. Vertebral Efficacy with Risedronate Therapy (VERT) Study Group. Osteoporos Int 2000; 11: 83–91
Harris ST, Watts NB, Genant HK, et al. Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. Vertebral Efficacy with Risedronate Therapy (VERT) Study Group. JAMA 1999; 282: 1344–52
McClung MR, Geusens P, Miller PD, et al. Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med 2001; 344: 333–40
Wells G, Cranney A, Peterson J, et al. Risedronate for the primary and secondary prevention of osteoporotic fractures in postmenopausal women. Cochrane Database Syst Rev 2008; 23(1): CD004523
Zhong ZM, Chen JT. Anti-fracture efficacy of risedronic acid in men: a meta-analysis of randomized controlled trials. Clin Drug Investig 2009; 29: 349–57
Yoshikawa T, Turner CH, Peacock M, et al. Geometric structure of the femoral neck measured using dual-energy-X-ray absorptiometry. J Bone Miner Res 1994; 9: 1053–64
Takakuwa M, Iwamoto J, Konishi M, et al. Risedronate improves proximal femur bone density and geometry in patients with osteoporosis or osteopenia and clinical risk factors of fractures: a practice-based observational study. J Bone Miner Metab 2011; 29: 88–95
Shiraki M, Fukunaga M, Kushida K, et al. A double-blind dose-ranging study of risedronate in Japanese patients with osteoporosis (a study by the Risedronate Late Phase II Research Group). Osteoporos Int 2003; 14: 225–34
Kishimoto H, Fukunaga M, Kushida K, et al. Efficacy and tolerability of once-weekly administration of 17.5 mg risedronate in Japanese patients with involutional osteoporosis: a comparison with 2.5-mg once-daily dosage regimen. J Bone Miner Metab 2006; 24: 405–13
Orimo H, Sugioka Y, Fukunaga M, et al. Diagnostic criteria of primary osteoporosis. J Bone Miner Metab 1998; 16: 139–50
Orimo H, Hayashi Y, Fukunaga M, et al. Diagnostic criteria for primary osteoporosis: year 2000 revision. J Bone Miner Metab 2001; 19: 331–7
Orimo H. Japanese guideline for prevention and treatment of osteoporosis. Life Science 2006 (in Japanese)
Xu H, Li J, Wu Q, Zhou Q. The correlation between DXA femur strength index and QUS heel stiffness index in Chinese women. ASBMR Annual Meeting, Montreal (QC) 2008: M464
Shepherd JA, Fan B, Lu Y, et al. Comparison of BMD precision for Prodigy and Delphi spine and femur scans. Osteoporos Int 2006; 17: 1303–8
Fukunaga M, Kushida K, Kishimoto H, et al. A comparison of the effect of risedronate and etidronate on lumbar bone mineral density in Japanese patients with osteoporosis: a randomized controlled trial. Osteoporos Int 2002; 13: 971–9
Melton III LJ, Beck TJ, Amin S, et al. Contributions of bone density and structure to fracture risk assessment in men and women. Osteoporos Int 2005; 16: 460–7
Greenspan SL, Beck TJ, Resnick NM, et al. Effect of hormone replacement, alendronate, or combination therapy on hip structural geometry: a 3-year, double blind, placebo controlled clinical trial. J Bone Miner Res 2005; 20: 1525–32
Bonnick SL, Beck TJ, Cosman F, et al. DXA-based hip structural analysis of once-weekly bisphosphonate-treated postmenopausal women with low bone mass. Osteoporos Int 2009; 20: 911–21
Iwamoto J, Sato Y, Takeda T, et al. Hip fracture protection by alendronate treatment in postmenopausal women with osteoporosis: a review of the literature. Clin Interv Aging 2008; 3: 483–9
Nelson L, Gulenchyn KY, Atthey M, et al. Is a fixed value for the least significant change appropriate? J Clin Densitom 2010; 13: 18–23
Eastell R, Vrijens B, Cahall DL, et al. Bone turnover markers and bone mineral density response with risedronate therapy: relationship with fracture risk and patient adherence. J Bone Miner Res 2011; 26: 1662–9
Rabenda V, Mertens R, Fabri V, et al. Adherence to bisphosphonates therapy and hip fracture risk in osteoporotic women. Osteoporos Int 2008; 19: 811–8
Rabenda V, Hiligsmann M, Reginster JY. Poor adherence to oral bisphosphonate treatment and its consequences: a review of the evidence. Expert Opin Pharmacother 2009; 10: 2303–15
Downey TW, Foltz SH, Boccuzzi SJ, et al. Adherence and persistence associated with the pharmacologic treatment of osteoporosis in a managed care setting. South Med J 2006; 99: 570–5
Acknowledgements
We thank Masahisa Konishi (GE Healthcare, Tokyo, Japan) and Qi Zhou (GE Shanghai, China) for their technical assistance with the AHA analysis and Yoshinori Suzuki (Eisai Co., Ltd., Tokyo, Japan) for his assistance with preparation of the manuscript.
No funding was received for this study. Koichi Itabashi and Yoshinori Suzuki are the product managers of Eisai Co., Ltd., Tokyo, Japan, who deals with risedronate. He contributed to the statistical analysis. The other authors have no conflicts of interest that are directly relevant to the content of this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Takakuwa, M., Iwamoto, J. & Itabashi, K. Three-Year Experience with Risedronate Therapy for Patients with an Increased Fracture Risk. Clin Drug Investig 32, 121–129 (2012). https://doi.org/10.2165/11597990-000000000-00000
Published:
Issue Date:
DOI: https://doi.org/10.2165/11597990-000000000-00000