We evaluated the risk of incident CVD according to the LDL-C and FPG levels in participants without DM. We observed significant positive associations between the increased risk of CVD and high LDL-C levels in participants without DM, and the risk of CVD increased in participants without DM who had LDL-C levels ≥ 100 mg/dL. We demonstrated that elevations in the FPG levels, even in the same LDL-C category, were associated with an increased risk of CVD. The risk of CVD increased more significantly in participants with FPG levels ≥ 110 mg/dL than in those in the other FPG categories. These findings suggested that elevations in the FPG and LDL-C levels independently contributed to the increased risk of CVD in participants without DM. To the best of our knowledge, this was the first nationwide study to investigate the optimal ranges of LDL-C that were associated with the lowest risk of CVD in East Asian adults without DM.
Previous epidemiological investigations have consistently demonstrated a strong positive, continuous, independent, and graded relationship between LDL-C levels and the incidence of CVD [11, 12]. Furthermore, recent meta-analyses of Mendelian randomization studies involving over 300,000 participants and 80,000 CVD cases provided convincing evidence regarding the causal correlation between LDL-C levels and the risk of ASCVD. Moreover, they showed that the causal impact of LDL-C levels on ASCVD might essentially be independent of the mechanism by which LDL-C levels are “lowered” [13]. Therefore, most international guidelines suggest strategies for managing LDL-C levels and setting LDL-C targets for the primary prevention of CVD. These guidelines consider DM to be a major risk factor for CVD and recommend the use of statins, regardless of the LDL-C levels, for the prevention of CVD in patients with DM [14–16]. However, the implementation of guidelines among members of the general population, especially among those without DM, has been a challenge for a long time. The American College of Cardiology/American Heart Association (ACC/AHA) guidelines removed specific target LDL-C levels since 2013 and emphasized a strategy of fixed-dose statin therapy based on cardiovascular risk in individuals without DM [14]. However, calculating the ASCVD risk is challenging due to the lack of time and complexities in clinical calculations. Moreover, this ASCVD risk calculator was designed based on data mainly from populations other than those from East Asia. Considering the established strong graded relationship between LDL-C levels and incident CVD, determining the optimal LDL-C range for the primary prevention of CVD in individuals without DM is needed in the Asian population.
The present study found that among participants without DM and a history of CVD, there was an increased risk of CVD in those with LDL-C levels ≥ 100 mg/dL This cut-off value was in line with that recommended by several international guidelines. The 2019 European Society of Cardiology/European Atherosclerotic Society guidelines suggest an LDL-C goal of < 116 mg/dL for the primary prevention of CVD in individuals with a low risk of CVD [16]. However, guidelines for dyslipidemia management in Korea suggest an LDL-C goal of < 130 mg/dL in individuals without DM and a moderate CVD risk, and < 160 mg/dL in individuals without DM and a low CVD risk [15]. The suggested target LDL-C levels according to the Korean guidelines in individuals without DM were significantly higher than those in our study (LDL-C levels < 100 mg/dL). However, the Korean dyslipidemia guidelines were made based on data from other countries. Further prospective randomized controlled studies are warranted to determine the optimal LDL-C levels for the initiation of pharmacological intervention for the primary prevention of CVD in Korean adults without DM.
In the current study, we observed a graded positive trend for CVD risk starting from an LDL-C level of 100 mg/dL, which increased for the higher LDL-C categories among participants who were non-statin users. The risk of CVD was higher whose LDL-C levels were ≥ 130 mg/dL in statin users than in those in the LDL-C reference group. From these results, we suggest that the uptitration of statins may be considered if LDL-C levels are ≥ 130 mg/dL during statin treatment, with consideration of the CVD risk in individuals without DM. Furthermore, the risk of CVD was relatively more attenuated in statin users than in non-statin users, even in the same LDL-C categories. The attenuated CVD risk in statin users was prominent in those in the higher LDL-C and FPG categories. It demonstrated the benefit of using statin for the primary prevention of CVD, regardless of the LDL-C levels in individuals without DM. This finding was consistent with those of previous primary prevention trials that demonstrated the benefits of statin therapy [17]. These studies showed that statins can reduce CVD risk through pleiotropic effects, including the inhibition of inflammation [6, 18].
We found that modestly elevated FPG levels (110–125 mg/dL), even it is not suitable level for diagnosing diabetes, were independently associated with a higher risk of CVD compared to the reference groups (FPG level of 70–99 mg/dL and LDL-C level of 70–99 mg/dL). A higher risk of CVD in participants with modestly elevated FPG levels was still observed even when their LDL-C levels were low (70 mg/dL). This suggested that well-controlled LDL-C levels might not be protective against a higher CVD risk in individuals with modestly elevated FPG levels. Moreover, we observed that the combination of higher FPG and LDL-C levels synergistically elevated the risk of CVD in participants without DM. This finding was consistent with the biological synergistic interaction between glucose and cholesterol levels reported in previous studies [19, 20]. There are some possible biological mechanisms that support the interaction between glucose and LDL-C. It is widely believed that the oxidation of LDL-C plays an important role in atherogenesis, and excess circulating glucose levels might facilitate cholesterol peroxidation [21]. It was found that DM might be related to oxidative stress, which is linked to atherogenesis [22–24]. This biological interaction indicates that optimal LDL-C goals might differ according to glucose levels, which might be clinically significant. Our findings warrant a clinical trial to determine whether using glucose levels to advise about cholesterol control would improve outcomes. Our findings indicated that the target LDL-C goal for the primary prevention of CVD should be lower, and more aggressive statin use may be considered in individuals with FPG levels of 110–125 mg/dL, similar to those with DM.
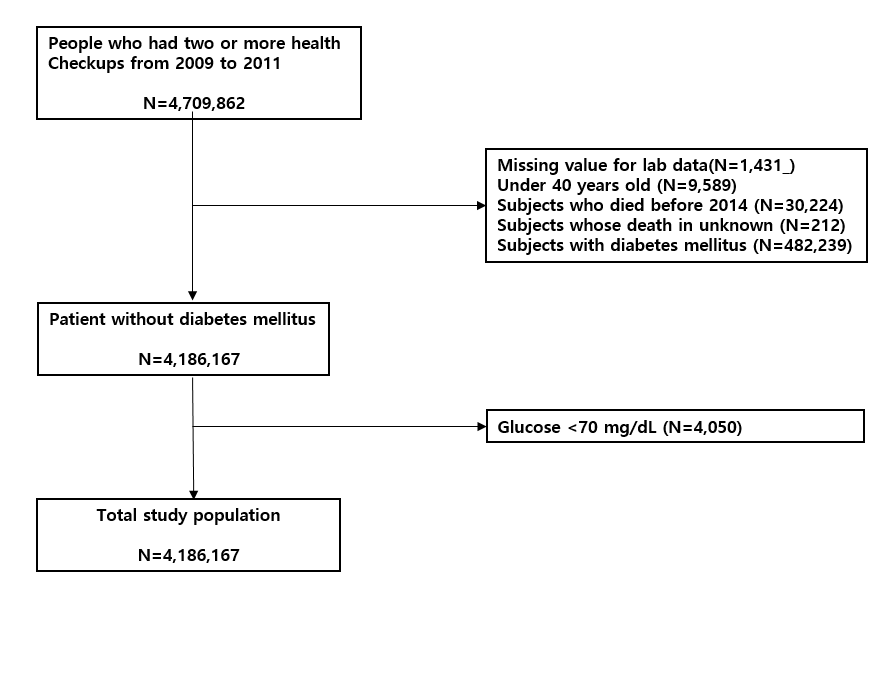
Our study had several limitations. First, as the NHIS database relies on the issuance of a diagnostic code for CVD by physicians, there might have been a risk of misdiagnosis, which might have contributed to the underestimation or overestimation of the prevalence of CVD. Second, day-to-day variabilities might have influenced the findings due to laboratory errors or biological variations, as we used the results of a single LDL-C and FPG test in the analyses. Additionally, as we could not directly measure LDL-C levels and used the Friedewald formula instead, it might have led to the underestimation of the LDL-C levels. Third, there was lack of data on antidyslipidemic medication use among our participants during the follow-up period. Over time, cholesterol levels can increase, which could have led to statin use even among non-users, thereby mitigating the observed risk of CVD. Fourth, we did not obtain data on changes in medications or interventions during the follow-up period. Furthermore, we did not account for many confounders in our study, such as genetic factors, medication use, and socioeconomic status, which might have influenced our results. Fifth, we could not calculate the 10-year risk of ASCVD due to lack of data and consider individual cardiovascular risks in our analysis. Finally, as the present study only included the Korean population, our findings could not be generalized to other ethnicities. However, the major strengths of the current study were its large sample size, with approximately 4,000,000 relatively healthy participants, and use of longitudinal data. Thus, our results reflect “real-world” evidence on the association of LDL-C levels with CVD risk in individuals without DM on a national scale.
{kind=link}