
Summary
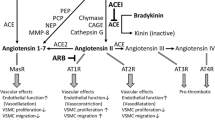
Angiotensin II type 1 (AT1) receptor antagonists inhibit the renin-angiotensin system more completely than ACE inhibitors, and do not increase bradykinin levels as ACE inhibitors do. ACE inhibitors have been proven to increase survival and improve quality of life in patients with congestive heart failure (CHF). At the 48-week follow-up of the Evaluation of Losartan in the Elderly (ELITE) Study, the AT1 receptor antagonist losartan (at a dosage of 50 mg/day) was found to be superior to captopril 50mg 3 times daily in terms of its effects on total mortality, total mortality and/or hospitalisation for CHF, and hospitalisation for any reason. Hospitalisation for CHF was the same for both drugs. Adverse effects occurred in 12 and 21% of those receiving losartan and captopril, respectively. Cough, rash, angioedema or taste disturbances/reduced appetite prompted the cessation of drug treatment in 0 and 7% of those receiving losartan and captopril, respectively. Until additional data are available, this author recommends that elderly patients with CHF and an abnormal or normal left ventricular ejection fraction, and who are unable to tolerate ACE inhibitors, should receive losartan 50 mg/day.
Similar content being viewed by others
References
Abdelrahman AM, Burrell LM, Johnston CI. Blockade of the renin-angiotensin system at different sites: effect on renin, angiotensin and aldosterone. J Hypertens 1993; 11Suppl. 3: S23–6
Burrell LM, Johnston CI. Angiotensin II receptor antagonists: potential in elderly patients with cardiovascular disease. Drugs Aging 1997; 10: 421–34
Pitt B, Chang P, Timmermans P. Angiotensin II receptor antagonists in heart failure: rationale and design of the Evaluation of Losartan in the Elderly (ELITE) trial. Cardiovasc Drugs Ther 1995; 9: 693–700
Gavras I. Bradykinin-mediated effects of ACE inhibition. Kidney Int 1992; 42: 1020–9
Israili ZH, Hall WD. Cough and angioneurotic edema associated with angiotensin-converting enzyme inhibitor therapy: a review of the literature and pathophysiology. Ann Intern Med 1992; 117: 234–42
Chalmers D, Dombey SL, Lawson DH. Post-marketing surveillance of captopril (for hypertension): a preliminary report. Br J Clin Pharmacol 1987; 24: 343–9
Lacourciere Y, Brunne H, Irwin R, et al., Losartan Cough Study Group. Effects of modulators of the renin-angiotensin-aldosterone system on cough. J Hypertens 1994; 12: 1387–93
Johnston CI. Angiotensin receptor antagonists: focus on losartan. Lancet 1995; 346: 1403–7
Bauer JH, Reams GP. The angiotensin II type 1 receptor antagonists. Arch Intern Med 1995; 155: 1361–8
Timmermans PB, Wong PC, Chiu AT, et al. Angiotensin II receptors and angiotensin II receptor antagonists. Pharmacol Rev 1993; 45: 205–51
Miura S, Ideishi M, Sakai T, et al. Angiotensin II formation by an alternative pathway during exercise in humans. J Hypertens 1994; 12: 1177–81
Urata H, Kinoshita A, Misono KS, et al. Identification of a highly specific chymase as the major angiotensin II-forming enzyme in the human chymase. J Biol Chem 1990; 265: 22348–57
Urata H, Strobel F, Ganten D. Widespread tissue distribution of human chymase. J Hypertens 1994; 12: S17–22
Aldigier JC, Huang H, Dalmay F, et al. Angiotensin-converting enzyme inhibition does not suppress plasma angiotensin II increase during exercise in humans. J Cardiovasc Pharmacol 1993; 21: 289–95
Cleland JGF, Dargie HJ, Hodsman GP, et al. Captopril in heart failure: a double blind controlled trial. Br Heart J 1984; 52: 530–5
Cleland JGF, Dargie HJ, Ball SG, et al. Effects of enalapril in heart failure: a double blind study of effects on exercise performance, renal function, hormones, and metabolic state. Br Heart J 1985; 54: 305–12
Webster MWI, Fitzpatrick MA, Nicholls MG, et al. Effect on enalapril on ventricular arrhythmias in congestive heart failure. Am J Cardiol 1985; 56: 566–9
Captopril-Digoxin Multicenter Research Group. Comparative effects of therapy with captopril and digoxin in patients with mild to moderate heart failure. JAMA 1988; 259: 539–44
Fletcher RD, Cintron GB, Johnson G, et al., V-HeFT II VA Cooperative Studies Group. Enalapril decreases prevalence of ventricular tachycardia in patients with chronic congestive heart failure. Circulation 1993; 87Suppl. VI: VI49–55
Pratt CM, Gardner M, Pepine C, et al., SOLVD Investigators. Lack of long-term ventricular arrhythmia reduction by enalapril in heart failure. Am J Cardiol 1995; 75: 1244–9
CONSENSUS Trial Study Group. Effect of enalapril on mortality in severe congestive heart failure: results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N Engl J Med 1987; 316: 1429–35
Cohn JN, Johnson G, Ziesche S, et al. A comparison of enalapril with hydralazine-isosorbide dinitrate in the treatment of chronic congestive heart failure. N Engl J Med 1991; 325: 303–10
SOLVD Investigators. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med 1991; 325: 293–302
Acute Infarction Ramipril Efficacy (AIRE) Study Investigators. Effect of ramipril on mortality and morbidity of survivors of acute myocardial infarction with clinical evidence of heart failure. Lancet 1993; 342: 821–8
Garg R, Yusuf S, for the Collaborative Group on ACE Inhibitor Trials. Overview of randomized trials of angiotensin-converting enzyme inhibitors on mortality and morbidity in patients with heart failure. JAMA 1995; 273: 1450–6
Pfeffer MA, Braunwald E, Moye LA, et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction: results of the Survival and Ventricular Enlargement Trial. N Engl J Med 1992; 327: 669–77
Ambrosioni E, Borghi C, Magnani B, Survival of Myocardial Infarction Long-Term Evaluation (SMILE) Study Investigators. The effect of the angiotensin-converting-enzyme inhibitor zofenopril on mortality and morbidity after anterior myocardial infarction. N Engl J Med 1995; 332: 80–5
Kober L, Torp-Pedersen C, Carlsen JE, et al. A clinical trial of the angiotensin-converting-enzyme inhibitor trandolapril in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med 1995; 333: 1670–6
Aronow WS, Kronzon I. Effect of enalapril on congestive heart failure treated with diuretics in elderly patients with prior myocardial infarction and normal left ventricular ejection fraction. Am J Cardiol 1993; 71: 602–4
Pitt B, Segal R, Martinez FA, et al. Randomised trial of losartan versus captopril in patients over 65 with heart failure (Evaluation of Losartan in the Elderly Study, ELITE). Lancet 1997; 349: 747–52
Klinger G, Jaramillo N, Ikram H, et al. Effects of losartan on exercise capacity, morbidity and mortality in patients with symptomatic heart failure [abstract]. J Am Coll Cardiol 1997; 29Suppl. A: 205A
Brasch H, Sierolawski L, Dominiak P. Angiotensin II increases norepinephrine release from atria by acting at angiotensin subtype 1 receptors. Hypertension 1993; 22: 699–704
Minisi AJ, Thames MD. Distribution of left ventricular sympathetic afferents demonstrated by reflex responses to transmural myocardial ischemia and to intracoronary and epicardial bradykinin. Circulation 1993; 87: 240–6
Aronow WS, Ahn C, Kronzon I. Prognosis of congestive heart failure in elderly patients with normal versus abnormal left ventricular systolic function associated with coronary artery disease. Am J Cardiol 1990; 66: 1257–9
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Aronow, W.S. The ELITE Study. Drugs & Aging 12, 423–428 (1998). https://doi.org/10.2165/00002512-199812060-00001
Published:
Issue Date:
DOI: https://doi.org/10.2165/00002512-199812060-00001