Effect of Piper Betle Linn Extract Concentration and Contact Time on Reducing Bacillus Subtilis and Bacillus Stearothermophilus in Medical Waste

Elanda Fikri*![]() | Nany Djuhriah
| Nany Djuhriah![]() | Neneng Yety Hanurawaty
| Neneng Yety Hanurawaty![]() | Angreni Ayuhastuti
| Angreni Ayuhastuti![]() | Yura Witsqa Firmansyah
| Yura Witsqa Firmansyah![]()
© 2023 IIETA. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Non-optimized medical waste treatment can produce biological residues of Bacillus subtilis and Bacillus stearothermophilus bacteria, which are agents of various diseases. The first purpose of this study was to determine the difference in the length of contact time and dose of green betel leaf (Piper betle Linn.) extract on the number of Bacillus sp. in the medical waste recycling process. This study’s second purpose was to determine the total Bacillus subtilis and Bacillus stearothermophilus reduction after treatment. This study’s research design was an experimental design (the after-only design). The concentrations used were 0.03%, 0.05%, 0.07%, 0.3%, 0.5%, 0.7%, 3%, 5% and 7%, and contact times of 15, 30, and 45 minutes with 144 samples each. The ANOVA (one-way) test results showed that there were no differences in the length of contact time and dose of Piper betle Linn. extract as a disinfectant on the number of Bacillus subtilis in the medical waste recycling process. The smallest amount of Bacillus sp. was found at a concentration of 0.05% green betel leaf immersion (330 colonies/ml), and the largest colonies occurred at a concentration of 3% immersion (658 colonies/ml). The contact time and concentration of green betel leaves had no difference on the number of Bacillus sp., but the concentration of 3% showed optimal results in reducing these bacteria. Antimicrobial Piper betle Linn. content can be developed for further research in the removal of bacteria or other parasites.
antimicrobial, disinfectan, medical waste treatment
During the COVID-19 pandemic, a marked increase in medical waste quantities was observed worldwide, with daily global production reaching 2.6 million tons [1, 2]. The World Health Organization (WHO) declared that high-income countries generally produce around 0.5kg of medical waste per hospital bed daily [3]. Conversely, a significant surge in medical waste was reported in Indonesia, with the daily output reaching 18,460 tons in June 2021, as per the Indonesian Ministry of Environment and Forestry (KLHK) and the Indonesian Hospital Association (PERSI) [4]. This figure greatly surpasses the country's medical waste treatment capacity of 314.29 tons/day, with actual services only managing 244.08 tons/day [5]. Medical waste, originating from various sources including screening and testing sites, primary health facilities, hospitals, and quarantine centers, poses severe health risks if improperly managed [6-8]. Typical waste constituents encompass medical aprons, masks, face shields, gloves, medical hoods, syringes, and COVID-19 test kits [6-8]. Unprocessed medical waste serves as a disease transmission vector, transforming waste disposal sites into breeding grounds for pathogens, insects, and rodents [9]. As toxic substances, medical waste can cause health complications and injuries, with dust particles potentially contaminating medical equipment and food, thereby exacerbating disease transmission [10-12].
In Indonesia, the predominant method for medical waste treatment is incineration [13, 14]. However, this practice has sparked controversy due to the resultant air pollution. Incineration at temperatures ≥850℃ yields pollutants such as carbon monoxide (CO), fly ash, heavy metals, nitrogen oxides (NOx), sulfur dioxide, hydrogen chloride, and organic compounds [15, 16]. Furthermore, the combustion process impacts autoclave decontamination and contributes to the transportation carbon footprint and carbon gas emissions [15, 16]. Despite incinerators being the primary technology employed for medical waste disposal, their limited availability poses a significant challenge in Indonesia. As of November 2020, only 111 hospitals were licensed to operate incinerators, with a mere six utilizing autoclaves [13]. Moreover, incineration does not fully eliminate medical waste, leaving behind biological, chemical, or physical residues.
Bacillus sp. is an aerobic bacterium and one of the bacteria that can be found in incinerator residue. Bacillus sp. is an aerobic, secretory, and rod-shaped bacterium. Bacillus subtilis and Bacillus stearothermophilus are some of the species of Bacillus sp. found in medical waste. Bacillus subtilis and Bacillus stearothermophilus are bacteria that are resistant to heat, radiation, chemicals, drying, and disinfection, making them difficult to remove from medical waste [17]. Bacillus sp. bacteria are common causative agents of respiratory, urinary, wound, burn, and ear infections, as well as ophthalmitis, abscesses, osteomyelitis, bacteremia/septicemia, endocarditis, meningitis, and peritonitis. Bacillus subtilis and Bacillus stearothermophilus species can be agents of occasional infections [17]. Bacillus subtilis and Bacillus stearothermophilus are the species of Bacillus sp. bacteria that are harmful and can affect public health. Due to this, the presence of these bacteria needs to be eliminated from medical waste to eliminate the possibility of disease transmission when it comes in contact with humans.
Bacillus subtilis and Bacillus stearothermophilus are resistant to heat, chemicals, drying, and disinfection, meaning technological innovation efforts are needed to eliminate them. The betel leaf (Piper betle Linn.) is a medicinal plant commonly found in Asian countries. In general, Piper betle Linn. is used to maintain oral health [18-20]. In addition, Piper betle Linn. is used as a traditional medicine for headaches, joint inflammation and joint pain, and skin conditions [18, 21]. Review studies conducted by Nayaka et al. [22] found that Piper betle Linn. has antibacterial and antifungal properties. Piper betle Linn. has been shown to effectively kill Pseudomonas aeruginosa, Escherichia coli, Candida albicans, and Staphylococcus aureus [22]. By considering the antibacterial and antifungal properties of Piper betle Linn., technological innovations can be made to create disinfectants made from Piper betle Linn. extract. This study had several objectives, the first being to determine the difference in the length of contact time and dose of green betel leaf extract (Piper betle Linn.) as a disinfectant against all Bacillus subtilis and Bacillus stearothermophilus in the medical waste recycling process. The second objective was to determine the percentage of reduced Bacillus subtilis and Bacillus stearothermophilus before and after being treated. This study has good originality and novelty, as it aimed to produce a new disinfectant product for the removal of Bacillus subtilis and Bacillus stearothermophilus in medical waste.
2.1 Type of research and study design
This study is classified in terms of objective (explanatory research). This research study’s design is classified as an experimental design (the after-only design). One group of subjects with two conditions was treated directly without a comparison group. The after-only in this study was the total Bacillus subtilis and Bacillus stearothermophilus in the medical waste recycling process after treatment (disinfection method). The study was conducted in March 2023, wherein Bacillus subtilis and Bacillus stearothermophilus were tested in the microbiology laboratory of the Environmental Health Department at the Polytechnic Ministry of Health Bandung, Indonesia.
2.2 Sampling technique and sample size
The sample in this study consisted of the recycled medical waste materials used for testing Bacillus subtilis and Bacillus stearothermophilus. The total samples used in this study were 144 samples with four repetitions, including controls. Grab sampling was used, which is a sample taken at a certain time in one location. The sample was already able to represent the recycled medical waste material as a whole.
2.3 Univariate and bivariate data analysis
Univariate and bivariate data analyses were conducted. The univariate analysis aims to explain or describe the characteristics of each research variable. The independent variables in this study were the length of contact time and dose of green betel leaf extract (Piper betle Linn.), while the dependent variable in this study was the total Bacillus subtilis and Bacillus stearothermophilus in the medical waste. This univariate analysis was used to obtain the mean, median, mode, minimum value, maximum value, standard deviation, variance, and linear quartile range. The results were used to determine the decrease in Bacillus subtilis and Bacillus stearothermophilus percentage in the medical waste recycling process. Meanwhile, the bivariate analysis is carried out on variables that are thought to be related or have an influence, and to examine the magnitude of the independent variable’s influence on the dependent variable. The bivariate analysis used in the study was two-way ANOVA, while testing differences between groups utilized the assumption of homogeneity Levene Test.
The number of pages for the manuscript must be no more than ten, including all the sections. Please make sure that the whole text ends on an even page. Please do not insert page numbers. Please do not use the Headers or the Footers because they are reserved for the technical editing by editors.
3.1 Measurement of temperature, pH, and TDS in the immersion process of Piper betle Linn. in medical waste
In the beginning, physical parameters were measured in the immersion process (disinfection) with green betel leaf extract (Piper betle Linn) in the medical waste recycling process. The physical parameters measured were temperature, pH, and total dissolved solid (TDS). The measurement results are presented in Figure 1 (temperature), Figure 2 (pH), and Figure 3 (TDS) below.
Figure 1. Temperature measurement in the immersion process of Piper betle Linn. in medical waste
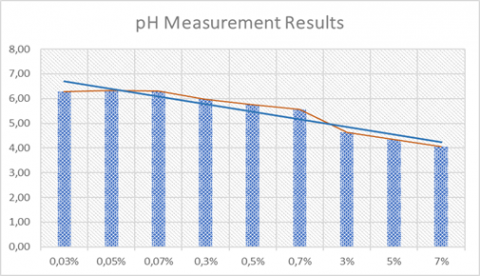
Figure 2. Measurement of pH in the immersion process of Piper betle Linn. in medical waste
Figure 3. Measurement of total dissolved solid (TDS) in the immersion process of Piper betle Linn. in medical waste
Based on the temperature measurement results in Figure 1, there was a decrease in temperature during the immersion process (disinfection) with green betel leaf (Piper betle Linn.) extract in the medical waste recycling process. The lowest temperature occurred at a green betel leaf immersion concentration of 7% (24.21℃), and the highest temperature occurred at an immersion concentration of 0.7% (25.15℃). The average temperature reached 25.04℃ with a standard deviation of 0.39. Determination of the appropriate temperature can affect the quality of the betel leaf extract (Piper betle Linn). This is in line with a study conducted by Kusuma et al. [23], who observed that Piper betle Linn. extract conditions in the temperature range of 26-28℃ had moderate inhibition of green betel leaf extract (Piper betle Linn.) on Streptococcus agalactiae bacteria. Moreover, room temperature conditions in immersions containing Piper betle extract have been found to inhibit Streptococcus intermedius, Streptococcus mutans, and Candida albicans [24, 25].
Based on the pH measurement results Figure 2, the immersion process (disinfection) with green betel leaf extract in the medical waste recycling process showed a decrease in pH. The lowest pH occurred at a concentration of 7% green betel leaf immersion (4.07), and the highest pH occurred at a concentration of 0.05% immersion (6.33). The average pH reached 5.47 with a standard deviation of 0.89. The decrease in pH was due to the active ingredient’s (betel leaf extract) pH being acidic (pH=4). This means that with increasing amounts of extract, the pH will be lower [26, 27].
Based on the TDS measurement results, there was an increase in TDS values during the immersion process (disinfection) with green betel leaf extract in the medical waste recycling process. The lowest TDS value occurred at a concentration of 0.03% green betel leaf immersion (179ppm), and the largest TDS value occurred at an immersion concentration of 7% (1934ppm). The average TDS reached 628ppm with a standard deviation of 644.89.
The reason for the high TDS increase is thought to be due to the saponin content in the betel extract. Some saponins have acidic properties due to the presence of carboxyl groups on aglycones and or sugar groups [28]. Protein solubility will increase if given excessive acid treatment. This happens because the positive ions in the acid will cause proteins which were originally neutrally charged to become positively charged and cause its solubility to increase, making the tube turbid [29, 30]. This means the difference in turbidity is not due to the presence or absence of bacteria, but due to the concentration of the extract. The higher the extract’s concentration, the higher the turbidity level.
3.2 Univariate, homogeneity, and bivariate analysis
The Pier betle Linn. was observed in doses of 0.03%, 0.05%, 0.07%, 0.3%, 0.5%, 0.7%, 3%, 5% and 7%. Meanwhile, the time intervals used were 15, 30, and 45 minutes. The complete results are presented in Table 1 (univariate independent variables), Table 2 (homogeneity assumption), and Table 3 (ANOVA test).
Table 1. Statistical descriptive results of contact time and Piper betle Linn. dose
|
Dose |
Length of Contact Time |
Mean |
Std. Deviation |
N |
|
0.03% |
15 minutes |
469.00 |
263.056 |
4 |
|
30 minutes |
511.50 |
515.463 |
4 |
|
|
45 minutes |
686.25 |
339.959 |
4 |
|
|
Total |
555.58 |
364.002 |
12 |
|
|
0.05% |
15 minutes |
408.75 |
326.140 |
4 |
|
30 minutes |
315.00 |
371.759 |
4 |
|
|
45 minutes |
267.25 |
268.293 |
4 |
|
|
Total |
330.33 |
300.169 |
12 |
|
|
0.07% |
15 minutes |
419.50 |
460.845 |
4 |
|
30 minutes |
467.75 |
400.339 |
4 |
|
|
45 minutes |
298.00 |
267.273 |
4 |
|
|
Total |
395.08 |
355.919 |
12 |
|
|
0.3% |
15 minutes |
273.25 |
263.292 |
4 |
|
30 minutes |
482.50 |
366.308 |
4 |
|
|
45 minutes |
205.00 |
33.615 |
4 |
|
|
Total |
320.25 |
266.487 |
12 |
|
|
0.5% |
15 minutes |
419.50 |
243.034 |
4 |
|
30 minutes |
684.50 |
595.768 |
4 |
|
|
45 minutes |
665.75 |
534.966 |
4 |
|
|
Total |
589.92 |
454.826 |
12 |
|
|
0.7% |
15 minutes |
523.25 |
490.326 |
4 |
|
30 minutes |
526.25 |
379.423 |
4 |
|
|
45 minutes |
706.00 |
157.211 |
4 |
|
|
Total |
585.17 |
345.742 |
12 |
|
|
3% |
15 minutes |
670.25 |
421.865 |
4 |
|
30 minutes |
512.00 |
352.615 |
4 |
|
|
45 minutes |
792.25 |
133.145 |
4 |
|
|
Total |
658.17 |
318.813 |
12 |
|
|
5% |
15 minutes |
333.75 |
257.967 |
4 |
|
30 minutes |
501.00 |
247.202 |
4 |
|
|
45 minutes |
668.50 |
396.041 |
4 |
|
|
Total |
501.08 |
312.995 |
12 |
|
|
7% |
15 minutes |
341.75 |
400.215 |
4 |
|
30 minutes |
333.00 |
270.078 |
4 |
|
|
45 minutes |
600.50 |
137.963 |
4 |
|
|
Total |
425.08 |
292.516 |
12 |
|
|
Total |
15 minutes |
428.78 |
334.886 |
36 |
Table 1 above shows the average value of the total of Bacillus sp. colonies based on the dose and contact time of immersion (disinfection) using green betel leaf extract in the medical waste recycling process. The lowest average was at a concentration of 0.3% with a contact time of 45 minutes (205 colonies/ml), and the highest average was at a concentration of 3% with a contact time of 45 minutes (792 colonies/ml). Moreover, the results of the homogeneity test are presented in Table 2 below.
Table 2 shows the output results of the homogeneity test. Based on these results, a p-value of 0.001 was found. The analysis criteria were if the p-value is larger than α (0.05), then the data are homogeneous or H0 is rejected. Table 2 shows that the p-value for the number of Bacillus sp. obtained was greater than α (0.05); therefore, the data were categorized as homogeneous and H0 was rejected. Moreover, the results of the ANOVA test are presented in Table 3 below.
Table 2. Levine test homogeneity assumption results
|
Dependent Variable: Bacillus sp. |
|||
|
F |
df1 |
df2 |
Sig. |
|
1.636 |
26 |
81 |
0.059 |
Table 3. Dependent variable two-way ANOVA test results
|
Dependent Variable: Bacillus sp. |
|||||
|
Source |
Type III Sum of Squares |
df |
Mean Square |
F |
Sig. |
|
Corrected Model |
2633476.963a |
26 |
101287.576 |
0.809 |
0.724 |
|
Intercept |
25353885.040 |
1 |
25353885.040 |
202.428 |
0.000 |
|
Dose |
1428066.130 |
8 |
178508.266 |
1.425 |
0.199 |
|
Contact Time |
236476.519 |
2 |
118238.259 |
0.944 |
0.393 |
|
Dose*Contact Time |
968934.315 |
16 |
60558.395 |
0.484 |
0.949 |
|
Error |
10145164.000 |
81 |
125248.938 |
|
|
|
Total |
38132526.000 |
108 |
|
|
|
|
Corrected Total |
12778640.960 |
107 |
|
|
|
|
a. R Squared=0.206 (Adjusted R Squared=-0.049) |
|||||
Table 3 shows the two-way ANOVA test results, which include the p-value of the dose (0.199), contact time (0.393), and dose contact time (0.949). The provisions of the analysis were if the p-value is larger than α (0.05), then H0 is rejected or the variable is said to have a significant difference. Based on the table above, the p-value was larger than 0.05; therefore, H0 is accepted. This means that there was no difference in the length of contact time and dose of green betel leaf extract as a disinfectant on the amount of Bacillus subtilis in the medical waste recycling process.
The bivariate statistical test results showed that there were no differences in the length of contact time and dose of green betel leaf extract as a disinfectant on the number of Bacillus subtilis in the medical waste recycling process. On the other hand, the descriptive analysis results show that the betel leaf extracts with a concentration of 0.3% and a contact time of 45 minutes had the lowest average number of Bacillus subtilis (205 colonies/ml). It is estimated that the essential oil content in betel leaves reaches 5%, and it mostly consists of bitter phenols that can be used as antibacterials [31, 32]. This implies that betel leaf extract has active anti-bacterial substances, including Bacillus sp.
Result of identification and measurement of Bacillus sp.
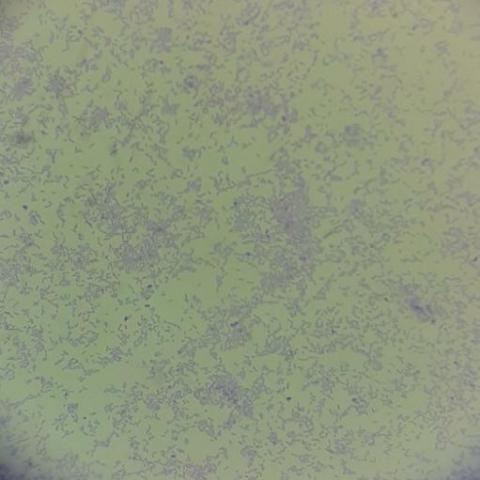
The presence of Bacillus sp. (Figure 4 and Figure 5) was identified identified in the green betel leaf extract immersion (disinfection) process in the medical waste recycling process. Figure 4 shows the presence of Bacillus subtillis, while Figure 5 shows the absence of Bacillus stearothermophillus in the gram staining process.
The presence of Bacillus sp. was identified in the immersion process (disinfection) with green betel leaf extract in the medical waste recycling process [33]. Meanwhile, Bacillus stearothermophillus was not found in the gram staining process. The measurement results of Bacillus subtillis and Bacillus stearothermophillus are presented in Figure 6 below.
Figure 4. Bacillus stearothermophillus bacteria gram staining results
Figure 5. Bacillus subtillis bacteria identification results
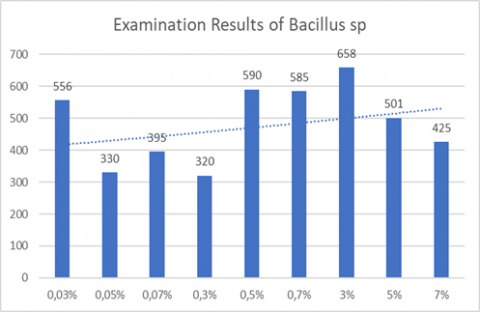
Figure 6. Bacillus subtillis and bacillus stearothermophillus measurement results
The results show fluctuating Bacillus sp. measurements in the process of immersion (disinfection) with green betel leaf extract in the medical waste recycling process. The smallest amount of Bacillus sp. was found at a green betel leaf immersion concentration of 0.05% (330 colonies/ml), and the largest Bacillus sp. colony occurred at a concentration of 3% immersion (658 colonies/ml). The average Bacillus sp. colony reached 485 ml/colony with a standard deviation of 121.96.
The results of the above analysis prove that there is a very large possibility of Bacillus sp. dying due to green betel leaf extract. Betel green leaf extract contains certain substances that have antimicrobial effects. These substances are flavonoids, polyphenols, alkaloids, tannins, saponins, and essential oils [34]. Flavonoids include antibacterial substances. Flavonoids work by damaging the bacterial cell wall, microsomes, and lysosomes as a result of flavonoid interaction with bacterial DNA. In addition, the hydroxyl group found in the structure of flavonoid compounds causes changes in organic components, and nutrient transport in bacteria is disrupted [35]. In addition, flavonoids in green betel leaf extract can inhibit the enzyme topoisomerase II (DNA gyrase). This enzyme is important in the process of bacterial DNA replication and transcription. Inhibition of the topoisomerase II enzyme will have an impact on the replication and transcription process of bacterial DNA, possibly inhibiting it [36].
Tannin substances that are also possessed by green betel leaf extract have spasmolytic properties [35, 37]. It is thought that they can wrinkle the cell wall or cell membrane, thus disrupting the permeability of the cell itself. Due to the disruption of permeability, cells cannot carry out life activities. As a result, their growth is inhibited, or they may even die. Tannins are also thought to inhibit bacterial growth by inactivating enzymes [29]. If the work of enzymes in maintaining the continuity of microbial activity is inhibited, it will cause enzymes to require large amounts of energy for their activity. As a result, growth energy is reduced, and microbial activity becomes inhibited and lysis occurs if it continues.
Saponins work to reduce surface tension and damage cell walls. Essential oils will interfere with the process of cell wall formation, causing them to not formed or form incompletely. Damage to the cell wall causes the cell membrane to have no protection, which results in the loss of the semi-permeability of the cell membrane [29]. This will cause issues with the entry and exit of substances such as water and enzymes. A further impact is the disruption of cell metabolism, causing the process of ATP formation for cell growth to be inhibited. If this process continues, it will lead to bacterial cell death.
This study showed that green betel leaf extract has anti-bacterial power against Bacillus sp. Antibacterial testing using the liquid dilution method had a minimum kill level (KBM) at a concentration of 0.3%. This finding is supported by previous research conducted by Juliantina et al. [38], which found that red betel leaf extract (Piper crocatum) could inhibit growth and kill gram-positive Staphylococcus aureus test bacteria at a concentration of 25%. It also had the ability to inhibit growth and kill gram-negative Escherichia coli test bacteria at a concentration of 6.25%. Furthermore, Mutmainnah [39] research also supports these findings. This previous study observed the effects of red betel leaf extract (Piper crocatum) on the histopathological picture of skin incision wounds of white rats infected with Staphylococcus aureus, as well as the effectiveness of red betel leaf extract (Piper crocatum) against Aeromonas hydrophila bacteria in vitro. This shows that betel leaf extract has active anti-bacterial substances, including against Bacillus sp. The limitation in this study is that the test was only carried out after treatment without any pre-treatment and control treatment.
The results of the bivariate statistical tests showed that there were no differences in the length of contact time and dose of green betel leaf extract as a disinfectant on the total amount of Bacillus subtilis in the medical waste recycling process. The smallest amount of Bacillus sp. was found at a concentration of 0.05% green betel leaf immersion (330 colonies/ml). The largest Bacillus sp. colonies occurred at a concentration of 3% immersion (658 colonies/ml). The antimicrobial green betel leaf content be developed for further research in the removal of bacteria or other parasites.
The authors would like to thank the Bandung Health Polytechnic; Santo Borromeus University; and Sebelas Maret University for supporting this study.
[1] Wilson, D.C., Rodic, L., Modak, P., Soos, R., Carpintero, A., Velis, K., Iyer, M, Simonett, O. (2015). Global waste management outlook. UNEP. https://doi.org/10.18356/765baec0-en
[2] Andeobu, L., Wibowo, S., Grandhi, S. (2022). Medical waste from covid-19 pandemic-a systematic review of management and environmental impacts in Australia. International Journal of Environmental Research and Public Health, 19(3): 1381. https://doi.org/10.3390/ijerph19031381
[3] World Health Organization (WHO). Health-care waste, World Health Organization (WHO). https://www.who.int/news-room/fact-sheets/detail/health-care-waste, accessed on Feb. 22, 2023.
[4] Persi, Klhk: MOEF: 18,000 Tons of Hazardous Medical Waste During Pandemic, Perhimpunan Rumah Sakit Seluruh Indonesia, 2021. https://www.cnnindonesia.com/nasional/20210728143345-20-673357/klhk-ada-18-ribu-ton-limbah-medis-berbahaya-selama-pandemi, accessed on Feb. 22, 2023.
[5] Fikri, E., Kurniati, I., Wartiniyati, W., Budi Prijanto, T., Pujiono, P., Syarief, O., Sharaf Eldin Khair, A. (2021). The phenomenon of medical waste recycling in Indonesia: Contact time and chlorine dose as a disinfectant with the bio-indicator Bacillus subtilis and Bacillus stearothermophilus. Journal of Ecological Engineering, 2(4): 47-58. https://doi.org/10.12911/22998993/133965
[6] O’Sullivan, D., Rahamathulla, M., Pawar, M. (2020). The impact and implications of covid-19: An Australian perspective. The International Journal of Community and Social Development, 2(2): 134-151. https://doi.org/10.1177/2516602620937922
[7] Capoor, M.R., Parida, A. (2021). Biomedical waste and solid waste management in the time of covid-19: A comprehensive review of the national and international scenario and guidelines. Journal of Laboratory Physicians, 13(02): 175-182. https://doi.org/10.1055/s-0041-1729132
[8] Singh, N., Tang, Y., Ogunseitan, O.A. (2020). Environmentally sustainable management of used personal protective equipment. Environmental Science & Technology, 54(14): 8500-8502. https://doi.org/10.1021/acs.est.0c03022
[9] Jones, S. (2020). Waste management in Australia is an environmental crisis: What needs to change so adaptive governance can help?. Sustainability, 12(21): 9212. https://doi.org/10.3390/su12219212
[10] Akter, N., Tränkler, J. (2003). An analysis of possible scenarios of medical waste management in Bangladesh. Management of Environmental Quality: An International Journal, 14(2): 242-255. https://doi.org/10.1108/14777830310470459
[11] Bokhoree, C., Beeharry, Y., Makoondlall-Chadee, T., Doobah, T., Soomary, N. (2014). Assessment of environmental and health risks associated with the management of medical waste in Mauritius. APCBEE Procedia, 9: 36-41. https://doi.org/10.1016/j.apcbee.2014.01.007
[12] Udofia, E.A., Fobil, J.N., Gulis, G. (2015). Solid medical waste management in Africa. African Journal of Environmental Science and Technology, 9(3): 244-254. https://doi.org/10.5897/AJEST2014.1851
[13] Adiputra, I.G.A.B., Giriantari, I.A., Kumara, I.N. (2019). Kajian penggunaan incinerator untuk mengelola limbah medis padat di denpasar. Majalah Ilmiah Teknologi Elektro, 18(3): 369-376. https://doi.org/10.24843/MITE.2019.v18i03.P10
[14] Irianti, S., Prasetyoputra, P. (2019). Waste management in indonesian public health centres: Factors associated with waste segregation practices and disposal methods. Jurnal Ekologi Kesehatan, 18(1): 1-14.
[15] Sharma, R., Sharma, M., Sharma, R., Sharma, V. (2013). The impact of incinerators on human health and environment. Reviews on Environmental Health, 28(1): 67-72. https://doi.org/10.1515/reveh-2012-0035
[16] Rizan, C., Bhutta, M.F., Reed, M., Lillywhite, R. (2021). The carbon footprint of waste streams in a UK hospital. Journal of Cleaner Production, 286: 125446. https://doi.org/10.1016/j.jclepro.2020.125446
[17] Turnbull, P.C.B. (1996). Medical Microbiology. 4th Edition. University of Texas Medical Branch, Galveston, USA.
[18] Fazal, F., Mane, P.P., Rai, M.P., Thilakchand, K.R., Bhat, H.P., Kamble, P.S., Palatty, P.L., Baliga, M.S. (2014). The phytochemistry, traditional uses and pharmacology of Piper Betel. linn (betel leaf): A pan-asiatic medicinal plant. Chinese Journal of Integrative Medicine, 1-11. https://doi.org/10.1007/s11655-013-1334-1
[19] Kaypetch, R., Thaweboon, S. (2018). Antifungal property of Piper betle leaf oil against oral Candida species. In MATEC Web of Conferences. EDP Sciences, 242: 01021. https://doi.org/10.1051/matecconf/201824201021
[20] Chowdhury, U., Baruah, P.K. (2020). Betelvine (Piper betle L.): A potential source for oral care. Curr. Bot, 87-92. https://doi.org/10.25081/cb.2020.v11.6130
[21] Arambewela, L.S., Arawwawala, M.L., Withanage, D., Kulathunga, S. (2010). Efficacy of betel cream on skin ailments. Journal of Complementary and Integrative Medicine, 7(1). https://doi.org/10.2202/1553-3840.1391
[22] Nayaka, N.M.D.M.W., Sasadara, M.M.V., Sanjaya, D.A., Yuda, P.E.S.K., Dewi, N.L.K.A.A., Cahyaningsih, E., Hartati, R. (2021). Piper betle (L): Recent review of antibacterial and antifungal properties, safety profiles, and commercial applications. Molecules, 26(8): 2321. https://doi.org/10.3390/molecules26082321
[23] Kusuma, M.S., Susilorini, T.E., Surjowardojo, P. (2017). Effect of duration and storage temperature of green betel leaf extract (Piper betle linn) with distilled water on the inhibition of Streptococcus agalactiae bacteria causing mastitis in dairy cows. TERNAK TROPIKA Journal of Tropical Animal Production, 18(2): 14-21. https://doi.org/10.21776/ub.jtapro.2017.018.02.3
[24] Okonogi, S., Phumat, P., Khongkhunthian, S., Suttiat, K., Chaijareenont, P. (2021). Denture-soaking solution containing piper betle extract-loaded polymeric micelles; inhibition of candida albicans, clinical study, and effects on denture base resin. Antibiotics, 10(4): 440. https://doi.org/10.3390/antibiotics10040440
[25] Phumat, P., Khongkhunthian, S., Wanachantararak, P., Okonogi, S. (2020). Comparative inhibitory effects of 4-allylpyrocatechol isolated from Piper betle on Streptococcus intermedius, Streptococcus mutans, and Candida albicans. Archives of Oral Biology, 113: 104690. https://doi.org/10.1016/j.archoralbio.2020.104690
[26] Sari, R., Isadiartuti, D. (2006). Effectiveness study of betel leaf extract hand antiseptic gel preparation (Piper betle Linn.). Majalah Farmasi Indonesia, 17(4): 163-169.
[27] Aznury, M., Sari, R.P. (2020). Green betel leaf liquid extract-based hand sanitizer gel product (Piper betle linn.) sebagai antiseptik. Kinetika, 11(1): 27-35. https://jurnal.polsri.ac.id/index.php/kimia/index.
[28] Basak, S. (2018). The use of fuzzy logic to determine the concentration of betel leaf essential oil and its potency as a juice preservative. Food Chemistry, 240: 1113-1120. https://doi.org/10.1016/j.foodchem.2017.08.047
[29] Periyanayagam, K., Jagadeesan, M., Kavimani, S., Vetriselvan, T. (2012). Pharmacognostical and phyto-physicochemical profile of the leaves of Piper betle L. var Pachaikodi (Piperaceae)-valuable assessment of its quality. Asian Pacific Journal of Tropical Biomedicine, 2(2): S506-S510. https://doi.org/10.1016/S2221-1691(12)60262-7
[30] Karak, S., Acharya, J., Begum, S., Mazumdar, I., Kundu, R., De, B. (2018). Essential oil of Piper betle L. leaves: Chemical composition, anti-acetylcholinesterase, anti-β-glucuronidase and cytotoxic properties. Journal of Applied Research on Medicinal and Aromatic Plants, 10: 85-92. https://doi.org/10.1016/j.jarmap.2018.06.006
[31] Syahidah, A., Saad, C.R., Hassan, M.D., Rukayadi, Y., Norazian, M.H., Kamarudin, M.S. (2017). Phytochemical analysis, identification and quantification of antibacterial active compounds in betel leaves, Piper betle methanolic extract. Pakistan Journal of Biological Sciences: PJBS, 20(2): 70-81. https://doi.org/10.3923/pjbs.2017.70.81
[32] Bari, M.S., Khandokar, L., Haque, E., Romano, B., Capasso, R., Seidel, V., Haque, M.A., Rashid, M.A. (2021). Ethnomedicinal uses, phytochemistry, and biological activities of plants of the genus Gynura. Journal of Ethnopharmacology, 271: 113834. https://doi.org/10.1016/j.jep.2021.113834
[33] Hidup, M.L. (2015). Peraturan menteri lingkungan hidup dan kehutanan republik indonesia nomor 56 tahun 2015. Tata Cara Dan Persyaratan Teknis Pengelolahan Limbah Bahan Berbahaya Dan Beracun Dari Fasilitas Pelayanan Kesehatan. Indonesia: Kementerian Lingkungan Hidup Republik Indonesia.
[34] Madhumita, M., Guha, P., Nag, A. (2019). Extraction of betel leaves (Piper betle L.) essential oil and its bio-actives identification: Process optimization, GC-MS analysis and anti-microbial activity. Industrial Crops and Products, 138: 111578. https://doi.org/10.1016/j.indcrop.2019.111578
[35] Taukoorah, U., Lall, N., Mahomoodally, F. (2016). Piper betle L.(betel quid) shows bacteriostatic, additive, and synergistic antimicrobial action when combined with conventional antibiotics. South African Journal of Botany, 105: 133-140. https://doi.org/10.1016/j.sajb.2016.01.006
[36] Kurnia, D., Hutabarat, G.S., Windaryanti, D., Herlina, T., Herdiyati, Y., Satari, M.H. (2020). Potential allylpyrocatechol derivatives as antibacterial agent against oral pathogen of S. sanguinis ATCC 10,556 and as inhibitor of MurA enzymes: In vitro and in silico study. Drug Design, Development and Therapy, 2977-2985. https://doi.org/10.2147/DDDT.S255269
[37] Balaji, K., Lisa, T., Sarnnia, T.S., Mirza, B. (2011). Antibacterial activity of Piper betel leaves. International Journal of Pharmacy Teaching and Practices, 2(3): 129-132.
[38] Juliantina, F., Citra, D.A., Nirwani, B., Nurmasitoh, T., Bowo, E.T. (2009). Manfaat sirih merah (Piper crocatum) sebagai agen anti bakterial terhadap bakteri gram positif dan bakteri gram negatif. Jurnal Kedokteran dan Kesehatan Indonesia, (1): 12-20.
[39] Mutmainnah, A. (2013). Pengaruh pemberian ekstrak daun sirih merah (Piper crocatum) terhadap gambaran histopatologi luka insisi kulit tikus putih yang terinfeksi Staphylococcus aureus. Universitas Airlangga. http://repository.unair.ac.id/id/eprint/21536.