
Abstract
The implantable cardioverter defibrillator (ICD) is a therapy for patients at risk of sudden cardiac death due to ventricular tachycardia (VT) or ventricular fibrillation (VF). But the apparent high cost of ICD therapy relative to antiarrhythmic drugs such as amiodarone has raised questions about the cost effectiveness of ICD therapy versus drug therapy. To inform this debate we reviewed the literature on ICD cost effectiveness.
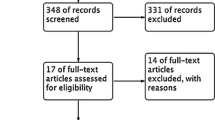
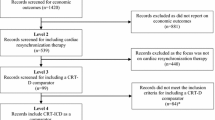
An electronic and manual search was conducted for articles published since 1980 reporting original data on the cost effectiveness of ICD versus drug therapy for patients at risk of VT/VF. Data on costs and life-years gained were abstracted and studies were grouped into those that used decision-analysis models and those that were trial-based analyses. Cost-effectiveness ratios were inflated to 2001 US dollars.
Nine studies were included in the review; five studies were modelling studies and four were part of randomised trials of ICD therapy. Studies varied in time horizon, but all except one indicated that ICD therapy was more costly than drug therapy. Early decision models assumed larger survival benefits than those observed in subsequent trials and therefore had attractive incremental cost-effectiveness ratios in the range of $US27 000 to $US60 000 per life-year gained. Trial-based studies, with the exception of one small trial, indicated cost per life-year gained in the range $US44 000 to $US144 000. Stratified analysis shows clearly that patients with a greater risk of mortality due to structural heart disease (e.g. left ventricular ejection fraction.35%) benefit more from ICD therapy and therefore have a more attractive cost effectiveness ratio than patients at lower risk.
ICD therapy is still evolving over time with implant costs declining and device technology improving. Current evidence is that, in selected patients who are at high risk of VT/VF, ICD therapy can be a cost-effective option. Future research should focus on (i) patient selection to optimise benefits for available resources; and (ii) more comprehensive outcome measures to include health-related quality of life.







Similar content being viewed by others

References
Myerburg RJ, Castellanos A. Cardiac arrest and sudden cardiac death. In: Braunwald E, editor. Heart disease: a textbook of cardiovascular medicine. New York: WB Saunders, 1997: 742–79
Kannel WB, Doyle JT, McNamara PM, et al. Precursors of sudden coronary death: factors related to the incidence of sudden death. Circulation 1975; 51 (4): 606–13
Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico. GISSI-2: a factorial randomised trial of alteplase versus streptokinase and heparin versus no heparin among 12 490 patients with acute myocardial infarction. Lancet 1990; 336 (8707): 65–71
International Study Group. In-hospital mortality and clinical course of 20 891 patients with suspected acute myocardial infarction randomised between alteplase and streptokinase with or without heparin. Lancet 1990; 336 (8707): 71–5
Weaver WD, Cobb LA, Hallstrom AP, et al. Factors influencing survival after out-of-hospital cardiac arrest. J Am Coll Cardiol 1986; 7 (4): 752–7
Myerburg RJ, Kessler KM, Castellanos A. Sudden cardiac death: epidemiology, transient risk, and intervention assessment. Ann Intern Med 1993; 119 (12): 1187–97
Bigger JT, Fleiss JL, Kleiger R, et al. The relationship among ventricular arrhythmias, left ventricular dysfunction, and mortality in the 2 years after myocardial infarction. Circulation 1984; 69: 250–8
Greenberg H, McMaster P, Dwyer Jr EM. Left ventricular dysfunction after acute myocardial infarction: results of a prospective multicenter study. J Am Coll Cardiol 1984; 4 (5): 867–74
Gregoratos G, Cheitlin MD, Conill A, et al. ACC/AHA guidelines for implementation of cardiac pacemakers and antiarrhythmia devices: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Pacemaker Implementation). J Am Coll Cardiol 1998; 31: 1175–209
Connolly SJ, Talajic M. Chapter 1: summary of the CCS consensus conference on prevention of sudden death from cardiac arrhythmia. Can J Cardiol 2000; 16: 1298–302
Hine LK, Laird NM, Hewitt P, et al. Meta-analysis of empirical long-term antiarrhythmic therapy after myocardial infarction. JAMA 1989; 262: 3037–40
Echt DS, Liebson PR, Mitchell LB, et al. Mortality and morbidity in patients receiving encainide, flecainide, or placebo: the Cardiac Arrhythmia Suppression Trial. N Engl J Med 1991; 324: 781–8
Randomized antiarrhythmic drug therapy in survivors of cardiac arrest (the CASCADE Study): the CASCADE Investigators. Am J Cardiol 1993; 72: 280–7
Jafri SM, Borzak S, Goldberger J, et al. Role of antiarrhythmic agents after myocardial infarction with special reference to the EMIAT and CAMIAT trials of amiodarone. European Myocardial Infarct Amiodarone Trial. Canadian Amiodarone Myocardial Infarction Trial. Prog Cardiovasc Dis 1998; 41: 65–70
Coumel P, Prystowsky EN. Implantable cardioverter defibrillator therapy: 15 years experience and future expectations. Pacing Clin Electrophysiol 1995; 18: 505–631
Kuppermann M, Luce BR, McGovern B, et al. An analysis of the cost effectiveness of the implantable defibrillator. Circulation 1990; 81: 91–100
O’Brien BJ, Buxton MJ, Rushby JA. Cost effectiveness of the implantable cardioverter defibrillator: a preliminary analysis. Br Heart J 1992; 68: 241–5
Larsen GC, Manolis A, Sonnenberg F, et al. Cost-effectiveness of the implantable cardioverter-defibrillator: effect of improved battery life and comparison with amiodarone therapy. J Am Coll Cardiol 1992; 19: 1323–34
Kupersmith J, Hogan A, Guerrero P, et al. Evaluating and improving the cost-effectiveness of the implantable cardioverter defibrillator. Am Heart J 1995; 130: 507–15
Owens DK, Sanders GD, Harris RA, et al. Cost effectiveness of implantable cardioverter defibrillators relative to amiodarone for prevention of sudden cardiac death. Ann Intern Med 1997; 126: 12
Wever EF, Hauer RN, van Capelle FL, et al. Randomized study of implantable defibrillator as first-choice therapy versus conventional strategy in postinfarct sudden death survivors. Circulation 1995; 91: 2195–203
Mushlin AI, Hall WJ, Zwanzziger J, et al. The cost effectiveness of automatic implantable cardiac defibrillators: results for MADIT. Circulation 1998; 97: 2129–35
Larsen GC, Hallstrom AP, McAnulty J, et al. Cost-effectiveness of the implantable cardioverter defibrillator versus antiarrhythmic drugs in survivors of serious ventricular tachyarrhythmias. Circulation 2002; 105: 2049–57
O’Brien BJ, Connolly SJ, Goeree R, et al. Cost-effectiveness of the implantable cardioverter-defibrillator: results from the Canadian Implantable Defibrillator Study (CIDS). Circulation 2001; 103: 1416–21
Moss AJ, Hall WJ, Cannom DS. Improved survival with an implantable defibrillator in patients with coronary disease at high risk for ventricular arrhythmia: Multicentre Automatic Defibrillation Trial Investigation. N Engl J Med 1996; 335: 1933–40
Connolly SJ, Gent M, Roberts RS, et al. Canadian implantable defibrillator study: a randomized trial of the implantable cardioverter defibrillator against amiodarone. Circulation 2000; 101: 1297–302
Kuck KH, Cappato R, Siebels J, et al. Randomized comparison of antiarrhythmic drug therapy with implantable cardioverter defibrillators in patients resuscitated from cardiac arrest: the Cardiac Arrest Study Hamburg. Circulation 2000; 102: 748–54
A comparison of antiarrhythmic drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. The antiarrhythmics versus implantable defibrillators (AVID) investigators. N Engl J Med 1997; 337: 1576–83
Sheldon R, O’Brien BJ, Blackhouse G, et al. The effect of clinical risk stratification on the cost-effectiveness of the implantable cardioverter defibrillator: the Canadian Implantable Defibrillator Study. Circulation 2001; 104: 1622–6
Sheldon RS, Connolly SJ, Krahn A, et al. Identification of patients most likely to benefit from implantable cardioverter-defibrillator therapy: the Canadian Implantable Defibrillator Study. Circulation 2001; 101: 1660–4
Lothgren M, Zethreaus N. Definition, interpretation and calculation of cost-effectiveness acceptability curves. Health Econ 2000; 9: 623–30
Moss AJ, Cannom DS, Daubert J, et al. Multicentre automatic defibrillator trial II (MADIT II): design and clinical protocol. Ann Noninvasive Electrocardiol 1999; 4: 83–91
Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med 2002; 346 (12): 877–83
Bigger TJ. Expanding indications for implantable cardiac defibrillators. N Engl J Med 2002; 346 (12): 931–3
O’Brien BJ. Cost effectiveness of ICD therapy: a review of published evidence. Can J Cardiol 2000; 16: 1307–12
Hohnloser SH, Connolly SJ, Kuck KH, et al. The defibrillator in Acute Myocardial Infarction Trial (DINAMIT): study protocol. Am Heart J 2000; 140: 735–9
Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36): I. conceptual framework and item selection. Med Care 1992; 30: 473–83
Feeny D, Furlong W, Boyle MH, et al. Multi-attribute health status classification systems: Health Utilities Index. Pharmacoeconomics 1995; 7 (6): 490–502
Acknowledgements
This work commenced while Marian Spath was a visiting graduate student at the Centre for Evaluation of Medicines at St Joseph’s Hospital, Hamilton, Ontario, Canada and was completed while Bernie O’Brien was a Visiting Professor at the Centre for Health Economics Research and Evaluation and the NHMRC Clinical Trials Centre at the University of Sydney, Australia. We are grateful to these institutions for their hospitality.
Bernie O’Brien is supported by a Senior Investigator award from the Canadian Institutes of Health Research. The manuscript was a non-funded graduate student project. The authors have no conflicts of interest that are directly relevant to the content of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Spath, M.A., O’Brien, B.J. Cost Effectiveness of Implantable Cardioverter Defibrillator Therapy versus Drug Therapy for Patients at High Risk of Sudden Cardiac Death. Pharmacoeconomics 20, 727–738 (2002). https://doi.org/10.2165/00019053-200220110-00002
Published:
Issue Date:
DOI: https://doi.org/10.2165/00019053-200220110-00002