
Abstract
Objectives
A developed population pharmacokinetic model of the humanized monoclonal antibody (mAb) matuzumab was evaluated by external evaluation. Based on the estimates of the final model, simulations of different dosing regimens and the covariate effect were performed.
Methods
The development dataset included 90 patients, and the evaluation dataset included 81 patients; the two sets of patients were from three different studies. In all studies, the patients had different types of advanced carcinoma — mainly colon, rectal and pancreatic cancer. They received matuzumab as multiple 1-hour intravenous infusions in a wide range of dosing regimens (development dataset: from 400 mg every 3 weeks to 2000 mg in the first week followed by 1600 mg weekly; evaluation dataset: from 100 mg weekly to 800 mg weekly). In addition to 1256 serum mAb concentrations for model development, there were 1124 concentrations available for model evaluation. Serum concentration-time data were simultaneously fitted using NONMEM™ software. The developed two-compartment model — with the parameters central volume of distribution (V1) and peripheral volume of distribution (V2), intercompartmental clearance and linear clearance (CLL), an additional nonlinear elimination pathway (Michaelis-Menten constant: the concentration with the half-maximal elimination rate and Vmax: the maximum elimination rate) and covariate relations — was evaluated by an external dataset. Different simulation scenarios were performed to demonstrate the impact of the incorporated covariate effect and the influence of different dosing regimens and dosing strategies on the concentration-time profiles.
Results
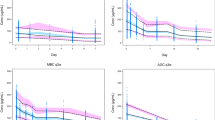
The developed model included the covariate fat-free mass (FFM) on V1 and on CLL. The evaluation did not support the covariate FFM on V1 and, after deletion of this covariate, the model parameters of the refined model were estimated. The model showed good precision for all parameters: the relative standard errors (RSEs) were <42% for the development dataset and ≤51% for the evaluation dataset (excluding the higher RSEs for the correlation between V2 and Vmax and the interindividual variability on V2 for the evaluation dataset). The model showed good robustness for the ability to estimate highly precise parameters for the combined dataset of 171 patients (RSE <29%). Simulations revealed that variability in concentration-time profiles for minimum and maximum steady-state concentrations was reduced to a marginal extent by a proposed dose adaptation.
Conclusion
The population pharmacokinetic model for matuzumab was improved by evaluation with an external dataset. The new model obtained precise parameter estimates and demonstrated robustness. After correlation with efficacy data simulation results in particular could serve as a tool to guide dose selection for this ‘targeted’ cancer therapy.






Similar content being viewed by others


References
De Luca A, Carotenuto A, Rachiglio A, et al. The role of the EGFR signaling in tumor microenvironment. J Cell Physiol 2008; 214: 559–67
Cohen S, Carpenter G, King Jr L, et al. Epidermal growth factor-receptorprotein kinase interactions: co-purification of receptor and epidermal growth factor-enhanced phosphorylation activity. J Biol Chem 1980; 255: 4834–42
Oda K, Matsuoka Y, Funahashi A, et al. A comprehensive pathway map of epidermal growth factor receptor signaling. Mol Syst Biol 2005; 1: 2005–10
Baselga J. The EGFR as a target for anticancer therapy: focus on cetuximab. Eur J Cancer 2001; 37 Suppl. 4: S16–22
Baselga J. Why the epidermal growth factor receptor? The rationale for cancer therapy. Oncologist 2002; 7 Suppl. 4: 2–8
Baselga J. New therapeutic agents targeting the epidermal growth factor receptor. J Clin Oncol 2000; 18: 54S–9S
Goel S, Mani S, Perez-Soler R. Tyrosine kinase inhibitors: a clinical perspective. Curr Oncol Rep 2002; 4: 9–19
Raymond E, Faivre S, Armand JP. Epidermal growth factor receptor tyrosine kinase as a target for anticancer therapy. Drugs 2000; 60 Suppl. 1: 15–23; discussion 41–2
Cunningham D, Humblet Y, Siena S, et al. Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med 2004; 351: 337–45
Walker RA, Dearing SJ. Expression of epidermal growth factor receptor mRNA and protein in primary breast carcinomas. Breast Cancer Res Treat 1999; 53: 167–76
Brabender J, Danenberg KD, Metzger R, et al. Epidermal growth factor receptor and HER2-neu mRNA expression in non-small cell lung cancer is correlated with survival. Clin Cancer Res 2001; 7: 1850–5
Ohsaki Y, Tanno S, Fujita Y, et al. Epidermal growth factor receptor expression correlates with poor prognosis in non-small cell lung cancer patients with p53 overexpression. Oncol Rep 2000; 7: 603–7
Hemming AW, Davis NL, Kluftinger A, et al. Prognostic markers of colorectal cancer: an evaluation of DNA content, epidermal growth factor receptor, and Ki-67. J Surg Oncol 1992; 51: 147–52
Bruno R, Washington CB, Lu JF, et al. Population pharmacokinetics of trastuzumab in patients with HER2+ metastatic breast cancer. Cancer Chemother Pharmacol 2005; 56: 361–9
Ritter CA, Arteaga CL. The epidermal growth factor receptor-tyrosine kinase: a promising therapeutic target in solid tumors. Semin Oncol 2003; 30: 3–11
Wells A. EGF receptor. Int J Biochem Cell Biol 1999; 31: 637–43
Herbst RS, Shin DM. Monoclonal antibodies to target epidermal growth factor receptor-positive tumors: a new paradigm for cancer therapy. Cancer 2002; 94: 1593–611
Harding J, Burtness B. Cetuximab: an epidermal growth factor receptor chemeric human-murine monoclonal antibody. Drugs Today (Barc) 2005; 41: 107–27
Office of Oncology Drug Products, US FDA Center for Drug Evaluation and Research. Erbitux (cetuximab) approved for use in combination with radiation therapy [media release]. 2006 Jul 20 [online]. Available from URL: http://www.fda.gov/cder/Offices/OODP/whatsnew/cetuximab.htm [Accessed 2008 May 18]
US FDA Center for Drug Evaluation and Research. FDA expands labeling for cetuximab (marketed as Erbitux) [media release]. 2007 Oct 12 [online]. Available from URL: http://www.fda.gov/cder/Offices/OODP/whatsnew/centuximab200710.htm [Accessed 2008 May 18]
Socinski MA. Antibodies to the epidermal growth factor receptor in non small cell lung cancer: current status of matuzumab and panitumumab. Clin Cancer Res 2007; 13: s4597–601
Vallbohmer D, Lenz HJ. Epidermal growth factor receptor as a target for chemotherapy. Clin Colorectal Cancer 2005; 5 Suppl. 1: S19–27
Graeven U, Kremer B, Sudhoff T, et al. Phase I study of the humanised antiEGFR monoclonal antibody matuzumab (EMD 72000) combined with gemcitabine in advanced pancreatic cancer. Br J Cancer 2006; 94: 1293–9
Rodeck U, Williams N, Murthy U, et al. Monoclonal antibody 425 inhibits growth stimulation of carcinoma cells by exogenous EGF and tumor-derived EGF/TGF-alpha. J Cell Biochem 1990; 44: 69–79
Murthy U, Basu A, Rodeck U, et al. Binding of an antagonistic monoclonal antibody to an intact and fragmented EGF-receptor polypeptide. Arch Biochem Biophys 1987; 252: 549–60
Kettleborough CA, Saldanha J, Heath VJ, et al. Humanization of a mouse monoclonal antibody by CDR-grafting: the importance of framework residues on loop conformation. Protein Eng 1991; 4: 773–83
Kuester K, Kovar A, Lupfert C, et al. Population pharmacokinetic data analysis of three phase I studies of matuzumab, a humanised anti-EGFR monoclonal antibody in clinical cancer development. Br J Cancer 2008; 98: 900–6
Janmahasatian S, Duffull SB, Ash S, et al. Quantification of lean bodyweight. Clin Pharmacokinet 2005; 44: 1051–65
Brendel K, Dartois C, Comets E, et al. Are population pharmacokinetic and/or pharmacodynamic models adequately evaluated? A survey of the literature from 2002 to 2004. Clin Pharmacokinet 2007; 46: 221–34
Vanhoefer U, Tewes M, Rojo F, et al. Phase I study of the humanized antiepidermal growth factor receptor monoclonal antibody EMD72000 in patients with advanced solid tumors that express the epidermal growth factor receptor. J Clin Oncol 2004; 22: 175–84
DeSilva B, Smith W, Weiner R, et al. Recommendations for the bioanalytical method validation of ligand-binding assays to support pharmacokinetic assessments of macromolecules. Pharm Res 2003; 20: 1885–900
Bonate PL. Pharmacokinetic-pharmacodynamic modeling and simulation. New York: Springer Science and Business Media, 2006
Bonate PL. The effect of collinearity on parameter estimates in nonlinear mixed effect models. Pharm Res 1999; 16: 709–17
Fliss G, Staab A, Tillmann C, et al. Population pharmacokinetic data analysis of cilobradine, an I(f) channel blocker. Pharm Res 2008; 25: 359–68
Yano Y, Beal SL, Sheiner LB. Evaluating pharmacokinetic/pharmacodynamic models using the posterior predictive check. J Pharmacokinet Pharmacodyn 2001; 28: 171–92
Michels GH. The use of collinearity diagnostics in PK model building [online]. Available from URL: http://www.ecpag.org/presentations/2006/0725/2_GregoryMichelsv4.pdf [Accessed 2008 Feb 27]
Belsley DA, Kuh E, Welsh RE. Regression diagnostics: identifying influential data and sources of collinearity. New York: John Wiley & Sons, Inc., 1980
Mager DE. Target-mediated drug disposition and dynamics. Biochem Pharmacol 2006; 72: 1–10
Hing JP, Piotrovsky V, Kimko H, et al. Pharmacokinetic simulation for switching from galantamine immediate-release to extended-release formulation. Curr Med Res Opin 2005; 21: 483–8
Aarons L, Karlsson MO, Mentre F, et al. Role of modelling and simulation in phase I drug development. Eur J Pharm Sci 2001; 13: 115–22
Rombout F, Aarons L, Karlsson M, et al. Modelling and simulation in the development and use of anti-cancer agents: an underused tool? J Pharmacokinet Pharmacodyn 2004; 31: 419–40
Bauer RJ, Guzy S, Ng C. A survey of population analysis methods and software for complex pharmacokinetic and pharmacodynamic models with examples. AAPS J 2007; 9: E60–83
Dingemanse J, Appel-Dingemanse S. Integrated pharmacokinetics and pharmacodynamics in drug development. Clin Pharmacokinet 2007; 46: 713–37
Gieschke R, Steimer JL. Pharmacometrics: modelling and simulation tools to improve decision making in clinical drug development. Eur J Drug Metab Pharmacokinet 2000; 25: 49–58
Anderson BJ, Allegaert K, Holford NH. Population clinical pharmacology of children: general principles. Eur J Pediatr 2006; 165: 741–6
Hortobagyi GN. Overview of treatment results with trastuzumab (Herceptin) in metastatic breast cancer. Semin Oncol 2001; 28: 43–7
Kloft C, Wallin J, Henningsson A, et al. Population pharmacokineticpharmacodynamic model for neutropenia with patient subgroup identification: comparison across anticancer drugs. Clin Cancer Res 2006; 12: 5481–90
Kloft C, Graefe EU, Tanswell P, et al. Population pharmacokinetics of sibrotuzumab, a novel therapeutic monoclonal antibody, in cancer patients. Invest New Drugs 2004; 22: 39–52
Acknowledgements
Bioanalytical samples were measured at the Institute of Drug Metabolism and Pharmacokinetics, Merck KGaA (Grafing, Germany). Raw datasets were provided by Merck KGaA (Darmstadt, Germany). Katharina Kuester received a travel/research grant and Charlotte Kloft received research funding from Merck KGaA. Andreas Kovar, Christian Lüpfert and Brigitte Brockhaus are current employees at Merck KGaA. The authors have no other conflicts of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Rights and permissions
About this article
Cite this article
Kuester, K., Kovar, A., Lüpfert, C. et al. Refinement of the Population Pharmacokinetic Model for the Monoclonal Antibody Matuzumab. Clin Pharmacokinet 48, 477–487 (2009). https://doi.org/10.2165/11313400-000000000-00000
Published:
Issue Date:
DOI: https://doi.org/10.2165/11313400-000000000-00000